
Abstract
Johnson developed a typology of intimate partner violence (IPV) which includes two different categories of violence: situational couple violence (SCV) and intimate terrorism (IT). Johnson proposed that IT is more likely to be found in clinical samples (e.g., batterer intervention programs or domestic violence shelters) compared to nonclinical (general population) samples. This meta-analysis (n = 149 studies; k = 216 effect sizes) examines differences in the strengths of IPV risk markers in clinical and nonclinical samples of male perpetrators and female victims. All variables (communication and conflict resolution, demand–withdraw patterns, relationship dissatisfaction, controlling behaviors, jealousy, patriarchal beliefs, power in the relationship, and stalking) were expected to be significantly related to IPV for both clinical and nonclinical populations. However, specific variables indicative of IT (control, jealousy, patriarchal beliefs, power, and stalking) were expected to be more strongly associated with clinical samples compared to nonclinical samples. As expected, most variables were significant for clinical and nonclinical populations, and IT risk markers (control, power, jealousy, and patriarchal beliefs) were significantly stronger risk markers for IPV in clinical samples. These results indicate that Johnson’s typology may be conceptualized as representing a continuum of violence, with IT being more severe due to the controlling nature of the violence. Sample type needs to be considered when research about IPV is disseminated, as different degrees of IPV (IT vs. SCV) may be present depending on sample type. Implications from this study include the need to differentiate the level of violence and to tailor intervention for IPV appropriately.
Johnson’s intimate partner violence (IPV) typology has had a profound influence on IPV research and intervention (Johnson, 1995, 2007, 2008; Johnson, Leone, & Xu, 2014). According to Johnson’s typology of IPV, there are two prevalent forms of IPV: intimate terrorism (IT) and situational couple violence (SCV). The type of IPV (IT or SCV) that is being examined in a research study may be dependent on the data collection method that was utilized (Johnson, 2007). For example, data collected from clinical populations (e.g., batterer intervention programs and domestic violence shelters) may be more representative of IT, and data collected from nonclinical (e.g., general population) populations may be more representative of SCV. A number of meta-analytic studies have been conducted to synthesize research on IPV risk markers (e.g., Archer, 2000; Kimmes et al., 2017; Smith-Marek et al., 2015; Spencer, Cafferky, & Stith, 2016; Spencer et al., 2017; Stith, Green, Smith, & Ward, 2008; Stith, Smith, Penn, Ward, & Tritt, 2004), without the focus of sample type as a differentiating factor for Johnson’s typology. Previous studies have included sample type as an association of violence in relationships (e.g., Graham-Kevan & Archer, 2003a); however, no previous meta-analytic studies have examined the moderation effect of sample type on risk markers for IPV. In this study, we seek to determine whether or not the strength of risk markers related to IT and SCV significantly differ between studies collected from clinical data sets (e.g., batterer intervention programs or domestic violence shelters) and studies examining nonclinical populations.
Johnson (2007) describes IT and SCV as significantly different from one another based on one particular key element: control. Johnson and others have defined IT as marked by a general need to exert control over one’s partner, often through dominance and potentially physical violence (Johnson & Leone, 2005, p. 323). Conversely, SCV is the result of a mutually escalating conflict between partners that leads to physical violence (Johnson, 2006b). Based on the difference between the presence of controlling behaviors or dominance in each of these situations, it is argued that the prevalence, severity, and context of violence may vary by the type of sample used in research studies (Johnson et al., 2014). The purpose of this meta-analysis is to understand how the strength of risk markers often associated with IT and SCV compare/differ by sampling pools. Based on the work of Johnson and colleagues, we hypothesize that risk markers associated with IT (i.e., controlling behaviors, jealousy, patriarchal beliefs, perpetrator’s power, and stalking) will be significantly stronger in the clinical population than in the nonclinical population. However, we hypothesize that the strength of SCV risk markers (e.g., communication and conflict resolution, demand–withdraw patterns, and relationship satisfaction) would not differ between samples drawn from clinical and nonclinical samples because it is assumed that each of these risk markers would be significant for violence in any relationship.
Theories of Violence
According to Johnson’s descriptions of IT, the need to assert control over one’s partner is rooted in dominance, which is associated with feminist theories of violence. Feminist theories of violence purport that violence in relationships is predominantly due to a societally ingrained hostility toward women and that violence is used as a means to maintain control and power over women (Bograd, 1988; Dobash & Dobash, 1979; Marin & Russo, 1999). This hostility derives from patriarchal notions of gender traditionalism and control and has been demonstrated by multiple studies to be a contributing factor of violence from men toward women (Felson & Messner, 2000; Holtzworth-Munroe, Meehan, Herron, Rehman, & Stuart, 2000; Johnson, 2007; Sugarman & Frankel, 1996).
SCV, on the other hand, is associated with family violence theories. According to those that study from a family violence perspective, violence is not more likely to be perpetrated by either gender and is instead initiated through mutually escalating conflict (Straus, 2011). Often, this type of conflict begins as arguing or shouting and then leads to some form of physical involvement, such as pushing, slapping, or hitting. Retaliation is likely to occur in these situations, but not always through physical violence. This description resembles Johnson’s (2006b, 2008) SCV, which Johnson agrees is equally likely to be perpetrated by men and women.
Risk Markers for Violence
IT risk markers
Coercive control is the primary motive for IT (Johnson, 2008). Controlling behaviors in a relationship may include threatening violence, limiting access to friends or family, abusing pets, not allowing the partner access to bank accounts, or keeping the partner away from their biological children. In IT, controlling behaviors are typically used in conjunction with physical violence toward the partner. These controlling behaviors often instill fear or terror in the partner as she is unsure how the perpetrator will abuse her next (Johnson, 2008). Power, on the other hand, describes the influence one partner has over the relationship (Johnson, 2006a). Power may be overtly displayed, such as taking full responsibility for the finances or child-rearing, or more covertly, such as making important decisions without consulting the partner (Johnson, 2008). Although increased power in the relationship is not necessarily a singular risk factor for IT, if the power is excessively unbalanced in the relationship (i.e., the other partner has very little or none), it has potential to be a risk factor (Frye, Manganello, Campbell, Walton-Moss, & Wilt, 2006).
Other variables that frequently appear in IPV literature include jealousy and stalking, which are both related to a partner’s desire to control the other (Davis, Ace, & Andra, 2000; Melton, 2007). Jealousy is often included in research on IPV as a motivating factor for violence and is a behavioral demonstration of control (Frye et al., 2006). Examples of jealous behavior may include anger at the partner for talking to or spending time with others, prohibiting the partner from engaging in certain activities, or checking the partner’s phone or accounts. Extreme forms of jealousy can lead to stalking behaviors, such as following or watching the partner, often without the partner’s knowledge or consent (Cupach & Spitzberg, 2000). Severe forms of stalking have been associated with more severe IPV (Burgess et al., 1997; Norris, Huss, & Palarea, 2011). Each of these risk markers are characteristic of IT and are likely to be stronger risk markers for IT than for SCV. In this study, we examine controlling behaviors, jealousy, perpetrator’s power in the relationship, perpetrator’s patriarchal beliefs, and stalking as IPV risk markers, which we hypothesize to be more strongly related to IT than to SCV.
SCV risk markers
Johnson (2008) described SCV as violence that is “situationally provoked” (p. 11). In other words, this is violence that escalates from a mutual conflict and is not motivated by a need to control or overpower the other partner. SCV stems from how the couple manages conflict, which is impacted by both interpersonal dynamics and conflict management skills (Johnson, 2008). Conflict resolution and communication skills are common variables to assess when examining violence in relationships because couples who engage in verbal aggression or possess verbal skill deficits have greater potential to escalate to violence (Johnson, 2008). However, we did not hypothesize that conflict resolution or communication skills would be less predictive of IPV in clinical samples since it was expected that this risk marker would be present in either type of sample. Further, engaging in other destructive conflict resolution strategies, including withdrawal patterns or conflict engagement, are more likely to escalate conflicts to the point of violence (Feldman & Ridley, 2000).
Demand and withdraw patterns in relationships frequently stems from insecure attachment (usually anxious attachment) in one or both partners. Individuals with anxious attachment develop a significant fear of abandonment and rejection, which can lead individuals to act out when their partner shows signs of lack of support or commitment to the relationship (Mikulincer & Shaver, 2007). Anxiously attached individuals are likely to pursue or demand attention and loyalty from their partner, which may cause the partner to withdraw from the overly demanding individual. The demand–withdraw pattern is well-documented in its association with aggression and violence, particularly in men, toward their female partners (Fournier, Brassard, & Shaver, 2011; Mikulincer & Shaver, 2007; Roberts & Noller, 1998). This attachment pattern is consistent with Johnson’s (2008) description of SCV, in that conflicts may escalate when one or both partners does not receive the desired response, particularly in stressful conversations or situations; however, this pattern may also be prevalent in IT when an offender demands a specific response from a partner. Therefore, we did not hypothesize that this pattern would be more prevalent in community samples than in clinical samples.
Relationship dissatisfaction is commonly associated with insecure attachment, and as such is a documented risk marker for IPV (Feeney, 1999; Stith et al., 2008). Dissatisfaction within a romantic relationship is a particularly strong risk marker for male-perpetrated violence (O’Leary, Smith Slep, & O’Leary, 2007). Relationship dissatisfaction may stem from a variety or culmination of factors, including demand–withdraw patterns (Eldridge, Sevier, Jones, Atkins, & Christensen, 2007), exhibition of dominance behaviors (Sadikaj, Moskowitz, & Zuroff, 2016), low trust in the other partner (Wieselquist, 2009), or circumstantial events (e.g., infidelity, illness). It is difficult to discern whether relationship dissatisfaction or violence precedes the other, particularly, as many IPV studies are cross-sectional (Ulloa & Hammett, 2015). However, in studies that examined temporal ordering, dissatisfaction in the relationship and perpetration of violence have a bidirectional relationship for men. It is hypothesized that men’s lack of satisfaction in the relationship may prompt aggressive behaviors to exert more influence, but a lack of impact from these behaviors may lead to further dissatisfaction (Lawrence & Bradbury, 2007). Although the cause of dissatisfaction in the present study is not known, relationship dissatisfaction was included due to its likely correlation with violence in both types of samples.
In this study, we examine communication and conflict resolution, demand–withdraw relationship patterns, and relationship dissatisfaction as IPV risk markers related to SCV but do not anticipate that they would be significantly stronger risk markers in SCV than in IT.
Clinical Versus Nonclinical Data
There is debate in the IPV literature about the motivation, intensity, and characteristics of violence in relationships. Johnson (1995) argues that different types of violence emerge depending on the source from which the sampling was drawn. He argues that sampling is biased and reveals different patterns of violence, which may then be erroneously generalized to all IPV scenarios. Previous studies that examine the potential for Johnson’s typology include a focus on victim outcomes, which yield conflicting conclusions regarding typologies of violence due to lack of focus on the perpetrator and are often limited by only including survey data (Anderson, 2008; Dutton & Goodman, 2005). Studies that measure controlling behaviors of the perpetrator provide support for Johnson’s description of IT (Graham-Kevan & Archer, 2003a, 2003b); however, these studies are limited in sample size and scope. Meta-analyses that intentionally included sample type as a moderator (e.g., Archer, 2000; Stith et al., 2008) did not compare strengths of risk markers for clinical and nonclinical samples to discern how different samples yield differing forms of violence. Due to the different types of violence being measured, shelter (clinical) population data cannot be generalized to survey data, just as survey data cannot be generalized to shelter populations (Graham-Kevan & Archer, 2003a). Coercive control is assumed to be the differentiating factor between SCV and IT (Johnson, 2008); without this element, it is difficult to make assumptions about which type of violence is being studied (Haselschwerdt, 2014). The purpose of this meta-analysis is to review IPV risk markers associated with IT and SCV in existing studies to determine whether different sampling populations do, in fact, reveal a discrepancy in the strength of risk markers for different types of violence found in these populations.
Survey data, generated from random sampling or convenience sampling, are a commonly used methodological approach for gathering participants. Survey data are generally distributed to an entire population and therefore tend to include a large amount of variability, which makes it ideal for studying topics such as IPV. Couples who experience SCV may not perceive their behavior to be abnormal or severe and are therefore more likely to report instances of “minor” violence in the relationship, particularly if it is mutual (Johnson, 1995). The hazard of using nonclinical population survey data to measure IPV, according to Johnson (1995; Johnson et al., 2014), is that perpetrators and victims of IT are less likely to complete survey data and are more likely to appear in clinical samples. SCV is presumed to be most likely to emerge in survey data distributed to nonclinical populations (Johnson, 2007; Johnson et al., 2014). Partners who perpetrate IT are hypothesized to prevent their victim from taking surveys or from engaging in surveys themselves, possibly for fear of revealing their level of violence or the severity of their controlling behaviors.
Clinical samples, such as samples drawn from clinical interventions, hospital settings where injuries were caused by IPV, domestic violence shelters, or police records, tell a very different story about IPV. These samples include predominantly women as victims, based on resources currently available to women that have been abused, such as battered women’s support groups and women’s shelters. Further, the injuries sustained by women in these sampling methods tend to be more severe (Johnson, 1995). For instance, women being interviewed in a hospital setting are likely to have severe enough injuries that treatment was necessary. Due to their size and strength compared to women, men are less likely to be hospitalized from injuries due to IPV (Johnson, 1995). Similarly, police record data include perpetrators who have been arrested or details of situations severe enough for police involvement. The strength of IPV risk markers related to IT and SCV are expected to be significantly different between nonclinical survey data versus clinical data. The hypotheses addressed in this study are as follows:
Method
Literature Search
Based on standards given by meta-analytic researchers (Borenstein, Hedges, Higgins, & Rothstein, 2011; Card, 2012), studies were selected and identified through a process of phases, producing a total of 149 studies reporting risk markers associated with physical IPV in both clinical and nonclinical populations, with a total of 216 effect sizes. The list of studies included in meta-analysis (n = 149) can be found in the Supplemental material.
The first phase of our literature search consisted of examining 509 studies from 1980 to 2000 which were previously considered and reviewed for a meta-analysis on risk markers for physical IPV (Stith et al., 2004). The articles in this first wave were obtained from databases (i.e., ERIC, PsychLit, Sociological Abstracts, MEDLINE, Social Sciences Abstracts, and Social Sciences Citations Index) using search terms identified in the previous study (Author, year). The kisecond literature search phase consisted of articles from 2001 to 2012 from databases such as MEDLINE, PROQUEST, and Web of Science. The search consisted of using key word terms such as risk markers (predictor, risk, factor, pathway, or correlate), partner aggression (aggression, domestic violence, abuse, batter, maltreatment, or violence), and couple (marital, spouse, husband, wife, intimate partner, or same-sex partner). The third literature search phase was included to update the data in the meta-analysis. This search used the same key terms previously used, searching articles from 2012 to 2016 in databases (PubMed, Web of Science, and PROQUEST).
Inclusion and Exclusion Criteria
Studies were included and excluded from this study based on certain criterion. The criteria for including articles was (1) if the outcome variable measured male perpetration of physical IPV, (2) the articles had pertinent information needed to compute bivariate effect size(s), (3) the articles were published in English, and (4) the sample included adult romantic relationships. Articles were selected for male perpetration of IPV due to male perpetration making up the majority of the IPV literature. Articles were excluded if they did not distinguish physical IPV from other forms of IPV such as emotional, psychological, or sexual. If articles contained samples from college students or adolescents, they were excluded because the focus of this meta-analysis was on risk markers in adult romantic relationships.
Included Samples
Articles were found by browsing reference lists (n = 470) and through databases (n = 24,668), totaling 25,138 studies. Duplicate articles (n = 5,535) were excluded, with 19,579 remaining studies to be evaluated during the first screening round. Out of these studies, 16,986 were removed from analysis based on the inclusion and exclusion criteria. Following this removal, 2,593 studies remained for additional screening (see Figure 1). Overall, 2,444 studies were excluded because they lacked sufficient information needed to calculate at least one effect size (9.2%), did not include pertinent risk markers (9.3%), measured dating violence (8.9%), physical IPV was not the target of the study (67.0%), the outcome was homicide (3.5%), the study sampled special populations (1.6%), or the study wasn’t published in English (0.5%). We contacted authors for studies that did not report information needed to compute a bivariate effect size. This study’s final sample contained 149 studies yielding 216 effect sizes.

Exclusion criteria flowchart.
Coding Procedures
The articles that were analyzed in this study were coded following recommended coding procedures (Card, 2012; Hunter & Schmidt, 2004). A graduate research team used a 37-item code sheet to track appropriate study information. Information gathered in the code sheet included statistical information to calculate a bivariate effect size, as well as study and sample characteristics such as publication date, international or domestic sample, and the location from which the sample was drawn. Over 75% of studies were cross-coded to check for discrepancies and accuracy of the coders and coders attained a 96% agreement rate. If discrepancies between coders were not resolved, researchers met with the project leader to collectively come to an agreed consensus.
Statistical Approach and Analyses
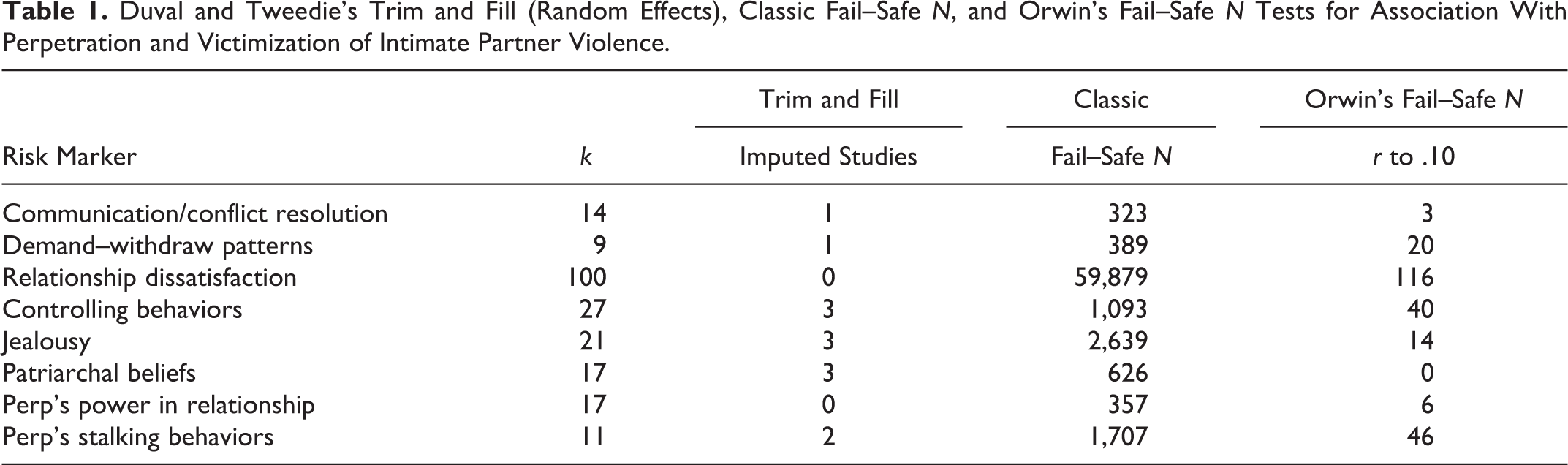
In order to assess the possibility for publication bias in our sample, knowing that our sample did not include every possible study (Hunter & Schmidt, 2004), we conducted tests to evaluate the possible effect that publication bias may have had on the accumulated effect sizes of (a) communication/conflict resolution, (b) demand–withdraw patterns, (c) relationship dissatisfaction, (d) controlling behaviors, (e) jealousy, (f) patriarchal beliefs, (g) perpetrator’s power in the relationship, and (h) stalking behaviors and their associations to male IPV perpetration. First, researchers ran a trim and fill test (Duval & Tweedie, 2000) utilizing a random effects plot in order to analyze the needed number of studies’ effect sizes to make a symmetrical distribution. Afterward, we projected fail–safe Ns for all of the correlates to assess how many possible studies are needed to raise the mean effect size under the p < .05 threshold (Rosenthal, 1979). Lastly, we utilized Orwin’s fail–safe Ns to estimate the number of possible missing studies where r = .00 needed to reduce the mean effect size (per correlate) down to r = .10 (the lower limit of small effect sizes; Cohen, 1992; Orwin, 1983). After running these three publication bias tests, our results indicated that the combined effect sizes were robust against potential publication bias (Table 1).
Duval and Tweedie’s Trim and Fill (Random Effects), Classic Fail–Safe N, and Orwin’s Fail–Safe N Tests for Association With Perpetration and Victimization of Intimate Partner Violence.
To account for the possibility there were actual population differences between studies, we used a random-effects model instead of a fixed-effect model. This allowed us to account for the within- and between-study variance. Had we elected to run a fixed-effects model, it would have only accounted for the variance within the study. Utilizing a random-effects model gives us the possibility to make generalized inferences beyond the studies which were included in this meta-analytic study (Card, 2012). A random-effects model was used when comparing clinical samples and nonclinical samples.
Data and effect sizes were analyzed with Comprehensive Meta-Analysis software (Version 3; Borenstein, Hedges, Higgins, & Rothstein, 2014) to assess the correlation of selected risk markers (i.e., communication/conflict resolution, demand–withdraw patterns, relationship dissatisfaction, controlling behaviors, jealousy, patriarchal beliefs, perpetrator’s power in the relationship, and stalking behaviors) with male physical IPV perpetration. Bivariate effect sizes that examined the direct relationship between the risk marker and male perpetration of IPV were used in the analysis. For studies that examined a risk marker using two different measures (i.e., measuring frequency and severity of controlling behaviors), mean effect sizes were computed for that particular study, so that there was only one effect size, per risk marker, included per study.
For our analysis, we created a variable that discerned whether the sample used in the study was considered to be a clinical sample or a nonclinical sample. For the purpose of the study, a clinical sample was considered a sample taken from a women’s shelter, a batterer’s intervention program, emergency room visits, or other samples where the participants were recruited from some type of violence intervention. Nonclinical samples included community samples or other recruitment methods that were aimed at the general public. Next, we measured the strength of the correlation between each variable (communication/conflict resolution, demand–withdraw patterns, relationship dissatisfaction, controlling behaviors, jealousy, patriarchal beliefs, perpetrator’s power in the relationship, and stalking behaviors) and male IPV perpetration for both clinical and nonclinical samples. We then compared each variable on whether or not they were significantly stronger risk markers for the clinical samples or nonclinical samples. We used Cohen’s (1992) suggested criteria for appraising the strength of the mean effect sizes (r < .01), small (r = .10), medium (r = .30), and large (r = .50).
Results
SCV Risk Markers
Of the SCV risk markers, we found that demand–withdraw relationship patterns was the strongest risk marker for IPV in both the clinical sample (r = .40, p < .001) and the nonclinical sample (r = .37, p < .001). Relationship dissatisfaction was significantly related to IPV for both the clinical sample (r = .30, p < .001) and the nonclinical sample (r = .26, p < .001). Lastly, communication and conflict resolution skills were significantly negatively related to IPV in the nonclinical sample (r = −.16, p < .01) but was not significantly related to IPV in the clinical sample.
IT Risk Markers
Stalking was the strongest IT risk marker for IPV in both the clinical sample (r = .45, p < .001) and the nonclinical sample (r = .46, p < .001). For the clinical sample, the next strongest risk marker for male IPV perpetration was controlling behaviors (r = .40, p < .001), followed by jealousy (r = .33, p < .001), the perpetrator’s power in the relationship (r = .29, p < .001), and patriarchal beliefs (r = .25, p < .001). For the nonclinical sample, the next strongest risk marker was control (r = .26, p < .001), jealousy (r = .16, p < .001), the perpetrator’s power in the relationship (r = .11, p < .05), and patriarchal beliefs (r = .09, p < .01).
Comparing Strength of Risk Markers Between Samples
When examining the situational violence risk markers (communication/conflict resolution, demand–withdraw relationship patterns, and relationship satisfaction), as hypothesized, there were no significant differences in the strength of risk markers between the clinical and nonclinical samples. Although all of the IT risk markers were significantly related to IPV in both samples, we found four risk markers that significantly differed in strength between the two samples. As hypothesized, controlling behaviors (Qb = 9.17, p < .01), patriarchal beliefs (Qb = 7.31, p < .01), jealousy (Qb = 5.37, p < .05), and perpetrator’s power in the relationship (Qb = 4.37, p < .05) were all found to be significantly stronger risk markers for IPV in the clinical sample compared to the nonclinical sample. However, there were no significant differences in the strength of stalking as a risk marker for IPV between the clinical and nonclinical sample (Table 2).
Examining and Comparing Intimate Partner Violence Risk Markers for Clinical and Nonclinical Samples.

Note. k = number of effect sizes; r = point estimate of effect size; CI = confidence interval; Qb = heterogeneity of between-group differences.
*p < .05. **p < .01. ***p < .001.
Discussion
More than two decades ago, Johnson (1995) created a typology of IPV to include IT and SCV. This has had a significant impact on the way researchers interpret results and in ways practitioners designed interventions for violence in relationships. It was hypothesized (Johnson, 1995, 2007; Johnson et al., 2014) that SCV would be most represented in the general or nonclinical population, whereas IT would be most represented in the clinical population. In order to verify Johnson’s theory, we utilized research from 1980 to 2016, resulting in a total of 149 studies, to meta-analyze risk markers that were previously associated with IT. Even though all risk markers included in this study were associated with couples experiencing violence in both the clinical and nonclinical samples, significant differences in the strengths of associations were found. As hypothesized in this study and by Johnson (1995), most risk markers characterized as related to IT were stronger predictors of IPV in the clinical sample than in the nonclinical population sample.
Based on the findings of this study, perpetrators of IT are more likely to be identified in clinical samples, such as shelters, hospitals, intervention programs, and police records. Perpetrators in these setting are more likely to exert high levels of power over their partners, exhibit more controlling behaviors, display more jealousy in the relationship, and be more likely to endorse patriarchal beliefs than perpetrators found in nonclinical samples (Hypothesis 1). These findings are consistent with findings from previous studies, in which victims of IT are more likely to seek formal help (e.g., police, hospitals, and counseling/social services; Haselschwerdt, 2014; Leone, Johnson, & Cohan, 2007). These findings indicate that strength of risk markers differ depending on where samples are drawn from and are therefore not equally applicable to all violence. Previous research addressing Johnson’s typology (e.g., Anderson, 2008; Felson & Outlaw, 2007; Ross & Babcock, 2009) does not specifically account for sampling; therefore, this study establishes a new critical understanding of differing risk markers for violence based on previous studies’ findings.
Further, this study examines perpetrator risk markers for violence, not victim risk markers. The variables in this study that is significantly associated with IT (controlling behaviors, power, jealousy, patriarchal beliefs, and stalking) are each characteristics or beliefs held by the perpetrator which then serve as risk markers for IPV. This is significantly different from examining characteristics of victims (e.g., fear or attempting to leave relationship). The fact that all of the risk markers examined in this study were related to IPV in nonclinical samples, as well as in clinical samples, suggests that we may want to start thinking of Johnson typology not as distinct categories, but instead as a continuum. The same risk markers were statistically significant for both the clinical and the nonclinical population. As the level of coercive control, patriarchal beliefs, jealousy, and power increases, the violent relationship may be closer to representing IT than SCV.
Implications for Practice, Policy, and Research
The results of this study have significant implications for research and practitioners alike. To begin with, all of the risk markers for IPV perpetration were significant in both sample types, with the exception of communication/conflict resolution, which was only significant for IPV in the nonclinical sample. This indicates that the risk markers included in this study must be taken in to account when conducting research or developing interventions for IPV, regardless of whether the offender is court ordered or part of a community sample. Currently, many intervention models are designed to address IT, but fewer interventions target SCV (Johnson, 2008). When couples choose to remain together after the offender completes a treatment program focused on coercive control but do not participate in an intervention addressing relationship factors, the likelihood of violence occurring again remains high. If a perpetrator were to attend an intervention for IT, which may address controlling behaviors, patriarchal beliefs, and jealousy, violence in the relationship may reduce on the continuum to more closely resemble SCV. However, the risk markers for SCV (e.g., communication and conflict resolution) would still need to be addressed to prevent further violence in the relationship or future relationships involving the perpetrator. Conversely, if a couple presents for treatment based on both partners perpetrating violence, it is still important to individually assess each partner’s frequency and severity of violence and overall safety in the relationship. Conjoint treatment of IPV when IT is present is contraindicated and may lead to further perpetuation of controlling behaviors.
Conducting studies on different risk markers for IPV perpetration or victimization without being intentional about sampling pools may lead to erroneous generalizations about how and why IPV occurs. Studies that utilize convenience sampling, such as general surveys, are unlikely to include a sample that represents the spectrum of violence. Similarly, studies that are specific to clinical samples are best utilized to describe relationships where one partner has significantly more control over the other, not violence that is bilateral. Further research that seeks to encompass and describe the continuum of violence in relationships will inform future clinical interventions for perpetrators and victims alike.
Strengths and Limitations
A significant limitation of this study is the examination of male perpetrators only. Although the researchers attempted to include female perpetration into the analysis, few or no studies were found that included these same risk markers for female perpetrators. As research on female perpetration of IPV increases, it would greatly benefit the field to mimic the design of this study to discern gender differences in strengths of risk markers for IT.
Another limitation is that this analysis included only one time point. This study is unable to identify the increase or decrease of risk markers associated with IPV over time; therefore, it does not allow for examining whether couples move through the continuum of violence between SCV and IT. Since risk markers predominantly associated with IT are also present in couples experiencing SCV, one could begin to question whether and how some couples’ experiences of risk markers are able to move them from SCV into IT, or vice versa. Future studies could look at this phenomenon by examining these risk markers longitudinally.
Conclusion
This study supports the theory that perpetrators of IPV in clinical samples are more likely to have risk markers strongly associated with IT. Risk markers associated with IT were significantly stronger in the clinical sample than in the nonclinical sample. Thus, the sampling design of a study is a proxy to study IT and SCV. This study also challenges the idea that risk markers present in relationships identified as IT in clinical populations differ from risk markers present in relationships of victims in the nonclinical population. Risk markers often associated with IT are not only significantly associated with IPV in clinical samples but also in nonclinical populations. The difference between the two groups, clinical and nonclinical, is not in the kind of risk markers associated with each of them but instead in the strength of the association. Thus, risk markers such as controlling behaviors, power, patriarchal beliefs, and jealousy, which are highly associated with IT, are more strongly associated with clinical samples than nonclinical samples. Perhaps a more accurate way to understand IPV typology is to think of each category not as a distinct type of violence, but as a continuum. Couples experiencing violence may experience controlling behaviors, power, and jealousy, in different levels; however, couples in the clinical population (IT) and those in the nonclinical population (SCV) experience them in different levels.
Supplemental Material
Supplemental Material, Appendix_A_Risk_Markers_for_IT_and_SCV - Perpetrator Risk Markers for Intimate Terrorism and Situational Couple Violence: A Meta-Analysis
Supplemental Material, Appendix_A_Risk_Markers_for_IT_and_SCV for Perpetrator Risk Markers for Intimate Terrorism and Situational Couple Violence: A Meta-Analysis by Heather A. Love, Chelsea M. Spencer, Scott A. May, Marcos Mendez and Sandra M. Stith in Trauma, Violence, & Abuse
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.