
Abstract
Violence against women is a pattern of behavior that violates their rights, limits their freedoms, blocks their individual development, and damages their health and well-being (Krug, 2002). Globally, an estimated 30% of women have experienced violence from their intimate partners (Devries et al., 2013). Intimate partner violence (IPV) is defined as behaviors within an intimate relationship that causes physical, sexual, or psychological harm, including physical aggression, sexual coercion, psychological abuse, and controlling behaviors. A multi-country study by the World Health Organization (WHO) focused on domestic violence against women reported that about 60% of women had experienced IPV at some point during their life (Garcia-Moreno et al., 2006; Mikton, 2010). Over the past two decades, abundant research has been conducted on the prevalence of IPV and its health impacts, figuring out that IPVs against women may lead to physical injury, disability or death, and women who experienced IPV reported a higher prevalence of health problems and risk behaviors (Fikree & Bhatti, 1999; Golding, 1996; Koss et al., 1991; Krug, 2002; Leserman et al., 1996; Makayoto et al., 2013; McCauley et al., 1995; Roberts et al., 1998; Salazar et al., 2009).
IPV during pregnancy is a serious form of violence. Its global prevalence is 28%, with it being higher in Africa (up to 57%) (Garcia-Moreno et al., 2006; Shamu et al., 2011). IPV negatively affects the health of both the woman and the fetus (Azene et al., 2019; Wang et al., 2017). Adverse health outcomes can be caused by direct injuries from physical abuse or due to the physiological effects of stress on the fetus’ growth and development. Non-fatal outcomes are generally more evident and include adverse pregnancy complications (e.g., premature delivery, miscarriage, antepartum hemorrhage, or intrauterine growth retardation), negative health behaviors (e.g., maternal drug and alcohol abuse, smoking, or delayed prenatal care), and adverse psychosomatic disorders (e.g., depression, anxiety, self-harm, or suicidal tendencies) (Alhusen et al., 2015; Azene et al., 2019; Donovan et al., 2016; Islam et al., 2017; Laelago et al., 2017; Miura & Fujiwara, 2017; Shamu et al., 2016).
Women with human immunodeficiency virus (HIV) also face an increased risk of IPV (Cohen et al., 2000; Koenig et al., 2002). Studies have suggested that this risk may be even higher in pregnant women with HIV (Dunkle et al., 2004; Maman et al., 2000). For instance, among pregnant women with HIV in Nigeria, one-third reported IPV (Ezeanochie et al., 2011). A study found that two-thirds of pregnant, HIV-infected Nigerian women reported verbal abuse, threats of violence, and sexual deprivation (Ezechi et al., 2009; Kapetanovic et al., 2014). The combination of IPV and HIV infection may result in even greater adverse consequences among women, and they seemed to have distinct pathways linking them to one another during pregnancy (Hatcher et al., 2014). First, the fear and experience of previous IPV changed the pregnant women’s decisions to take up HIV care services, and the anticipated IPV was associated with a decline in HIV testing (Hatcher et al., 2012; Maman et al., 2011; Medley et al., 2004; Turan et al., 2011; Turan et al., 2012). And then, if they were HIV-positive, women who experienced IPV in the past may fear violence upon disclosing their HIV status to their male partners as it could trigger IPV during pregnancy (Gielen et al., 2000; Gielen et al., 1997). Also, IPV, in turn, worsened HIV-related health through key pathways of lack of treatment adherence and poor mental health (Hatcher et al., 2014). IPV decreased the likelihood of HIV-positive women taking antiretroviral treatment (ART) when medically eligible, and women with IPV experience always missed clinic visits and delayed linkage to care (Cohen et al., 2004; Jones et al., 2010; Siemieniuk et al., 2010). Pregnant and post-partum women are a crucial population who need to be emphasized that nonadherence to HIV treatment can not only lead to death but also increase the risk of HIV transmission to their infants and partners (Lehman et al., 2009; Mofenson, 2010). Hence, IPV has been described as a common barrier to HIV treatment adherence during pregnancy (Mepham et al., 2011). Additionally, IPV, mental health, and HIV are closely related (Murray et al., 2006). Abundant literature has shown that IPV leads to depression and anxiety among pregnant women, and studies reported that poor mental health significantly lowered the ART adherence to HIV treatment (Beydoun et al., 2012; Groves et al., 2012; Urquia et al., 2011). Hence, for pregnant women, depressive symptoms were associated with a faster HIV disease progression and higher mortality (Ammassari et al., 2004; Antelman et al., 2007; Cook et al., 2002; Sumari-de Boer et al., 2012). Finally, IPV can lead to an increased risk of HIV transmission, both in terms of vertical transmission due to mother-to-child transmission (MTCT) or secondary transmission to partners due to unprotected sex. As known, the prevention of MTCT (PMTCT) has a huge potential of eliminating new HIV infections among infants. It has been proven to reduce new infant infections from an estimated 32% in the absence of treatment to as low as 1% (Coutsoudis et al., 1999; Lehman et al., 2009; Miura & Fujiwara, 2017; Mofenson, 2010). IPV, an obstacle to PMTCT uptake, worsens it and greatly increases the risk of HIV transmission from pregnant or breastfeeding women to the infant, potentially in a drug-resistant form (Cooper et al., 2002). The likelihood of secondary transmission to partners is also increased by high viral loads related to nonadherence to ART, particularly regarding unprotected sex (Hatcher et al., 2014). IPV, to its full extent, exacerbates adverse pregnancy and HIV outcomes.
Although a high prevalence of IPV was detected among pregnant women with HIV, previous studies have treated IPV as a common risk factor for HIV transmission. Limited research has been conducted with HIV-positive pregnant women as the main subject and aimed to understand their trauma of experiencing IPV, and no more information was about the specific adverse health impacts on this population with increased vulnerability (Hampanda, 2016; Kiarie et al., 2006; Yee et al., 2018). Therefore, in this meta-analysis, we focused on pregnant women with HIV, examined the adverse impact of IPV during pregnancy and post-partum, and intended to identify the gaps in psychological well-being and HIV treatment utilization between them and their IPV-free counterparts. Our results are expected to provide evidence for formulating targeted and effective interventions for IPV against HIV-positive pregnant women.
Methods
Search Strategy
We searched for observational studies that investigated the impact of IPV on HIV-positive women during pregnancy and post-partum and had quantitative results. Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, we developed a systematic literature search using the electronic databases (PubMed, Web of Science, Cochrane Library, and Embase) with no starting date and extended it up till December 31, 2020 (Moher et al., 2010). Individual studies about the populations of interest were presented as outcomes of effect sizes as odds ratios (ORs). Our search strategy was initially developed for the PubMed database and then adapted to other databases. The following themes and keywords were used to search for the related studies: (1) HIV infection: human immunodeficiency viruses or HIV or AIDS; (2) Domestic violence: domestic violence or intimate partner violence or IPV; and (3) Pregnancy: mother or infant or child or pregnant women or gravida. All three themes were combined by the Boolean operator “AND”. All references of the eligible studies were manually searched to identify additional relevant papers.
Eligibility Criteria
Observational studies that met the criteria were included. The study should (1) quantitatively examined the effect size of the association between any form of intimate partner or domestic violence and the adverse maternal or neonatal/infant outcomes among pre-and post-partum women living with HIV, (2) limited the violence that only occurred during pregnancy and post-partum (up to one year after childbirth) or from the current partner, (3) applied a clear definition/measurements and timeframe of violence (e.g., name of the questionnaire/scale/tool; during the past year or past month), and (4) was a peer-reviewed full-text article published in English. Papers were not excluded by sample size, exposure/outcome measure method, or geographical region. However, they were excluded if they were (1) literature reviews, meta-analyses, laboratory studies, descriptive studies, or case reports, (2) having outcomes presented without the impact of IPV, or (3) no effect size reported. If data were duplicated, we included the study with the longest observation period.
Data Extraction
We developed a standardized data collection form following the search criteria, and two authors independently performed the data extraction and comparison. The extracted items included title, first author, publication year, geographical region, study design, number of participants, adverse maternal or neonatal events, violence measures, survey period, and measures of association (i.e., adjusted ORs). Duplicate data from different publications were excluded, and the study with the most informative and complete data was selected. Data were used to establish a dataset systematically. Any discrepancies were resolved by discussion or by referring to the original articles.
Outcome Measure
The outcomes were reported as ORs. The ORs were directly used if the original study presented an association between any form of violence (physical, emotional, psychological, or sexual) and adverse maternal or neonatal impact (adverse impact was defined by the authors, e.g., ART nonadherence, and this definition differed across studies). To ensure the maximum comparability of the outcomes across studies, we inverted the reported ORs if studies presented an association between IPV and related positive maternal, neonatal, and HIV treatment outcomes.
Quality Assessment
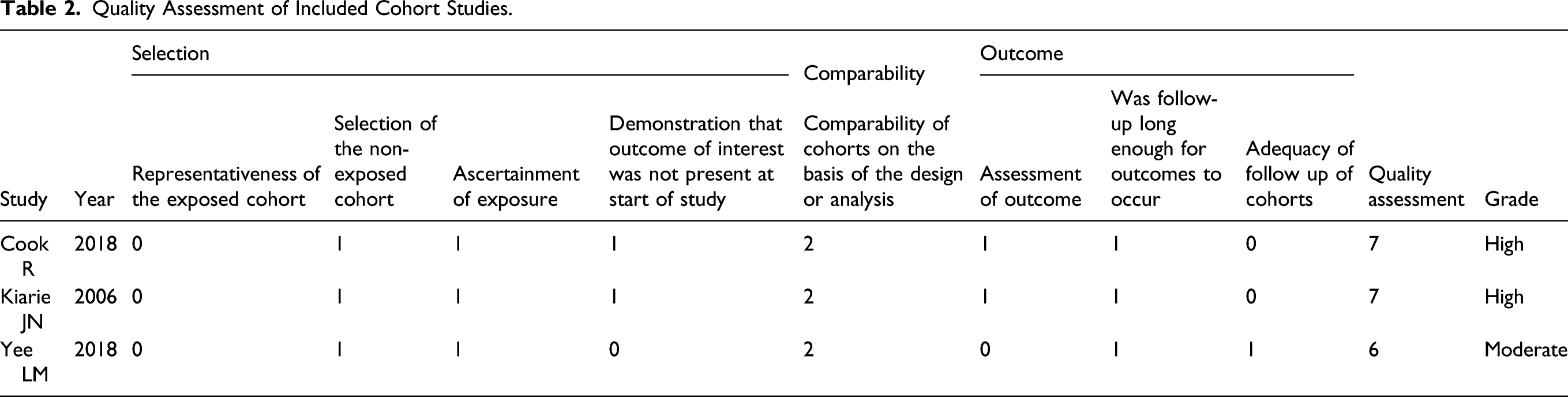
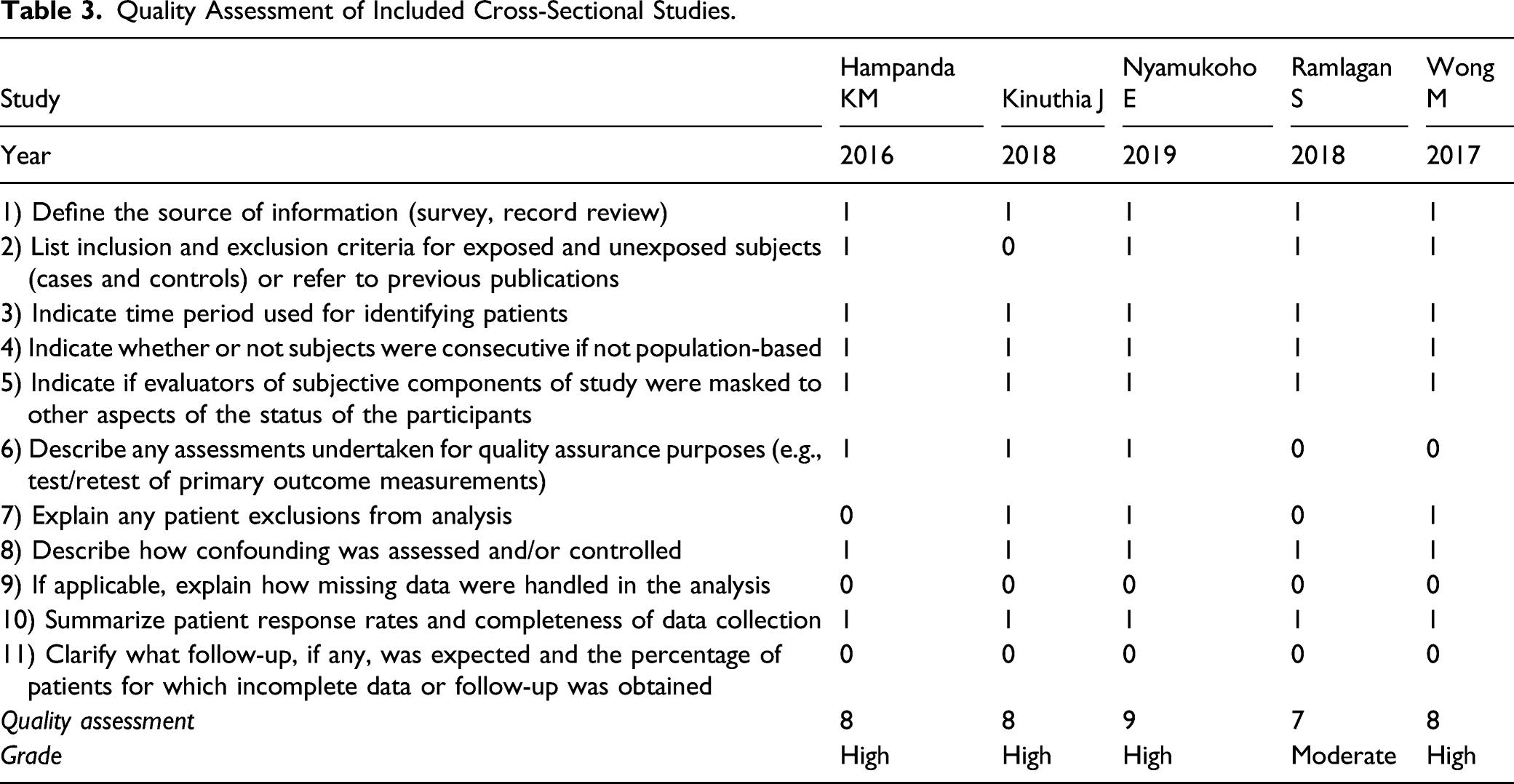
The quality of each included cohort study was assessed by two authors independently using the nine-star Newcastle-Ottawa Scale (NOS) (Margulis et al., 2014). The overall score ranged between zero and nine stars, and we considered a study awarded seven or more stars as a high-quality study. The methodological quality of the cross-sectional studies was assessed using the 11-item checklist recommended by the Agency for Healthcare Research and Quality (AHRQ) from the National Institutes of Health (Ma et al., 2020). We considered a study awarded eight or more stars as a high-quality study (Hu et al., 2015). Any disagreements were resolved via consensus through a discussion.
Data Synthesis and Statistical Analyses
In this study, the quantitative findings were analyzed, and outcomes presented as ORs and their 95% confidence intervals (CIs) were extracted. Crude (unadjusted) or adjusted ORs were used in the pooled meta-analysis calculations. The effect size from a multivariate model was selected when ORs were generated from both univariate and multivariate models. All results were summarized in forest plots that showed the individual OR estimates. Heterogeneity was recognized and was confirmed by the Q test, I 2 statistic, and H statistic. Cochran’s Q test was applied to qualitatively assess the heterogeneity across the studies (Engels et al., 2000). The Q test assessed whether differences in study estimates were due to chance alone, and a Q-statistic value of p < .05 suggested the presence of heterogeneity (Paz-Bailey et al., 2016). The I 2 statistic was used to quantify the heterogeneity and determine the proportion of total variation in the study estimates accounted for by it (Melsen et al., 2014). The results ranged from 0 to 100%, and a larger I 2 indicated that the total variation between studies was due to true heterogeneity rather than sampling error (chance). The interpretation of the amount of heterogeneity was: I 2 from 0% to 40%: might not be important; I 2 from 30% to 60%: may represent moderate heterogeneity; I 2 from 50% to 90%: may represent substantial heterogeneity; I 2 from 75% to 100%: considerable heterogeneity (Higgins, 2019). The H statistic may have quantified heterogeneity in this meta-analysis as it would seem that values that exceeded 1.5 might induce considerable caution, and values below 1.2 caused little concern (Higgins & Thompson, 2002). If the heterogeneity was low, we used fixed-effect models to pool the effect estimates. If the high heterogeneity was clearly identified, a DerSimonian and Laird random-effects model was employed to pool the ORs across the studies, and source exploration was conducted by meta-regression, subgroup analyses, and sensitivity analyses (DerSimonian & Laird, 2015). We used the test of funnel plot asymmetry to examine publication bias if more than ten studies were included in the meta-analysis (Sterne et al., 2011). All analyses were two-tailed, and p-value less than 0.05 indicated statistical significance. All analyses were conducted using Stata version 15.
Results
Literature Search Results and Study Characteristics
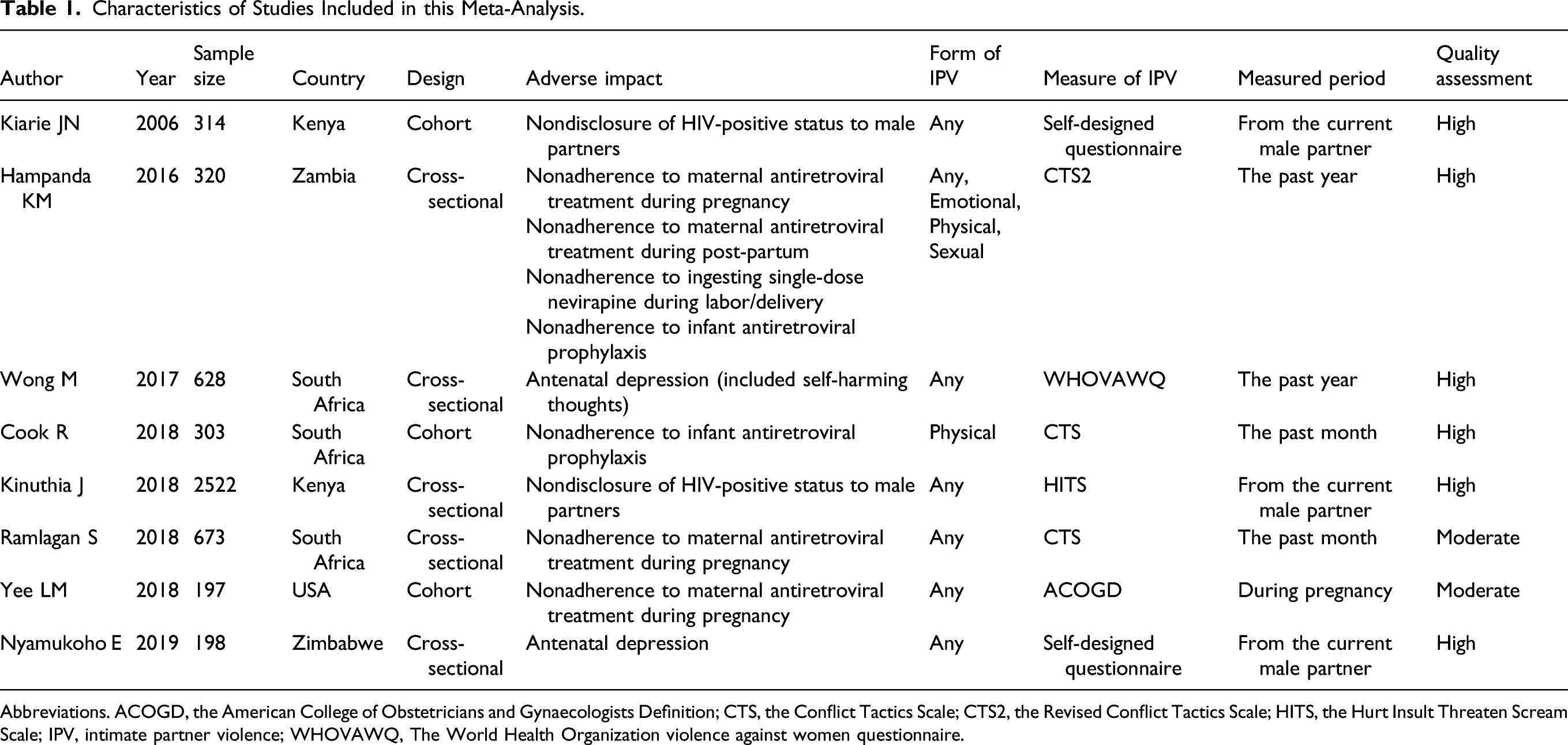
The electronic database and manual search discovered 444 potentially relevant articles, and 327 were excluded after the abstract was screened, which resulted in 117 records for full-text reading. Finally, eight studies that fulfilled the eligibility criteria were included in the meta-analysis (Cook et al., 2018; Hampanda, 2016; Kiarie et al., 2006; Kinuthia et al., 2018; Nyamukoho et al., 2019; Ramlagan et al., 2018; Wong et al., 2017; Yee et al., 2018). The search flow is shown in Figure 1. Overall, three cohort studies and five cross-sectional studies were included. These studies were conducted between 2001 and 2016 in five countries and reported between 2006 and 2019. Most of the studies were conducted in Africa after the 2010s. Many of them recorded any form of IPV and chose the Conflict Tactics Scale to measure it. The measurement periods of IPV were varied, and studies paid attention to IPV against pregnant women from their current male partner (n = 3), during the past year (n = 2), past month (n = 2), and entire gestation period (n = 1). Several direct adverse impacts on pregnant women with HIV linked to IPV were extracted, which included nonadherence to maternal ART during pregnancy (n = 3), nondisclosure of HIV-positive status to partners (n = 2), nonadherence to infant antiretroviral prophylaxis (n = 2), antenatal depression (n = 2), nonadherence to maternal ART during post-partum (n = 1), and nonadherence to ingesting single-dose nevirapine during labor/delivery (n = 1). The characteristics of the eligible studies are presented in Table 1. Flow diagram for searches of databases. Characteristics of Studies Included in this Meta-Analysis. Abbreviations. ACOGD, the American College of Obstetricians and Gynaecologists Definition; CTS, the Conflict Tactics Scale; CTS2, the Revised Conflict Tactics Scale; HITS, the Hurt Insult Threaten Scream Scale; IPV, intimate partner violence; WHOVAWQ, The World Health Organization violence against women questionnaire.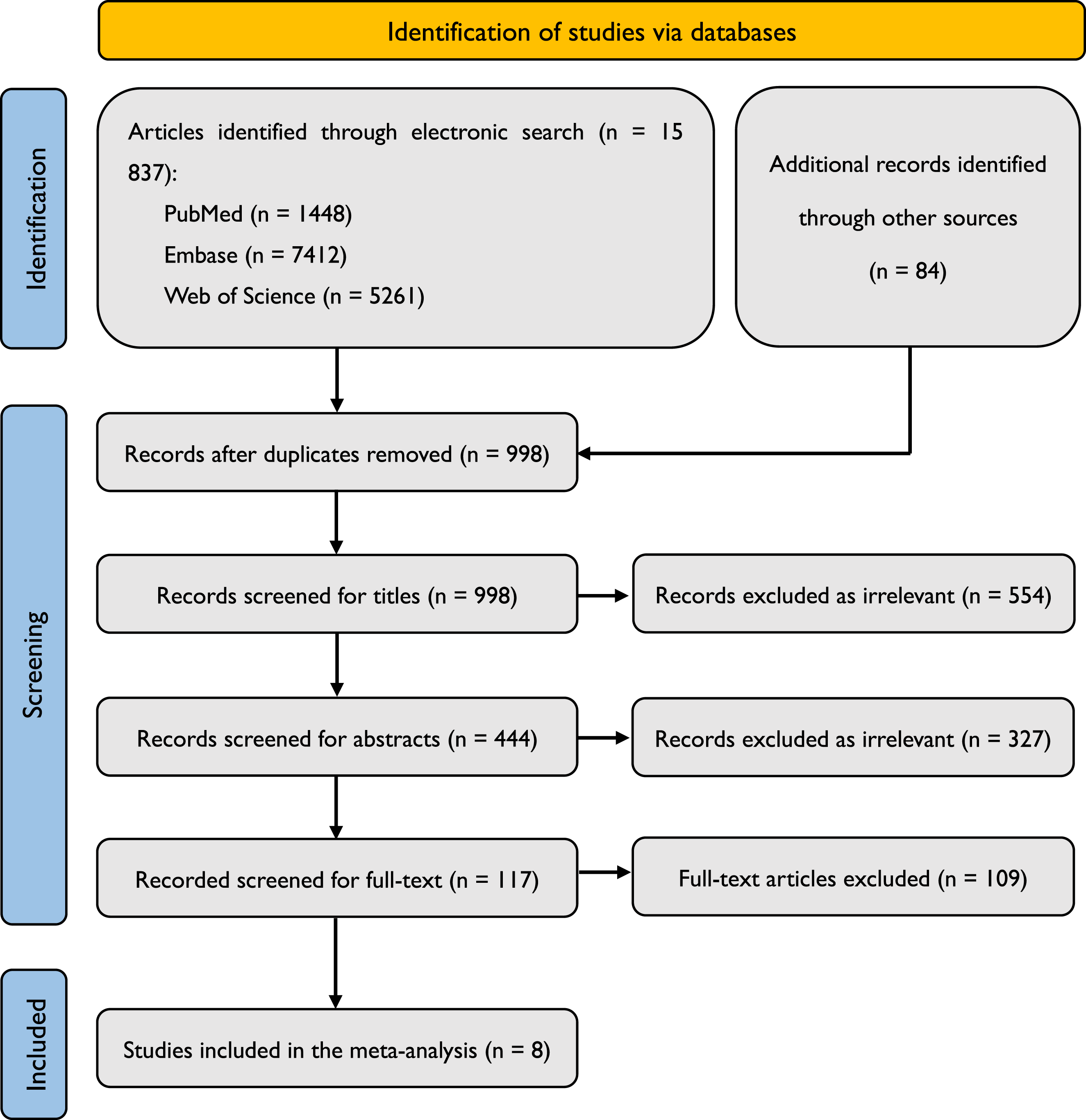
Study Quality
Quality Assessment of Included Cohort Studies.
Quality Assessment of Included Cross-Sectional Studies.
Impacts of IPV against HIV-Positive Women During Pregnancy and Post-Partum
After duplicate data were excluded from different publications, eight studies were selected to examine the impact of IPV against HIV-positive pregnant women. Regarding the impact of nonadherence to maternal ART during pregnancy and nondisclosure of HIV-positive status to male partners, the pooled estimates indicated no higher odds for HIV-positive pregnant women who experienced IPV (OR = 1.48, 95% CI: 0.98–2.22; OR = 1.35, 95% CI: 0.95–1.92). However, for the impacts of antenatal depression and nonadherence to infant antiretroviral prophylaxis, compared to HIV-positive women who did not experience IPV during pregnancy or post-partum, HIV-positive pregnant women who experienced IPV had 180% and 145% higher odds for triggering these adverse outcomes (OR = 2.80, 95% CI: 1.66–4.74; OR = 2.45, 95% CI: 1.40–4.27). The pooled association effect sizes (OR values) with their 95% CIs and those from individual studies are presented in Figure 2. Pooled odds ratio for impacts of intimate partner violence on HIV-positive women during pregnancy and post-partum.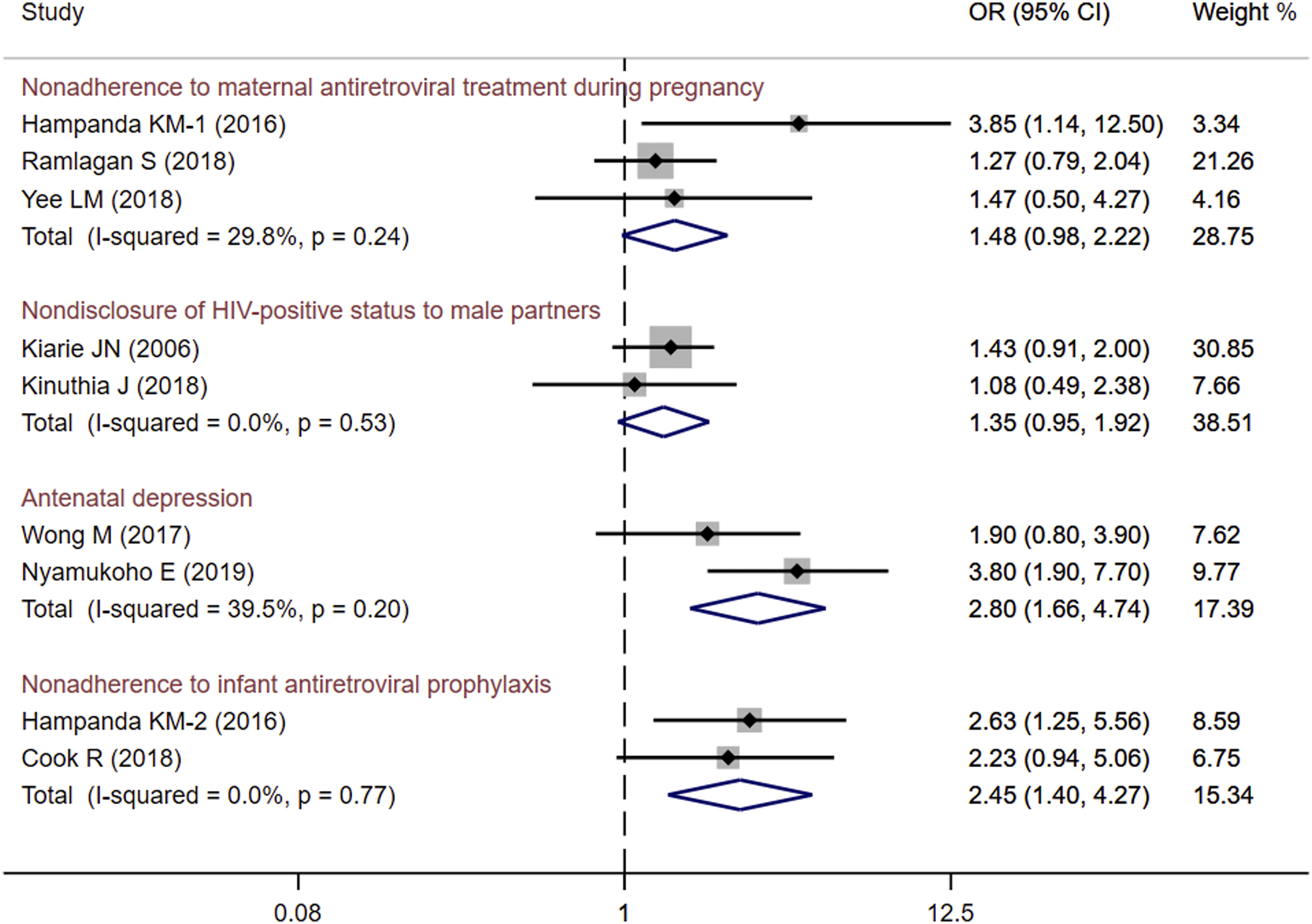
Heterogeneity
All the I 2 values were less than 40% and all the p values of Q were larger than 0.05 in the analysis, indicating insubstantial statistical heterogeneity among studies. All H values were less than 1.5, which also demonstrated lower heterogeneity. Publication bias was not assessed because our analysis did not include more than ten studies. Sensitivity analyses, meta-regression, and subgroup analyses were also waived.
Discussion
HIV-positive pregnant women are at a particularly increased risk of experiencing IPV. Putting aside the established relationship between IPV and adverse pregnancy outcomes, we identified the negative impacts of IPV on HIV-positive pregnant women and their offspring (Doi et al., 2019). Compared with HIV-positive women who never experienced IPV during pregnancy and post-partum, HIV-positive women who experienced IPV faced nearly three times the odds of having antenatal depression, and their infants had about 2.5 times higher odds of PMTCT nonadherence. Regarding the current focus on how social factors influence health, we offer new evidence of an association between the underprivileged group and adverse health outcomes (Kapilashrami et al., 2015). From the meta-analysis, we observed that gender-based violence was a visible social barrier that hampered access to health services in different settings. Therefore, policymakers and healthcare providers are the targeted readers who need to be informed of the pooled data extracted from existing studies involving IPV, HIV, and pregnancy. Although it was not surprising that IPV had negative impacts on PMTCT, ART adherence, HIV status disclosure, or mental balance in HIV-positive pregnant women, no available data supported these cognitions. To the best of our knowledge, this is the first meta-analysis to present a comprehensive synthesis across individual studies on this issue and found strong evidence of the adverse impacts among HIV-positive women exposed to IPV during pregnancy and post-partum.
Our results showed that IPV might increase antenatal depression or thoughts of self-harm in HIV-positive pregnant women. Epidemiologic evidence has suggested that all types of IPV are associated with depression, and the relative risk of depression in female victims of IPV is three times as high as that in non-victims (Bonomi et al., 2009; Mburia-Mwalili et al., 2010). Women who experienced IPV during pregnancy were more prone to score above the threshold for psychological distress, anxiety, and depression, which have been reported to contribute to adverse infant outcomes (Al Qahtani, 2017; Bernstein et al., 2016; Martin et al., 2006; Tsai et al., 2016; Wathen et al., 2018). Depression is common in HIV-positive pregnant women, and higher rates of suicidal ideation have also been reported (Psaros et al., 2009; Rodriguez et al., 2017). Depression, identified as a robust predictor of poor medication adherence or HIV treatment outcomes, also creates difficulties in prenatal care among HIV-positive pregnant women (Sheth et al., 2015). An overlapping situation occurred when HIV-positive pregnant women experienced IPV, which was associated with higher levels of depression and other mental disorders (Matseke et al., 2016; Njim & Mbolingong, 2018). However, we found only two studies have reported antenatal depression caused by IPV among HIV-positive women (Nyamukoho et al., 2019; Wong et al., 2017). Future studies are encouraged to investigate the post-partum depression and long-term psychological disorders caused by IPV against HIV-positive women during and after pregnancy. Our findings also highlight the urgent need to offer diagnosis and treatment of antenatal depression among this vulnerable population, which may have implications for improving prenatal health services.
In our analysis, the infants of HIV-positive mothers who experienced IPV during pregnancy or post-partum showed a nearly 150% increase in nonadherence to antiretroviral prophylaxis, which was a strong predictor of PMTCT failure. All newborns exposed perinatally to HIV should receive post-partum antiretroviral drugs to prevent MTCT (Chi et al., 2013; Little et al., 2017; Takah et al., 2018). The WHO guidelines recommend four-to-six weeks of antiretroviral as postnatal prophylaxis (Beste et al., 2018). If adherence to antiretroviral prophylaxis in infants is high, the risk of vertical transmission of HIV is reduced to less than 5% (World Health Organization, 2010). However, studies on mothers’ adherence to the infant antiretroviral prophylaxis are limited, particularly on very young infants (Desmond et al., 2015). Strikingly, one survey-based study found a significant association between IPV and decreased PMTCT behaviors during and after pregnancy. Their results reported the 91% reduced odds of adherence to infant antiretroviral prophylaxis for HIV-positive IPV survived mothers compared to their IPV-free counterparts (Hampanda, 2016). Poor adherence to infant antiretroviral prophylaxis could lead to drug resistance, treatment failure, and HIV vertical transmission (Haas et al., 2016; Hill et al., 2021; Kirsten et al., 2011; Nachega et al., 2012). Our study identified that women who experienced IPV during pregnancy or post-partum had the higher odds of having poor adherence to HIV prophylaxis for their infants. The finding indicated that eliminating IPV might enhance the adherence to infant prophylaxis and optimize the PMTCT program. Obviously, for HIV-positive women experiencing IPV, additional support such as post-partum adherence counseling is an essential intervention approach to reduce the risk of MTCT.
We did not find any impact of IPV on nonadherence to maternal ART during pregnancy or post-partum and nondisclosure of HIV-positive status to male partners (OR = 1.48, 95% CI: 0.98–2.22; OR = 1.35, 95% CI: 0.95–1.92), which was inconsistent with the results from previous studies. A consensus was given to the priority of treatment adherence due to the disease nature of HIV. For HIV-positive non-pregnant women who experienced IPV, a systematic review that included 13 cross-sectional studies paid attention to the association between IPV and HIV care and treatment engagement. The results showed that IPV was significantly associated with poorer self-reported ART adherence (OR = 0.48, 95% CI: 0.30–0.75) and even lower odds of viral load suppression (OR = 0.64, 95% CI: 0.46–0.90) (Hatcher et al., 2015). Meanwhile, HIV-positive women who reported IPV during pregnancy or post-partum were also more likely to report having missed one or more antiretroviral medication doses, which suggested that IPV was associated with decreased antiretroviral adherence (Yee et al., 2018). However, in our study, the pooled data did not support the link between IPV and maternal ART nonadherence in pregnant women. Nevertheless, the suppressive effect of pregnancy between IPV and maternal nonadherence was questionable since pregnant women may have a strong incentive to achieve virologic suppression to stop HIV transmission to their children.
In high prevalence settings, women test for HIV disproportionately, often during pregnancy, and are expected to disclose status to their sexual partners (Medley et al., 2004; Shamu et al., 2014; Turan et al., 2011). However, decisions about the disclosure of HIV-positive status are often influenced by anticipation. After disclosure to their partners, 85% of the women experienced IPV in some settings, and evidence documented women’s fears of IPV due to status disclosure (Aloyce et al., 2021; Deribe et al., 2010). As a result, nondisclosure to male partners can limit women receiving HIV care, increase the risk for sexual transmission, and increase the likelihood of suboptimal adherence to PMTCT interventions (Desgrees-du-Lou et al., 2009; Jasseron et al., 2013). In contrast, disclosure to and involvement of a male partner in HIV testing was associated with higher adherence to PMTCT and improved infant outcomes (Jasseron et al., 2013; Kiarie et al., 2003; Medley et al., 2004; Peltzer et al., 2010). Subsequently, IPV-related nondisclosure has become one of the barriers to the elimination of MTCT of HIV. However, our synthesized results did not show a negative effect of IPV on nondisclosure. The two original studies that involved IPV during pregnancy and disclosure of HIV status in our analysis were from the same setting (in Kenya), where all parties made great efforts to achieve PMTCT (du Plessis et al., 2014; Mwau et al., 2017; Nduati et al., 2015). We speculated that the HIV-positive women in this setting might have obtained adequate support outside the families and their partners, which attenuated the fear brought about by disclosure-related IPV.
The adverse impact of IPV puts HIV-positive pregnant women at a disadvantage. The dangers inherent in the violence against high-risk pregnancies in HIV-infected women make IPV elimination an urgent priority (Matseke et al., 2016). Our findings call for IPV to be addressed in these women. Enforcing multidimensional interventions that could empower and protect HIV-positive pregnant women against IPV is essential, and the health sector must play a greater role. Scholars note that antenatal care provides an important “window of opportunity” for HIV-positive women exposed to IPV to access health services. However, a comprehensive health response to IPV will likely require either policy support or service implementation, both of which may be acceptable in local clinics in the community (Bacchus et al., 2004; Christofides & Jewkes, 2010; Joyner & Mash, 2012). Since IPV appears to be widespread and in need of immediate action, new clinical and policy guidelines of the health sector’s response to violence against women should be designed to improve the health and social well-being of HIV-positive pregnant women. Also, effective strategies should be designed to support these women during the healthcare services (Ezeanochie et al., 2011). Remarkably, appropriate intervention strategies such as the current PMTCT guidelines, which promote male involvement during the pregnancy to enhance medication adherence and retention in care, may have significant implications for preventing new mother-to-infant HIV transmission. Healthcare providers need to understand the association between exposure to violence and women’s physical and psychological well-being, and medical staffs need to identify women at risk of IPV and respond appropriately. In addition, increased funding for anti-IPV programs may also contribute to IPV elimination among HIV-positive pregnant women (Brooks et al., 2019).
Limitations
Our study has some limitations that need to be considered while interpreting the findings. First, we grouped limited types of adverse health and behavior outcomes and believed that there was a commonality regarding IPV victims owing to overlap in their experience of vulnerability to violence. However, we could not identify a sufficient number of studies performed with this issue (only eight studies in this meta-analysis) and hope that further work will comprehensively describe the IPV experience of HIV-positive pregnant women and the related health outcomes. Second, the representativeness of our analysis is limited for reasons. There was uniformity in the geographical distribution of the included studies. Seven studies were from Africa and one from the USA, which resulted in an unequal weighting of the pooled estimates and made it impossible to generalize our findings to HIV-positive pregnant IPV victims in specific contexts or generally resource-rich settings. Third, although we confirmed that the subjects investigated in Africa were from different research projects, most studies were based on the same program (Protect Your Family), suggesting duplicated data and overly narrow CIs. Fourth, a reporting bias may have been introduced by the methods used to measure IPV. Five types of questionnaires or scales were used in the eight studies included in our analysis. Although they were all standard methods for collecting IPV information, their significance cannot be accurately measured without a universal standard. Furthermore, a considerable proportion of the observed heterogeneity might be explained by differences in the forms of IPV, measure periods, and study designs. The forms of IPV were different in the studies, and the measured period ranged from one month to one year or more. The absence of universal definitions of the forms and time frames for measuring IPV was likely to explain some of the variations, although it was small. Lastly, although the multivariate logistic regression analyses in the included studies controlled for many important confounders, such as age, race, education, and employment status, there was a possibility of residual confounding due to the presence of unknown confounders or imprecise adjustment strategies (Aibibula et al., 2017).
Conclusion
We synthesized and analyzed the available data from studies designed to capture HIV-positive pregnant women’s experiences of IPV and highlighted the adverse impacts during pregnancy and post-partum. IPV puts pregnancy complicated by HIV at risk, caused psychological distresses in pregnant women, and blocks PMTCT prevention. Our findings have implications for medical and social services for this disadvantaged group. There is a clear need to enhance efforts across various sectors to prevent IPV occurrences and provide necessary help for HIV-positive pregnant women experiencing IPV.
Critical Findings
●Limited studies were concerned about IPV against HIV-positive pregnant women. In our meta-analysis, only two out of eight included studies mainly focused on this issue. ●Antenatal depression was one of the adverse impacts of IPV against HIV-positive women during pregnancy. Compared with HIV-positive women who never experienced IPV during pregnancy, HIV-positive women who experienced IPV faced nearly three times the odds of having antenatal depression or thoughts of self-harm. ●Nonadherence to infant antiretroviral prophylaxis was also associated with IPV during pregnancy or post-partum for HIV-positive women. The infants of HIV-positive mothers who experienced IPV had about 2.5 times higher odds of antiretroviral prophylaxis nonadherence than their IPV-free counterparts. Nonadherence could accelerate the mother-to-child transmission of HIV. ●Our study found no evidence for an increased risk in nonadherence to maternal antiretroviral treatment during pregnancy or nondisclosure of HIV-positive status to male partners among these pregnant women. Although data from our results could not identify the significance, these two adverse impacts are suggested to be listed in the background information used for policy development against IPV.
Recommendations and Implications for Practice, Policy, and Research
● IPV should be addressed in both HIV infection and pregnancy for women. IPV identification and support services should be incorporated into routine care for HIV-infected pregnant women. ● The adverse impacts of IPV during pregnancy and post-partum on the long-term maternal and child health outcomes in the context of HIV infection require further research attention. ● Routine screening to identify victims of IPV who are at risk of depression should be integrated into antenatal care or service of HIV. ● Focused attention should be paid to the nonadherence to infant antiretroviral prophylaxis caused by IPV. Necessary support specifically for HIV-positive women in the postnatal period may lead to more optimal adherence. ● Almost all the studies were conducted in Africa, where the prevalence of HIV has reached epidemic proportions, and HIV-positive pregnant women are not the minority group. In other regions or countries, however, as members of a minority group, HIV-positive pregnant women who experience IPV may face more challenges other than the adverse impacts mentioned in our meta-analysis. These women are more helpless. Therefore, it is suggested that special investigations should be carried out worldwide to understand what these women suffer from IPV and prepare for protection policymaking. ● Future studies are encouraged to analyze IPV in different forms (emotional, physical, or sexual) since the current literature on HIV-positive pregnant women rarely reports the impacts on a specific form.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors disclosed that funding was received from the Key Discipline Program of the Fifth Round of the Three-Year Public Health Action Plan (2020–2022 Year) of Shanghai (GWV-10.1-XK08).