
Abstract
Throughout the last two decades, research on poly-victimization (PV) has evolved from examinations of a core set of past-year victimization types in youth samples to investigations of a broad range of victimization types experienced during variable time intervals in diverse samples of varying ages. As the concept of PV expands, greater clarity regarding the definition and measurement of PV is needed to advance understanding of its risk and protective factors as well as its associated outcomes. This scoping review aimed to (a) identify approaches used to operationally define and measure PV across studies and (b) synthesize empirical findings concerning risk factors and outcomes associated with PV. A systematic search of peer-reviewed research published before 2022 across 12 databases yielded 98 studies that met inclusion criteria. Study characteristics including the research design, sample type, victimization timeframe, operational definition(s) of PV, measurement of PV, analytic methods, and key findings were synthesized across studies. Findings indicated that the majority of reviewed studies were cross-sectional investigations that utilized categorical measures of lifetime PV in samples of youth. Results also demonstrated that PV is robustly associated with a broad range of predictors, including mental health symptoms and diagnoses as well as family- and community-level factors. PV is also associated with numerous adverse outcomes including depression, anxiety, suicidality, substance use, and delinquency across diverse study types and populations. Future research that examines the conditional effects of PV is needed to identify subgroups of individuals at higher risk of adverse outcomes following PV and modifiable targets for interventions.
Empirical studies concerning the impact of violence and victimization on psychological health and psychosocial functioning are consistent in showing that exposure to violence and victimization is associated with a wide range of negative outcomes, including depression (e.g., Andrews et al., 2015), anxiety (e.g., Charak et al., 2019), posttraumatic stress (e.g., Ayer et al., 2019), substance use (e.g., Davis et al., 2020), and suicidality (e.g., Ford et al., 2018). However, the majority of research on victimization has focused on outcomes linked to a single victimization type, such as sexual assault, bullying, or intimate partner violence (IPV). Given that individuals who report exposure to violence and victimization are likely to experience more than one type of victimization during their lifetime (Finkelhor, Ormrod, & Turner, 2009) as well as exposure across multiple settings (i.e., home, school, and in the broader community; Butcher et al., 2016; Finkelhor, Ormrod, et al., 2009), studies that examine single categories of victimization likely underestimate the full burden of individuals’ victimization histories. Furthermore, studies that examine the effects of victimization based on assessments of single victimization types may overestimate the impact of particular types on survivor outcomes and bias findings concerning individual-difference factors associated with elevated risk of adverse outcomes. Conclusions about the effects of victimization drawn from studies that fail to assess individuals’ exposure to a broad spectrum of victimization types may also misguide the development of interventions designed to prevent or reduce the negative consequences of victimization.
To address these concerns, scholars across multiple disciplines have begun to investigate the cumulative impact of exposure to multiple types of victimization experiences. Finkelhor et al. introduced the term “poly-victimization (PV)” in 2005 based on research showing that youth exposed to multiple types of victimization exhibit more severe negative outcomes compared to youth who experience one victimization type (Finkelhor, Ormrod, et al., 2005) as well as youth who experience repeated exposure to the same type of victimization (Finkelhor et al., 2007b). Results consistent with these findings have since emerged in research on clinical and nonclinical samples of poly-victims of varying ages (i.e., children, adolescents, adults) and backgrounds (e.g., incarcerated women, Radatz & Wright, 2017; foster care youth, Schneiderman et al., 2013) as well as across diverse fields of study, including criminology, psychology, public health, social work, and sociology.
As research on PV has advanced, how PV has been operationally defined and measured has likewise expanded. In Finkelhor, Ormrod et al.’s (2005) seminal study, poly-victims were defined as youth who experienced four or more different types of lifetime or past-year victimizations that occurred during separate incidents. An additional distinction was made between low PV (four to six types) and high PV (six or more types) subgroups among poly-victims. In subsequent research, alternative a priori approaches to operationally defining PV have been used, including exposure to specific numbers of victimization types (e.g., four or more types; Cuevas et al., 2009) and percentile thresholds (e.g., participants in the top 10% of the sample; Finkelhor, Ormrod, & Turner 2009). Various methods of weighting victimization types for severity and chronicity have also been used to account for differences in incident severity and repeated exposure to a single victimization type among poly-victims (e.g., Finkelhor et al., 2007a; Finkelhor, Ormrod, & Turner, 2009).
In contrast to these a priori variable-centered approaches to operationally defining PV, several recent studies have used empirically driven person-centered methods, including latent class analysis (LCA) and latent profile analysis (LPA). These methods identify homogeneous classes or subgroups of participants within a sample that have similar patterns of exposure to victimization types. Studies that use person-centered methods of defining PV indicate the particular types of victimization that tend to co-occur, which may advance understanding of the phenomenology of PV and facilitate efforts to identify individuals in greatest need of prevention and intervention efforts.
Given the substantial variability in how PV has been defined in research across a broad range of disciplines, a review of the existing literature is needed. Accordingly, we conducted a scoping review of peer-reviewed studies on PV to summarize how PV has been operationally defined and measured throughout behavioral science and medical research and to synthesize empirical findings concerning risk factors and outcomes associated with PV. Current gaps in the literature were also identified.
Method
Search Strategy
A systematic search of peer-reviewed research journals was conducted by a university social science librarian. The following databases were searched for articles published between January 1, 2000 and October 22, 2021: ERIC on ProQuest, National Criminal Justice Reference Service, Social Services Abstracts on ProQuest, Web of Science, Sociological Abstracts on ProQuest, PsycInfo on Ebscohost, EbscoHost Academic Search Complete, Criminal Justice Abstracts on Ebscohost, PubMed, and PILOTS: Published International Literature On Traumatic Stress on ProQuest. Titles, abstracts, and subjects were searched using the following terms: (measure* OR define* OR definition* OR defining OR assess* OR diagnos*) AND (polyvictimi* OR “poly-victimization” OR “poly-victimisation” OR “poly-victimised” OR “poly-victim”). Duplicates (n = 918) were first omitted from the initial 1,420 identified articles. Authors then reviewed the abstracts of the remaining 502 articles and eliminated 377 that did not meet the following inclusion criteria: (a) empirical research; (b) quantitative study; (c) published in a peer-reviewed journal; (d) the intent to examine PV as an independent variable (IV), dependent variable (DV), or mediator was stated in the article title or abstract; and (e) examined a U.S. sample. The full texts of the remaining 125 articles were reviewed, and 27 were excluded due to the following reasons: (a) duplicate articles (n = 2); (b) non-U.S. sample (n = 4); (c) PV was not an IV, DV, or mediator (n = 20); and (d) not available in English (n = 1). Figure 1 summarizes the search process.

PRISMA flow diagram.
For the remaining 98 unique articles, the following categories of information were extracted and are summarized in Table 1: author(s) and publication year; youth or adult sample; victimization timeframe; operational definition(s) of PV and variable type; PV measure; PV variable type (IV, DV, or mediator); and analysis type. To ensure consistency between authors who screened articles for inclusion eligibility and extracted key study characteristics, 10 articles were randomly selected and reviewed by two co-authors each (five authors total). The agreement of inclusion eligibility decisions between authors was 100%. Agreement of key study characteristics reported in Table 1 was 96% (67/70). Differences were discussed among all reviewing authors until reconciled. The remaining 88 articles were reviewed by four authors.
Key Characteristics of Reviewed Studies
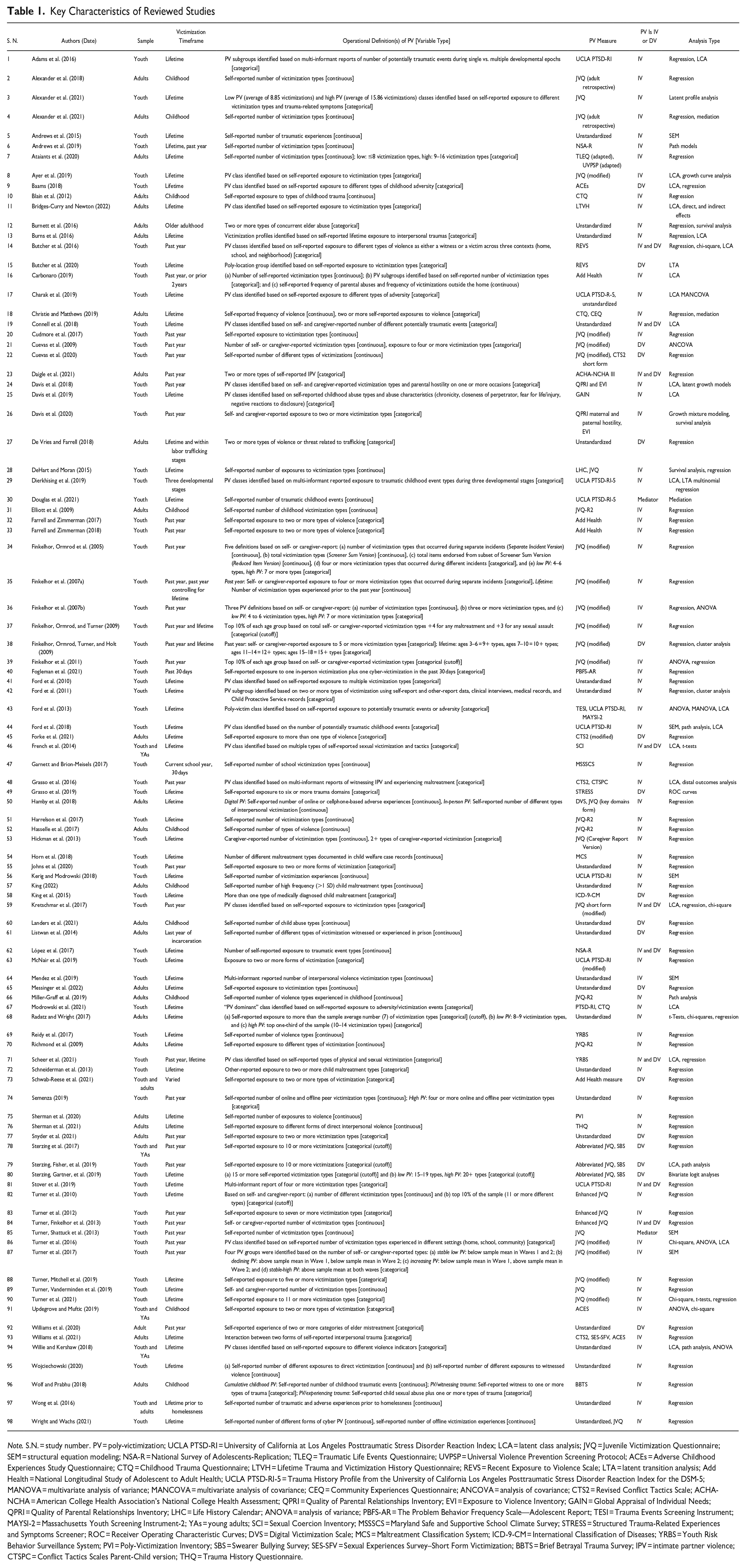
Note. S.N. = study number. PV = poly-victimization; UCLA PTSD-RI = University of California at Los Angeles Posttraumatic Stress Disorder Reaction Index; LCA = latent class analysis; JVQ = Juvenile Victimization Questionnaire; SEM = structural equation modeling; NSA-R = National Survey of Adolescents-Replication; TLEQ = Traumatic Life Events Questionnaire; UVPSP = Universal Violence Prevention Screening Protocol; ACEs = Adverse Childhood Experiences Study Questionnaire; CTQ = Childhood Trauma Questionnaire; LTVH = Lifetime Trauma and Victimization History Questionnaire; REVS = Recent Exposure to Violence Scale; LTA = latent transition analysis; Add Health = National Longitudinal Study of Adolescent to Adult Health; UCLA PTSD-RI-5 = Trauma History Profile from the University of California Los Angeles Posttraumatic Stress Disorder Reaction Index for the DSM-5; MANOVA = multivariate analysis of variance; MANCOVA = multivariate analysis of covariance; CEQ = Community Experiences Questionnaire; ANCOVA = analysis of covariance; CTS2 = Revised Conflict Tactics Scale; ACHA-NCHA = American College Health Association’s National College Health Assessment; QPRI = Quality of Parental Relationships Inventory; EVI = Exposure to Violence Inventory; GAIN = Global Appraisal of Individual Needs; QPRI = Quality of Parental Relationships Inventory; LHC = Life History Calendar; ANOVA = analysis of variance; PBFS-AR = The Problem Behavior Frequency Scale—Adolescent Report; TESI = Trauma Events Screening Instrument; MAYSI-2 = Massachusetts Youth Screening Instrument-2; YAs = young adults; SCI = Sexual Coercion Inventory; MSSSCS = Maryland Safe and Supportive School Climate Survey; STRESS = Structured Trauma-Related Experiences and Symptoms Screener; ROC = Receiver Operating Characteristic Curves; DVS = Digital Victimization Scale; MCS = Maltreatment Classification System; ICD-9-CM = International Classification of Diseases; YRBS = Youth Risk Behavior Surveillance System; PVI = Poly-Victimization Inventory; SBS = Swearer Bullying Survey; SES-SFV = Sexual Experiences Survey–Short Form Victimization; BBTS = Brief Betrayal Trauma Survey; IPV = intimate partner violence; CTSPC = Conflict Tactics Scales Parent-Child version; THQ = Trauma History Questionnaire.
Findings
Research Design of Reviewed Studies
The majority of studies (n = 82) were cross-sectional. The remaining 16 studies were longitudinal (S6, S8, S12, S15, S22, S26, S32, S33, S35, S38, S64, S73, S83, S87, S95, and S98). Several studies analyzed cross-sectional data derived from longitudinal datasets (e.g., S24, S29).
Research Questions
Most studies (n = 69) examined PV as an IV to test its impact on or association with aspects of survivors’ psychosocial functioning, health, or behavior. The majority (n = 64) of these studies examined mental health outcomes, including trauma symptoms (S37, S39, S53, S82, S86, S88, S89, S90, S91, and S96). Other common outcomes included delinquency (S20, S28, S41, S56, S62, S64, and S90) and criminal behavior (S16, S28, S32, S33, and S51). Another set of studies (n = 18) examined PV as a DV in relation to risk factors or correlates, such as demographic characteristics, including race (S60), sexual and gender minority status (S9, S61, S65, S73, S77, S78, S80, and S92), family and environmental factors (S38 and S78), and mental health symptoms or disorders (S21 and S77). In addition, nine studies examined PV as both an independent and a DV (S14, S19, S23, S46, S59, S62, S71, S81, and S84). An analysis of data from the National Survey of Children’s Exposure to Violence (NatSCEV) examined PV as a mediator of the association between community disorder and distress symptoms (S85), and another study examined PV as a mediator of the association between race/ethnicity and posttraumatic stress symptoms (S30). Protective factors for PV, such as social support (S61) and religiosity (S78), were also examined.
Samples
The majority of studies (n = 65) examined youth under age 18. Six studies examined youth and adults ages 18 and older. The remaining 27 examined adults only. Nationally representative samples were examined in 27 studies (S5, S6, S13, S16, S21, S32, S33, S34, S35, S36, S37, S38, S39, S41, S55, S62, S71, S73, S82, S83, S84, S85, S86, S87, S89, S90, and S92). Of these, nine analyzed data from the NatSCEV (S39, S82, S83, S84, S85, S86, S87, S89, and S90). Single-gender samples were common, with 12 studies examining females only (S2, S7, S18, S28, S31, S67, S68, S70, S71, S75, S76, and S77) and 6 males only (S3, S4, S10, S13, S51, and S61). Thirteen studies (S14, S17, S26, S28, S43, S44, S49, S56, S61, S63, S67, S68, and S95) examined justice-involved populations. Other studies examined samples from particular sub-populations or ethnicities, including undergraduates (S2, S4, S11, S18, S23, S31, S45, S46, S52, S66, and S77), gender minority populations (S10, S65, S75, S76, S78, and S79), older adults (S12), foster care youth (S54, S60, and S72), and Latinos (S20 and S22).
Respondent Type
Victimization experiences were primarily documented via self-report. In studies examining children, the cutoff age for self-report was typically 10 years old (i.e., studies that analyzed NatSCEV data, studies that administered the Juvenile Victimization Questionnaire [JVQ, Finkelhor, Hamby et al., 2005]), but occasionally a different threshold was selected (e.g., S21). When the sample included only young children, caregivers typically reported youth victimization histories. A few studies combined self- and/or caregiver-report data with administrative (e.g., Child Protective Services records) or clinical data (S1, S18, S28, S42, S64, and S81), whereas other studies exclusively utilized administrative data or clinical data (S12, S25, S54, and S72). Medical diagnostic codes were exclusively used in one study (S58).
Mode
Phone interviews were a common (n = 20) mode of data collection and used in several studies of nationally representative samples, including the Developmental Victimization Survey (S21, S34, S35, S36, S37, and S38), NatSCEV (S39, S82, S83, S86, S87, S84, S85, and S90), the National Survey of Adolescents (S41), the National Survey of Adolescents-Replication (NSA-R) Study (S5, S6, and S62), and the National Elder Mistreatment Study (S92). Surveys (i.e., researcher- or clinician-administered, online, and paper formats, n = 45), in-person interviews (n = 10), computer-assisted interviews (n = 4), or a combination (n = 12) of methodologies were also used. Several studies used data drawn from administrative, clinical, or health records (S1, S12, S25, S27, S54, S58, and S72).
Operational Definitions of PV and Measurement
All reviewed studies broadly defined PV as self- or other-reported exposure to different types of victimization, potentially traumatic events, abuse/maltreatment, trauma, or adversities. Using this definition as a foundation, studies then varied with respect to the following dimensions of PV: victimization types, victimization timeframe, PV variable types (IV, DV, or mediator), co-occurring victimization types, and victimization severity.
Victimization Types
The victimization types examined in each study were typically determined by the measure used to assess victimization exposure. Many studies (n = 10) measured PV using the original (Finkelhor, Hamby, et al., 2005) or revised JVQ (JVQ-R2), which assesses 34 types of victimization categorized into five domains: conventional crime, child maltreatment, peer and sibling victimization, sexual victimization, and witnessing and indirect victimization. Several studies utilized alternative or modified versions of the JVQ (n = 25) including an adult retrospective version (S2 and S4), an adolescent/caregiver version (S53), abbreviated versions (S50, S59, and S78–S80), and an enhanced version (S82, S83, and S84).
Other standardized measures of victimization included the Recent Exposure to Violence Scale (Singer et al., 1999; S14, S15), the Exposure to Violence Inventory (Selner-O’Hagan et al., 1998; S26, S24), the Universal Violence Prevention Screening Protocol (Dutton et al., 1996; S7), the Maltreatment Classification System (Barnett et al., 1993; S54), the Sexual Coercion Inventory (Waldner et al., 1999; S46), the Problem Behavior Frequency Scale (Farrell et al., 2018; S40), and the Conflict Tactics Scale (Straus, 1979; S22, S45, S48, and S93). Trauma-focused victimization measures included the Traumatic Experiences Screening Instrument (Ford et al., 2000; S43), the Trauma History Questionnaire (Hooper et al., 2011; S76), the Childhood Trauma Questionnaire (Bernstein & Fink, 1998; S10, S18, and S67), the Trauma History Profile from the UCLA Posttraumatic Stress Disorder-Reaction Index (UCLA PTSD-RI; Steinberg et al., 2004) or the revised UCLA PTSD-RI-5 (S1, S17, S29, S30, S43, S44, S56, S63, S67, and S81), the Traumatic Life Events Questionnaire (Kubany et al., 2000; S7), the Brief Betrayal Trauma Survey (Goldberg & Freyd, 2006; S96), and the Lifetime Trauma and Victimization History Questionnaire (Widom et al., 2005; S11). Several studies used measures designed to assess general adversity, such as the Adverse Childhood Experiences Study Questionnaire (Felitti et al., 1998; S9, S91, and S93), or a specific type of childhood adversity, such as bullying (S78–S80). A few studies measured PV using medical diagnostic codes (S58) or behavioral health screening instruments, such as the Global Appraisal of Individual Needs (S25), the Massachusetts Youth Screening Instrument (S43), and questions from the Youth Risk Behavior Surveillance System (S71). In addition, many studies assessed individuals’ history of violence or traumatic events using measures that are not specific to victimization, such as the Life History Calendar (Freedman et al., 1988; S28) and the Community Experiences Survey (Schwartz & Proctor, 2000; S18).
Among studies that did not utilize standardized measures to assess victimization (n = 21), most examined a broad range of victimization types. Others focused on specific types of victimization, including childhood maltreatment (S57, S60, and S72), elder abuse (S12), IPV types (S23), violence witnessed or experienced in prison (S61), and online victimization (S98). Two studies used both standardized and unstandardized measures to assess PV (S7 and S17).
Victimization Timeframe
Most studies examined either lifetime PV (n = 53) or past-year PV (n = 27). Ten studies on adults examined childhood PV. A few studies (S6, S37, and S38) measured both lifetime and shorter victimization timeframes and compared their relative impact. Other victimization timeframes included the last 2 years (S22), the last 30 days (S40 and S47), the last 12 months of incarceration (S61), the current school year (S47), and older adulthood (S12).
In studies that define PV as lifetime exposure to different types of victimization, age is a potential confounding variable given that older respondents have had more time to be exposed to victimization than younger respondents. The role of victim age is further complicated by results showing that after young adulthood the likelihood of violent victimization in a given year decreases (see Garofalo, 1979). The potential confounding role of respondent age has been addressed in several ways in research on PV. In particular, age is often used as a control variable in multivariate statistical models. Alternatively, many studies limit samples to specific age groups, such as childhood and adolescence (n = 65) or older adulthood (S12). Other strategies included testing separate statistical models for different age groups (S34, S35, and S36), tracking age of onset (S28 and S38), defining PV as respondents with more than the top 10% of total victimizations within their age group (S37, S39, and S82), and measuring PV at multiple points throughout the lifespan (S98).
PV Variable Types
Most studies (n = 54) analyzed a categorical PV variable. Of those, many used categories selected a priori based on prior research (e.g., S34) or an a priori selected cutoff. For example, in a few studies, the number of victimization types experienced by respondents was assessed and individuals with scores in the top 10% of the sample (or each age group) were categorized as poly-victimized (S37, S39, and S82). Another set of studies categorized individuals who experienced greater or fewer victimization types than a selected threshold into high PV and low PV groups (S3, S7, S34, S36, S68, and S80). Others defined PV (S35, S36, and S68) or high PV (S7) as more than the sample average number of victimization types. In contrast, S39 and S68 categorized participants with scores in the top one-third of the sample as high PV. One study identified stable-low, increasing, decreasing, and stable-high PV subgroups by comparing the number of victimization types endorsed at two time points (S87).
A large minority (n = 33) of studies utilized a continuous PV variable defined as the total number of victimization types experienced. Eleven studies (S7, S16, S18, S21, S34, S35, S36, S53, S74, S82, and S96) analyzed PV as both a continuous and a categorical variable. Among this group, several (S16, S34, S35, S53, and S96) examined differences between models that tested categorical and continuous PV variables.
Finally, approximately one-quarter of the reviewed studies (n = 25) examined one or more PV profiles using LCA (S1, S8, S9, S11, S13, S14, S16, S17, S19, S24, S25, S29, S41, S43, S44, S46, S48, S59, S67, S71, S86, and S94), LPA (S3), cluster analysis (S42), or latent transition analysis (S15) to identify homogeneous classes or subgroups of participants within a sample who had similar patterns of exposure to various types of victimization. S43 identified latent classes based on the number of victimization types and categorized participants into high, moderate, and low levels of victimization. The setting or context of the victimization, such as home, school, community, or poly-location, defined subgroups in several studies (S14, S15, S16, and S86). Other studies defined subgroups according to the developmental timing of the victimizations (S1, S13, and S29).
Co-occurring Victimization Types and Severity Weighting
Although most studies did not specify how the potential co-occurrence of victimization types was accounted for in their definition of PV, a few (S20, S32, S33, S34, S35, S38, and S59) explicitly required different victimization types to occur on separate occasions. For example, S34 and S35 used the Separate Incident Version of the JVQ which includes questions to determine the number of victimizations that occurred at different times and places. Victimization types were weighted for severity prior to the construction of the PV variable in three studies (S35, S37, and S80).
Empirical Findings
Impact of PV
Despite the substantial variability in how PV is operationally defined throughout the literature, results are relatively consistent in showing that PV is a robust predictor of adverse outcomes. The majority of both cross-sectional and longitudinal studies found a linear relationship between PV and greater symptom severity, number of symptoms, or frequency of problematic behavior. Furthermore, this pattern of results was reported for a broad spectrum of psychological health variables, including depression (S5, S11, S17, S19, S31, S34, S40, S44, S48, S57, S63, S70, S75, S96, and S97), anxiety (S11, S17, S31, S34, S40, S44, S48, S50, S57, S70, and S96), substance use/abuse (S1, S7, S17, S24, S25, S26, S28, S31, S32, S33, S43, S44, S63, S64, S67, S68, S76, S93, and S95), PTSD (S1, S3, S5, S6, S8, S11, S13, S17. S19, S30, S43, S48, S50, S63, S66, S67, S75, and S97), suicidality (S1, S2, S17, S31, S43, S44, S55, S67, S68, and S83), and emotion dysregulation (S11, S17, S43, S57, and S70); sexual risk behaviors (S2, S46, S67, and S94); as well as delinquency (S20, S28, S41, S56, S62, S64, and S90) and criminal behavior (S16, S28, S32, S33, and S51). This observed relationship between PV and negative outcomes was also generally consistent across studies that analyzed continuous measures of PV and in studies that used categorical measures in which poly-victims were compared to single-victimized individuals and/or individuals with histories of no victimization. Studies that utilized empirically driven methods of defining PV (e.g., LCA, LPA) also generally found that poly-victimized subgroups within their samples exhibited higher levels of negative outcomes compared to less victimized and/or non-victimized subgroups. In contrast, results from the few studies that examined physical health outcomes associated with PV revealed mixed findings regarding the negative physical health consequences of PV, such as high body mass index (BMI) (S18 and S72) and mortality (S12).
Risk Factors for PV
Despite the wide range of risk factors examined across the reviewed studies, results were relatively consistent in showing that mental health-related predictors, including PTSD (S78 and S81), eating disorders (S77), psychiatric diagnoses broadly defined (S21 and S81), and internalizing and externalizing behaviors (S14 and S81); social predictors, including peer rejection (S78) and membership in sororities and fraternities (S77); family-related predictors, including residential instability (S84), family problems (S38), parental conflict (S84), and family or maternal history of mental illness (S14, S15, and S84); school-related predictors, such as school climate (S78); and indices of community danger (S38) and disorder (S84), are associated with higher levels or greater odds of PV. Only two studies (S61 and S77) found that PV was not significantly associated with the hypothesized risk factors, including higher BMI, learning disabilities, physical disabilities, drug use, gang affiliation, and treatment participation. Of the few studies that examined protective factors, social support (S22, S61, and S92) and religiosity (S78) were found to be negatively associated with PV or associated with lower risk.
Mediators and Moderators of PV
Although relatively few studies (n = 13) examined the processes through which PV leads to negative outcomes, a broad spectrum of potential explanatory mechanisms were tested, including emotion dysregulation (S11, S24, and S79), posttraumatic stress (S64 and S79), insecure caregiver attachment (S51), executive functioning (S54), and social support (S87). All studies reported evidence of mediation except S18 and S54. Contrary to study hypotheses, no evidence was found to support the role of cortisol as a mediator of the association between PV and BMI (S18). Similarly, executive functioning did not mediate the association between PV and externalizing problems in S54.
Four studies (S5, S30, S62, and S85) examined PV as a mediator. Analyses of NSA-R data (S5) indicated that PV mediated differences in mental health symptoms between ethnicity groups, such that mental health disparities between Hispanic and White youth and between non-Hispanic Black youth and White youth were explained by higher levels of PV among the ethnic minority groups. Similarly, in a separate analysis of NSA-R data (S62), PV accounted for ethnic disparities in delinquency, PTSD symptoms, and depression symptoms. Analyses of NatSCEV data indicated that PV mediated the association between community disorder and symptoms of distress (S85). Finally, among bereaved youth, the association between race and elevated posttraumatic stress was mediated by higher PV (S30).
The reviewed studies also included several investigations of potential moderators of the association between PV and psychological health and psychosocial functioning (S5, S20, S54, S55, S62, S69, S75, and S98) or the association between a predictor variable and PV (S73). Information about the conditional effects of PV yielded by moderation studies may help to identify intervention targets as well as subgroups at higher risk of adverse outcomes following victimization. The majority of studies that tested moderators reported results that can be used to advance these goals (S5, S54, S55, S62, S69, and S98). S5 reported that the association between PV and poor mental health was stronger in youth from low-income families compared to youth from moderate-to-high income families. Similarly, PV was more strongly associated with sexual and injury perpetration among boys compared to girls, and among younger compared to older youth in S69. In a nationally representative sample of adolescents (S62), PV was more strongly associated with delinquent behavior in non-Hispanic White compared to Hispanic youth, but no evidence of moderation was found for PTSD symptoms, substance use, or depression symptoms. In S55, the associations between suicide risk and PV varied by sexual minority status, such that sexual minority youth with histories of PV had higher odds of suicide risk behaviors compared to heterosexual youth with histories of PV. Similarly, PV was related to externalizing problems among children with low executive functioning scores, but not among children with high executive functioning scores in S54. Finally, among middle school students (S98), parental social support moderated the associations between cyber PV and academic outcomes (e.g., school readiness, academic performance, absenteeism).
An additional four studies reported nonsignificant results from tests of moderation. In S20, no evidence was found to indicate social support moderated the relation between PV and hostility. Similarly, neither age nor gender moderated the association between PV and sexual or injury victimization in S69. Gender also did not moderate the association between sexual orientation and PV in S73. Finally, in a sample of transgender and gender-diverse adults (S75), the association between PV and depression was not moderated by community connection.
Discussion
Throughout the last two decades, research on PV has expanded from a focus on a core set of past-year victimization types assessed by the JVQ in samples of youth to investigations of a broad range of victimization types experienced during variable time intervals in diverse study populations. As the concept of PV continues to evolve, greater clarity with respect to the definition and measurement of PV is needed to advance understanding of its prevalence, risk and protective factors, associated outcomes, and effective interventions. The goals of this scoping review were to identify the approaches used to operationally define and measure PV in extant research and to summarize empirical findings concerning risk factors and outcomes associated with PV. Our findings indicate that the majority of studies were cross-sectional investigations that utilized categorical measures of lifetime PV in samples of youth. In addition, despite substantial diversity in research designs, study populations, and measurement methods, our results indicate that PV is robustly associated with a broad range of predictor variables, including mental health symptoms and diagnoses as well as family- and community-related factors. PV is also robustly associated with numerous adverse outcomes including depression, anxiety, suicidality, substance use, and delinquency. Although very few studies reported nonsignificant findings for hypothesized risk factors or outcomes, divergent or inconsistent results across studies can likely be attributed to variability in the operation definitions of PV used in prior studies, which ranged from continuous variables indexing the total number of victimization types experienced during a given timeframe, categorical variables that divided samples into groups, and person-centered methods that identify latent groups of poly-victims relative to individuals exposed to no or low levels of victimization.
The reviewed studies also used a diverse array of methods to assess PV, including tailored versions of the JVQ (Finkelhor, Hamby, et al., 2005) and other victimization questionnaires, as well as standardized and unstandardized measures of trauma exposure, adversity, and behavioral health. Given that the victimization types examined in a study are largely determined by the measure used to assess PV, the wide range of measurement methods employed in the reviewed studies limits the ability to compare results across studies. This variability may also pose challenges to clinical decision-making regarding screening and treatment. To advance the field in identifying the optimal method of measuring PV, more research is needed that compares methods used to assess and define PV in diverse samples. In particular, studies that compare measurement methods as well as continuous and categorical definitions of PV may yield critical information regarding the relative explanatory power of different definitions and measures of PV in relation to outcomes that can be used to inform intervention efforts.
Another dimension of PV along which studies varied is the temporal co-occurrence of victimization types. Although most studies do not specify whether the definition of PV required victimization types to occur on separate occasions, some studies identified victimization types (e.g., rape and robbery) that occurred at the same time and place as PV while others did not. In addition, some victimization measures conceptualize victimization types that typically involve a combination of victimization experiences (e.g., sexual assault and physical abuse during an incident of IPV) as a single victimization type, which may underestimate exposure to PV among violence victims.
Methods of accounting for and defining victimization severity also varied across studies. In addition, studies rarely developed criteria for assessing or weighting the severity of victimization types before construction of the PV variable which can be problematic. For example, when severity is exclusively based on the number of victimizations, an individual who experienced multiple types of theft (e.g., on person, in home, from vehicle) could be categorized as having higher levels of PV than an individual exposed to repeated sexual abuse. Multiple experiences of the same type of severe victimization (e.g., sexual abuse) may also be obscured in PV definitions that index the number of victimization types without accounting for event severity and chronicity. Operational definitions that index the number of victimization types, incident severity, and chronicity may better capture individuals’ lived experience of victimization compared to those that assess only the total number of victimization types.
Despite the rapid growth in research on PV throughout the last two decades, our review revealed several gaps in the existing research (Table 2). First, very few investigations employed longitudinal research designs. Additional longitudinal research is warranted given the potential for the impact of PV to change over time and for individuals to experience more victimization types with age. Longitudinal data also have the potential to yield critical insight into factors that promote acute versus long-term consequences of PV as well as greater understanding of the conditional effects of PV when examined using moderation analyses. Second, relatively few studies to date have examined factors that modify the adverse effects of PV on psychological health and well-being. Additional research on potential moderators of the influence of PV on a range of outcomes is needed to identify targets for intervention efforts that seek to prevent future victimization and promote recovery in affected populations. In addition, the field is dominated by studies of risk factors for PV with less attention paid to protective factors. Intervention studies are also scarce. Given the prevalence of PV and the wide range of associated negative consequences, the field would benefit from greater understanding of protective factors and effective interventions that reduce the risk of future victimization, minimize the immediate and long-term negative effects of PV, and promote resilience in poly-survivors. In general, this work may be especially beneficial for minority and oppressed groups who are overrepresented among violence survivors.
Implications of Research on PV.
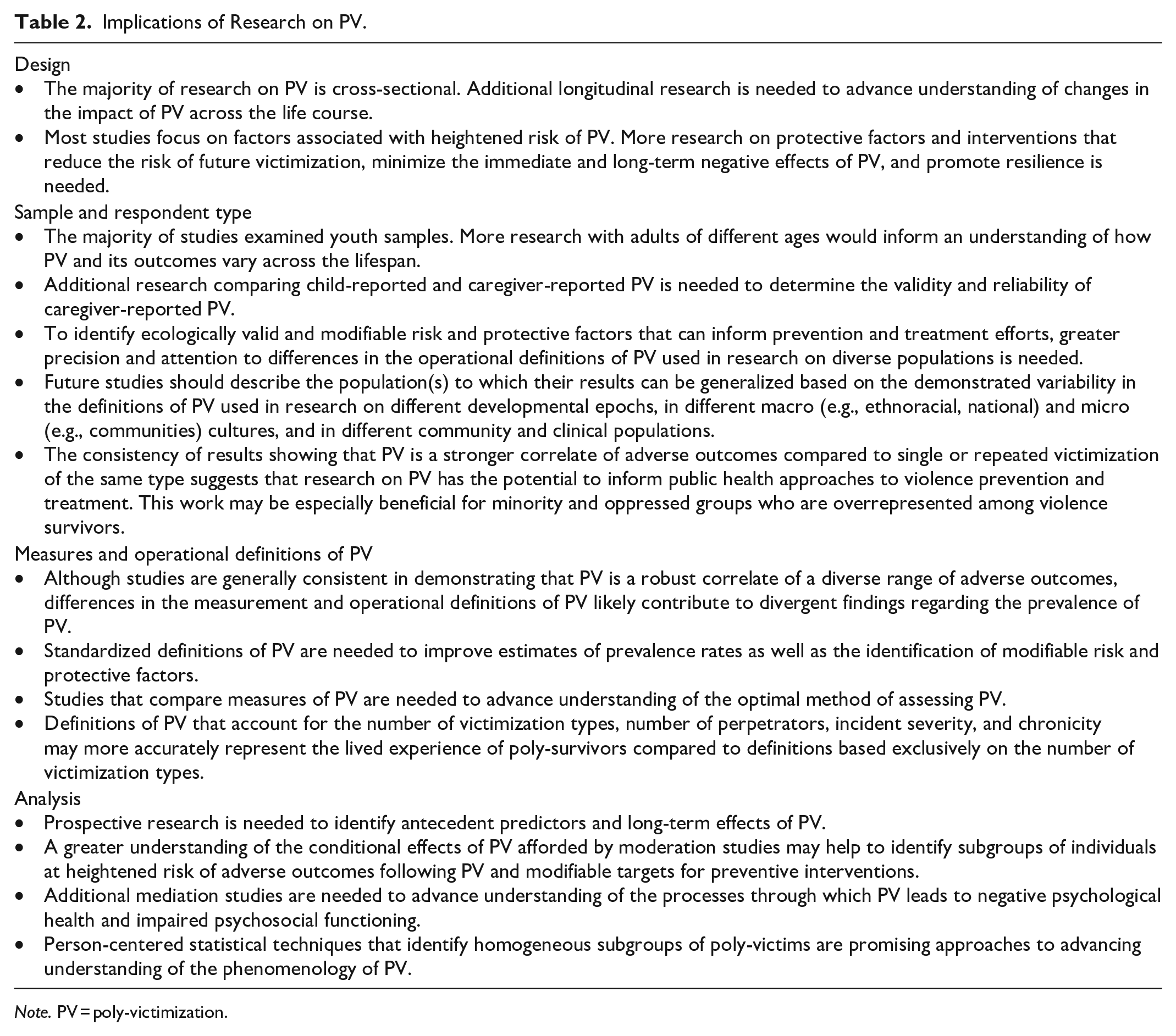
Note. PV = poly-victimization.
Research on changes in the impact of PV across the lifespan is another critical gap in the literature. The majority of reviewed studies examined youth under age 18, which advances understanding of risk factors and outcomes associated with PV during childhood and adolescence, but not differences in the predictors and consequences of PV across the life course. Furthermore, in studies on youth samples, youths’ PV history is typically reported by parents which may impact accuracy. Additional research comparing child-reported and caregiver-reported PV is needed to determine the validity and reliability of caregiver-reported PV. In addition, similar to victimization research in general, many studies included in our review are characterized by dual validity challenges wherein residential samples are not representative of the general population because they are more victimized by definition, and community samples often include healthier individuals who are better able or motivated to discuss traumatic experiences (Schneider, 1981). Investigations of PV in national and large-scale population-based studies could address these limitations of the existing research.
In addition, few studies used measures of PV that assessed the victim’s relationship to the perpetrator (see S38) or victimization in multiple contexts (see S14) which may index victimization perpetrated by different individuals (e.g., adults, peers). As a result, understanding of how PV outcomes are differentially influenced by the victim’s relationship to the perpetrator and by experiences with multiple versus single perpetrators remains limited. Future work should focus on measurement methods that address these issues without overburdening respondents.
Although this is a wide-ranging review of research on PV, several features of the review should be noted as they may limit the generalizability of the findings. First, studies on constructs that are similar to PV, such as cumulative trauma exposure, multiple victimization, and repeated victimization, were not included because these studies typically assess victimization as well as other types of traumatic but non-victimization events, such as disasters and bereavement. Similarly, studies that expand the concept of PV from individual victims to victimized groups (e.g., family PV) were outside the scope of our review. Future reviews of these areas of study may further inform understanding of co-occurring victimization and potentially traumatic events. In addition, comparisons of PV assessment methods and definitions in relation to prevalence estimates and associated outcomes were beyond the goals of this study but would be useful extensions of this review. Finally, due to cross-national differences in legal definitions and cultural perceptions of violence and victimization, our study was limited to research on U.S. samples. Future research comparing U.S. and international samples is needed to determine the generalizability of our results.
In conclusion, the construct of PV is critical to advancing understanding of the impact of victimization on health and well-being across the lifespan and to improving outcomes for victims. Rather than placing victimization types in research, practice, and policy silos, survivors may be better served by a holistic approach that accounts for cumulative exposure to victimization across the life course, as such an approach is likely to represent a more accurate picture of a survivor’s lived experience of victimization. Funding structures must also advance to better support integrated research, services, and intervention efforts to meet the needs of poly-survivors. Additional longitudinal studies, studies on adult samples, and studies on moderators of PV as well as associated protective factors are needed to address current gaps in the literature. Together these lines of research have the potential to inform public health approaches to violence prevention as well as interventions and treatments to improve outcomes in poly-victims.
Footnotes
Authors’ Note
The opinions and assertions expressed herein are those of the author(s) and do not reflect the official policy or position of the Uniformed Services University of the Health Sciences or the Department of Defense. The contents of this publication are the sole responsibility of the author(s) and do not necessarily reflect the views, opinions, or policies of The Henry M. Jackson Foundation for the Advancement of Military Medicine, Inc. Mention of trade names, commercial products, or organizations does not imply endorsement by the U.S. Government.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.