
Abstract
Refugees within the post-migration context experience higher rates of mental health symptoms due to a variety of pre- and post-migration factors. However, there is a lack of research in understanding best practices in culturally grounded interventions aimed at improving well-being outcomes. Recent research shows group interventions are a potential pathway to mental health treatment for refugees. This systematic review aimed to (1) assess best practices among group-based interventions within the refugee context, (2) provide literature-informed guidance on best practices within group-based interventions for this population, and (3) examine the impact of group-based interventions on the mental health outcomes of adult refugees in the post-migration context in high-income countries. A systematic literature search was conducted using Academic Search Complete, Social Work Abstracts, and PsycINFO. A total of 2,243 studies were identified, with 19 meeting the inclusion criteria to be from a peer-reviewed journal article; be published from 2003 to 2023; be written in English; have a study population of refugees in the post-resettlement context in a high-income country; include a group-based intervention model; and be quantitative or mixed methods. Results demonstrated that group-based interventions improve mental health symptoms, including post-traumatic stress disorder, depression, and anxiety. Studies varied on their use of culturally grounded mechanisms in developing and implementing interventions. Future research is needed to understand the longitudinal impacts of group-based interventions on mental health and better support current practices to facilitate access to intervention implementation.
Keywords
Globally, the number of displaced persons at the end of 2022 was estimated to be 108.4 million—the highest number in recorded history (UNHCR, 2023). Refugees experience elevated levels of trauma pre-migration and myriad resettlement challenges in the post-migration context (Porter & Haslam, 2005), leaving refugees, including those in high-income settings, with increased mental health needs (Blackmore et al., 2020; Henkelmann et al., 2020). Trauma experiences among refugees and other displaced persons are high and include war exposure, torture, sexual violence, and forced family separation (Steel et al., 2009). Recent studies have also found that refugees experience high levels of violence post-resettlement, including gun violence and sexual assault, which may impact their mental health more than pre-migration trauma (Salhi et al., 2021). There is evidence that refugees resettled in high-income countries have higher violence exposure from both pre- and post-migration experiences than comparison groups (Scoglio & Salhi, 2021). Additionally, refugee communities experience elevated levels of collective trauma, including loss of land and culture, colonization, and genocide (Kirsch et al., 2024; Jorden et al., 2009; Magan et al., 2023; Somasundaram, 2010). Researchers have identified elevated prevalence rates of anxiety, depression, and post-traumatic stress disorder (PTSD) among refugees in both the pre- and post-migration contexts (Blackmore et al., 2020; Fazel et al., 2005; Henkelmann et al., 2020). These traumatic experiences and critical mental health needs impact refugees’ ability to be successful and productive members after they are resettled in high-income countries.
Despite the prevalence of unmet mental health needs, multiple systematic and cultural barriers have led to lower mental health service utilization rates among refugee populations living in high-income countries (Satinsky et al., 2019). One of the most significant gaps in research pertaining to refugee mental health is the lack of evidence-based, culturally tailored interventions to support these individuals and communities (Poudel-Tandukar et al., 2019). Mental health interventions among refugees have traditionally focused on individualized clinical treatment options. This approach fails to address the complex barriers and daily stressors refugees face post-resettlement, as well as their cultural differences from Western society (Im et al., 2021). For example, traditional talk therapies and clinical treatments target mental illness and trauma from an individualistic cultural perspective rather than the culturally specific ways trauma may present itself within different populations (Kronick, 2018). Integrating refugees’ cultural understandings of their current distress and the best way to heal are critical factors for social workers and other mental health professionals to use within any therapeutic intervention with this population. Further, this current lack of cultural integration in available mental health services may help explain the low levels of mental health service utilization among refugees, as they may not see these clinical interventions fitting their current needs. This mismatch leads to a lack of engagement and participation in currently available services (Shannon et al., 2015).
Therefore, culturally grounded group-based interventions may be a solution to use with refugee populations in the post-migration context in high-income countries. Researchers have increasingly emphasized the importance of developing and implementing interventions with the cultural context of target populations in mind (Fennig, 2021; Filler et al., 2021; McCleary & Horn, 2023). Studies indicate that culturally adapted interventions are more effective than un-adapted ones (Griner & Smith, 2006). Horn and McCleary (2022) note in a scoping review exploring the cultural adaptation of interventions for refugee populations that the current level of intervention adaptations varies widely. Further, this variation remains true, even when there is a strong documented need for mental health interventions grounded in the community’s cultural background.
Group therapy modalities have a long history of successful treatment for those with complex trauma (Mahoney et al., 2019; Schwartze et al., 2019; Sloan et al., 2012) and may offer benefits that individual therapy cannot, such as decreased isolation (Esplen et al., 2004) and peer support (Goubert et al., 2011). Successful use of group-based intervention in other populations includes veterans (Cox et al., 2014; King et al., 2013), survivors of intimate partner violence (Crespo et al., 2021), and those with suicidal ideation (Chalker et al., 2023). Refugees have also expressed a desire and preference to receive mental health treatment in a group setting (Kirsch, 2023; Mitschke et al., 2017). A meta-analysis of various mental health interventions among asylum seekers and refugees demonstrates the effectiveness of group-based interventions among asylum seekers and refugees (Turrini et al., 2021). Similarly, there is evidence that group-based interventions positively address mental health symptoms among refugee children (Rafieifar & Macgowan, 2022). Small et al. (2016) compared individual therapy delivered in office and home settings and a group therapy approach across multiple refugee groups in the United States, with findings revealing group therapy modalities to be the most effective in treating mental health concerns. In a review of mental health interventions among refugee populations in the United States, Peterson et al. (2020) highlighted the growing prevalence of group therapy modalities among refugees. They underscored the alignment of these modalities with refugee cultures and their effectiveness in addressing mental health issues. Bunn et al. (2018) observed a recent increase in utilization of group modalities among torture survivors and identified their potential to address a range of treatment issues that individual therapies possess. Given the extensive evidence supporting the effectiveness and cultural alignment of group intervention modalities in addressing mental health concerns among diverse refugee groups, a systematic review of the literature focused on such interventions is needed. To our knowledge, no systematic review exists that examines the impact of group-based interventions on refugee adults in high-income countries.
The Current Study
While knowledge supporting group-based interventions among refugee populations exists, there is no published systematic review of the literature to aid in understanding recent findings and current best practices. This systematic review seeks to assess best practices among group-based interventions within the refugee context and provide literature-informed guidance on best practices for this population. Second, the study aims to examine the impact of group-based interventions on the mental health outcomes of adult refugees in the post-migration context. Three key research questions guided this systematic review: (1) How are group interventions conducted among refugee populations? (2) What cultural considerations are being implemented for group interventions among refugee populations? and (3) How do group interventions impact refugee mental health? By carefully examining these questions, we can uncover insights into the current understanding of group-based interventions for this population and the impact they have on improving the well-being of refugee populations.
Methods
Eligibility Criteria
To meet inclusion criteria, an article needed to (1) be from a peer-reviewed journal article; (2) be published from 2003 to 2023; (3) be written in English; (4) have a study population of refugees in the post-resettlement context in a high-income country; (5) include a group-based intervention model; and (6) be quantitative in its analyses including mixed methods studies. We excluded articles if they (1) were published outside of 2003–2023; (2) were not written in English; (3) did not focus on refugees post-resettlement; (4) did not include a group-based intervention model; (5) took place pre-resettlement; (6) were conceptual or focused on program description without empirical analyses; and (7) used solely qualitative methods. We operationalized the term “refugee” in accordance with the definition provided by the United Nations High Commissioner for Refugees (UNHCR), as articulated in the 1951 Refugee Convention, which delineates a refugee as an individual unable or unwilling to return to their country of origin due to a substantiated fear of persecution based on factors such as race, religion, nationality, membership in a specific social group, or political opinion (UNHCR, 2023). We made the decision to narrow our search to post-migration in high-income countries due to the extensive differences in available resources and needs of refugees in differing contexts. Our date range was decided on due to preliminary searches showing no relevant data earlier than the chosen date range. Additionally, we decided to investigate only studies in high-income countries due to the immense differences in resourcing and the needs of refugee populations in high versus low-income countries.
Search Strategy
The first author conducted a comprehensive search of relevant databases, including Academic Search Complete, Social Work Abstracts, and PsycINFO, and completed the search for relevant articles in August 2023. The search included the following terms, used in a variety of combinations to produce relevant articles: (“refugees” OR “migra*”) AND (“group-based” OR “group intervention” OR “group therapy” OR “social support group” OR “ground counseling”).
Selection and Data Collection Process
Three research team members used Covidence (2023), a streamlined platform for conducting systematic reviews, to review and synthesize all articles. As shown in Figure 1, we identified and imported an initial 2,243 articles, and Covidence removed 260 duplicates. The review team completed two rounds of review to assess the eligibility and inclusion of each article. We held weekly meetings to discuss disagreements and reach consensus. First, we completed a title and abstract review, resulting in 1,983 articles deemed eligible for full-text review. Upon completing the full-text review, we excluded 1,907, leaving 76 for further consideration. A total of 19 articles met our inclusion criteria and were included in the review.
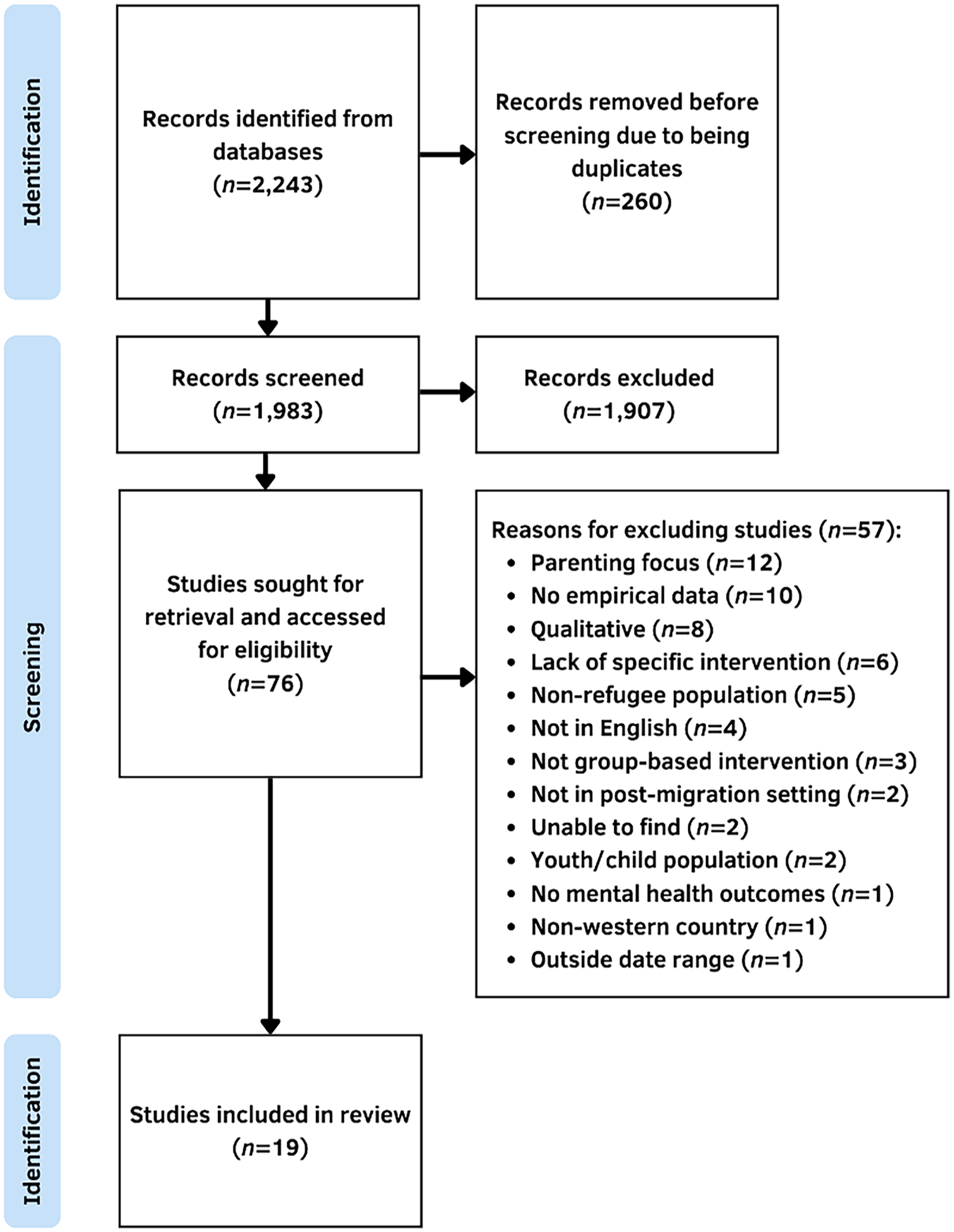
Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) flowchart.
Risk of Bias Assessment
We implemented the Methodological Index for Non-Randomized Studies (MINORS) in conducting our systematic review, focusing on its first eight criteria tailored for non-comparative studies. This robust tool, developed by Slim et al. (2003), enabled a thorough assessment of study design and reporting quality. The criteria range from 0 (not reported) to 2 (reported and adequate), covering aspects from study aims to follow-up. The first two authors conducted the evaluations, and a high Cronbach’s alpha (α = .96) confirmed their inter-rater reliability, indicating a strong consensus in their assessments.
Results
Studies took place in multiple resettlement countries including two in the United Kingdom (Bahu, 2019; Griggs et al., 2022), two in Australia (Bernardi et al., 2019; Blignault et al., 2021), three in the Netherlands (Drožđek & Bolwerk, 2010; Drožđek et al., 2012, 2014), five in the United States (Haefner et al., 2019; Han et al., 2012; Mazzulla et al., 2021; Mitschke et al., 2013; Shaw et al., 2022), three in Germany (Kananian et al., 2017, 2020; Lehnung et al., 2017), one in Norway (Hasha et al., 2022), one in Denmark (Husby et al., 2020), one in Austria (Renner et al., 2021). Additionally, one study took place in multiple countries (Purgato et al., 2021). Participants’ country of origin also varied greatly, with participants from Sri Lanka, Burma (Myanmar), Iraq, Lebanon, Syria, Libya, Iran, Afghanistan, Nepal, Cambodia, Palestine, Somalia, Bhutan, Nigeria, Pakistan, Russia, and the Democratic Republic of Congo. Year of publication ranged from 2010 through 2022. Study design also varied with most studies using a pre-post-intervention design (Bahu, 2019; Bernardi et al., 2019; Blignault et al., 2021; Drožđek & Bolwerk, 2010; Griggs et al., 2022; Haefner et al., 2019; Han et al., 2012; Husby et al., 2020; Kananian et al., 2017; Mazzulla et al., 2021; Shaw et al., 2022). Other study designs included controlled comparison cohort (Drožđek et al., 2014), longitudinal (Drožđek et al., 2012), waitlist control group design (Lehnung et al., 2017), quasi-experimental (Mitschke et al., 2013), and randomized controlled trial (RCT; Hasha et al., 2022; Kananian et al., 2020; Purgato et al., 2021; Renner et al., 2011). Sample sizes varied, with the smallest being 7 participants (Bernardi et al., 2019) and the largest being 459 participants (Purgato et al., 2021). There were two separate groups of studies that used the same intervention. The Den Bosch method, an intensive day treatment group, was the topic of three of the studies (Drožđek & Bolwerk, 2010; Droždek et al., 2012, 2014). Two studies described a Culturally Adapted Cognitive Behavioral Therapy (CA-CBT) group intervention (Kananian et al., 2017, 2020).
Intervention Features
Reasoning for Group Modality
About half the articles stated a reason for choosing a group versus individual-level intervention. The main reasons provided were cultural adaptation and the desire to increase social connections among participants. For example, Drožđek and Bolwerk (2010) stated that the group modality mitigates the impact of interpersonal trauma experienced by refugee groups. Many described the benefit of increasing social connectedness (Kananian et al., 2017, 2020; Shaw et al., 2022) and how important this was for refugees who come from a collectivist culture (Bernardi et al., 2019; Haefner et al., 2019; Mitschke et al., 2013). Beyond cultural aspects, several articles also described the logistical benefits of group therapy, including increasing access to mental health services (Husby et al., 2020), reducing economic costs for agencies and providers (Kananian et al., 2017), and increasing scalability of interventions in the population (Kananian et al., 2020).
Group Participant Demographics
The age of participants ranged from 16 to 70 years old. Most study participants were middle-aged, with the range of mean ages being 22.1 (Kananian et al., 2020) to 54 years (Han et al., 2012) and the most common mean age being 32 (Bahu, 2019; Lehnung et al., 2017; Purgato et al., 2021). Three studies did not report age (Haefner et al., 2019; Husby et al., 2020; Mazzulla et al., 2021). Most studies did not report length of stay. However, among those that did, one study reported all participants to have arrived within the last 12 months (Mitschke et al., 2013), and another reported that all participants arrived in the previous 2 years (Shaw et al., 2022). Other studies reported average lengths ranging from 6 (Bernardi et al., 2019) to 25.6 years (Renner et al., 2011).
Finally, the mental health diagnoses of participants varied. Participants were not required to have a formal diagnosis in six studies (Blignault et al., 2021; Husby et al., 2020; Lehnung et al., 2017; Mitschke et al., 2013; Renner et al., 2011; Shaw et al., 2022), while 10 studies included participants based on having a formal diagnosis (Bahu, 2019; Bernardi et al., 2019; Droždek et al., 2012, 2014; Haefner et al., 2019; Han et al., 2012; Hasha et al., 2022; Kananian et al., 2017, 2020; Purgato et al., 2021). Two studies based inclusion on mental health symptoms rather than a formal diagnosis (Griggs et al., 2022; Hasha et al., 2022; Mazzulla et al., 2021; Purgato et al., 2021). Inclusion diagnoses and symptoms varied and included PTSD (Bernardi et al., 2019; Drožđek & Bolwerk, 2010; Droždek et al., 2012, 2014; Haefner et al., 2019; Kananian et al., 2017, 2020), traumatic symptoms/stressors (Hasha et al., 2022; Mazzulla et al., 2021) and anxiety (Kananian et al., 2017). One study determined inclusion based on a collaborative decision by providers, who assessed whether participants’ symptoms indicated a better fit for individual or group therapy (Bahu, 2019).
Intervention Logistics
Group size varied across studies. The largest group included 230 participants (Purgato et al., 2021), and the smallest group comprised seven (Bernardi et al., 2019; Kananian et al., 2017). The most common group size was 18 (Lehnung et al., 2017; Mazzulla et al., 2021). Most groups used a closed structure where new members were not able to join once sessions began (Drožđek & Bolwerk, 2010; Droždek et al., 2012, 2014; Hasha et al., 2022; Husby et al., 2020; Kananian et al., 2020; Lehnung et al., 2017; Mazzulla et al., 2021; Mitschke et al., 2013; Purgato et al., 2021; Renner et al., 2011; Shaw et al., 2022). Three studies used an open group structure (Bahu, 2019; Blignault et al., 2021; Haefner et al., 2019). Additionally, some studies did not specify if the group was open or closed (Bernardi et al., 2019; Griggs et al., 2022; Haefner et al., 2019; Han et al., 2012; Kananian et al., 2017). Studies using a closed-group format where researchers could measure the intervention dose varied drastically. Three studies described the highest dose intervention using the Den Bosch method, where participants received a total of 85 group therapy sessions lasting 90 min each over 1 year (Drožđek & Bolwerk, 2010; Droždek et al., 2012, 2014). The smallest dose was an eye-movement desensitization and reprocessing group traumatic episode protocol (EMDR G-TEP) intervention that was given in two sessions lasting 2 hr each (Lehnung et al., 2017). The most common number of sessions was 12, and the most common length of sessions was 90 min to 2 hr.
In most studies, participants did not receive other treatment besides the group intervention (Bernardi et al., 2019; Drožđek & Bolwerk, 2010; Droždek et al., 2012, 2014; Griggs et al., 2022; Hasha et al., 2022; Kananian et al., 2017, 2020; Mitschke et al., 2013). However, some studies stated that clients were also receiving individual treatment (Blignault et al., 2021; Haefner et al., 2019; Han et al., 2012), medication management (Haefner et al., 2019; Han et al., 2012), and/or crisis/secondary care support (Bahu, 2019). One study used a mobile application (Mazzulla et al., 2021), and two studies used pre-recorded audio recordings (Blingnault et al., 2021; Purgato et al., 2021) in conjunction with group therapy. Two studies did not specify if participants received additional treatment (Husby et al., 2020; Renner et al., 2011).
Therapeutic Modalities
Studies varied in the use of formal therapeutic modalities. The most common modalities were CBT (Drožđek & Bolwerk, 2010; Droždek et al., 2012, 2014; Griggs et al., 2022; Haefner et al., 2019; Hasha et al., 2022; Renner et al., 2011) and CA-CBT (Bahu, 2019; Kananian et al., 2017, 2020; Shaw et al., 2022). Other modalities included mindfulness (Blignault et al., 2021; Haefner et al., 2019), psychodynamic (Drožđek & Bolwerk, 2010; Droždek et al., 2012, 2014), modified family therapy (Han et al., 2012), CPT (Bernardi et al., 2019; Han et al., 2012), EMDR G-TEP (Lehnung et al., 2017), acceptance and commitment therapy (Purgato et al., 2021), and Culture-sensitive and Resource Oriented Peer (Renner et al., 2011). Additionally, one study did not specify a specific modality (Mitschke et al., 2013). Most studies used only one modality, while some used a mix (Bernardi et al., 2019; Drožđek & Bolwerk, 2010; Droždek et al., 2012, 2014; Haefner et al., 2019; Han et al., 2012; Renner et al., 2011). Several studies also stated they used psychoeducation as either the only form of intervention (Husby et al., 2020) or in conjunction with another modality (Bahu, 2019; Bernardi et al., 2019; Drožđek & Bolwerk, 2010; Droždek et al., 2012, 2014; Griggs et al., 2022; Haefner et al., 2019; Kananian et al., 2017, 2020; Lehnung et al., 2017).
Cultural Considerations
Intervention Development
The studies incorporated cultural considerations to varying degrees with considerable variability. While some studies provided little or no information on how the intervention was developed or adapted for the culture of the study population, others provided extensive detail. Most interventions used community members to create or adapt the intervention specifically for refugee communities (Bahu, 2019; Blignault et al., 2021; Han et al., 2012; Hasha et al., 2022; Husby et al., 2020; Kananian et al., 2017, 2020; Mazzulla et al., 2021; Mitschke et al., 2013; Shaw et al., 2022). However, among those who did, the level and processes varied widely. For example, Blignault et al. (2021) culturally adapted a previously developed mindfulness intervention. They noted that content underwent a primary review for translation and language interpretation by bilingual staff members, with changes made to a specific section to enhance “cultural and spiritual relevance” (p. 8233). Conversely, Bahu (2019) extensively described their “bottom up” approach and the community’s co-creation of the intervention. They stated that “the community itself holds experience and solutions to some difficult obstacles” (p. 6) and incorporated those concepts throughout the intervention.
Group Participant Gender and Ethnicity
Numerous studies indicated that cultural adaptation involved uniform gender and ethnic groups. There were 5 studies with mixed-gender groups (Bahu, 2019; Haefner et al., 2019; Han et al., 2012; Lehnung et al., 2017; Purgato et al., 2021), 12 studies with single-gender groups (Bernardi et al., 2019; Blignault et al., 2021; Drožđek & Bolwerk, 2010; Droždek et al., 2012, 2014; Griggs et al., 2022; Hasha et al., 2022; Kananian et al., 2017, 2020; Mazzulla et al., 2021; Mitschke et al., 2013; Renner et al., 2011), two studies that used both single- and mixed-gender groups (Husby et al., 2020; Shaw et al., 2022), and one study that did not specify (Griggs et al., 2022). Several studies with single-gender groups pointed to cultural reasons and suggestions from community members as to why they decided on single-gender groups (Blignault et al., 2021; Hasha et al., 2022; Kananian et al., 2017, 2020; Mitschke et al., 2013). Six studies indicated their groups consisted of only one ethnic group (Bahu, 2019; Bernardi et al., 2019; Han et al., 2012; Hasha et al., 2022; Mitschke et al., 2013; Renner et al., 2011). All others reported mixed ethnicity groups. Similar to gender, homogenous groups pointed to cultural differences among refugees as the reason for limiting groups to one ethnicity (Bahu, 2019; Han et al., 2012; Mitschke et al., 2013). Additionally, some studies grouped participants based on shared language rather than ethnicity (Bahu, 2019; Blignault et al., 2021; Kananian et al., 2017, 2020; Lehnung et al., 2017).
Group Facilitation and Language Access
The facilitator of the intervention varied throughout studies. A mental health professional facilitated most interventions with the assistance of a professional or volunteer language interpreter (Bernardi et al., 2019; Drožđek & Bolwerk, 2010; Droždek et al., 2012, 2014; Griggs et al., 2022; Hasha et al., 2022; Lehnung et al., 2017; Mazzulla et al., 2021). One study used the co-facilitation of a mental health professional and a community member with language capacity (Husby et al., 2020). In four studies, the facilitator was a mental health professional who shared the same language as group members (Bahu, 2019; Blignault et al., 2021; Kananian et al., 2017, 2020; Lehnung et al., 2017; Purgato et al., 2021). A non-specialist-trained facilitator facilitated the intervention in the participants’ native language in three studies (Purgato et al., 2021; Renner et al., 2011; Shaw et al., 2022). A social worker and research assistant facilitated one study, although there was no mention of interpretation or language access (Haefner et al., 2019). Finally, a Buddhist monk with language capacity facilitated one study (Han et al., 2012), and a non-professionally trained staff and an interpreter facilitated another (Mitschke et al., 2013). When studies used an interpreter, most did not state if the person was a member of the community or had language training only (Bernardi et al., 2019; Blignault et al., 2021; Drožđek & Bolwerk, 2010; Droždek et al., 2012, 2014; Griggs et al., 2022; Mazzulla et al., 2021).
Additionally, some studies also used written material within their intervention. Blignault et al. (2021) provided participants with a handbook. They showed PowerPoint slides throughout the intervention that were in English only, with the bilingual facilitator interpreting the material into Arabic during the group sessions. Purgato et al. (2021) provided an illustrated handbook that accompanied the intervention offered in participants’ native language. Mazzulla et al. (2021) created a phone app that did not use language but pictures and diagrams to bypass the need for translation and for the intervention to be accessible to those unable to read.
Intervention Outcomes
All studies used a pre-post-study design, with four studies using a RCT design (Han et al., 2012; Kananian et al., 2020; Purgato et al., 2021; Renner et al., 2011) and one study using a longitudinal design (Droždek et al., 2012). Only two studies investigated feasibility but found it to be high (Blignault et al., 2021; Griggs et al., 2022). Group adherence was also found to be high, with two studies reporting no dropouts (Bahu, 2019; Bernardi et al., 2019) and others reporting dropout rates lower than found in individual-level interventions with refugees (Drožđek & Bolwerk, 2010; Droždek et al., 2012). Participants also reported having a positive experience (Haefner et al., 2019) and having high levels of satisfaction with the interventions (Bahu, 2019; Bernardi et al., 2019; Husby et al., 2020). One study found high levels of provider satisfaction (Haefner et al., 2019). We provide findings for specific mental health outcomes below. See Table 1 for measures used to assess outcomes.
Study Details.
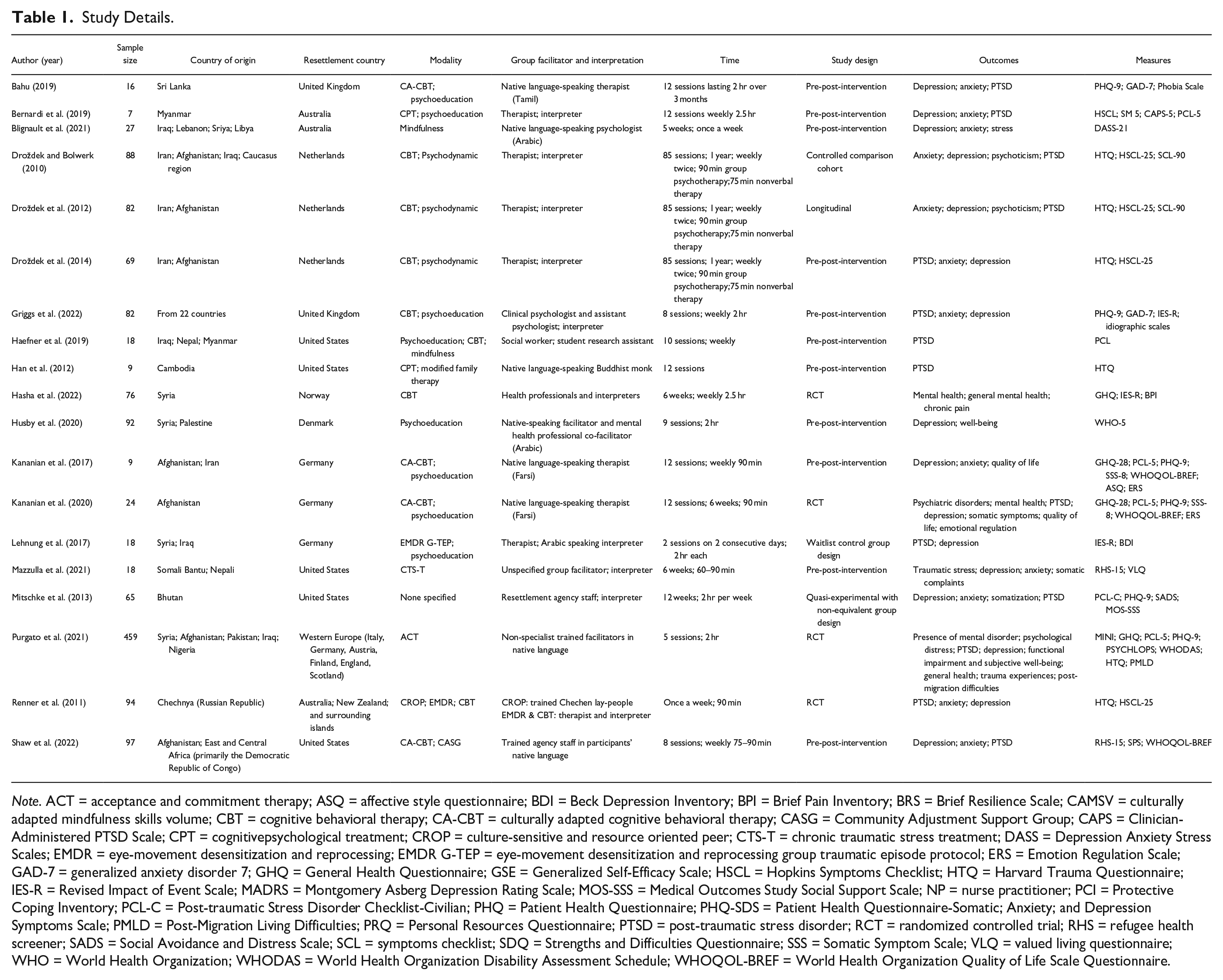
Note. ACT = acceptance and commitment therapy; ASQ = affective style questionnaire; BDI = Beck Depression Inventory; BPI = Brief Pain Inventory; BRS = Brief Resilience Scale; CAMSV = culturally adapted mindfulness skills volume; CBT = cognitive behavioral therapy; CA-CBT = culturally adapted cognitive behavioral therapy; CASG = Community Adjustment Support Group; CAPS = Clinician-Administered PTSD Scale; CPT = cognitivepsychological treatment; CROP = culture-sensitive and resource oriented peer; CTS-T = chronic traumatic stress treatment; DASS = Depression Anxiety Stress Scales; EMDR = eye-movement desensitization and reprocessing; EMDR G-TEP = eye-movement desensitization and reprocessing group traumatic episode protocol; ERS = Emotion Regulation Scale; GAD-7 = generalized anxiety disorder 7; GHQ = General Health Questionnaire; GSE = Generalized Self-Efficacy Scale; HSCL = Hopkins Symptoms Checklist; HTQ = Harvard Trauma Questionnaire; IES-R = Revised Impact of Event Scale; MADRS = Montgomery Asberg Depression Rating Scale; MOS-SSS = Medical Outcomes Study Social Support Scale; NP = nurse practitioner; PCI = Protective Coping Inventory; PCL-C = Post-traumatic Stress Disorder Checklist-Civilian; PHQ = Patient Health Questionnaire; PHQ-SDS = Patient Health Questionnaire-Somatic; Anxiety; and Depression Symptoms Scale; PMLD = Post-Migration Living Difficulties; PRQ = Personal Resources Questionnaire; PTSD = post-traumatic stress disorder; RCT = randomized controlled trial; RHS = refugee health screener; SADS = Social Avoidance and Distress Scale; SCL = symptoms checklist; SDQ = Strengths and Difficulties Questionnaire; SSS = Somatic Symptom Scale; VLQ = valued living questionnaire; WHO = World Health Organization; WHODAS = World Health Organization Disability Assessment Schedule; WHOQOL-BREF = World Health Organization Quality of Life Scale Questionnaire.
General Mental Health
Overall, studies showed a significant reduction in general mental health symptoms (Hasha et al., 2022; Husby et al., 2020; Kananian et al., 2017, 2020; Purgato et al., 2021; Shaw et al., 2022). Most studies additionally reported on effect sizes with moderate to large effects identified (Husby et al., 2020; Kananian et al., 2017, 2020; Shaw et al., 2022). One study looked at mental health outcomes at a 6-month follow-up and did not find significant results (Purgato et al., 2021), indicating a lack of long-term impact of the intervention.
Post-Traumatic Stress Disorder
PTSD was the most common outcome measured, and studies overwhelmingly found significant reduction in PTSD symptoms (Bahu, 2019; Bernardi et al., 2019; Drožđek & Bolwerk, 2010; Droždek et al., 2012, 2014; Griggs et al., 2022; Han et al., 2012; Lehnung et al., 2017; Mazzulla et al., 2021; Mitschke et al., 2013). Effect sizes varied from moderate (Kananian et al., 2020) to large (Droždek et al., 2012; Han et al., 2012; Mazzulla et al., 2021; Renner et al., 2011). One study reported that a reduction of symptoms was maintained after termination of intervention at delayed post-test (5 years; Drožđek et al., 2014), while other studies found symptoms increased with time (Bernardi et al., 2019). One study found no differences in delayed post-test depression symptoms between control and intervention groups (Mitschke et al., 2013).
Depression
Many studies also investigated the impact of group interventions on depression and found statistically significant improvement in symptoms (Blignault et al., 2021; Drožđek & Bolwerk, 2010; Droždek et al., 2012, 2014; Griggs et al., 2022; Husby et al., 2020; Kananian et al., 2017, 2020; Mazzulla et al., 2021; Mitschke et al., 2013; Purgato et al., 2021). Large effect sizes were found for those studies that reported them (Drožđek & Bolwerk, 2010; Droždek et al., 2012, 2014; Griggs et al., 2022; Kananian et al., 2017, 2020; Mazzulla et al., 2021). Some studies found improvements in symptoms that were not statistically significant (Bahu, 2019; Bernardi et al., 2019; Lehnung et al., 2017). One study found that symptoms were not maintained at delayed post-test (Bernardi et al., 2019), and another study found no differences in delayed post-test depression symptoms between control and intervention groups (Mitschke et al., 2013).
Anxiety
Studies found group interventions to have positive impacts on anxiety. Almost all studies that investigated anxiety found a significant reduction in anxiety symptoms (Blignault et al., 2021; Drožđek & Bolwerk, 2010; Droždek et al., 2012, 2014; Griggs et al., 2022; Kananian et al., 2017, 2020; Mazzulla et al., 2021). All studies that ran for effect sizes found large effects (Bahu, 2019; Drožđek & Bolwerk, 2010; Droždek et al., 2012; Griggs et al., 2022; Kananian et al., 2017, 2020; Mazzulla et al., 2021). One study showed reduced anxiety levels that did not reach clinical or statistical significance (Bernardi et al., 2019). One study found no statistically significant change in anxiety (Mitschke et al., 2013). Regarding delayed post-intervention follow-up, all three studies investigating delayed post-intervention follow-up found sustained improvement varying from a 3-month follow-up (Bernardi et al., 2019; Mitschke et al., 2013) to a 1-year follow-up (Kananian et al., 2020).
Other Outcomes
Four studies measured quality of life and found significant improvement (Kananian et al., 2017, 2020; Mazzulla et al., 2021; Shaw et al., 2022), and another study found significant improvement in stress symptoms (Blignault et al., 2021). One study did not show significant improvement in post-migration difficulties (Purgato et al., 2021). Somatic symptoms had mixed findings, with some studies reporting no significant improvement (Hasha et al., 2022; Mitschke et al., 2013) and others finding significant improvements (Kananian et al., 2020; Mazzulla et al., 2021). Psychoticism also had mixed findings, with one study reporting no significance (Drožđek & Bolwerk, 2010) and one study reporting significant improvement with medium effect sizes (Droždek et al., 2012).
Risk of Bias
The analysis of the 19 selected articles yielded an average MINORS score of 9.74 (SD = 2.42) out of 16. Notably, the studies generally scored well in articulating clear aims (M = 1.89, SD = 0.33) and prospective data collection (M = 1.82, SD = 0.42). However, the raters identified areas of concern, particularly in the unbiased assessment of study endpoints (M = 0.29, SD = 0.68) and the prospective calculation of study size (M = 0.37, SD = 0.75). Concerning the inclusion of consecutive patients, the studies scored an average of 1.42 (SD = 0.56), suggesting moderate adherence to this criterion. The average score for having endpoints appropriate to the study aim was 1.66 (SD = 0.44), indicating a generally adequate definition of outcomes. The studies averaged 1.37 (SD = 0.70) in the criterion of appropriate follow-up period, showing some variability in their follow-up methods. Lastly, the loss to follow-up criterion averaged 0.92 (SD = 0.85), highlighting a need for improved follow-up consistency across the reviewed studies. These findings underscore a critical need for future research to address these gaps, especially in ensuring objective endpoint assessment and methodical study size determination to enhance the overall quality and reliability of non-randomized studies.
Discussion
This systematic review explored the current state of literature regarding the use of group-based intervention in treating the mental health of refugees in the post-resettlement context. This review attempted to identify the current features of group-based interventions, explore how researchers incorporate cultural considerations into interventions, and determine how group interventions impact refugee mental health outcomes. We identified 19 studies that met inclusion criteria and found group interventions among refugees to be a promising intervention to treat mental health. Despite variations in the specifics of the group interventions, the results remained that all the interventions included showed some positive outcomes for participants. These findings highlight the potential efficacy of group interventions as a viable strategy for improving mental health outcomes among forced migrant and refugee populations with considerable trauma histories and mental health challenges. Critical findings can be found in Table 2.
Critical Findings.
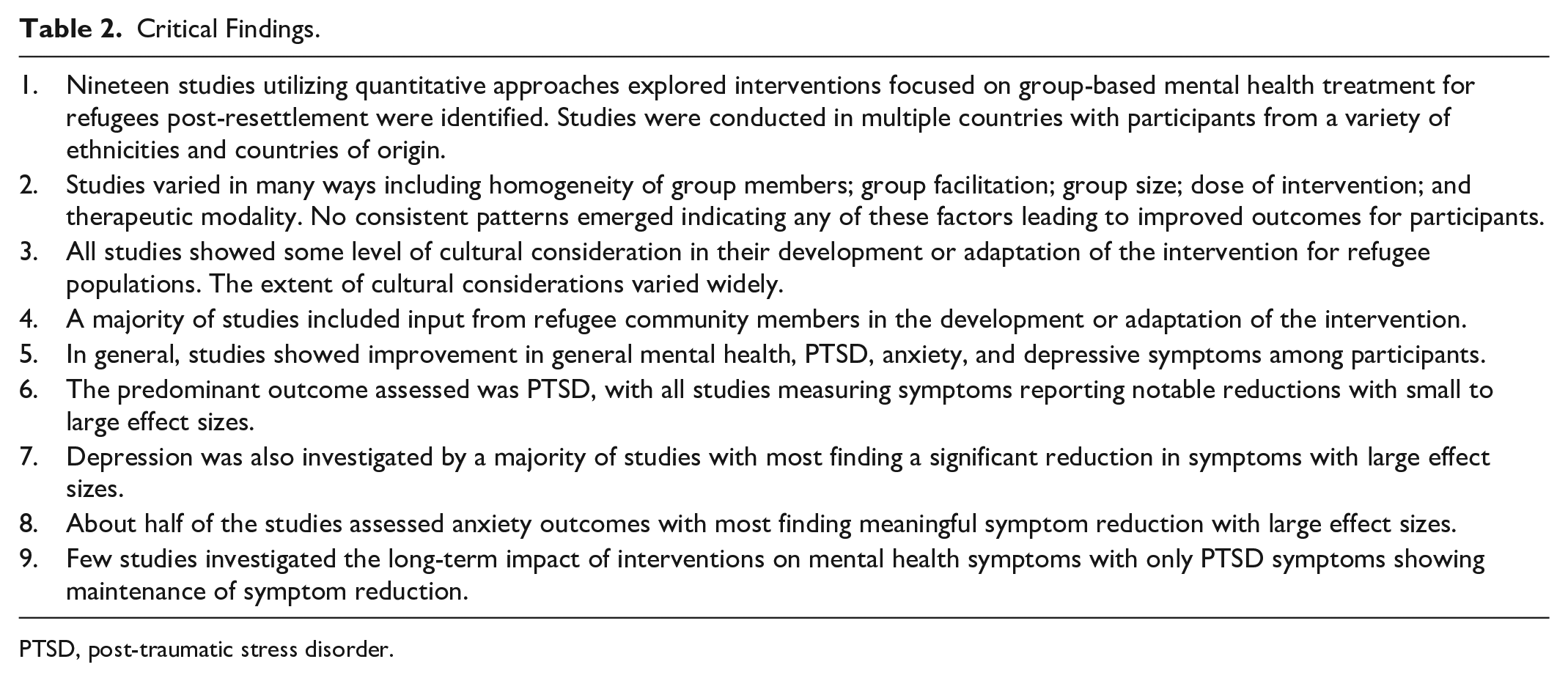
PTSD, post-traumatic stress disorder.
The limited availability of culturally grounded mental health interventions for implementation within refugee populations poses a critical barrier to improving the well-being of these communities. Studies within our review identified group interventions as culturally aligned with refugee populations and an intervention method participants found to be culturally grounded. While the advantages of group intervention included feasibility and cost-effectiveness, most studies consistently cited cultural relevance as the primary rationale for opting for this modality. Low dropout rates were another advantage seen, which is often high within refugee mental health interventions (Semmlinger & Ehring, 2022). Most importantly, all studies showed positive—though not all statistically significant—impacts on mental health outcomes. The variation in therapeutic modalities used and the continued positive effect on outcomes is evidence of the strength that group intervention may have, regardless of the therapeutic modality used. For example, the two included studies that used more than one group intervention curriculum found positive impacts on mental health for both group intervention curricula (Renner et al., 2011; Shaw et al., 2022). Refugee mental health literature has recently begun acknowledging the importance and impact of collective trauma and the need for collective healing among refugee groups (Kirsch, 2023; Magan et al., 2023). Members of collectivist communities often perceive traumatic experiences like war, political unrest, and displacement as attacks on not themselves as individuals but rather as a target to the entirety of the community (Abramowitz, 2005; Somasundaram, 2014). Research also points to the negative impact that collective trauma experiences can have on the individual when communities are not able to heal as a group and create a collective group narrative surrounding the traumatizing event (Abramowitz, 2005; Kirsch, 2023). Interventions at the group level acknowledge the collective culture prevalent in many refugee groups, providing a culturally anchored group setting that allows refugees space for healing. The interventions in this review highlight the possibility of group intervention to assist refugee populations in healing at the individual and community levels.
The level and extent of cultural adaptation and consideration among interventions varied considerably among studies. Language concordance between provider and client is the most basic and imperative cultural adaptation for interventions with this population. While it was encouraging to see all studies except one discuss how language was facilitated in the groups, the lack of acknowledgment of the importance of language concordance and its potential impacts was of concern. In a qualitative study of therapists working with migrants in Denmark, participants describe potential concerns in the therapeutic alliance when an interpreter is needed and how this can be a potential detriment to quality mental health care (Hanft-Robert, 2023). Chen and Chen (2020) specifically explore the interpreter’s role of the interpreter in a group therapy setting with forcibly displaced individuals and underscore the impact of the interpreter on group dynamics, stating that the interpreter inevitably impacts both interpersonal interactions and the group’s power dynamics. A native-speaking facilitator from the participant community will provide the most culturally competent group intervention because the facilitator can relate to and understand the group linguistically and culturally. However, interpreters will likely be needed due to the lack of available social work and other mental health professionals with a forced migration history. Providers must ensure that the language interpreter is seen as a person of vital importance in the dynamics of the group who can interpret both linguistic and cultural nuances from participant to therapist and vice versa (Chen & Chen, 2020).
Many cultural decisions and adaptations aligned with previous research on cultural adaptation, including using community members as facilitators, community consultants or advisory boards, homogenous ethnic and gender groups, and train the trainer models. While the wide breadth of cultural adaptations and lack of consistency across studies on the cultural adaptations used does not allow us to analyze the direct impact of each of these, the success of the above cultural adaptations within studies of this review and previous literature point their continual best practice among these populations. Incorporating cultural adaptation in how interventions are designed and conducted is imperative to treating the specific trauma history and mental health symptoms of refugee communities. Extensive research shows that interventions and research that better engage communities and incorporate cultural adaptations lead to improved outcomes. A systematic review of post-traumatic growth (PTG) among refugees identified community-based interventions as a facilitator for PTG (Sultani et al., 2024). It is hard, if not impossible, to measure what types or how much community involvement or adaptation is considered “enough” or appropriate, but McCleary and Horn (2023) state the importance of clearly stating and documenting cultural adaptation within intervention research manuscripts. For example, Akhtar et al. (2021) sufficiently described their adaptation of an intervention for Syrian refugees by validating it through qualitative data collection from community members, ensuring alignment with community needs. Additionally, there is a need to develop tools and assessments to more rigorously analyze the impact of certain adaptation choices to understand which are most important and should be encouraged for future research (McCleary & Horn, 2023).
Studies often overlooked post-resettlement structural barriers that exacerbate poor mental health outcomes, including financial struggles, lack of employment, transportation, and housing. While some did report that participants received case management through another entity while receiving the intervention, no study reported case management as part of the intervention. There is evidence that these structural barriers and post-migration difficulties exacerbate previous trauma and mental health symptoms (Byrow et al., 2020; DeSa et al., 2022). Maslow’s hierarchy of needs is a psychological theory proposed by Maslow (1943), which posits that humans have five levels of needs ranked from basic to more complex: physiological, safety, love and belonging, esteem, and self-actualization. According to this theory, individuals must satisfy basic-level needs before addressing higher-level growth needs. When applying Maslow’s hierarchy, providers must consider ways of ensuring that refugee clients are provided with their basic needs before they implement higher levels of mental health treatment to reduce trauma symptoms. Research shows the need to implement case management approaches as part of a holistic mental health intervention (Soukenik et al., 2022; Im et al., 2021).
Further, in the United States, extended case management programs have been shown to improve well-being outcomes (Shaw & Poulin, 2015). Similarly, an unexpected finding was the lack of support participants received when enrolled in the intervention, such as childcare or transportation assistance, to overcome structural barriers to access interventions. These are significant barriers to refugees that negatively impact their ability to access mental health services (Farber et al., 2018). The addition of these factors could improve access to interventions.
Limitations
While we took several steps to enhance the rigor of our review, several limitations may still exist. The included studies exhibited a wide range of methodologies, making it challenging to synthesize findings cohesively. Variability in intervention types, outcome measures, and follow-up durations across studies may introduce limitations in drawing conclusive insights. The systematic review incorporated studies with varying levels of methodological quality and rigor. Differences in study design, sample sizes, and measurement tools may impact the overall reliability of the synthesized evidence. Due to these variances in both study designs and outcomes assessed, a meta-analysis was not feasible, limiting the ability to strengthen the reliability of our findings. The reviewed literature involved refugees from diverse geographic regions and cultural backgrounds. The heterogeneous nature of these populations may limit the generalizability of findings to specific refugee subgroups or regions. We did not include gray literature in this study, which may have excluded studies that met inclusion criteria. Additionally, though the data range was purposefully identified based on an understanding of the literature, articles outside this date range that met the criteria may have been missed.
Finally, it is important to acknowledge that our study investigated only group-based interventions in high-income countries. This decision was a deliberate decision due to the vast differences in both need and resources available to carry out mental health interventions in high-income versus low-income settings. However, this focus does not reflect the authors’ perceptions of the importance of these interventions in one setting over the other. The decision to investigate interventions in high-income settings was based on the lead author’s extensive experience of mental health care in high-income settings and ability to assess the interventions based on this experience. The authors believe a systematic review of group-based interventions within LMIC is warranted, knowing that 75% of the world’s refugees currently live in countries that are not considered high-income (UNHCR, 2022). We encourage researchers with this practical experience to do so, as group-based interventions could be a valuable intervention model in these settings due to the cultural alignment and potential increased feasibility and cost.
Implications and Conclusion
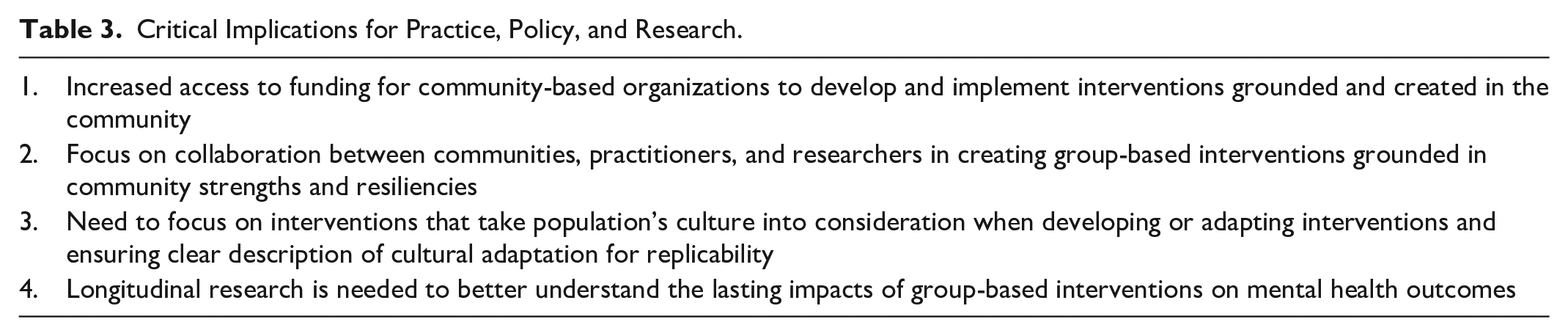
Our study has research, practice, and policy implications (See Table 3 for critical implications). While studies showed group-based interventions to reduce mental health symptoms, few studies investigated the long-term impact of interventions on mental health outcomes. Those that did show symptoms often increased over time after the intervention ended. Future research is needed using longitudinal methods to better understand the impact of these interventions over time compared to individual-level interventions. While several RCTs were completed, more rigorous methods are needed in future research to better understand best practices for group-based interventions.
Critical Implications for Practice, Policy, and Research.
While refugee communities have undergone extensive trauma throughout their migration experience, causing mental health symptoms, these populations also show great strength and resilience. Interventions that build upon the inherent strength of communities and their cultures are needed to improve the well-being of these communities. Funding for future programming and research on interventions for refugees should be focused on collaboration between refugee community members, providers, and researchers so that interventions are grounded in the voices, strengths, and experiences of refugees themselves. Our study highlights that group-based interventions are seen as a culturally grounded intervention model that may improve mental health outcomes. Leveraging these findings and including refugee organizations and communities in the development of interventions will allow for increased PTG and build off the resiliency refugees have following their often-traumatic migration histories.
As the number of global refugees continues to increase (UNHCR, 2023) and refugees continue to show high levels of mental health concerns in the post-migration context (Henkelmann et al., 2020), there is a critical need for culturally tailored mental health interventions for this population that improve mental health and well-being outcomes. This systematic review recognizes group-based intervention as a feasible approach that aligns with the cultural needs of refugee communities. Future funding should be allocated to enhance comprehension of group-based interventions to advance the field. Rigorous research designs are essential to uncover best practices in implementing such interventions. Moreover, providing resources for collaboration between researchers and refugees will facilitate the development of interventions that are co-created with, rather than for, the community.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.