
Abstract
Health education and behavior change interventions typically pay little attention to the intervention’s instructional foundation. Combining the fields of health literacy, cognitive psychology, and adult learning theory, this article provides an integrative scientific approach, called the BEAN (Better Education and iNnovation) model, to creating an instructional foundation based on how individuals acquire knowledge and skills. The article uses a case study example from an adult literacy center’s health literacy class to explore how environmental factors and instructional strategies can be applied to health education and behavior change interventions. Data for this case study were derived through 20 hours of classroom observation and qualitative interviews with 21 adult education students and 3 instructors. Results provide practical examples of environmental factors and instructional strategies designed to facilitate learning, such as fostering autonomy, activating prior knowledge, and fostering perspective change. Results also describe the resulting health behavior changes of students attending the health literacy class, such as increased medication adherence and physical activity, improved nutritional habits, and increased question asking of health practitioners. This article serves as a first step to encouraging researchers and educators to consider the importance of drawing on cognitive psychology and theories of adult learning to create a scientifically based instructional foundation for health behavior change programs. Additionally, by drawing on the expertise of adult educators well versed in the science of instructional design, this article also demonstrates that the adult education classroom is an excellent setting for conducting health education and behavior change interventions.
I don’t like theoretical crap, okay? I don’t like it. Tell me something I can understand, all right? Tell me something I can use in my life.
Pedagogy, the science of education, is often absent from public health intervention development because most public health professionals are trained in theories of behavior change and have no training in how individuals learn (Institute of Medicine, 2004). Thus, many interventions are developed with attention to the selection and use of behavior change theories, with little attention to the instructional foundation of how individuals learn information and acquire skills (Glanz, Rimer, & Viswanath, 2008; Jeffery, 2004; Rothman, 2004). Recent challenges to the field of health education and behavior recommend looking to other disciplines for the expertise currently missing from the field in order to increase the effectiveness of future interventions (Bosworth & Voils, 2005; Institute of Medicine, 2004; Resnicow & Vaughn, 2006). To that end, the integration of two additional disciplines, cognitive psychology and adult learning theory, may provide the instructional foundation missing from current interventions.
Most health education and behavior change interventions seek to impart skills, not just teach content knowledge. In the language of health literacy, these are called functional health literacy skills—the basic health-related skills needed for daily living activities to ensure personal health (Parker, Baker, Williams, & Nurss, 1995). Given the amount and complexity of skills required to prevent and manage chronic disease, it can be helpful to consider a focus on functional health literacy skill acquisition as part of health education and behavior interventions. To meet this challenge, the Institute of Medicine (2004) has recommended the use of adult education programs as a vehicle to teach functional health literacy skills.
Cognitive psychology can provide an explanation of how individuals perceive, process, and organize information so as to later recall and apply this information appropriately (Bruner, 1990; Chomsky, 1967). Similarly, adult education focuses specifically on using strategies that can motivate adults to learn information and acquire functional daily living skills (U.S. Department of Health and Human Services, 2003). In this article, we first provide a brief summary of key concepts from cognitive psychology and adult learning theory as related to health education and behavior change interventions. Next, we use a case study example from an adult literacy center’s health literacy class to demonstrate how these key concepts may be applied in a health education setting.
Cognitive Psychology
Cognitive psychology sees information acquisition as a series of steps, beginning with perceiving and processing sensory information (Kellogg, 1995). When an individual spends cognitive energy trying to see or hear something (e.g., in an environment that is loud or dimly lit), he or she is less able to remember it, thus limiting the subsequent use of the information (Wingfield, Tun, & McCoy, 2005). According to one perspective, processing abilities involve the speed with which an individual can select and use meaningful sensory information (Kellogg, 1995). Ability to recall information is affected by how deeply information is processed, which is determined by how connected new information is to existing information in the brain, and how much time is spent processing the information (Byrnes, 1996; Kellogg, 1995). Deeply processed information is ultimately more likely to be remembered and used (Kellogg, 1995). Interventions that focus on creating environments conducive to learning and use strategies that promote retention of information and skills may ultimately be more successful in promoting behavior change (Byrnes, 1996; Culos-Reed, Rejeski, McAuley, Ockene, & Roter, 2000).
Theories of Adult Learning
Most theories of adult learning rely heavily on placing learning in the context of real-life situations, making learning immediately relevant, and empowering learners to take an active role in posing questions and developing solutions (Candy, 1991; Freire, 2000; Knowles, 1973, 1980). Newer theories of adult learning also focus on the process of perspective change (Mezirow, 1996; Taylor, 1998), methods to increase motivation (Wlodkowski, 2008), and collaboration (Brookfield, 1986)—all with a focus on increasing knowledge and skill acquisition.
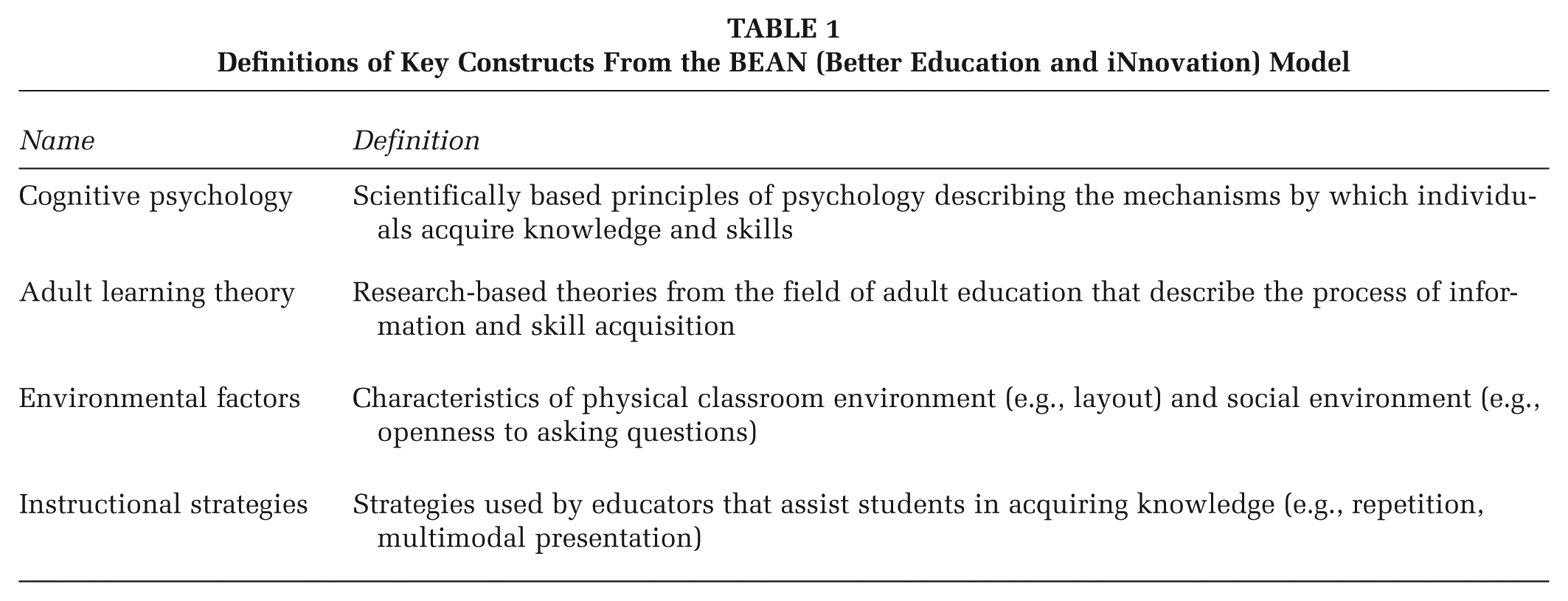
Figure 1, the BEAN (Better Education and iNnovation) model, derived from the health literacy case study described in this article, demonstrates how integrating cognitive psychology with theories of adult learning can influence environmental factors and instructional strategies. These factors and strategies can then be used together to increase acquisition of functional health literacy skills and promote behavior change. The model also shows that sharing knowledge and skills can be an important aspect of acquiring skills and using them. Table 1 provides definitions for each of the concepts listed in the model, two of which are described in greater detail below.

The BEAN (Better Education and iNnovation) Model: An Instructional Foundation for Increasing Acquisition, Use, and Sharing of Functional Health Literacy Skills
Definitions of Key Constructs From the BEAN (Better Education and iNnovation) Model
Environmental Factors
Physical layout
Theories of adult learning propose that classrooms become learner centered, placing value on the role that students play in teaching each other (Davis, 1993; McCombs & Whisler, 1997). These classrooms are generally organized in a circle or U shape to foster greater communication between students (McCombs & Whisler, 1997).
Social environment
Theories of adult learning also emphasize that learners must feel that they are in an emotionally safe and supportive space before they are ready to share and learn from others (McCombs & Whisler, 1997). Educators can foster social support by providing opportunities for students to share questions, concerns, and experiences.
Instructional Strategies
Drawing on cognitive psychology and theories of adult learning, educators must learn how to identify what participants already know and find ways to add new information into what is already known. The following examples of how environmental factors and instructional strategies can be applied are taken from the case study of an adult education health literacy class described below. The examples from this study directly relate to concepts from adult learning theory and cognitive psychology as described in the BEAN model and Table 1.
Case Study Background
This study was conducted with students from an adult literacy center in the Atlanta area attending a health literacy class. The course was based on the National Institute for Literacy’s Health Literacy Curriculum, which includes preventive care, physical activity, nutrition, and communication with health care professionals. Classes met twice a week for 2 hours at a time, spanning a 12-week period. This study explored the types of environmental factors and instructional strategies that helped students acquire these broad-based functional health literacy skills (Kutner, Greenberg, Jin, & Paulsen, 2006). Results describe these factors and strategies through the integrated lenses of cognitive psychology and adult learning theory and then describe participants’ resulting changes in health behavior.
Method
This qualitative study consisted of a series of classroom observations, interviews with adult literacy students, and interviews with instructors. Ten 2-hour classroom observations were conducted over the Fall 2009 and Spring 2010 semesters. The researcher developed an observation guide to capture educator strategies and student responses to strategies. Interviews were conducted with adult learners to explore attributes of the class environment that facilitated learning, perceptions and use of skills taught in class, and opportunities for sharing information and skills. Interviews were also conducted with each of the three health literacy adult educators, exploring philosophy of teaching and educational strategies. Most interviews lasted approximately 60 minutes.
To be eligible, potential student participants must have attended at least 12 hours of the health literacy classes during the 2009-2010 program year and be sufficiently fluent in English to complete the consent process and engage fully in the interview. Participant variation was sought in both age and gender. In qualitative research, the sample size is typically driven by theoretical saturation, reached when the interviewer hears similar themes and issues emerging from participant stories (Strauss & Corbin, 1998). Interviews were conducted until theoretical saturation was reached at 24 interviews (21 students and 3 educators). All participants were given $20 for their participation in the interview. The Emory University Institutional Review Board approved all study procedures.
Data Analysis
Descriptive statistics were calculated to summarize participant demographic information, including gender, age, race/ethnicity, employment status, and frequency of class attendance. Transcripts and field notes were analyzed by one team member over the course of 6 months under the guidance of a lead qualitative methodologist and consultation from other team members, including experts in health literacy, cognitive psychology, and adult education. Analysis incorporated a combination of thematic analysis, a data-driven method used for identifying, analyzing, and reporting patterns in the data, and content analysis, a theory-driven process designed to find previously identified themes in the data (Braun & Clarke, 2006; Maxwell, 2002; Weber, 1990). The initial codebook was generated by identifying codes based on the transcripts and observations. These codes were then defined by the primary researcher and discussed with additional team members. The codes were used to identify themes—overarching areas of commonality among groups of codes—as part of thematic analysis. Content analysis was subsequently conducted by identifying key concepts from the adult learning theory and cognition literatures and exploring transcripts for their presence. Together, these inductive and deductive processes resulted in the identification of environmental factors and instructional strategies derived from both the data and the theory that explain the manner in which adult students acquire and use functional health literacy skills (Yin, 1989). NVivo software was used for data management.
To increase interpretive validity, the researcher conducted member checks in the form of a focus group, which involved discussing preliminary findings with nine adult learners in the health literacy classes and soliciting feedback on the accuracy of interpretations. The researcher also conducted a member check with the primary health literacy educator.
Results
Demographics
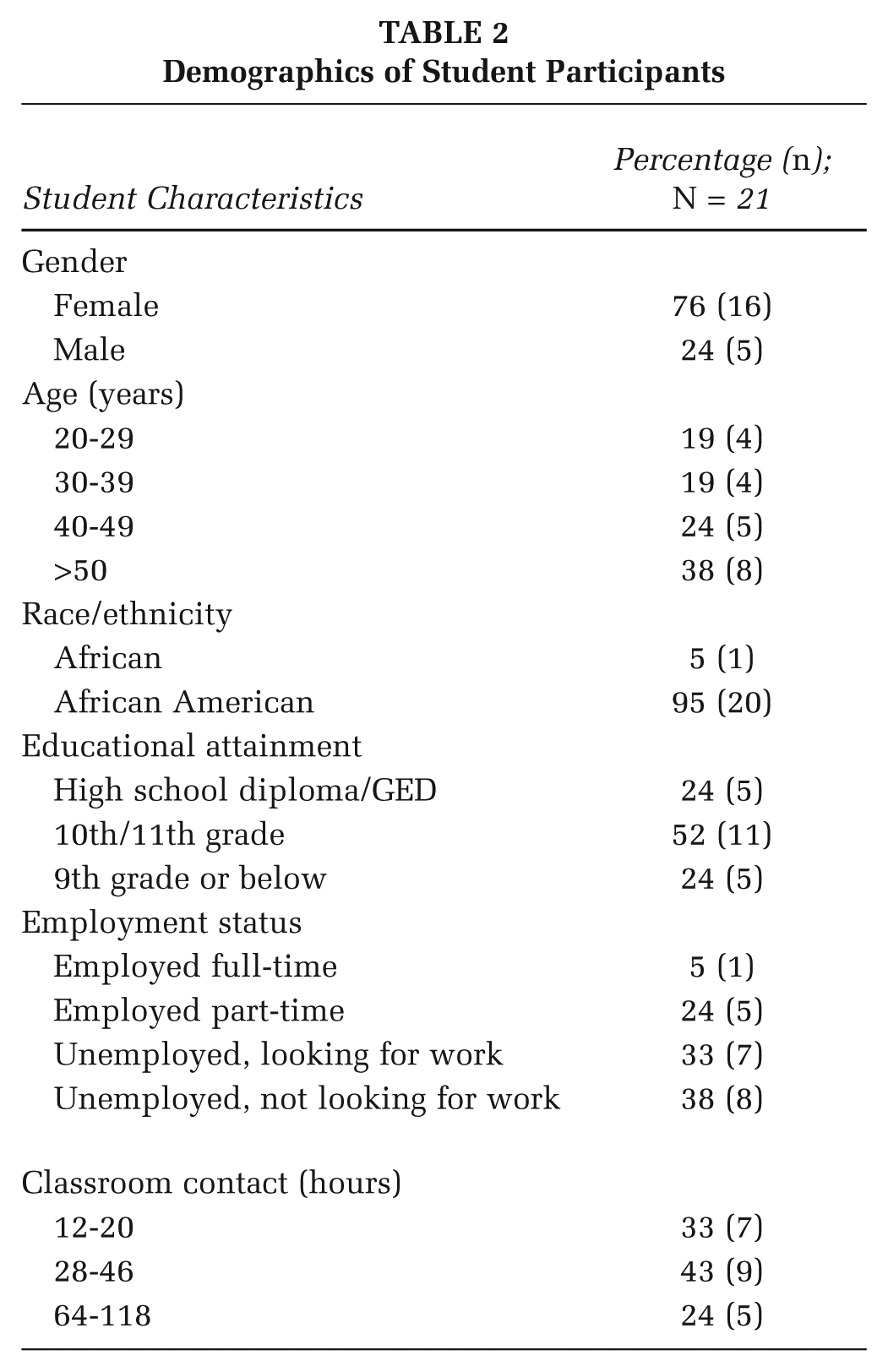
The majority of students (76%) were female, and all were African or African American. The average age was 42 years, ranging from early 20s to mid-60s. Most students read between a 4th- and 6th-grade reading level, although most had completed the 10th or 11th grade. Average number of classroom contact hours varied, with a mean of 37.5 hours and a median of 32 hours. Six students had taken the class multiple times, whereas other students had only recently taken the class for the first time. Table 2 summarizes the demographic characteristics of student participants. All three instructors were female and ranged from having little formal education on teaching adults to having an advanced degree in adult education.
Demographics of Student Participants
Results from this study describe the environmental factors and types of instructional strategies used by educators to help students acquire functional health literacy skills. Table 3 provides a summary of these strategies and examples of their application in the health literacy class case study.
Summary of Environmental Factor and Instructional Strategy Examples
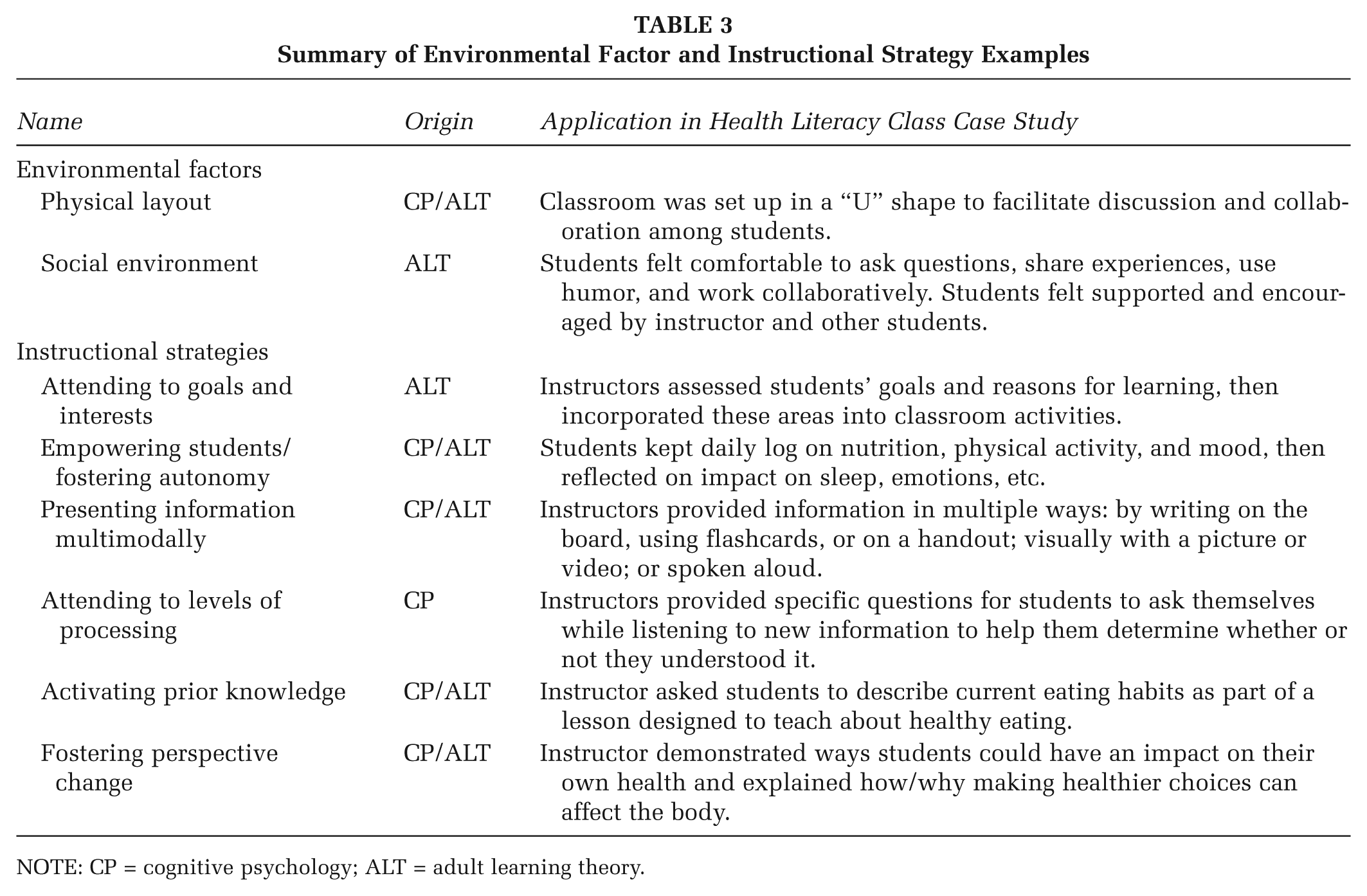
NOTE: CP = cognitive psychology; ALT = adult learning theory.
Environmental Factors Influencing Knowledge Acquisition
Physical layout
Observations took place in two classrooms. Both classrooms had a general “U” shape, with the educator at the front near the whiteboard. Students were easily able to see each other and the instructor across the room, which helped facilitate classroom discussions.
Social environment
The classroom also embodied a spirit of collaborative learning—a place in which students were excited to be learning with and from each other, without a sense of competition or rivalry. For students dealing with shame and embarrassment from poor reading skills, this type of supportive social environment can be very beneficial, as explained by this older female student:
When you don’t know how to read . . . people sit there and laugh at you like you’re a little ant. Here, I don’t feel that way because they bring my spirit up.
Students felt encouraged and welcomed by the educator and other students in the classroom. These characteristics were key to providing a space where students felt comfortable to ask questions and be open to learning.
Instructional Strategies
Although each of the educators interviewed had a different philosophy toward teaching and learning, there were many commonalities in the ways they helped students learn. These common strategies included attending to individual goals, needs, and interests; empowering students and fostering autonomy; presenting information multimodally; attending to levels of processing; activating prior knowledge; and fostering perspective change.
Attending to individual goals, needs, and interests
All educators interviewed mentioned the importance of getting to know students as individuals and being responsive to their needs. This strategy stems from theories of adult learning and cognitive psychology, both of which focus on putting new information into existing and immediately useful contexts for learners.
Empowering students and fostering autonomy
All educators interviewed emphasized that their adult students are independent learners. As such, educators sought to create activities that foster independence, goal setting, self-sufficiency, and a sense of responsibility. For example, during the health literacy class, students created a diet and exercise log detailing food intake, daily activities, and emotions. Students kept this log for several weeks and reflected on how their dietary habits, daily activities, and emotions affected each other and their daily lives.
Presenting information multimodally
Similar to repetition, many learners do best when being presented with information in more than one modality, such as orally, in writing, or by video. One educator explains her approach to multimodal teaching:
Some people learn visually, some learn hands-on, some learn just by listening, some learn by reading. You have to incorporate all that into your classroom because you have all those different types of learners.
In the classroom, information was often presented initially in writing, and then students took turns reading the information aloud from their handouts. At times, the educator would read through the passage aloud again to ensure comprehension based on a fluid reading. Other times, the educator used note cards to present information and then also read the words aloud. These techniques for presenting information in multiple ways are especially useful when teaching vocabulary.
Attention to levels of processing
Educators discussed using activities that facilitate deeper levels of processing, which increases the likelihood that students will retain information. One important way to help students process information more deeply is to provide practical application while teaching, as explained by one educator:
When going to the doctor, remember, “What is wrong with me? What do I need to do? How often do I need to do it?” For some people, they don’t even have that sort of structure in their head of the who, what, when, where, and why.
This quote demonstrates the importance of using strategies that help students mentally organize new information.
Activating prior knowledge
According to cognitive psychology and theories of adult learning, tying in new concepts to previously known information can assist with memory, recall, and subsequent use of information. This strategy was used during a nutrition lesson when the educator began class by asking students to recount what they had eaten over the weekend. The subsequent lesson focused on making healthy food choices during meals. By using the students’ experiences as examples throughout the lesson, the educator was able to connect prior knowledge and experiences to new information and skills. This activity helped students make a concrete connection between unhealthy food options that they were currently making and healthier options that they might choose in the future.
Fostering perspective transformation
Many students were surprised to learn that their current behaviors, particularly surrounding diet and exercise, were unhealthy for them. Additionally, many students did not realize that they had control over their health and options for prevention and treatment, as explained by this middle-aged man:
That’s what I think the health class is really about, learning your options . . . And with a health issue, you probably don’t know your options.
This realization was often very empowering for students and motivated them to learn more about health topics that interested them. For other students who had previously been exposed to messages on health promotion, the class provided them an opportunity to understand the “why” behind the “what,” as illustrated by this older woman:
Somebody can tell you all day you know you’re not supposed to eat that . . but [it’s different when] you can understand and know the damage and what happens when you eat bad foods.
The explanation of why it was important to engage in a particular health-related behavior addressed students’ prior misunderstandings about the causes and outcomes of disease.
The collected use of these strategies not only helped students acquire new knowledge and skills but also motivated them to change their behavior, as illustrated next.
Behavior Change Following Acquisition of Functional Health Literacy Skills
In addition to learning new information and skills, most students also described using them to engage in some type of health-related behavior change. The most frequent types of behavior change related to diet and physical activity, but students also described asking questions of health care providers and increasing medication adherence.
Nutrition and physical activity
Eating healthfully is a complex process involving many skills, and the primary educator was careful to provide specific actions for students to take toward this goal. Several students began to walk more after the educator suggested getting off the bus early and walking the rest of the way to increase physical activity each day. Most of the students reporting a change in eating behaviors were female, which was discussed during member checks. Both men and women felt that this difference may exist because women tended to be caretakers and felt responsible to be good role models.
Asking questions at the doctor’s office
Many students described that they used to be uncomfortable during doctor visits because they felt intimidated and unable to admit confusion or ask questions. An important part of the class for most students was being “given permission” to ask questions. As many students felt that they should not question someone with so much education, the lessons on question-asking were empowering and motivating.
Medication adherence
Several students mentioned that they were unsure of whether or not they were taking their medications correctly until they learned how to read medication labels in class. One woman described how she had breakthrough seizures until learning in class that her medication label directed her to take one pill in the morning and one in the evening, not just two pills at any time. She began taking her medication as directed and subsequently stopped having seizures. Other students may have been able to read the medication labels but did not understand the consequences of taking medication haphazardly until the topic was discussed in class. One young diabetic woman made the connection during this lesson that her worsening diabetes-related symptoms were related to not adhering to her medication regimen. As she began to take her medication as directed, the symptoms disappeared.
The impact of these behavior changes on students’ lives was significant, ranging from weight loss to mood improvement to cessation of seizures. Although the original goal of the health literacy curriculum was not focused on health these types of outcomes, it is clear that educators able to impart knowledge and skills can have a wide-reaching impact on their students’ lives.
Discussion
Results from this study demonstrate how careful attention to environmental factors and instructional strategies can greatly affect how students learn. In this adult education classroom with a health literacy focus, a socially supportive environment served as a valuable motivator for students to attend class and participate in classroom sessions. Many students also reported improving their eating habits, beginning to exercise, asking questions of their health care provider, and increasing medication adherence.
These results have several limitations: specifically that these changes in behavior were assessed qualitatively and were not directly measured or observed. As such, it is possible that students may have exaggerated the extent to which they engaged in behavior change. Additionally, this study was conducted with a relatively homogenous, primarily English-speaking population in the urban South. Results may differ when conducted with rural populations, nonnative English speakers or in other parts of the country.
Conducting research in the adult education setting can be difficult, because of students’ competing priorities of school, family, work, health, transportation, or financial considerations (Comings & Soricone, 2007). Despite these challenges, there is a wealth of expertise in this setting regarding acquisition of functional health literacy skills that can be extremely valuable when applied to health behavior change interventions. Some of the success in the health literacy classes may be because of the way in which adult educators adapted instructional strategies to meet student needs, interests, and learning styles. By attending to learners’ goals and interests, fostering autonomy, activating prior knowledge, and presenting information in multiple ways, educators in any context can become more effective at imparting knowledge and skills, and ultimately in changing behavior.
As demonstrated by this case study, educators must seek to provide concrete examples over general suggestions. For example, “steam sweet potatoes rather than fry them” is a specific way to “eat less fat.” Many students simply do not know what specific behaviors they need to change, so it is important to provide real examples throughout lessons. Similarly, the health literacy class in this study may have been able to facilitate even greater change by focusing more on goal setting as a means to motivate students and monitor progress toward health-related goals. Revisiting these goals on a weekly basis and addressing challenges and facilitators could help students keep on track by working together. Additionally, the class may have considered engaging students in role-play activities, as practicing desired behaviors can help students process them more deeply, aiding with memory and subsequent use.
This article serves as a first step toward encouraging researchers and educators to consider the importance of drawing on cognitive psychology and theories of adult learning to create a scientifically based instructional foundation for health behavior change programs. More work must be done to determine which of the strategies identified here most contribute to learning and behavior change in health education interventions. Future studies should also consider a mixed-methods approach to data collection and analysis with a focus on measuring the methods by which individuals acquire knowledge and skills. Additionally, by drawing on the expertise of adult educators well versed in the science of instructional design, this article demonstrates that the adult education classroom is an excellent setting for conducting health education and behavior change interventions.
Footnotes
Authors’ Note:
The contents of this article do not necessarily represent the views of the U.S. Department of Veterans Affairs or the United States Government. This research was funded by Emory University, Laney Graduate School and Rollins School of Public Health, the Department of Behavioral Sciences and Health Education, and Letz Funds. We also extend our gratitude to the students and staff of Literacy Action, Inc., for their interest and willingness to participate in this study.