
Abstract
Intimate partner violence (IPV) is as prevalent in lesbian, gay, bisexual, and transgender (LGBT) relationships as it is in heterosexual ones; however, the issues, needs, and challenges associated with assisting or advocating on behalf of LGBT persons are poorly understood. Using community-based participatory approaches, we conducted a brief survey of professionals (e.g., shelter staff, domestic violence prevention and intervention programs, law enforcement) affiliated with one or more domestic violence prevention and/or intervention networks in Los Angeles, California. The sample, which included professionals (N = 54) from diverse programs/agencies, was obtained using purposive and snowball sampling. Participants self-administered a 33-item, online questionnaire. Analyses primarily involved descriptive statistics (frequencies, proportions). Most respondents had little or no training in LGBT IPV; nevertheless, nearly 50% of them reported having assisted LGBTs “sometimes” or “often” in the past year. Nearly all (92%) reported that their agencies/programs lack staff with dedicated responsibilities to LGBT IPV. The most frequent requests for assistance respondents reported receiving from LGBTs were for counseling, safe housing, legal assistance, and assistance navigating the medical system. The findings suggest that staff believe their agencies/programs inadequately address LGBT IPV but that many of the inadequacies (e.g., lack of staff training on LGBT IPV) are remediable.
Introduction
Lesbian, gay, bisexual, and transgender persons (LGBTs) who experience intimate partner violence (IPV) must be able to rely on publicly available prevention and intervention (prevention/intervention) resources. Rates of IPV are similar in LGBT and heterosexual relationships (Greenwood et al., 2002; Zahnd, Grant, Aydin, Chia, & Padilla-Frausto, 2010). An estimated 11% to 50% of women partnered with men, 7% to 55% of women partnered with women, and 11% to 44% of men partnered with men experience IPV (Burke & Follingstad, 1999; Kulkin, Williams, Borne, de la Bretonne, & Laurendine, 2007; Peterman & Dixon, 2003; Turell, 2000). Legal and attitudinal changes in society are making it easier for LGBTs to report IPV and seek assistance without fear of harm or criminalization; since 2009, reports of LGBT IPV have increased nearly 40%.(National Coalition of Anti-Violence Programs, 2011). How agencies/programs deal with LGBT IPV, however, is unclear.
Historically, IPV prevention/intervention has focused on the needs of heterosexual women survivors whose male partners perpetrate the abuse (Hassouneh & Glass, 2008). This approach misses many LGBT survivors (and abusers; Kulkin et al., 2007; Lundy & Leventhal, 1999; Ristock, 2003). The tendency to frame relationships according to heterosexual norms, the use of terminology such as battered women’s shelters instead of domestic violence shelters, and gendered assumptions (e.g., that only men are perpetrators) limit the appropriateness and effectiveness of available resources for LGBTs (Hassouneh & Glass, 2008; Seelau, Seelau, & Poorman, 2003). Although some of the issues LGBT survivors face are universal to all survivors (e.g., physical and/or emotional pain), other issues are unique to LGBTs (Patzel, 2005; Relf, 2001). For example, the threat of having one’s sexual orientation or HIV-positive status disclosed to employers or family members is a dominant feature of LGBT IPV that forces survivors to remain in abusive relationships, keep the abuse secret, and be selective about what they disclose when seeking help (Elliott, 1996; Kulkin et al., 2007).
In reviewing studies on LGBT IPV prevention/intervention services and resources, we identified several patterns (Ard & Makadon, 2011). The same factors (e.g., homophobia) that limit LGBT access to regular health care also affect LGBT access to and use of IPV prevention/intervention resources and services (Freedberg, 2006). Misconceptions about LGBTs influence how providers treat members of this population (Freedberg, 2006). IPV-related misconceptions include that women do not perpetrate violence, men cannot be victims of abuse, and violence occurring within same-sex relationships does not constitute IPV (Brown, 2008; Helfrich & Simpson, 2006). Fear of inappropriate, insensitive, or homophobic treatment affects when and where LGBTs seek help and whether they disclose sexual orientation (Freedberg, 2006) or IPV. Many LGBT survivors report having had negative experiences with staff and clients at non-LGBT agencies/programs, which leads them to rely heavily on the LGBT community for assistance (Bornstein, Fawcett, Sullivan, Senturia, & Shiu-Thornton, 2006; Merrill & Wolfe, 2000).
The literature also suggests that standard approaches to IPV screening may be ineffectual for LGBTs (Chan & Cavacuiti, 2008). Often sexual orientation is not routinely assessed; therefore, LGBT clients receive services that are not tailored to their needs. In one study, gay men survivors ranked battered women’s services and couple’s counselors as resources that had been “least helpful” or “harmful” to them (Merrill & Wolfe, 2000). In other research, battered LGBTs described how couples counselors did not acknowledge IPV in their relationships and encouraged them to remain in the abusive situations (Bornstein et al., 2006; Kulkin et al., 2007). Counselors with that orientation may suggest, for instance, that a battered gay man should hit his abusive partner back.
The tools agencies/programs use to screen participants often inadequately distinguish LGBT perpetrators from survivors. Additional screening or a different kind of screening from that used with heterosexual women may be necessary to distinguish perpetrators from survivors in same-sex relationships (Freedberg, 2006; Ristock, 2003). In LGBT IPV, the abusive partner may present herself or himself to service providers as the victim in order to access designated “safe spaces” such as shelters or support groups and continue controlling the survivor (Bornstein et al., 2006). Such spaces typically are gender specific, but that does not necessarily mean they are survivor specific. Further, law enforcement often inaccurately assesses IPV in domestic disputes among LGBTs. Battered LGBTs are more likely than their heterosexual counterparts to be arrested during domestic disputes, and dual arrests (i.e., arrest of both partners) are 30 times more likely in same-sex partnerships than in those involving a male perpetrator and female survivor (Hirschel, Buzawa, Pattavina, Faggiani, & Reuland, 2007).
Qualitative research with IPV agency staff suggests that the factors limiting LGBT IPV services are remediable. The staff want to improve services for LGBTs but lack the knowledge and skills to do so (Helfrich & Simpson, 2006; Younglove, Kerr, & Vitello, 2002).
The purpose of this brief assessment was to (a) understand agencies’/programs’ current approaches to addressing LGBT IPV, (b) identify key issues, needs, and challenges that IPV prevention– or intervention–related agencies/programs face in assisting or advocating on behalf of LGBT persons affected by IPV, and (c) obtain recommendations for improving LGBT IPV prevention– and intervention–related services and resources. This study focuses on the perspectives of staff. LGBT survivors’ and batterers’ experiences will be examined in a subsequent phase of the broader project.
Method
Population and Setting
Los Angeles, California, ranks second among U.S. metropolitan areas in the size of the lesbian, gay, and bisexual population (California Department of Finance, 2010; Gates, 2006; U. S. Census Bureau, 2010). An estimated 440,000 lesbians and gay men live in the Los Angeles metropolitan area, and many more bisexuals and transgender persons (whose numbers are less well documented) reside in this region (Gates, 2006). The city includes sexual orientation as a protected category within its nondiscrimination clause. In 2008, the Los Angeles City Council established an LGBT issues subcommittee of the Los Angeles City Domestic Violence Task Force (Los Angeles City Council, 2008). The Subcommittee, which included representatives from the City Attorney’s office, the Los Angeles Police Department, the L.A. Gay & Lesbian Center, domestic violence shelters, violence prevention programs, and other agencies/programs, was charged with developing a “comprehensive strategy which will help mitigate LGBT domestic violence issues” (Los Angeles City Council, 2008). To address this charge, the subcommittee decided to begin by obtaining a “snapshot” of the current prevention/intervention approaches and concerns of agency/program staff. This article presents the results of the brief assessment.
Design
This was a community-based participatory research project (Minkler, Wallerstein, & Hall, 2003) in which researchers, Task Force members, and other community members collaborated to plan and conduct a baseline assessment to understand how agencies/programs currently address LGBT IPV. We surveyed professionals affiliated with one or more IPV prevention networks in Los Angeles. This evaluation of ongoing programmatic activity was reviewed by the appropriate institutional review board and deemed exempt from human subjects review.
Recruitment
Respondents were enrolled using purposive and snowball sampling. An e-mail request was distributed to all persons affiliated with the city and county domestic violence prevention and intervention networks, and the county’s network of mental health providers. Members of these networks represent diverse organizations that work directly with persons affected by IPV (e.g., police, domestic violence shelters) or that advocate on their behalf (city attorney’s office). The e-mail explained that the purposes of the survey were to help the city better understand the domestic violence prevention/intervention needs of LGBT persons and improve the city’s capacity to provide prevention/intervention services and resources to the LGBT community. Network members could forward the e-mail to other professionals not affiliated with these formal networks.
Data Collection
Data were collected online using the Internet- based resource SurveyMonkey (1999). Online surveys represent low cost options for data collection. They also promote a sense of anonymity, which is important if respondents might disclose sensitive information (e.g., that might jeopardize their job). By clicking on a link provided in the introductory e-mail, recruits were transferred immediately to the questionnaire. They provided informed consent and self-administered the instrument, which took approximately 20 to 30 minutes to complete.
Instrument
Prior to data collection, we pretested the questionnaire. As part of pretesting, we conducted cognitive testing with four volunteers to explore the readability, comprehension, and validity of questionnaire items. Cognitive testing is an interview technique in which respondents “think aloud” in the presence of the investigator and discuss their understandings of each item as they complete the questionnaire. Only minor modifications resulted from the pretesting.
An extensive assessment of agencies/programs was not possible; nevertheless, the PRECEDE/PROCEED planning model (Green & Kreuter, 2005), which is widely used to plan, implement, and evaluate health promotion and disease prevention programs, guided the project in three important ways. Following community-based participatory approaches, academic and community partners shared in all decision making. We defined the outcome of interest as optimized provision of LGBT IPV prevention/intervention services and resources through available agencies/programs and conceptualized the determinants of this outcome as occurring on multiple socioecologic levels. Finally, we used the PRECEDE portion of PRECEDE/PROCEED to guide the development of the 33-item questionnaire.
PRECEDE, which stands for predisposing, reinforcing, and enabling constructs in educational/ecological diagnosis and evaluation, generally involves the systematic collection of information (both qualitative and quantitative) from diverse sources to understand a problem and implement a program to address it. In this brief assessment, questionnaire sections corresponded to PRECEDE’s assessment phases; literature reviews and key informant perspectives contributed information at each phase of the assessment. Phase 1 (social diagnosis) characterized the LGBT community and the nature of IPV prevention/intervention services, resources, and staff in Los Angeles. Phase 2 (epidemiologic diagnosis) explored the problem of LGBT IPV. Phase 3 (educational and ecologic diagnosis) explored risk factors and environments influencing LGBT IPV prevention/intervention. Phase 4 (administrative and policy diagnosis) focused on organizational, administrative and policy factors influencing LGBT IPV prevention/intervention services. Toward Phase 5 (Implementation), we obtained recommendations for improving service provision for LGBTs. Though most questionnaire items were closed ended, nine open-ended items and several follow-up items (e.g., “if yes, please describe”) assessed additional details.
Statistical Analysis
Descriptive statistics (i.e., frequencies, proportions, means) were obtained for the overall sample and by categories (e.g., respondents affiliated with non-LGBT vs. LGBT agencies/programs). Simple textual analysis was used to identify main themes in open-ended responses. The analyses were completed using SurveyMonkey’s analysis functions.
Results
Fifty-four respondents completed the questionnaire. Table 1 lists selected individual and agency/program characteristics of the sample. Respondents’ occupations included frontline professionals, managers, and others (e.g., lawyers). Respondents listed all of the networks with which they were affiliated. The greatest proportion were affiliated with the county-wide IPV prevention/intervention network; nearly three of five were also affiliated with the city network. Although six were from agencies/programs whose primary client population is the LGBT community, our findings focus on responses from non-LGBT affiliates except where otherwise stated.
Respondent and Agency/Program Characteristics

NOTE: LGBT = lesbian, gay, bisexual, and transgender.
May not sum to 100% because of missing data.
The sum may exceed 100% as respondents could indicate all of the major networks with which they were affiliated.
Table 2 summarizes the amounts of LGBT IPV experience and training sample members had. Fewer than 10% never worked with LGBTs in the past year. Only 24.4% of non-LGBT affiliates reported that sexual orientation is one of the demographic characteristics routinely assessed via a standard intake form. Many cited policies as a main reason for this:
We have a nondiscrimination policy . . . we do not discriminate for services [sic] or in hiring based on sexual orientation, and all clients receive a list of our policies as part of their orientation.
Experience and Training Assisting LGBT Persons Affected by IPV

NOTE: IPV = intimate partner violence; DV = domestic violence; LGBT = lesbian, gay, bisexual, and transgender; MTF = male-to-female; FTM = female-to-male.
May not sum to 100% because of missing data.
Excludes responses from respondents who work at LGBT organizations.
Respondents could check all that applied.
Excludes responses from persons who work at LGBT organizations.
Of 39 respondents who reported having received specific requests from LGBT clients.
Concerns that asking about sexual orientation might make LGBT clients feel uncomfortable were also noted. One participant explained that space limitations prevent them from asking sensitive questions:
Our [IPV] clinics provide very little privacy and make it difficult for people to feel completely comfortable telling their story—the person sitting at the next desk would be able to hear.
Other respondents, however, indicated that routine assessments of sexual orientation help staff tailor assistance to each client’s needs:
When we provide services to LGBTQ survivors of domestic violence, we are even more alert and cautious of making a detailed assessment of the situation and of the incident.
This respondent did not explain how the more detailed assessments inform service provision or why they are more important for LGBTs than for others.
Whereas all respondents affiliated with LGBT agencies/programs were trained on LGBT IPV (not shown), nearly a quarter (22.6%) of non-LGBT affiliates had received no such training at their current agency/program. Despite this, nearly half of non-LGBT affiliates reported working with LGBTs “sometimes” or “often” in the past year.
The majority (54.1%) of non-LGBT affiliates reported having services/resources at their agencies/programs that were designed for LGBTs (not shown), but when asked to describe these resources, the descriptions generally only connoted referrals to Los Angeles’s LGBT community center. These respondents also believed that most of the assistance (e.g., counseling) they provide is appropriate for all clients, regardless of sexual orientation or gender identity. The following quote is representative of that sentiment:
Everyone is treated the same when they request services. If someone is uncomfortable with our program, we will refer them [sic] to other agencies.
Only two of the many resources non-LGBT organizations reported offering were actually tailored to LGBT persons: a pamphlet on LGBT IPV and LGBT-specific counseling. Most non-LGBT affiliates (92.3%) were unaware of anyone at their agencies/programs with dedicated responsibilities to LGBT IPV (not shown).
Non-LGBT affiliates generally reported feeling, at best, only minimally prepared to work with LGBT clients (Table 2). How prepared they were depended on the subpopulation. They felt less able to assist men than women and less able to assist transgender persons than all others. Those whom the greatest proportion of sample members (50%) felt either not at all or only minimally prepared to assist were female-to-male transgender persons.
The following issues were reported as being particularly important for assisting LGBTs: sensitivity training for all staff, materials/resources designed specifically for LGBTs, safe housing for LGBTs, and LGBT-specific legal assistance (e.g., regarding domestic partnerships or child custody for nonbiological parents).
Table 2 lists the proportions of participants who received requests from LGBTs for specific types of assistance. Less frequent requests not listed in the table included support groups (12.8%), financial assistance (12.8%), case management (10.3%), help with restraining orders (9.8%), and help with law enforcement (7.7%).
Respondents believed organizational and governmental policies can either improve or impede LGBT IPV prevention/intervention service provision; the policies most relevant to LGBT service provision were perceived primarily as impeding it (Figure 1). Respondents perceived gender-neutral policies as improving as well as impeding services for LGBTs. They improve services by allowing LGBTs initial access to general types of assistance; they impede them by not permitting modifications for issues uniquely affecting LGBTs (e.g., gender-specific groups may not protect LGBTs from their abusers).
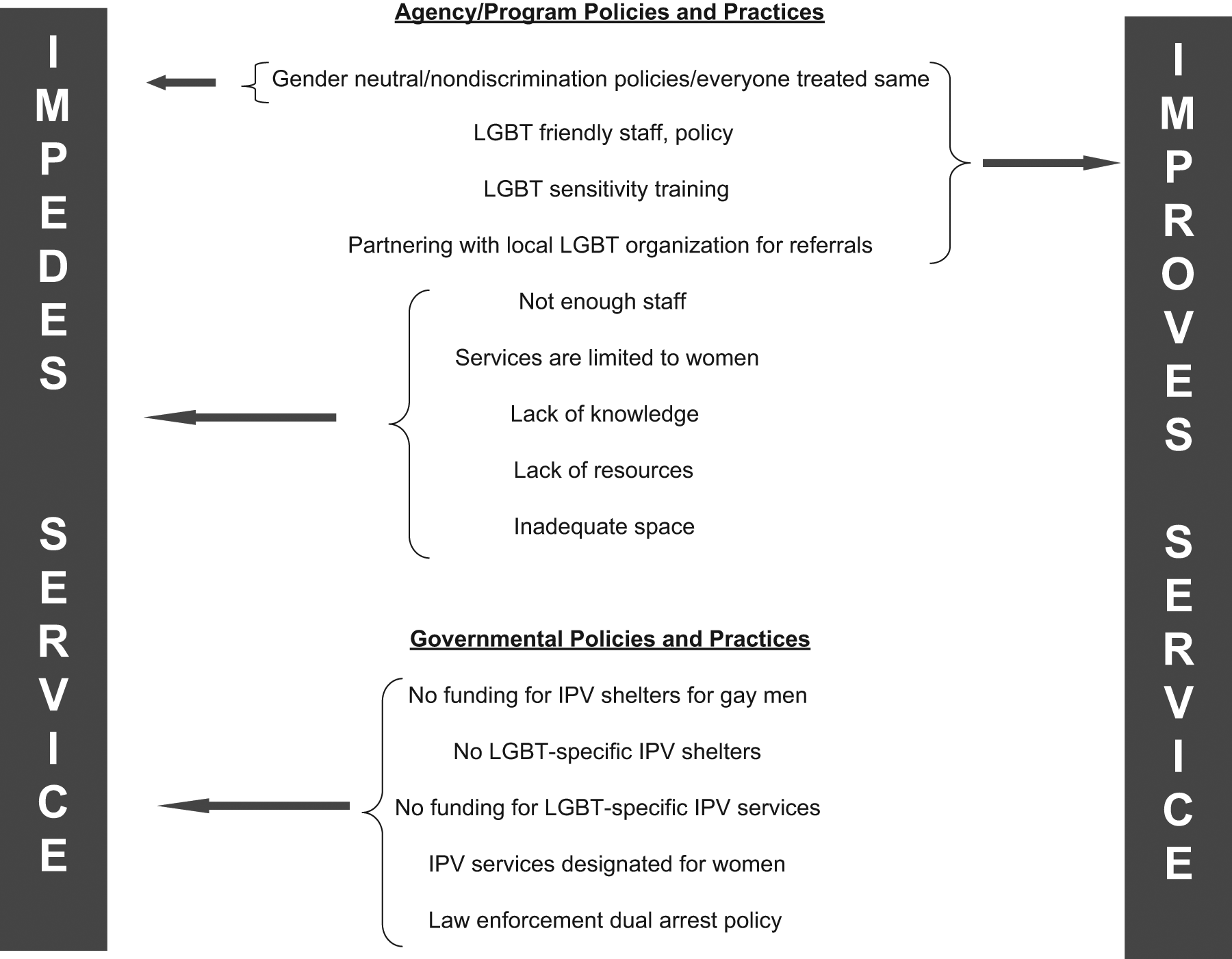
Impact of Policies and Practices on LGBT IPV Service Provision
Some policies were perceived as barriers for one or another LGBT subpopulation but not for all LGBTs. A representative quote follows:
From my knowledge, federal funding to shelters is not inclusive of gay men; therefore, many gay men who are survivors of sexual or domestic violence have a hard time being admitted into a safe place.
Respondents’ recommendations for improving assistance for LGBTs encompassed individual-, organizational-, and community-level factors (Box 1). Requiring staff training on LGBT IPV was frequently reported. The recommendations emphasized the need for LGBT-specific approaches, such as LGBT support groups where the risk of encountering homophobia is minimized and the discussion topics are more relevant to LGBTs.
Recommendations for Improving IPV Prevention Services and Resources for LGBT Persons

NOTE: IPV = intimate partner violence; LGBT = lesbian, gay, bisexual, and transgender.
Discussion
This article presents findings from a brief needs assessment undertaken to explore how agencies/ programs address LGBT IPV and to identify key issues, needs, and challenges staff face in providing IPV-related assistance to LGBT survivors and/or batterers in Los Angeles. The challenges generally are remediable. They include low levels of staff training on LGBT IPV, failure to routinely assess clients’ sexual orientation or gender identity at intake, and agency/program policies or practices that are inattentive to the needs of LGBTs.
Levels of training on LGBT IPV were low overall. All respondents were involved with IPV prevention and/or intervention; nevertheless, they generally felt inadequately prepared to assist LGBTs, especially men and transgender persons. This finding, which is consistent with prior findings of LGBT survivors receiving poor or negative treatment from providers (Merrill & Wolfe, 2000), suggests that the poor treatment may reflect, in part, staff incompetency. Poorly trained staff likely provide unhelpful, inappropriate, or potentially harmful assistance to LGBTs who are already vulnerable because of their abusive experiences (Patzel, 2005). For example, police may arrest battered partners, or shelter staff may unwittingly grant same-sex perpetrators entry to designated safe spaces. Given the low levels of training in this sample, even modest investments in training might substantially boost the quality of LGBT IPV assistance staff are able to provide. Training should include population- and agency-/program-specific considerations. It should teach professionals how to assess sexual orientation and gender identity, how to identify LGBT IPV, and teach them basic cultural competency skills. Improved service should acknowledge and account for LGBT identity when working with survivors, while at the same time not spotlighting it by segregating LGBT survivors.
Few agencies/programs systematically assess sexual orientation or gender identity at intake; therefore, they cannot tailor services to the needs of LGBT clients. The concerns most likely to be overlooked are those that LGBTs uniquely experience (e.g., threat of having sexual orientation or HIV status disclosed to employers; Merrill & Wolfe, 2000). Agencies/programs that do not routinely assess sexual orientation and gender identity may underestimate the true extent to which LGBTs rely on their services. Routinely assessing the sexual orientation and gender identity of all clients can help staff document LGBT service utilization and tailor services and resources for LGBT clients; however, the assessments should only be done by trained staff in LGBT-safe environments (Ard & Makadon, 2011).
Rarely were the services or resources staff reported providing to LGBTs designed to address their unique needs. Service providers encounter challenges working with LGBT clients that do not exist with other clients (Ard & Makadon, 2011). For example, though police are trained to respond to domestic disputes involving IPV, they may have difficulty recognizing it in same-sex domestic disputes (Hassouneh & Glass, 2008; Pattavina, Hirschel, Buzawa, Faggiani, & Bentley, 2007). Even when sexual minority status is known, it can still be challenging for police or other professionals to determine which LGBT partner is the perpetrator and which the survivor. LGBT perpetrators are known to exploit this source of confusion (Bornstein et al., 2006; McClennen, Summers, & Daley, 2002). Failure to distinguish perpetrators from survivors can harm survivors. For instance, although couples counseling typically is not appropriate in abusive relationships because information disclosed during counseling may lead to further abuse, many LGBTs in abusive relationships participate in couples counseling. Therapists often misdiagnose LGBT IPV, which can lead to inappropriately recommending couples counseling instead of one-on-one counseling or “blaming the victim” for relationship dynamics (e.g., suggesting a gay man should “be a man” or hit his male partner back; Kulkin et al., 2007).
LGBT-specific IPV training teaches professionals how to address these issues. In this sample, however, more than 20% had never received LGBT IPV training at their current agency/program; only 17% had participated in a mandatory class. Many felt inadequately prepared to assist LGBT clients, and gender disparities were apparent. Regardless of LGBT subpopulation (i.e., homosexual, bisexual, or transgender), respondents felt less prepared to assist clients who were men. Thus, survivors who are gay men, bisexual men, or transgender persons (either gender) may be particularly disadvantaged when seeking assistance. This is consistent with the limited prior evidence available; however, to truly understand the implications for LGBT IPV service provision requires much deeper exploration of these issues among LGBTs. The next phase of this project, an extensive mixed-methods study, uses qualitative and quantitative methods to explore issues surrounding LGBT IPV and prevention/intervention services among those whose perspectives matter most: LGBT survivors and batterers.
A substantial proportion of non-LGBT affiliates reported relying on the city’s LGBT community center, especially its domestic violence prevention/intervention programs, for secondary support with LGBT clients. They refer LGBT survivors to the Center and obtain LGBT sensitivity trainings. When, as is true in Los Angeles, LGBT centers have dedicated IPV prevention/intervention programs, these partnerships can be beneficial, especially for the non-LGBT agencies/programs and their clients. The partnerships must strive for balance, however, between ensuring that publicly available resources meet the needs of LGBTs and building the capacity of LGBT centers to assist non-LGBT organizations. Some LGBTs prefer obtaining assistance outside the LGBT community, particularly if the community is small, they share a social network with the perpetrator, or the LGBT community does not provide IPV-related assistance (Bornstein et al., 2006; Turell & Herrmann, 2008). In these circumstances, referrals to LGBT centers are not recommended.
Organizational and governmental policies and practices should be reviewed to make certain they accommodate, rather than ignore, differences by sexual orientation and gender identity (Ford, 2006). Agencies/programs may inadvertently overlook issues that are salient to LGBTs (Ristock, 2002). Gender-neutral policies imply equal access for all; however, they neglect concerns unique to LGBTs (e.g., risk of abuser being in the same shelter as the survivor). Some policies disproportionately affect only certain LGBT subpopulations (e.g., gay men).
Practice and Policy Implications
Even where gender-neutral policies were in place, respondents felt inadequately prepared to assist LGBTs, especially men and transgender persons. LGBT IPV training (and refresher sessions) should be required of all staff and be provided by dedicated LGBT IPV prevention programs.
Unless services and resources appropriately address the kinds of issues that uniquely affect LGBTs (e.g., perpetrators controlling HIV medications or accessing gender-specific safe spaces by pretending to be the victim), agencies/programs will inadvertently overlook important issues for this population. They can begin by routinely assessing the sexual orientation and gender identity of all clients at intake. This will allow staff to tailor resources to clients’ needs, obtain feedback for quality improvement, and document LGBT service utilization.
There are several limitations. This was a small, nonprobability sample, which limits the generalizability of the findings. The findings are not generalizable to nonurban areas and cities with small LGBT populations or few legal protections for LGBTs. Though an extensive assessment was beyond the purview of the original charge, more qualitative data (especially from LGBTs) would have enriched the findings. The findings do offer important guidance for the next phase of this work, which focuses on LGBTs affected by IPV. The self-reported data reflect perceived not official policies. It is likely, however, that perceived policies better reflect practices. Some participants skipped items, which affected the number of complete responses per item.
Strengths include the identification of basic issues that, if addressed, might efficiently enhance the capacity of agencies/programs to assist LGBT survivors. The sample comprised service providers and other professionals who work directly with or advocate on behalf of battered persons. Therefore, the findings reflect staff’s direct interactions with clients and firsthand experiences within relevant agencies/programs.
In conclusion, to improve IPV prevention/ intervention services and resources for LGBTs requires attention to staff-related, organizational and policy considerations. We offer the following recommendations: Routinely train staff on LGBT IPV issues, ensure adequate resources (i.e., funds, space) to address LGBT IPV, develop LGBT-specific resources as appropriate, and ensure that policies accommodate the needs of LGBTs.