
Abstract
Health Compass is an innovative, multiphased project that aims to transform health care practice and shift organizational culture by building the capacity of Provincial Health Services Authority (PHSA) health care providers to further promote the mental health and well-being of patients and families accessing PHSA’s health care services. Health Compass was developed within a health promotion framework, which involved collaboration and engagement with stakeholders across all partnering PHSA agencies. This approach led to the development of an educational and training resource that contributes to increased capacity for mental health promotion within the health care setting. Based on interviews with Health Compass’ internal Project Team and findings from a Stakeholder Engagement Evaluation Report, this article outlines the participatory approach taken to develop the Health Compass Mental Health Promotion Resource and E-Learning Tool. A number of key facilitators for collaboration and engagement are discussed, which may be particularly applicable to the implementation of a mental health promotion program or initiative within a complex health care setting.
Keywords
Introduction
Health Compass is an innovative, multiphased project that aims to transform health care practice and shift organizational culture by building the capacity of Provincial Health Services Authority (PHSA) health care providers to further promote the mental health and well-being of patients and families accessing PHSA’s health care services. The primary role of PHSA, located in British Columbia (BC), Canada, is to ensure that BC residents have access to a coordinated network of high-quality, specialized health care services delivered through provincial agencies and province-wide programs and services (www.phsa.ca). BC Mental Health & Addiction Services, one of PHSA’s agencies, is leading Health Compass in partnership with other PHSA Agencies: BC Cancer Agency, BC Centre for Disease Control, BC Children’s Hospital and Sunny Hill Health Centre, and BC Women’s Hospital and Health Centre.
Health Compass was developed within a health promotion framework, which involved collaboration and engagement across all partnering PHSA agencies. This approach led to the development of an educational and training resource that contributes to increased capacity for mental health promotion (MHP) within the health care setting. Based on interviews with the internal Project Team, and supported by findings from a Stakeholder Engagement Evaluation Report, facilitators to and benefits of collaboration and engagement within a complex health care system are discussed.
Background
Mental health is an integral component and important determinant of quality of life and overall health and well-being of individuals, communities, and society (Herrman & Jané-Llopis, 2005; World Health Organization [WHO], 2004). MHP aims to enhance the capacity of individuals and communities to take control over their lives and improve their mental health and overall well-being (Barry & Jenkins, 2006; BC Ministry of Health, 2007; Jané-Llopis, Barry, Hosman, & Patel, 2005; Keleher & Armstrong, 2006), and is increasingly being seen as a key focus in public health worldwide (Herrman, Saxena, Moodie, & Walker, 2004; WHO, 2004). The development of mental health–promoting health care systems is essential to promoting the mental health of a population, as such a system reinforces the multifactorial nature of health and encourages holistic clinical engagement (WHO, 2004). A mental health–promoting health care system, however, relies on investment in workforce capacity development (Barry & Jenkins, 2006). Continued education and training are key components to building capacity among health care providers to ensure that evidence-informed MHP is effectively incorporated into practice and service delivery (BC Ministry of Health, 2007; Jané-Llopis & Anderson, 2005).
Building on the evidence supporting the development of a mental health–promoting health care system through capacity-building efforts, Health Compass conducted focus groups with PHSA frontline health care providers, leaders, and middle and senior management as well as with patients and families to assess the current state of MHP within PHSA’s health care services. Findings from the focus groups revealed that PHSA health care providers and leaders lacked the confidence, skills, and capacity to address the mental health and well-being of patients and families and that further education and training were required. Focus group participants also identified e-learning (also known as online computer-based educational training) as the preferred learning modality. Benefits of e-learning include efficient and effective delivery of education materials, convenience and portability, flexibility, higher retention, greater collaboration, cost savings, and global opportunities (Childs, Blenkinsopp, Hall, & Walton, 2005; Nelson, 2003; World Wide Learn, 2013).
In response to these findings, Health Compass was established. Health Compass aims to increase the capacity of PHSA health care providers to promote the mental health and well-being of patients and families, and consists of a four-module, hard-copy MHP Resource (hereinafter referred to as the “Resource”) and an accompanying MHP E-Learning Tool (hereinafter referred to as the “E-Learning Tool”). The interactive and learner-driven Resource and E-Learning Tool include the following modules: Module 1: Mental Health Promotion Concepts and Principles; Module 2: Communicating to Empower; Module 3: Healthy Teams and Mental Well-Being; and Module 4: Healthy Organizations and Mental Well-Being.
Within this overarching health promotion framework, a foundational health promotion principle adhered to during the development of the Resource and the E-Learning Tool was participation, as participation has been found to be a key means of sustaining health promotion action (WHO, 1998). Participation can be understood as a core underlying philosophy of inclusivity and of recognizing the value of engaging those who are intended to be beneficiaries, users, and stakeholders (Cargo & Mercer, 2008). Two central participatory strategies are used within Health Compass: (a) collaboration within formal structures (collaboration includes activities such as sharing of planning, making decisions, setting goals, and working together cooperatively; Gardner, 2005) and (b) engagement with stakeholders (with engagement being defined as the process of working with groups of people to address issues affecting the well-being of those people; Centers for Disease Control and Prevention, 1997).
Such participatory strategies have been found to provide opportunities for discussion of an issue from various perspectives, for increased empowerment, and for innovative solutions to be discovered beyond what an individual person or organization could achieve (Jolley, Lawless, & Hurley, 2008). Furthermore, collaboration has been found to be particularly effective in accomplishing system-wide practice change in complex settings (Reinhardt & Keller, 2009). Given the diversity of mandates, services, and populations served by the PHSA agencies, collaboration and engagement were considered crucial to effecting practice change across the health care system.
Method of Development
Throughout development of the Resource and the E-Learning Tool, a number of formal structures for collaboration and processes for engagement were put in place. These structures and processes were overseen by an internal Project Team, who provided project management, content expertise, and executive leadership for Health Compass.
Structures to Foster Interdisciplinary Collaboration
Health Compass collaborated through formal structures with frontline health care providers, leaders, middle and senior management, and MHP experts. Developing formal structures and roles is critical for effective collaboration within health promotion initiatives (Barry & Jenkins, 2006; Delaney, 1994). The structures that were put in place to support collaboration included a cross-PHSA Agency Steering Committee, a cross-PHSA Agency Advisory Committee, and an external expert Reference Group. The Steering Committee was composed of learning and development leads, clinical education and training leads, professional practice leads, public health experts, and researchers. Steering Committee members acted as liaisons between Health Compass and their respective PHSA agency by guiding project implementation. The Advisory Committee was comprised of an interprofessional group of frontline health care providers and leaders from the partnering PHSA agencies. Advisory Committee members were key partners in developing the content and ensuring practical and clinical relevance. The external expert Reference Group was composed of national and international experts in the field of MHP, and provided MHP content expertise and guidance on the adaptability of Health Compass for other health care contexts.
Processes to Foster Engagement
Health Compass continually engaged with the intended beneficiaries, users, and stakeholders through processes including focus groups, interviews, consultations, and pilot testing. During Phase 1 (September 2009-July 2010), key informant interviews and focus groups were held with 124 PHSA frontline health care providers, leaders, and middle and senior management from all partnering PHSA agencies to assess the current state of MHP within PHSA’s health care services. Building on Phase 1 findings, the Resource and the E-Learning Tool were developed during Phase 2 (August 2010-January 2012) with project committees. During Phase 3 (February 2012-March 2012), Phase 1 participants and other health care providers and leaders participated in the pilot test for the E-Learning Tool. During pilot testing, 92 health care providers representing all partnering PHSA Agencies provided feedback to further enhance the relevance and applicability of the Resource and the E-Learning Tool. Throughout development, Health Compass further engaged key internal stakeholders, including PHSA Strategic Human Resources and PHSA Aboriginal Health, as well as diverse population groups of patients and families to better understand their perspective on mental health–promoting health care systems and to inform development.
Evaluation of the Resource and the E-Learning Tool
An Evaluation Framework and Protocol was developed for all three phases of project development. Evaluations were conducted to (a) assess increased MHP capacity across PHSA agencies, (b) assess the perceived quality and feasibility of the Resource and the E-Learning Tool, and (c) explore the degree of stakeholder participation in the development of the Resource and the E-Learning Tool. Increased MHP capacity was assessed, using the competencies of knowledge, attitude, and skills related to MHP as indicators, through a pre- and posttest questionnaire during pilot testing. To explore the quality and feasibility of the Resource and the E-Learning Tool and the degree of stakeholder participation, a qualitative evaluation was carried out by external evaluation consultants (Legare, Rootman, & Wilson, 2012). For this evaluation, a total of 18 individuals from the Steering Committee (n = 6), Advisory Committee (n = 9), external expert Reference Group (n = 2), and Phase 1 (n = 1) participated in semistructured, in-person interviews. The data were analyzed using an inductive, conventional content analysis, in which the researcher developed codes and themes from the data (Hsieh & Shannon, 2005). A final evaluation report (hereinafter referred to as the “Stakeholder Engagement Evaluation Report”) was provided to the internal Project Team in February 2012.
Interviews With the Internal Project Team
At the end of Phase 3 (March 2012), semistructured, in-person interviews were conducted by the first author with all three members of the internal Project Team (consisting of the Project Manager, Project Lead, and Executive Lead) to explore facilitators to and benefits of participation (collaboration and engagement) during all phases of development. Throughout the interview process, the interview guide that was initially developed was adapted in response to participant responses, based on Dahlgren, Emmelin, and Winkvist’s (2007) adaptive interviewing processes. Inductive, thematic analysis was used to identify, code, categorize, analyze, and report themes within the data, with the themes identified being strongly linked to the data (Braun & Clark, 2006). The process of analyzing data centered on coding data into categories through constant comparison, with the categories being conceptualizations of key aspects of the data. Three phases of coding, identified by Strauss and Corbin (1990; as cited in Dey, 2004), were conducted: open coding (breaking down and categorizing data), axial coding (putting data back together in new ways by making connections between categories), and selective coding (selecting the core category and systematically relating to other categories). These findings are reported below in the Results and Discussion section, along with findings from the Stakeholder Engagement Evaluation Report, as they support and relate to the generated themes from the internal Project Team interviews.
Results and Discussion
Themes generated from the interviews with the internal Project Team are discussed below, and relate broadly to (a) facilitators to and (b) benefits of collaboration and engagement, key participatory strategies within health promotion initiatives. In addition, these results are discussed as they relate to and extend the current health promotion literature.
Facilitators to Collaboration and Engagement
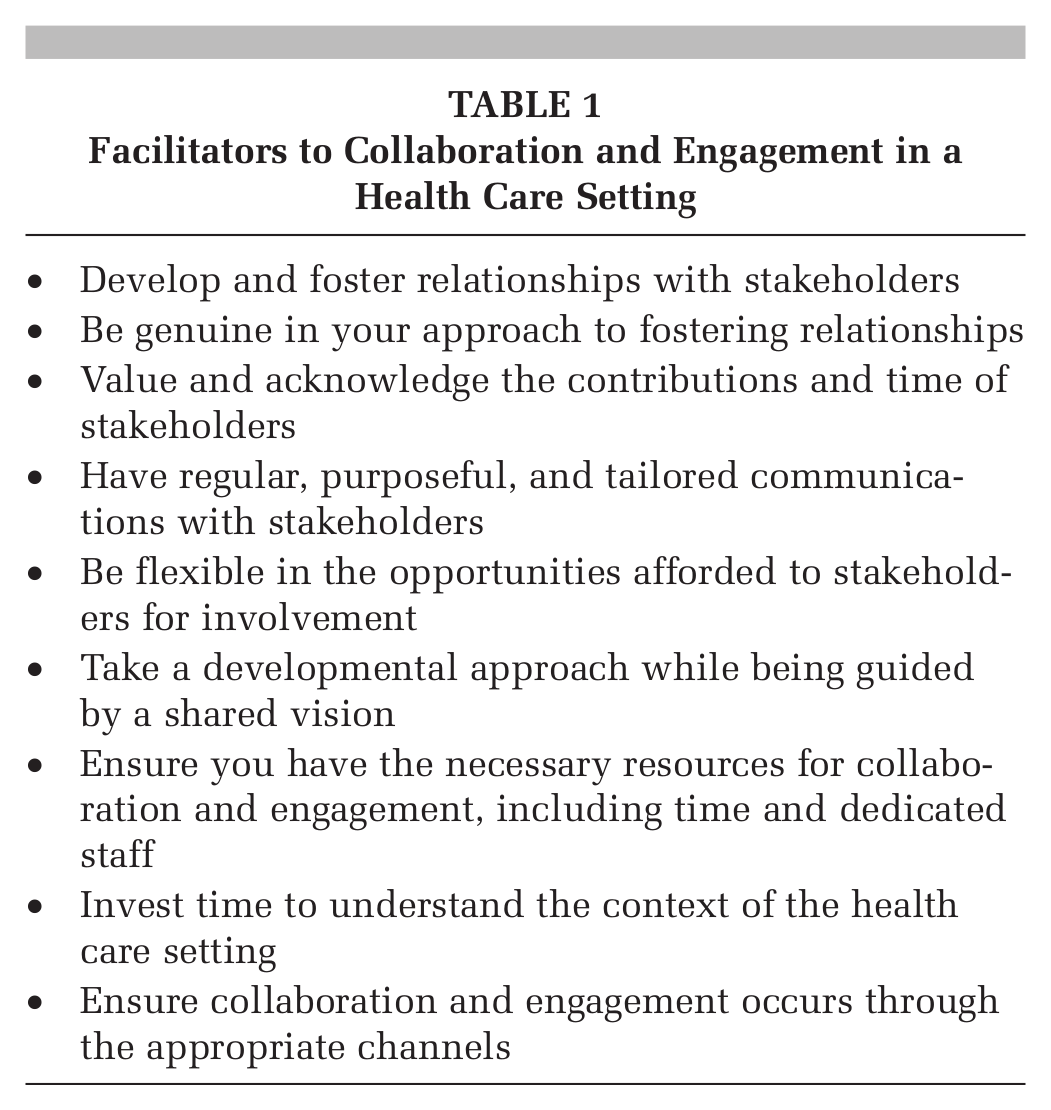
A number of facilitators were discussed by the internal Project Team as contributing to effective collaboration and engagement in the development of the Resource and E-Learning Tool. These facilitators are summarized in Table 1, and broadly include the following: (a) fostering relationships and valuing the contributions of stakeholders, (b) taking a developmental approach while maintaining a shared vision, and (c) having the necessary resources to effectively collaborate and engage.
Facilitators to Collaboration and Engagement in a Health Care Setting
Fostering relationships and valuing contributions
For the internal Project Team, a key facilitator to effective collaboration and engagement was the fostering of relationships, which involved being genuine and valuing the contributions and time of stakeholders. Although considered a key facilitator, fostering relationships was also recognized as something that took both time and energy by the internal Project Team, involving regular and purposeful communication, and flexibility with regard to opportunities for involvement. For instance, it was noted by an internal Project Team member that
it takes time . . . follow up e-mails, phone calls, one-on-one meetings . . . to show that I valued and appreciated the folks that were on board with us . . . that constant engagement was so key to ensuring somebody might come back to the next meeting.
A key aspect of valuing contributions was demonstrating to stakeholders that their involvement affected the final Resource and E-Learning Tool.
The internal Project Team spoke to the importance of being genuine in these relationships, with one internal Project Team member discussing how it was important for the Team members to be themselves:
Recognizing there are different ways to collaborate, and being genuine . . . and connecting with people in that way. Because if you’re sending out thank-you messages and that’s not who you are, they’re going to know that that’s fake . . . whereas if you do something that’s more true to yourself but still shows that you value somebody, that comes across.
Within the Stakeholder Engagement Evaluation Report, stakeholders discussed how feeling valued was cultivated by continual communication and flexibility in opportunities to be involved, with one stakeholder stating that “there were lots of opportunity for feedback and interaction—[the Project Team were] willing to make it work for us.” Findings from this report also revealed that stakeholders felt valued when it was clear that their contributions were affecting and shaping the Resource and the E-Learning Tool (Legare et al., 2012).
Exploration with a vision
The internal Project Team discussed how a key facilitator to collaboration and engagement was taking a developmental approach (i.e., being flexible and iterative) while at the same time having a shared vision with stakeholders. As noted by one Project Team member: “The developmental approach . . . really does allow for meaningful engagement because you are shaping the process as you go.” The internal Project Team found that although the developmental approach was necessary for meaningful participation, having a shared vision was equally important, as having a shared vision was found to contribute to a sense of joint ownership for the Resource and the E-Learning Tool. One Project Team member stated,
While we didn’t know what we were going to create we always had a vision of what we wanted to achieve . . . those are the two pieces to get people on board is not being so stuck on what you’re going to do but have a clear vision of where you’re going to go . . . that really is the stepping stone for collaboration.
A similar theme was discussed within the Stakeholder Engagement Evaluation Report, with a key finding being that the developmental approach allowed Committee members to take the prime role in determining the content and format of the Resource and the E-Learning Tool, allowing for meaningful input and tailoring of the best evidence to suit the unique needs of PHSA health care providers and the unique contexts of the diverse PHSA Agencies (Legare et al., 2012).
Having appropriate resources
For the internal Project Team, having an appropriate amount of time and dedicated staff was cited as a key facilitator. As discussed by one Project Team member: “We spent a whole year listening to people and building relationships, and that is a luxury in health care . . . by actually doing that you’re going to have something that people use and own.” In addition, the internal Project Team also stressed the importance of taking the time to understand the context of the organization and ensuring that participation occurred through appropriate channels within each PHSA agency. For example, when speaking about the time it took to prepare for Phase 1, one internal Project Team member noted,
It took awhile to work with the health authority to make sure they were a part of the process . . . I had to learn the organizational structure and landscape of each [PHSA] agency and work very differently with each agency.
Within the Stakeholder Engagement Evaluation Report, having an appropriate amount of time, although challenging for many stakeholders, was also cited as a key facilitator to collaboration and engagement. This was most often discussed in terms of the time required to respectfully incorporate the perspectives of multiple participants in Committee meetings, as well as the time required to attend meetings and review documents (Legare et al., 2012).
Benefits of Collaboration and Engagement
Findings from the interviews with the internal Project Team suggest the following benefits of collaboration and engagement: (a) development of a more relevant and comprehensive Resource and E-Learning Tool, (b) increased likelihood of uptake and sustainability, and (c) personal growth and gain.
A more relevant and comprehensive Resource and E-Learning tool
The internal Project Team felt that the participatory strategies of collaboration and engagement contributed to a more relevant and comprehensive Resource and E-Learning Tool. One Project Team member noted that because they “had everybody on board . . . what we got was a resource and a [e-learning] tool where the content is practical and relevant across [PHSA] Agencies.” A key component of ensuring the relevance of the Resource and the E-Learning Tool for frontline health care providers, and for PHSA as a whole, was aligning the content with existing PHSA initiatives and with professional competency development frameworks. Within the Stakeholder Engagement Evaluation Report, stakeholders also described how collaboration and engagement were necessary and highly valued and contributed to the development of a more comprehensive and relevant resource than would have otherwise been created (Legare et al., 2012).
Increased uptake and sustainability
The internal Project Team felt strongly that collaboration and engagement contributed not only to the relevance of the Resource and the E-Learning Tool but also to an increased likelihood of successful uptake and sustainability. As stated by one Project Team member, “I think if we hadn’t gotten to that place [making the content relevant], there’s no way we would have the uptake we have currently.” Within the Stakeholder Engagement Evaluation Report, a similar finding was reported, with stakeholders discussing how they felt their involvement would contribute to increased uptake within PHSA and the Agencies. For example, one Committee member noted how the members’ involvement provided valuable feedback for the implementation phase: “I tried to engage people myself with an eye to eventual implementation . . . If this was to land on my desk out of the blue, who would I pass it on to?” (Legare et al., 2012, p. 18).
Personal growth and gain
In addition to directly benefitting the relevance and uptake of the Resource and the E-Learning Tool, the internal Project Team members also noted that they experienced personal growth and gain throughout development. With regard to how they benefited, one Project Team member found that it was “enjoying the small things out of the process, recognizing the benefits to myself out of this . . . I got to meet incredible people.” Another member of the internal Project Team spoke to how the members had grown personally throughout this process: “It’s really about our own development as individuals so we can foster collaboration. You need self-awareness, reflection, good communication.”
This sense of personal growth and gain was also noted among the Committee members, as discussed within the Stakeholder Engagement Evaluation Report, with personal growth resulting both from engagement with the internal Project Team, as well as with other Committee members. For example, Committee members noted how they had developed a better understanding of the similarities across PHSA Agencies:
I learned a lot because of the connections; saw some common threads. People . . . were talking about community—I found it interesting that they were working with community in a setting yet what was being said rang absolutely true for the tertiary care setting I work in. (Legare et al., 2012, p. 15)
Contextualizing Results
The facilitators and benefits discussed are consistent with existing research on collaboration and engagement within health promotion initiatives. For instance, collaboration and engagement have been found to contribute to benefits such as shared ownership, secured commitment, more personalized involvement, more successful implementation of an initiative (Wilson, 2011), and improved outcomes (Jolley et al., 2008; Wilson, 2011). Facilitators for effective collaboration and engagement within health promotion initiatives discussed within existing research are also consistent with the facilitators discussed in this article. These include having an environment where work is valued, having trust and effective communication between partners (Delaney, 1994; Dowling, Powell, & Glendinning, 2004; Jolley et al., 2008), being genuine and flexible in collaborative relationships (Gardner, 2005), having a shared vision (Delaney, 1994; Jolley et al., 2008), and understanding the broader context in which the collaboration is taking place (Delaney, 1994).
This article supports the applicability of these facilitators and benefits for health promotion initiatives. In addition, this article adds to existing health promotion research by suggesting ways in which these facilitators can be adapted and applied to an MHP initiative within a complex health care setting, and how these benefits apply to such initiatives. Lastly, this article discusses additional facilitators and benefits found to be particularly applicable for a unique and complex health care setting.
Conclusion
The participatory approach taken to develop the Health Compass Mental Health Promotion Resource and the E-Learning Tool involved interprofessional collaboration and engagement with stakeholders across PHSA agencies. A number of key facilitators and benefits of the participatory strategies of collaboration and engagement were discussed; these benefits include contributing to the relevance and likelihood of uptake of the Resource and the E-Learning Tool, as well as personal growth and gain for both the internal Project Team and stakeholders. These findings extend the existing health promotion literature on collaboration and engagement and may be particularly applicable to the implementation of an MHP program or initiative within a complex health care setting.