
Abstract
Overweight and obesity are associated with several life-threating comorbidities, including type 2 diabetes and cardiovascular disease. Obesity is a growing health concern in North America, with some groups experiencing higher levels of obesity than others. One group of particular interest is urban Aboriginal youth because they are a quickly growing population who experience high rates of obesity. Obesity is a complex condition with many contributing factors, diet being one of the primary contributors. In this article, we discuss the findings from an ethnographic study that examined determinants of diet for urban Aboriginal youth. Results revealed two themes: (a) Traditions and Sharing, and (b) The Struggle. The findings with Traditions and Sharing showed that food-sharing networks are often used to acquire traditional food. Traditional foods were believed to be healthy and desired by the participants. The theme The Struggle provides insight into the daily challenges the participants faced with food insecurity. Health promotion professionals need to consider the multiplicity of determinants of diet for urban Aboriginal youth in order to plan and implement culturally appropriate health promotion programs.
Keywords
Introduction
Obesity is associated with several life-threatening morbidities, including type 2 diabetes and cardiovascular disease (Poirier et al., 2006). There is growing concern with the increasing rates of obesity for Indigenous Peoples globally (Garriguet, 2008; Kuhnlein et al., 2006). In North America, obesity rates are high regardless of ethnicity; however, for Aboriginal Peoples in Canada and for Native Americans, rates are substantially higher than in non-Aboriginal and White non-Hispanic populations (Jernigan, Duran, Ahn, & Winkleby, 2010; Public Health Agency of Canada [PHAC] & Canadian Institute for Health Information [CIHI], 2011). Furthermore, rates of obesity for Aboriginal and Native American youth are considerably higher than in their non-Aboriginal and non-Native counterparts (Fagot-Campagna et al., 2000; PHAC & CIHI, 2011). This is alarming, as youth who are obese are at risk to acquire many chronic diseases, leading to a lifelong struggle with health issues and a lower quality of life (Dehghan, Akhtar-Danesh, & Merchant, 2005).
Aboriginal Peoples of Canada are unique, both historically and culturally. In Canada, the term Aboriginal Peoples refers to First Nations, Métis, and Inuit People (Constitution Act of Canada, 1982). The differences within these groups are great and are related to having or not having treaty status, geography (remote, rural, on-reserve, and urban), and jurisdiction (federal, provincial, and band; Smylie & Anderson, 2006). The Aboriginal population in Canada has increased by 20% over the past 5 years, compared to 5% for non-Aboriginal Canadians (Statistics Canada, 2012). This rapidly growing Aboriginal population is becoming increasingly urban; more than half of all Aboriginal Peoples in Canada live in cities (Statistics Canada, 2012).
This young, quickly growing, and increasingly urban population has experienced large changes in diet over the past half-decade. Their diet has shifted from a traditional diet to a more Western diet, which is often lower in nutritional quality (Khalil, Johnson-Down, & Egeland, 2010; Ng, Young, & Corey, 2010). Traditional foods are described as culturally accepted foods available from local natural resources that constitute the food systems of Aboriginal Peoples (Willows, 2005). In Canada, common traditional foods are fish, wild game, berries, and other gathered vegetables, fruits, and grains.
There is little documented information about the dietary habits of urban Aboriginal youth, including what determines their food options and choices, or how culture affects their diet (Willows, 2005). Past research has shown that culture is a determinant of Aboriginal Peoples’ diets, including Aboriginal children living in rural or on-reserve First Nations communities (Pigford, Willows, Hold, Newton, & Ball, 2012; Willows, 2005). Aboriginal youth’s lives are often a blend of both modern and traditional lifestyles. The modern realities of Western living are mixed with cultural practices and values. This blending of modern and traditional lifestyles results in dietary determinants that are unique from those of non-Aboriginal youth (Gideon, Gray, Nicholas, & Ha, 2008; Pigford et al., 2012). Despite culture being a known determinant of diet for Aboriginal youth, few, if any, studies have been conducted to better understand the role of culture in the determinants of diet for urban Aboriginal youth.
The purpose of this qualitative study was to examine the determinants of diet for urban Aboriginal youth with specific emphasis on culture. This research addresses health issues for Indigenous Peoples and promotes linkages between academic institutes and health promotion practitioners. Those working in health promotion or education can use the findings from this research to develop culturally appropriate dietary health strategies that improve health outcomes for this unique group.
Method
Conceptual Framework
Health promotion for Indigenous Peoples has been largely ineffective due to external strategies that do not take into consideration the local and cultural ways that Indigenous Peoples understand health (Smylie et al., 2004). This study was informed by a critical Indigenous theoretical framework (Smylie et al., 2009) and assumes that Indigenous systems of health knowledge are unique and epistemologically different than Western systems. Western knowledge systems often decontextualize knowledge from its local context to make it more generalizable (Smylie et al., 2009). The critical Indigenous theoretical framework also posits that Indigenous Peoples’ health behaviors are formed through a mixing of precolonial systems of health, ongoing colonization, and Western systems of health (Smylie et al., 2009). This translates to complex behaviors that are often rooted in different worldviews. These assumptions were kept in the forefront of the researchers’ thoughts throughout this project and helped inform the methods and the contextualization of the results (Morse & Field, 1995a).
Setting and Participants
This study was conducted at an Aboriginal high school located in a Canadian prairie city. Ethical approval for this study was acquired from the researchers’ University Ethics Board and from the participating school division. Fifteen students in Grades 9 through 12 volunteered to participate in this study (see Table 1). Most participants lived in low-income neighborhoods with one parent or guardian or on their own. Half the participants discussed living on their family’s First Nation at some time, and almost all of the participants visited their family’s First Nation a few times a year.
Participant Demographics

Study Design
This study used a participatory research approach. The Canadian Institutes of Health Research’s Guidelines for Health Research Involving Aboriginal People (2008) were developed to assist researchers in carrying out ethical and culturally competent research involving Aboriginal Peoples. These guidelines stress the need for participatory research. Participatory research facilitates shared power and decision making and can be fostered by strong relationships and reciprocity in the community. The research team had a long-standing relationship with the school, and the researcher conducting the study spent a year at the school volunteering and immersing herself in the culture of the school community prior to data collection. This allowed her to engage in reciprocity by giving back to the school community and to build her own relationships.
During the researcher’s year volunteering at the school, she had heard many students, teachers, and administrators say that body weight issues were of importance to them. After approximately a year, the administrators and teachers interested in collaborating on a research project met with the researcher to formulate a study that would help shed light on body weight issues for Aboriginal youth. It was decided that one important aspect of body weight issues for Aboriginal youth was their diet. The group of teachers and administrators were interested in what their students thought about culture, traditional food, contemporary food, and living in a city. The researcher designed questions to ask in interview settings and informal conversations, and school leaders reviewed the interview questions prior to being used in the field.
The teachers and administrators from the school who were engaged in the study design believed that giving the participants options on how they wanted to participate in interviews was important. Options to be interviewed in one-on-one interviews or as focus groups were offered because it was believed that some students might have been more comfortable sharing in a group setting, whereas others might have preferred a more private one-on-one interview. All participants chose one-on-one interviews apart from two young women who, at their request, were interviewed together. Directly after interviewing took place, the audio-recorded interviews were transcribed verbatim into electronic word documents.
Ethnography was the methodology chosen for this study. An ethnographic study describes how a cultural system influences human behavior (Morse & Field, 1995a). In health sciences, ethnography is a means of gaining access to the health beliefs and practices of a culture (Morse & Field, 1995a). Relationships are a critical aspect of ethnography. The researcher was already immersed in the community and had built strong relationships with students and teachers through assisting in classrooms and running after-school programming. The strong relationships developed facilitated participant trust and openness, which led to insightful and rich information.
Data Collection
Participants were recruited through classroom canvasing, information sessions, and snowball sampling (Patton, 2002). All participants signed a student assent form and had parents or guardians sign a consent form if they were younger than 18 years. Interviews took place at lunch or after school and were conducted in an unused classroom. Questions discussed topics such as healthy foods in Aboriginal culture, definitions of health foods, and traditional foods (see Table 2; type, procurement, and healthfulness). Students were also asked about enablers and barriers to food security (social environment, built environment, and finances).
Interview Questions Relevant to Determinants of Diet
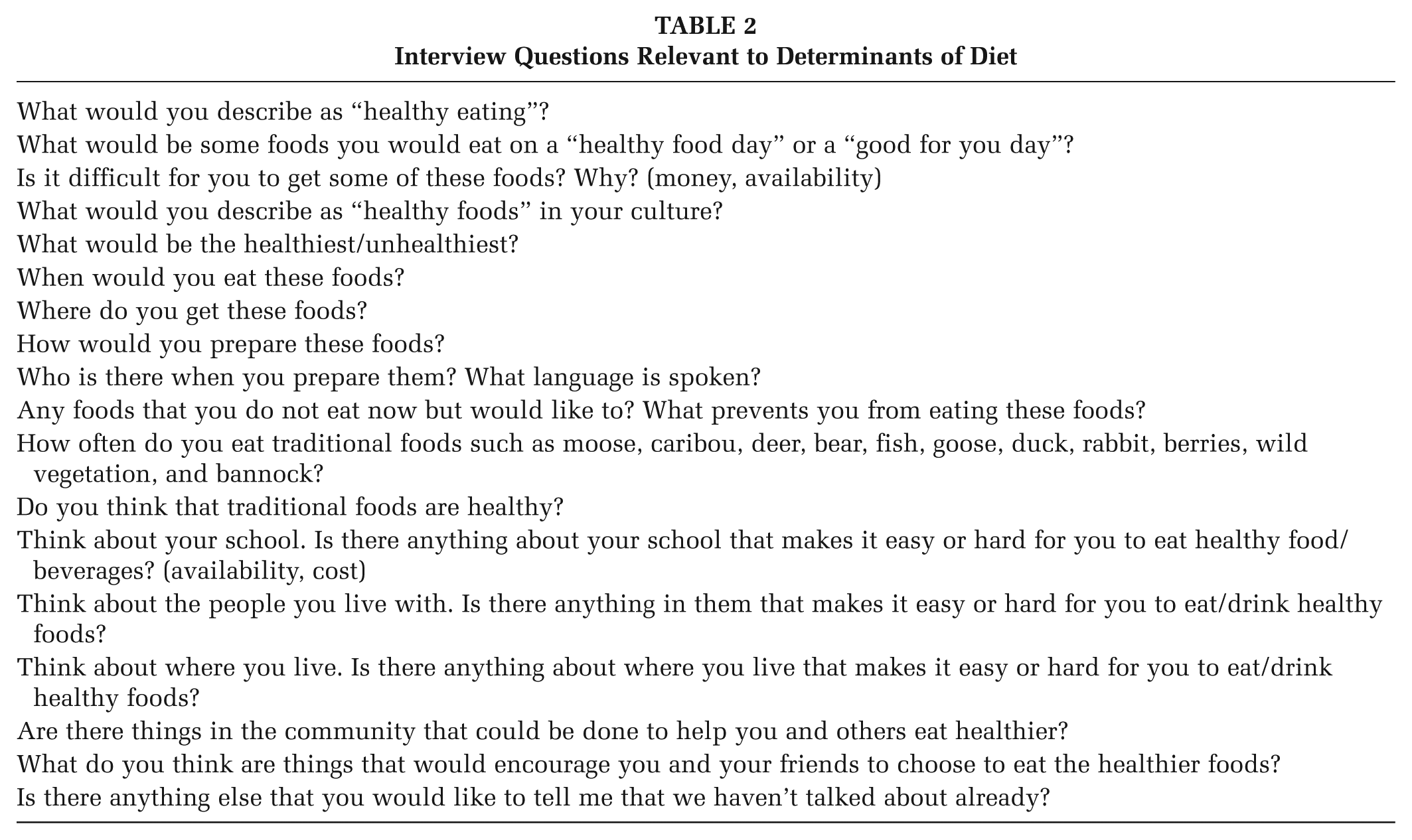
Each interview lasted approximately 45 minutes. After the interview, each participant received a $10 gift card for a healthy food vendor. The school principal suggested giving gift cards because it is customary to give a gift when you seek knowledge from an Aboriginal person, regardless of age.
Informal conversations and participant observation were also a source of data in this study (Patton, 2002). These conversations with teachers, staff, and students took place during more natural social interactions, such as in the lunchroom, in the office, or after class. Conversations were recorded in field notes. Observations of participants and other students at the school took place during lunch, after school, in class, and in the hallways and were also recorded in field notes.
Data Analysis
Data were analyzed according to the recommended analysis procedures for qualitative data (Morse & Field, 1995b). Data analysis started at the initiation of this study and continued throughout. Pieces of the interviews and field notes were categorized by coding for key words, phrases, and topics by the researcher (Morse & Field, 1995b). Phrases such as “I feel,” “I think,” and “I believe” along with action words such as “I do,” “I eat,” and “I play” were identified and coded. Electronic word documents were used to organize the coded categories. After categories were built, thematic analysis began. Thematic analysis involves the seeking out of common threads throughout the results (Morse & Field, 1995b). For this study, the categories that emerged from the coding were analyzed along with each transcript in its entirety to form the themes. Once themes were developed, another member of the research team with expertise in qualitative research checked the coding and themes.
Member checking was done with each participant once analysis began. The researcher and the participant got together privately to go over what the participant told the researcher, and the researcher shared with the participant how she was interpreting the data. Themes were checked by the participants in a talking circle at the end of the study. Talking circles are a method of discussion that can be comforting to Aboriginal research participants, because the circle has a long tradition in Aboriginal culture (Struthers, Hodge, Geishirt-Cantrell, & De Cora, 2003). Specific results from individual interview data were not disclosed during the talking circle. During the talking circle, the researcher explained how specific categories were grouped together to develop the themes. After each theme was discussed, the floor was open for participants to share their thoughts on that theme. Participants verified the themes and expanded on them by explaining how behaviors within the theme were shown by other urban Aboriginal youth who were not in the study, such as friends and siblings.
Results
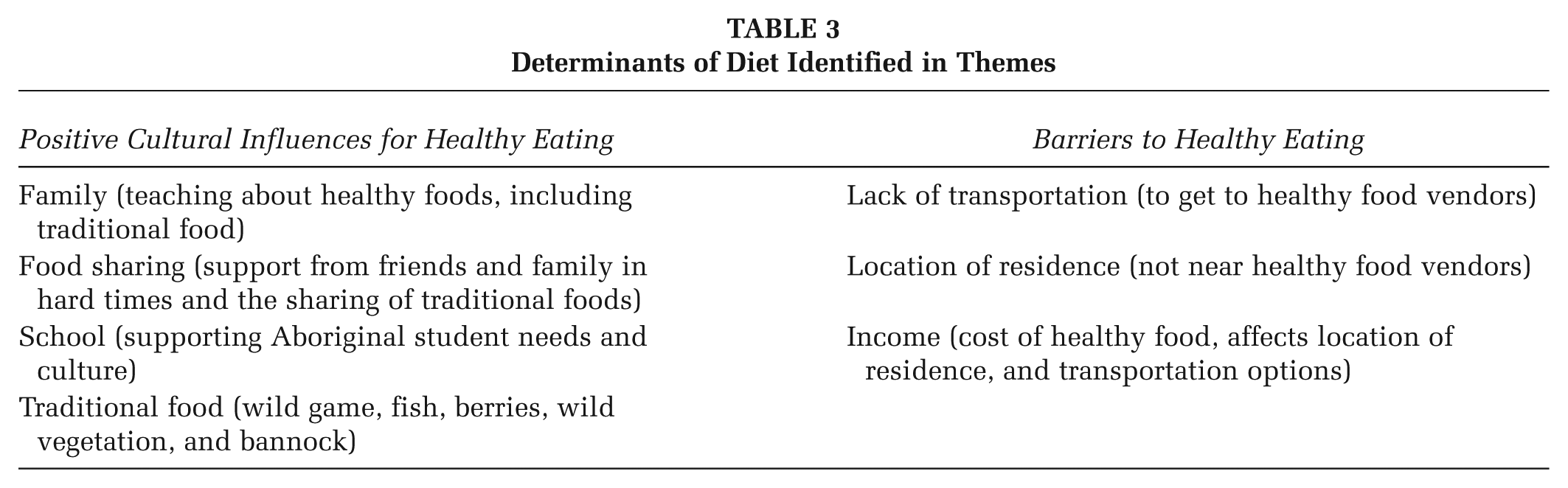
The theme of Traditions and Sharing discusses the role that culture played as a positive determinant of diet. The theme of The Struggle came forth from the data about barriers to healthy eating (see Table 3).
Determinants of Diet Identified in Themes
Traditions and Sharing
The theme of Traditions and Sharing is about the role that culture played as a determinant of diet. The participants discussed several cultural influences on their diets. The influences included traditional food, family, school, and food sharing. All of these influences were rooted in Aboriginal Peoples’ customs and the overarching concept of community sharing (Milburn, 2004).
Participants regularly ate traditional foods and felt they were nutritious, “Because Aboriginal People have always eaten them [traditional foods] and they used to all be healthy.” In addition to believing that traditional foods were healthy, many enjoyed eating traditional foods. The participants who took joy in eating traditional food associated their pleasure with family and culture. For example, participants reported that they enjoyed traditional foods because “That’s what we eat at celebrations and feasts.” Many individuals who liked traditional foods desired to eat more of them. One participant explained, “If I could, I would eat it every day, like wild meat and stuff. That’s why our people lived so long. There was never really anyone overweight. The meat we eat today is full of bad things.”
Many participants noted the influence of their families on their habits and beliefs about traditional foods. The participants whose families regularly cooked traditional foods enjoyed traditional foods, ate them more often, and assisted in the preparation of them. “Mom and Grandma teach me how to make real delicious Indian food. Like different kinds of meats, bannock [A traditional bread baked by Aboriginal Peoples].” Family living on the reserve often sent traditional food into the city for the participants.
As all participants attended an Aboriginal high school, it was no surprise that they reported that the school was a cultural influence. The school hosted many activities where traditional food was served. At such events, important cultural lessons were integrated, such as respecting and serving invited Elders, expressing gratitude for the food through prayer, and sharing and serving food to others.
Because many students came from low-income families, the school provided breakfast and lunch on all school days. This was part of school board policy. The participants had great appreciation for the food they received at school. “The school makes it easier to eat healthier; I get half of my food a day here,” stated one young man. Another young woman said, “The lunch room cooks good healthy food. There’s a lot of vegetables and meat and bread and milk and water.” In addition to the food the students received during the school day, the school cook always made an effort to ensure high-need students took leftover food home. For example, she offered milk to the mothers to take home, and larger quantities of food, such as bulk buns, to the students who had other siblings at home. This offering of food was not part of a school policy but a reflection of the cultural belief held by the Aboriginal cook and school leaders that sharing food is an important way to ensure community health.
Food sharing not only happened at school, it happened in most homes as well. Traditional food sharing was popular among participants’ families. “My uncle hunts and sends us meat,” said one participant. Another explained, “My next-door neighbor goes hunting, and when he has too much meat he gives us some.” In the past, food was gathered not for individuals or families alone but for the benefit of the community. Thus, these methods of food procurement by urban Aboriginal Peoples might be rooted in the ways of their ancestors.
In addition to traditional food sharing, participants discussed sharing to address food insecurity. Food insecurity refers to limited availability of nutritionally adequate, safe, and acceptable foods because of financial constraint (Bickel, Nord, Price, Hamilton, & Cook, 2000). Many participants had experienced food insecurity. Participants discussed “borrowing” food or money for food from family to address food insecurity. “One month we spend all our money on rent and we just had to bum food off my stepmom’s brother and all he had was junk food,” said one participant.
The Struggle
All participants discussed the influence of barriers to healthy eating. The participants often talked of the “struggles” they encountered to healthy eating. All participants identified three barriers to healthy eating: income, location, and transportation.
Income was the most discussed barrier to healthy eating for participants. “I want vegetables and fruits and stuff like that but I can’t fit them in the budget,” said a participant who lived on her own. Another participant who was a mother explained, “You have a budget to go by and sometimes you can’t fit everything in the budget when you go to the grocery store.” She also added, “They [her children] eat, just not what I want them to.” Others who lived with family members stated, “At the end of the month we don’t have enough money for healthy food when we pay bills and rent.” When asked what would help people eat healthier, one participant explained, “Lower the prices on healthy foods. I think that’s what people struggle with the most.”
Participants often used food banks. “It’s hard for some people in the city to eat healthy because in those places that give out food you don’t really get a choice in what you get, you get what they give.” Participants frequently stated the food from the food bank was inadequate. “Sometimes you don’t get very good stuff” and “Its ugly food and expired.”
Participants also explained that their place of residence was a barrier to healthy eating. The low-income neighborhoods where the participants resided were not nearby any grocery stores. Thus, finding transportation to a grocery store was necessary to get healthy food. Many of the participants came from homes where the primary method of transportation was public transit and walking. Participants said that taking the bus “takes a long time,” and they often “had to wait outside for the bus and then pack groceries on the bus.” All of these tasks increased the difficulty of getting healthy food from the grocery store.
Many fast-food restaurants and convenience stores were located close to the participants’ homes. A participant explained, “I live by A&W, McDonalds, KFC, and three other restaurants like that. So it’s pretty hard [to eat healthy], lots of fatty foods.” Another participant illustrated that the problem is not just fast-food restaurants: “I live by a store. That’s where I get chips and pop. It’s a corner store, like a confectionary.” A young man acknowledged that there were some healthy items at the corner stores near his house, but making a healthy choice was a challenge:
You see a whole shelf of chips, and then beside it there is a little one with bread. That does make an impact, even if you do not realize it. Because then you’re looking at the chips even though you need bread.
Discussion
This study’s findings on diet illustrate that although the young participants were living in an urban setting, many had eating practices rooted in traditional Aboriginal beliefs and behaviors. Much of the previous research on this topic has focused on Aboriginal Peoples living on First Nations or in rural locations; this study illustrates that urban Aboriginal youth also feel that traditional foods are healthy and that they desire to eat them. Research is continuing to show that Aboriginal Peoples believe that traditional foods are a healthier option, when compared to prepackaged prepared food (Gittelsohn et al., 1996; Gittelsohn et al., 2010; Pigford et al., 2012; Willows, 2005). Participants’ beliefs that traditional foods are healthy is backed by a growing body of evidence indicating that eating a traditional diet can be healthier than eating nontraditional foods (Kuhnlein & Receveur, 2007; Milburn, 2004; PHAC & CIHI, 2011).
In this study, the participants engaged in food sharing to address food insecurity and to get traditional foods. This is consistent with previous research that found that Aboriginal Peoples engage in the sharing of traditional food and nontraditional food to address food insecurity (Gittelsohn et al., 2010; Willows, 2005). Participants in this study had food-sharing networks to obtain traditional food from their reserves. This highlights the strong desire that these participants have for traditional foods.
Family and school positively influenced the beliefs and behaviors surrounding traditional food for the participants in this study. The school assisted the participants in learning about traditional food. This is consistent with other studies, which have demonstrated that the school is a place that can play an important role in dietary education (Oude et al., 2009).
Previous studies on school nutrition have used The World Health Organization’s health-promoting schools model to integrate curriculum, environment, and community in the nutrition education process (St. Leger, 1999). One such study by Viola (2006) used the health-promoting schools model to integrate a community garden and nutrition education at two Indigenous schools. The author noted that Indigenous communities are complex and dynamic and that this school nutrition program was successful because of the model and the innovation and creativity of the school leaders and researchers (Viola, 2006). Engaging with family was an important aspect of eating traditional food. Recently, Pigford et al. (2012) also found that Aboriginal children’s experiences around traditional food involved nuclear and extended family. Thompson, Gifford, and Thorpe (2000) suggests that for Aboriginal People, family is central to every aspect of food, including choice, preparation, and what it represents.
Although there were many optimistic findings in this study, it is clear that poverty was a barrier to healthy eating. This finding is consistent with the literature on barriers to health for Aboriginal Peoples (Waldram, Herring, & Young, 2006). Thirty-three percent of off-reserve Aboriginal Peoples in Canada experience food insecurity because of lack of money (Willows, Veugelers, Raine, & Kuhle, 2009). These findings indicate that addressing the deeper issue of poverty is a crucial way to address food insecurity for urban Aboriginal youth. Increasing opportunities for urban Aboriginal youth to attain higher levels of education and to have access to more employment opportunities is an important step to addressing poverty.
This study also has important implications for health promotion with other Indigenous youth internationally. The results of this study illustrate very culturally specific beliefs and behaviors. Furthermore, many of the responses given by the young people in this study were tied to precolonial Indigenous beliefs and behaviors, ongoing colonization, and contemporary ways of life (Smylie et al., 2009). This suggests that generalizations from non-Indigenous research should not be made when designing health promotion programming for Indigenous youth.
Conclusions and Recommendations
We believe that health promotion strategies for enhancing healthy eating should focus on the whole family. Having all members of the family work together to build healthy meals and then celebrate by eating together would be a culturally based strategy that could be used in future nutrition interventions for urban Aboriginal Peoples.
This recommendation for family-centered interventions is consistent with the results of a recent review (Schell & Gallo, 2012) that suggested interventions for obesity in Indigenous Peoples should occur at many points in the life cycle as obesity is a multigenerational problem. Many past interventions to improve the diets of Aboriginal Peoples have used a multi-institutional approach, targeting children in schools, adults, local food vendors, and health professionals in a single community (Ho et al., 2008; Saksvig et al., 2005). However, to our knowledge, there has only been one study that specifically focused on family-based intervention strategies with Aboriginal Peoples (Anand et al., 2007). This intervention helped Aboriginal families set and reach dietary goals, and the results showed some positive changes in dietary choices (Anand et al., 2007). Family-based interventions have been successful with non-Aboriginal Peoples in the Mind, Exercise, Nutrition, Do It! Program. This program is a multicomponent, community-based obesity intervention that actually brings children, their parents, and other family members together for educational sessions and workshops on food (Sacher et al., 2010). We believe that this type of strategy may be a good fit for Aboriginal families.
This study illustrated many positive aspects of diet for urban Aboriginal youth. One positive finding was that the Urban Aboriginal participants understood what healthy food was and had a desire to eat it. Thus, health promotion programming should consider focusing on higher level skills such as purchasing and preparing healthy food on a low budget.
With data now showing this desire for traditional foods from both on-reserve and urban youth, it becomes apparent that traditional food preference is not disappearing with the increasingly young and urban Aboriginal population. This finding indicates that increasing training for young Aboriginal People to acquire traditional food and prepare it might be a way to promote healthy body weights. Future research should examine how to increase the engagement of urban Aboriginal youth in the actual acquisition of traditional food from the land.
Last, the findings from our study illustrate that the school can be a place that promotes culturally specific values toward healthy eating. Past research shows that using innovation and creativity with set programs or models can produce successful nutrition interventions in Indigenous schools (Viola, 2006). Many current curriculums from K-12 contain nutrition education. With some creativity and innovation, school-based nutrition programs can take into account culture and devote time to traditional foods, which may result in further positive impact on the eating habits of urban Aboriginal youth. This might also be a way to promote cross-cultural understanding through school-based education.
Footnotes
Acknowledgements
We would like to thank the 15 young men and women who participated in this study and shared their knowledge and experiences with us. We would also like to express our gratitude to the teachers, staff, and administrators who facilitated this project.
This work was supported by the Canadian Institute for Health Research Banting and Best Graduate Scholarship.