
Abstract
Background. The application of evidence-based lifestyle interventions is suboptimal, but little is known what interventions are actually used. This study aimed to explore the range of lifestyle interventions used in Dutch ambulatory health care settings. Method. We conducted interviews (n = 67) in purposefully selected hospitals, general practices, and community care organizations. Interviews focused on identifying activities to help patients stop smoking, reduce alcohol consumption, increase physical activity, eat a healthy diet, and lose weight. We also asked who developed the interventions. All reported activities were registered and analyzed. Results. Four categories of health promotion activities emerged: giving advice, making referrals, offering counseling, and providing lifestyle interventions organized separately from the care process. In total, 102 lifestyle interventions were reported. Forty-five interventions were developed by researchers, of which 30 were developed by the Dutch Expert Center on Tobacco Control. Providers did not know the source of 31 interventions. Eighteen interventions were developed by the providers themselves, and eight were based on evidence-based guidelines. Conclusions. Health promotion activities seemed to be widely present in Dutch health care, in particular smoking cessation interventions. Although health care providers use many different interventions, replacing nontested for evidence-based interventions is required.
Introduction
Various studies have shown that the dissemination and implementation of evidence-based lifestyle interventions in health care practice are suboptimal (Carlfjord, Andersson, & Lindberg, 2011; Glanz, Rimer, & Viswanath, 2008; Goode & Eakin, 2013; Owen, Glanz, Sallis, & Kelder, 2006; Remington, Brownson, Wegner, & American Public Health Association, 2010). However, what lifestyle interventions are used within the health care system as a whole is largely unknown (Blonstein et al., 2013; Eakin, Brown, Marshall, Mummery, & Larsen, 2004; Estabrooks & Glasgow, 2006; Ma et al., 2013). One reason why little information is available on the kinds of lifestyle interventions that are used in health care is that many dissemination and implementation studies presume a linear model in which interventions are developed by researchers and disseminated to end users (Green, Ottoson, Garcia, & Hiatt, 2009). These studies mostly focus on a single intervention as the unit of implementation or dissemination. Consequently, aggregated data that describe the range of interventions used across health care settings, health behaviors, and patient groups on a national or local level are not available.
What kinds of lifestyle interventions are used in daily practice depends on many different factors (Green et al., 2009; Rabin, Brownson, Haire-Joshu, Kreuter, & Weaver, 2008), at the very least on what interventions are available, the strength of evidence supporting their effectiveness, and what is needed from a societal perspective.
An overview and guide of available evidence-based lifestyle interventions applicable to health care settings is currently lacking in the Netherlands (Brug et al., 2010; Hoeijmakers, 2009; Nielen et al., 2010), as well as support and assistance to select and implement lifestyle interventions in practice (Hamberg-van Reenen, Mikolajczak, Post, & Barte, 2011). With regard to the strength of evidence, the international literature shows that a strong evidence base is available for smoking cessation interventions (Jepson, Harris, Platt, & Tannahill, 2010; Stead, Bergson, & Lancaster, 2008; Stead & Lancaster, 2005), and for interventions to reduce hazardous alcohol intake (Jonas et al., 2012; Kaner et al., 2007). The evidence base for interventions addressing other health behaviors is less strong (Brownson, Fielding, & Maylahn, 2009; Green et al., 2006; Hillsdon, Foster, & Thorogood, 2005). With regard to the prevalence of unhealthy behaviors and related diseases in the Netherlands, one might expect that health care providers would at the very least use interventions addressing smoking, unhealthy diets, obesity, and physical inactivity. In brief, a proportion of 23% of the adult population are current smokers, 10% of Dutch adults can be classified as heavy drinkers, and 48% of the Dutch adult population is overweight (National Institute for Public Health and Environment, n.d/xref>.; www.volksgezondheidenzorg.info). Furthermore, 35% of the Dutch population does not exercise on a regular basis at least once a week and 90% to 95% of the Dutch population does not eat the minimum recommended daily amount of fruits and vegetables. In 2011, the two main causes of death were cancer and heart diseases, with lung cancer being the number one cause of death among men (www.nationaalkompas.nl).
A broad bottom-up exploration, without limiting the inquiry beforehand, identifies what kinds of lifestyle interventions are used by providers across different health care settings. In addition, identifying the source of these interventions can indicate the extent to which they are evidence based. This information is relevant for policy makers, researchers, and practitioners as it can point out where the dissemination and implementation of evidence-based lifestyle interventions require action. Therefore, the aim of this study is to describe the range of lifestyle interventions used in Dutch ambulatory health care settings and to identify who developed these interventions.
Method
Design
This qualitative descriptive study consisted of semistructured interviews with health care providers in various settings in the Netherlands to explore what they do to promote healthy lifestyles in their adult patients. We aimed to describe what kinds of lifestyle interventions are used, for what patient groups, delivered by what type of health care providers, and by whom the interventions are developed (Sandelowski, 2000, 2010). The exploration was not limited beforehand, to be able to describe the varied manifestations (Creswell, 2009).
The Medical Ethical Committee, CMO Regio Arnhem-Nijmegen, waived the need for approval of the study (Letter dated April 22, 2010; Registration No. 2010/120).
Participants, Setting, and Recruitment
Purposive sampling was used to include various health care settings in five geographic regions in the Netherlands. The sampling strategy aimed to recruit health care professionals from hospitals, community care organizations, and general practices. Recruitment started in hospitals. In all five selected hospitals, the outpatient clinics for cardiology, (vascular) surgery, internal medicine, pulmonary medicine and dermatology were contacted to recruit a key respondent from each clinic. Cardiology, (vascular) surgery, internal medicine, and pulmonary medicine were selected because of the high prevalence of lifestyle-related diseases among patients treated at these settings. We selected dermatology because of a previous collaboration in the development of a lifestyle program for patients with venous leg ulcers (van de Glind, Heinen, Evers, Wensing, & van Achterberg, 2012).
Subsequently, one community care organization and three general practices in the area of each of the included hospitals were chosen for inclusion. Dutch community care organizations are allowed to provide home nursing and personal care in any area in the Netherlands, resulting in the existence of competing agencies of different sizes within a region. To recruit community care organizations that are active in our areas of interest, respondents from outpatient clinics were asked which community care organization would be best to approach for this study. General practices were recruited through regional sector organizations and by approaching practice nurses by phone to enquire whether general practitioners in their practice would participate. Additionally, in two of the five regions, letters were sent to general practices, followed by phone calls as a reminder. Using this recruitment strategy, we aimed at conducting a minimum of 55 interviews.
Data Collection and Analysis
The research group developed an interview guide. We piloted it in the first three interviews, and no changes were necessary. Interviews comprised the following questions:
What do you do to help patients stop smoking, decrease alcohol consumption, increase physical activity, eat a healthy diet, and lose weight?
In follow-up questions we asked, (1) What are key elements of the activity/intervention? (2) For whom is the activity (patient group)? (3) Which health care professional(s) deliver(s) the activity (by whom)? (4) Who developed the intervention (from whom)?
Two researchers (IVDG, WG) conducted the interviews in Dutch during the period March to May 2011. For each interview a separate appointment was made. Interviews were conducted by telephone or face-to-face, with an average duration of 30 minutes (range 10-50 minutes). Interviews were digitally recorded, for which verbal, informed consent was obtained. During the interview researchers filled in a template, with the health behaviors in separate rows and the interview questions in the columns. Respondents’ answers were written in the blank spaces of the template. All activities mentioned by respondents were summarized and repeated during the interview to increase completeness and reliability of the data.
After each interview, all activities were entered into a database. Activities were reported at the level of practice or department to correct for duplicates, in case respondents worked in the same organization.
All reported activities were analyzed in the Dutch language using a framework analysis approach, which consisted of the following five steps (Pope, Ziebland, & Mays, 2000). Step 1, familiarization: Data were read and reread, and if necessary audiotapes were played back. Step 2, identifying a thematic framework: Similar activities were assembled into groups and assigned a descriptive label. This was done by first grouping activities into one of the two following groups: (1) performed within the practice or department of the respondent and (2) referring to other health care providers. Only activities within respondents’ practice or department were further analyzed and grouped by the nature and characteristics of the activity. Step 3, indexing: Generated codes (groups of activities) were systematically applied to all data. Step 4, charting: Data were rearranged, and summaries and charts were created. To discern patterns in the data, the identified activities were counted and summarized numerically (Sandelowski, 2000). Where relevant, numerical summaries are presented in the Results section to demonstrate patterns in the data. Step 5, mapping and interpretation: The charts were used to map the range and source of lifestyle interventions and provide explanations for the findings. One researcher coded and categorized the data (IVDG), and a second researcher checked the grouping of the data (WG). Any disagreement was resolved by discussion. To increase validity, the codes and charts were discussed in the research group (IVDG, WG, TVA). A number of quotations were selected and translated into English to illustrate the findings.
Results
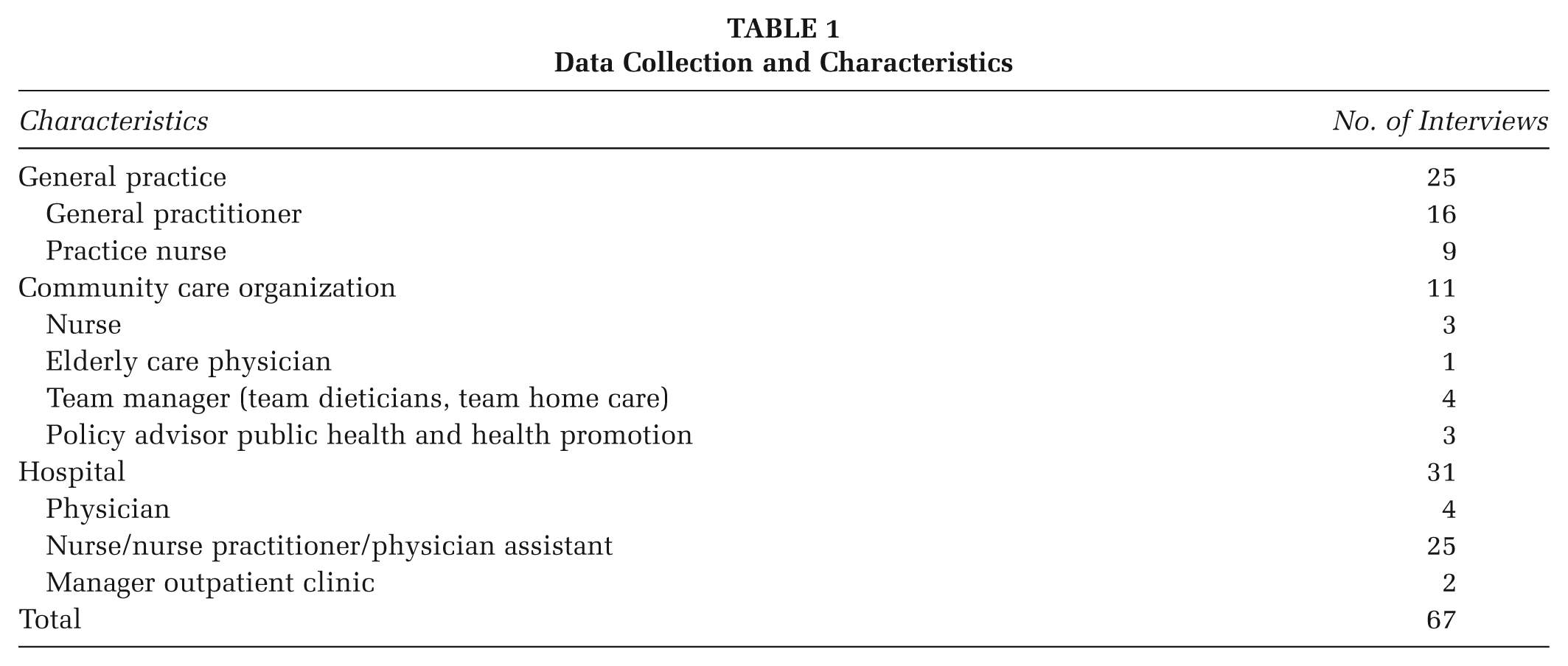
In each of the five regions, we were able to recruit key respondents in all targeted settings (outpatient hospital clinics, general practices, and community care organizations). In total, 67 interviews with health care professionals were conducted, 37 of which were conducted by telephone and 30 face-to-face. With respect to recruitment, all targeted settings in hospitals and community care organizations were willing to participate. However, two respondents, both physicians at a hospital, refused participation due to a lack of time. Two nurses were interviewed instead of the physicians. Furthermore, although the planned number of 15 general practices was achieved since we included 17 practices, 32 practices declined to participate. Reasons were as follows: no time (n = 25), no interest in the subject (n = 6) or maternity leave (n = 1). Table 1 presents the data collected in this study and characteristics of the respondents.
Data Collection and Characteristics
Activities to Promote Healthy Lifestyles
The analysis of interviews resulted in two main distinctions with respect to the reported activities (Table 2): (1) activities embedded in regular care and (2) lifestyle interventions organized separately from the regular care process.
Health-Promoting Activities in Dutch Health Care Settings
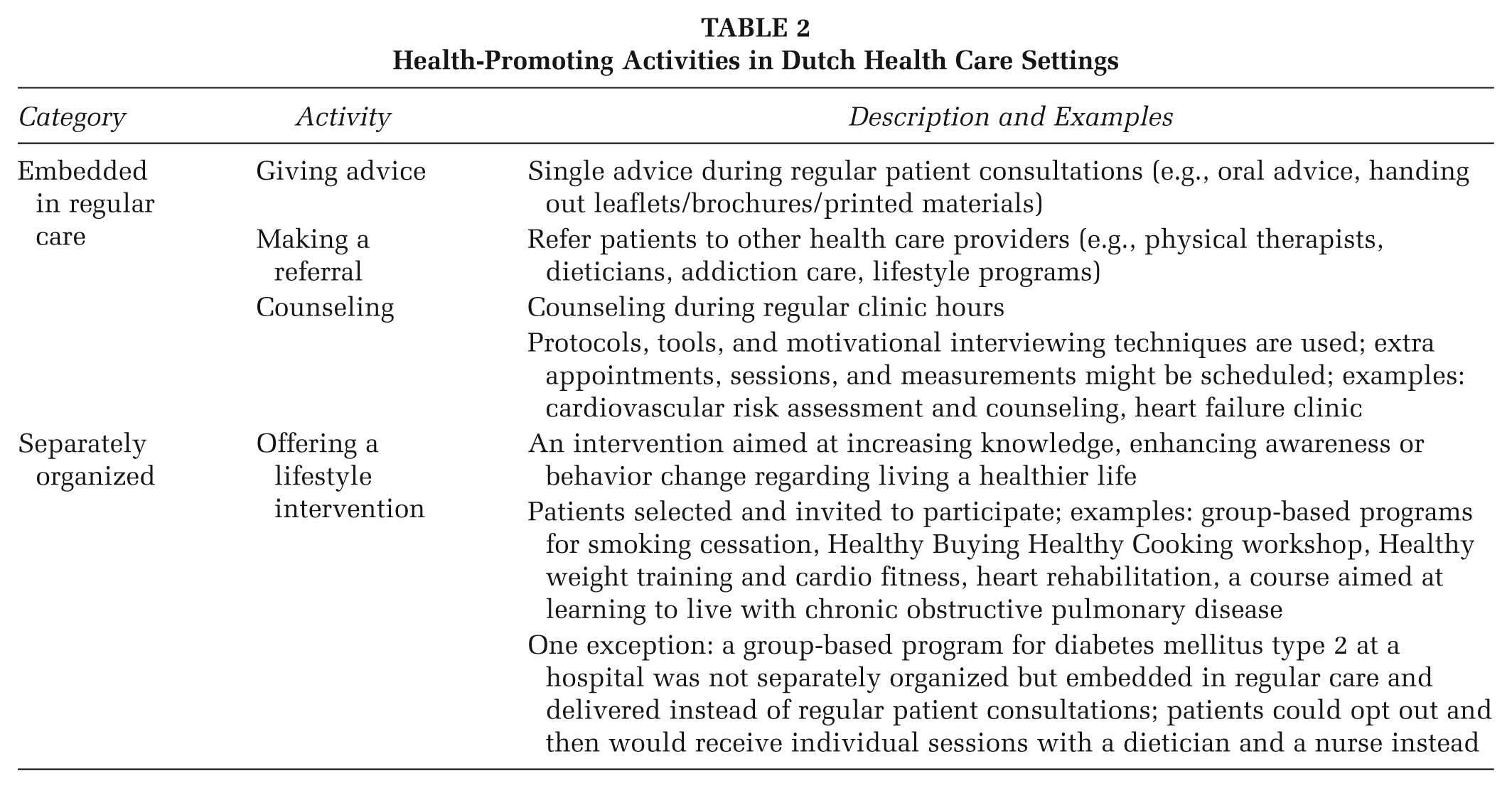
Activities embedded in regular care were further divided into the following: making referrals, giving advice, and offering structural counseling during regular patient consultations. Lifestyle interventions organized separately from the regular care process were defined as interventions, sessions, or programs for which patients were specifically selected and invited to take part. We describe all four activities in more detail below.
Activities Embedded in Regular Care
Making a referral
Almost all respondents reported referring patients to other health care providers or organizations, in particular to physical therapists, dieticians, or addiction care.
You can roughly say, if someone eats fries every day that’s not healthy. But as General Practitioners we can’t take a proper and careful medical history of a patient’s diet. And we shouldn’t want to do that either, because for that we have our auxiliary staff. So, if patients agree, and we believe that it could help them, we refer them to a dietician. (General practitioner, respondent code R2P3A)
Giving advice
Respondents mentioned that they give advice to patients about healthy behaviors in regular patient consultations. Advice could vary from a single general advice, or handing out a leaflet, to a single advice tailored to the patient’s situation. Some respondents mentioned that they specifically ask patients about lifestyle behaviors to bring up the subject and give them advice.
We have multiple leaflets and summaries of all kinds of healthy food, low-caloric food, food to lower your cholesterol level, that sort of thing . . . and we hand these to them. (Nurse, outpatient clinic internal medicine, respondent code R5HA)
Offering counseling embedded in regular consultations
Health care providers reported that they incorporated structured counseling during regular clinic hours, often performed by a nurse, to support patients making lifestyle changes. During these consultations, lifestyle behaviors were assessed and discussed, for which a protocol and (often) motivational interviewing techniques were used. Examples are cardiovascular risk assessment and counseling, heart failure clinics, diabetes mellitus clinics, or pulmonary clinics.
Basically, every new patient at the outpatient clinic gets screened. They receive a questionnaire, an ECG, blood work and some other tests. . . . Then the patient comes to our clinic and we report all results back to him. And then we develop a plan together with the patient. What are relevant health goals and what kinds of goals does the patient want to work on? And then after the screening, we give them support and counseling for one year. (Nurse practitioner, respondent code R1HC)
Activities Separately Organized
Lifestyle Interventions
Interviewees also reported performing programmatic or structured lifestyle interventions. Patients were specifically selected or invited to participate in these lifestyle interventions. Examples are smoking cessation interventions, physiotherapy exercise programs, self-management programs, weight loss programs, and rehabilitation programs offered to heart and lung patients in hospitals with explicit attention to health behavior change.
We have a program for the obese. . . . We offer a course, tied into the program, where people learn how to deal with going to parties, holidays, how to recognize their pitfalls. (Physician assistant, respondent code R2HE)
Referrals, giving advice, and lifestyle interventions were reported in all settings and in all regions. Counseling was not reported in community care organizations in two regions.
Range of Reported Lifestyle Interventions
In total, respondents reported 102 unique lifestyle interventions (see Table 3). Of these, 39 were for smoking cessation, 33 addressed eating a healthy diet, weight loss and/or physical activity, and 29 interventions combined multiple lifestyle topics and self-management skills. Only one intervention for reducing patients’ alcohol intake was reported, but a number of self-management interventions included alcohol as a topic.
Range of Reported Lifestyle Interventions in the Five Regions (n = 102)
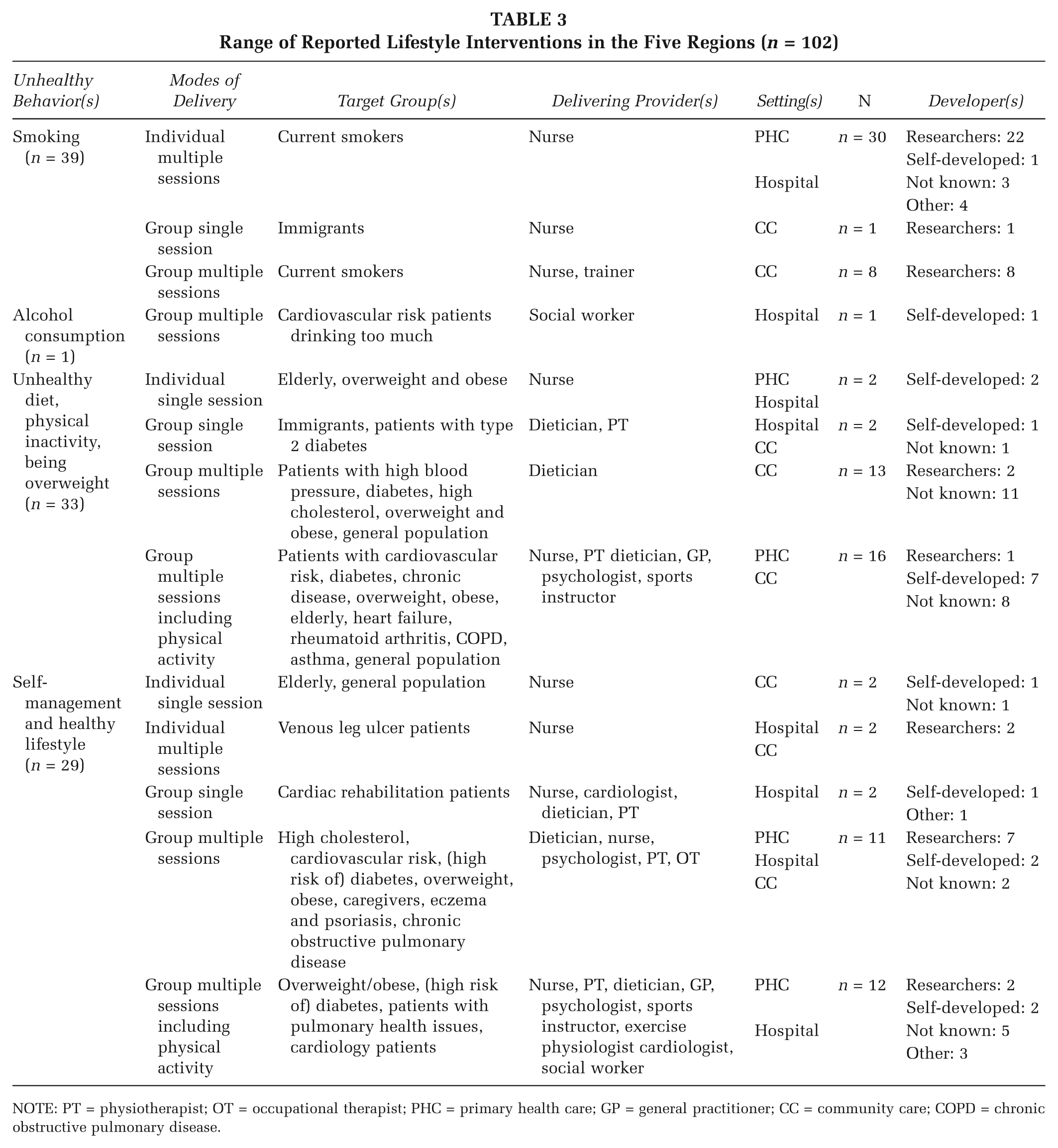
NOTE: PT = physiotherapist; OT = occupational therapist; PHC = primary health care; GP = general practitioner; CC = community care; COPD = chronic obstructive pulmonary disease.
Ninety-three interventions consisted of multiple sessions, and nine interventions consisted of a single session. Sixty-six interventions were group based: 29 for healthy diets, weight loss and/or physical activity and 23 for interventions combining lifestyle topics with self-management skills. Thirty-six interventions were individual based, of which 30 were for smoking cessation.
There was variation with respect to the type of professional delivering the interventions. Smoking cessation interventions and group-based diet interventions were all delivered by a single discipline (nurse/smoking cessation trainer, dietician). A multidisciplinary team delivered most other interventions.
Who Developed the Reported Lifestyle Interventions?
Analysis of the answers to the question who developed the lifestyle interventions (n = 102), revealed four main groups of developers:
In all, 44% (n = 45) of the lifestyle interventions were developed by researchers, research institutes, or centers of expertise. Of these, 30 were developed by the Dutch Expert Center on Tobacco Control.
For 30% (n = 31) of the interventions, who had developed it was unknown.
A total of 18% of the interventions (n = 18) were developed by the health care providers themselves.
A total of 8% (n = 8) of the interventions were categorized as “other” when respondents indicated that these were based on guidelines or were learned in school.
Discussion
The aim of this study was to describe the range of lifestyle interventions used in Dutch ambulatory health care settings and to identify who developed these interventions. Four health promotion activities were identified: making referrals, giving advice, offering counseling, and providing lifestyle interventions organized separately from the regular care process. Analysis of the lifestyle interventions showed that many different, both evidence based and nontested, lifestyle interventions are being used. Smoking cessation interventions in particular are widely present. Almost all these have been developed by the Dutch Expert Center on Tobacco Control. Lifestyle interventions targeting unhealthy diet, physical inactivity, and being overweight were also used. However, these were more heterogeneous with respect to the source of the intervention. Although several self-management interventions addressed alcohol consumption as a topic, specific interventions to reduce alcohol intake seemed to be lacking across health care settings.
The widespread presence of smoking cessation interventions is both reassuring and justified given the prevalence of current smokers and lung cancer in the Dutch population. One explanation why interventions aiming at other health behaviors were less widely reported across settings and more often nontested might be found in the level of available evidence for the effectiveness of these interventions. Interventions aimed at other health behaviors show promise, but, as yet, rigorous evidence of their effectiveness is less strong compared to that of smoking cessation interventions (Brownson, Chriqui, & Stamatakis, 2009; Green et al., 2006; Remington et al., 2010). There could also be other explanations, since many different factors have been reported in the literature why evidence-based interventions are not used in practice (Flottorp et al., 2013; Grimshaw, Eccles, Lavis, Hill, & Squires, 2012; Rabin et al., 2008; Wensing et al., 2014). For instance, the characteristics of the intervention might not match the setting, or the norms, values, or skills of the delivering professional. In addition, resources, incentives, available facilities, the capacity to change practice, and social or legal factors may also be of influence. Identifying the specific key factors that influence the dissemination and implementation of lifestyle interventions can help health care providers, policymakers, and researchers to develop strategies that match these factors in order to resolve barriers for implementation (Flottorp et al., 2013).
Beside the various evidence-based lifestyle interventions, this study also identified many interventions developed in everyday practice without any research component or evidence of effectiveness. Further research is necessary to get insight into the reasons why nontested interventions are used instead of evidence-based alternatives.
Many dissemination and implementation studies concentrate on one type of setting, intervention, health care provider, or patient group (Brownson, Fielding, et al., 2009; Glasgow, Green, Taylor, & Stange, 2012; Green et al., 2009). This study deliberately went beyond this and applied a broader scope. The study demonstrated the relevance of collecting real-world data across settings, patient groups, and interventions.
Our study had several limitations. First, the results of this study cannot necessarily be extrapolated to other countries because health care systems differ between countries. However, this study may encourage other researchers to conduct a similar exploration. Second, despite a careful recruitment strategy and selection of key respondents we cannot rule out selection bias, possibly resulting in an overrepresentation of respondents interested in promoting healthy lifestyles and the identification of false patterns. This may have particularly been the case for general practitioner. On the other hand, since we aimed to explore the range of activities in everyday practice, information from professionals who actually are more active in this respect was especially relevant. Third, interventions described in our study might in fact have evidence-based elements that interviewees failed to identify or recall during the interview. Finally, it should be noted that the reported presence of interventions does not necessarily imply frequent or adequate delivery. Previous research has shown that the frequency of delivery, the reach of priority populations, and the quality of delivery can be improved (Beswick et al., 2005; Hornsten, Lindahl, Persson, & Edvardsson, 2013; Noordman, Koopmans, Korevaar, van der Weijden, & van Dulmen, 2012; van Achterberg et al., 2011; Wilcox, Parra-Medina, Felton, Poston, & McClain, 2010).
The study points to the following implications. First, policy makers face the challenge of a wide variety of interventions with an unclear evidence base. A prominent question that needs to be addressed is, How can non-tested interventions be replaced by evidence-based alternatives? This requires a discussion about the extent to which coordination of this field is desired, who should coordinate it, and how. Second, given the large amount of reported lifestyle interventions, further research is needed regarding gaps and redundancies within regions. It would be interesting to explore to what extent (local) health care providers share information with each other about their health promotion activities, because this could help coordinate activities (Drenthen & Sturkenboom, 2015). Third, more research is needed to demonstrate (cost-)effectiveness of lifestyle interventions, in particular those aimed at increasing physical activity, eating a healthy diet, and losing weight. In addition, more insight into how health care professionals perceive evidence-based lifestyle interventions and why they adopt or reject them would provide more guidance for intervention developers to design interventions that fit the real-world environment (Glasgow et al., 2012; Green et al., 2009). Finally, it would be valuable to investigate how smoking cessation interventions found their way into Dutch practice, in order to learn from their successes and failures and speed up the dissemination and implementation of evidence-based interventions addressing other important health behaviors.
Conclusions
Health promotion activities seem to be widely present in Dutch health care settings, ranging from giving advice, making referrals, and counseling, to offering lifestyle interventions organized separately from the care process. Smoking cessation interventions from the Dutch Expert Center on Tobacco Control are particularly widespread. Lifestyle interventions targeting unhealthy diets, physical inactivity, and being overweight are also present, but their source is often unclear or not known. Interventions addressing alcohol consumption seemed to be lacking. Our results show that many different lifestyle interventions are used, but replacing nontested interventions by evidence-based interventions is required. In addition, coordination of lifestyle interventions is recommended to avoid gaps and redundancies in local health care systems.
Footnotes
Authors’ Note:
We would like to thank all health care professionals who participated in interviews. This work was supported by the Dutch Organisation for Health Research and Development, ZonMw (Project No. 510000003).