
Abstract
Objectives. The objective of this project was to determine whether intervention mapping is a suitable strategy for developing an Internet- and text message–based smoking cessation intervention. Method. We used the Intervention Mapping framework for planning health promotion programs. After a needs assessment, we identified important changeable determinants of cessation behavior, specified objectives for the intervention, selected theoretical methods for meeting our objectives, and operationalized change methods into practical intervention strategies. Results. We found that “social cognitive theory,” the “transtheoretical model/stages of change,” “self-regulation theory,” and “appreciative inquiry” were relevant theories for smoking cessation interventions. From these theories, we selected modeling/behavioral journalism, feedback, planning coping responses/if-then statements, gain frame/positive imaging, consciousness-raising, helping relationships, stimulus control, and goal-setting as suitable methods for an Internet- and text-based adult smoking cessation program. Furthermore, we identified computer tailoring as a useful strategy for adapting the intervention to individual users. Conclusion. The Intervention Mapping method, with a clear link between behavioral goals, theoretical methods, and practical strategies and materials, proved useful for systematic development of a digital smoking cessation intervention for adults.
Keywords
Introduction
The development of health promoting interventions is complex, involving decisions at various levels. Program planners rely on many sources, and the detailed development process is often not fully reported. Transparent descriptions of intervention development will clarify the logic of program objectives, intervention strategies, and their theoretical underpinnings and provide insight into the working mechanisms of the actual program (Bartholomew, Parcel, Kok, & Gottlieb, 2006; Kok & Mesters, 2011). In addition, it is important to have full understanding of how theoretical methods have been operationalized and adjusted to target groups in order to transfer experience from one context to another (Abraham & Michie, 2008; Glasziou, Meats, Heneghan, & Shepperd, 2008; Michie, Fixsen, Grimshaw, & Eccles, 2009). Thus, detailed descriptions of the actual planning process are important for the reader to fully understand how program planners can put research into practice.
Existing smoking cessation interventions have been shown to be effective (Stead & Lancaster, 2002), but they in general have limited reach (McDonald, 1999). Therefore, a challenge in smoking cessation intervention research is to develop intervention approaches that are not only effective but also have a high reach among smokers. One possible solution is to develop Internet-based smoking cessation interventions with supporting e-mail and mobile text messages (referred to as “Internet- and text-based” below). As many people have easy access to both Internet and cell phones, they can reach a large target group at low cost (Civljak, Sheikh, Stead, & Car, 2010). Nevertheless, substantial variation in quit rate has been found with Internet-based smoking cessation interventions (Shahab & McEwen, 2009). Although Web-based interventions can be effective (Head, Noar, Iannarino, & Grant, 2013), some studies show no effect (Buller, Borland, Bettinghaus, Shane, & Zimmerman, 2014; Civljak et al., 2010; Portnoy, Scott-Sheldon, Johnson, & Carey, 2008).
Intervention Mapping is a tool for planning theory- and evidence-based health promotion interventions that comprises six phases, each with clear tasks and a clear end product (Figure 1; Bartholomew et al., 2006). This article shows how following the steps of Intervention Mapping has guided identifying effective elements in the existing interventions and shows how various sources of research was put into practice in the development process of new Internet- and text-based smoking cessation intervention.
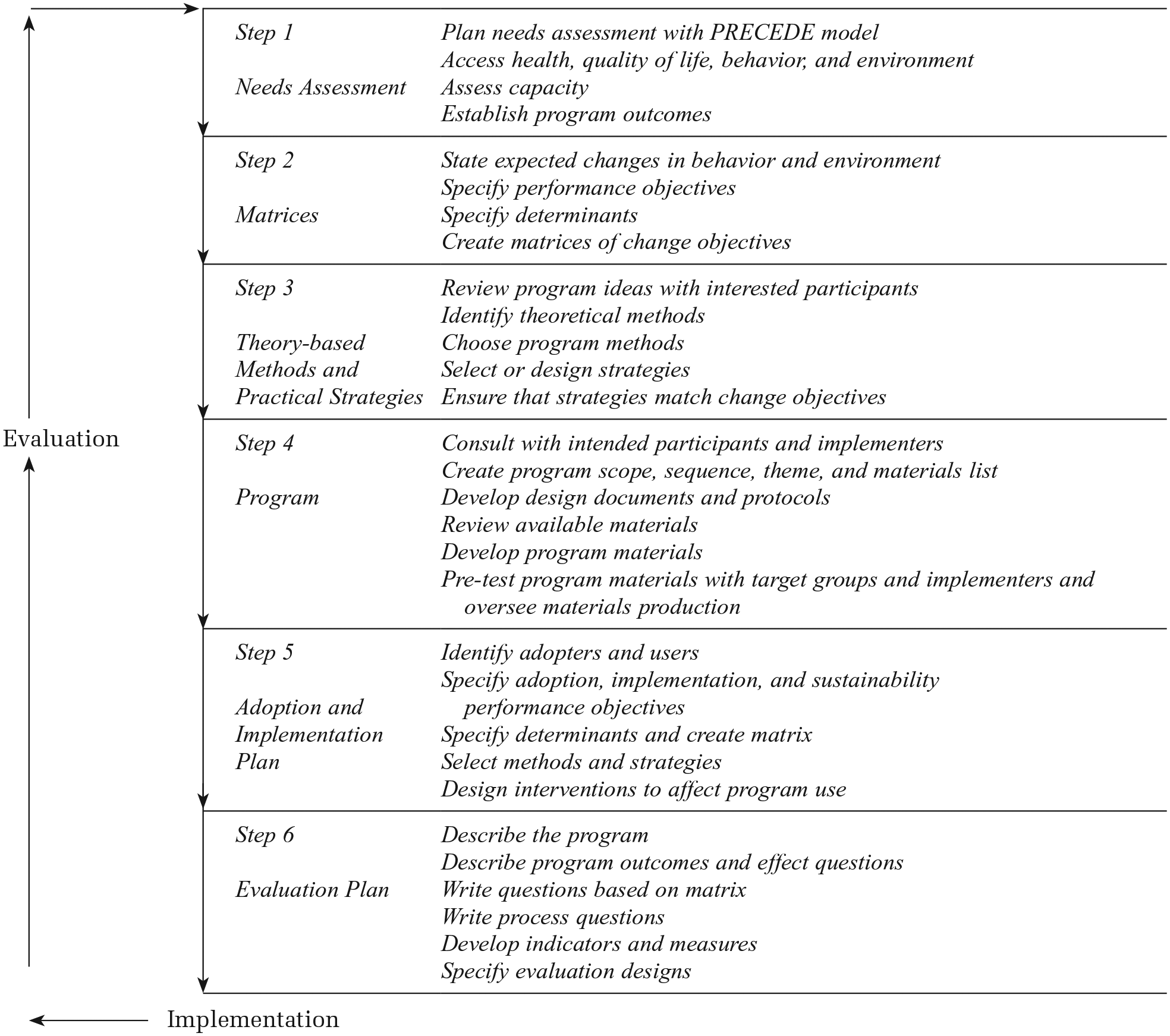
Protocol for the Intervention Mapping procedure. Adapted from Bartholomew, Parcel, Kok, & Gottlieb (2006) and Kok & Mesters, (2011).
Method and Results
Step 1: Needs Assessment
In Step 1 of Intervention Mapping, a planning group is established; the health problem, risk behaviors, and environments are assessed; and the program outcomes are defined. We established a planning group of interventionists and researchers at the Danish Cancer Society, which comprised expertise in web communication and experience in running a digital smoking cessation intervention for adolescents, general communication and communication theory, practical experience with smoking cessation counseling, theoretical understanding of behavioral change processes, and experience in systematic intervention development. In addition, we organized a steering committee consisting of representatives of the funders and staff responsible for implementing the program.
The intervention development took place in 2010-2011 and started with a needs assessment. First, best practices from the U.S. Centers for Disease Control and Prevention and other major organizations were identified to obtain general recommendations on adult smoking cessation interventions. Second, we conducted a systematic search of the literature on digital smoking cessation interventions to identify key elements and recommendations for the intervention. Finally, we used the results of a survey of the Internet use of the target group (Voss & Loland, 2007).
General Recommendations for Smoking Cessation Interventions
Smoking cessation literature generally accepts smoking cessation as a process that evolves over time, and many studies have described the process in terms of stages of change: precontemplation, contemplation, preparation, action, maintenance, and relapse. The various stages have different characteristics, and progression through the stages is thought to be mediated by “behavioral” or “cognitive” processes. Behavioral processes such as stimulus control or reinforcement management are the “actions” that are taken in a change process; cognitive processes such as consciousness-raising or self-reevaluation should be seen as mental “activities” performed during the change process (Prochaska, DiClemente, & Norcross, 1992).
Interventions should facilitate a learning process where the participant records tobacco use behaviors; raises awareness of thoughts, beliefs, and reasons for using or not using tobacco; gains knowledge about the physical and psychological effects of tobacco use; sets a specific and reasonable quit date; chooses a quitting strategy; sets short- and long-term goals; gains knowledge about physical and psychological symptoms of withdrawal; uses problem-solving techniques to minimize effects of situational triggers; develops coping skills (thoughts and actions); seeks social support from family and peers; and monitors and reinforces progress (Milton, Maule, Backinger, & Gregory, 2003). In addition, smokers are generally advised to consider using the medications available for tobacco dependence, including nicotine replacement therapy, varenicline, and bupropion sustained-release (U.S. Public Health Service, 2008).
Web-Based Smoking Cessation Interventions
Internet- and text-based smoking cessation interventions have the potential to reach a large target group with low cost (Civljak et al., 2010), and studies show that Web-based smoking cessation interventions can be effective (Head et al., 2013). However, there are also examples of studies with little or no effect, and there is a need to identify effective components in existing programs (Buller et al., 2014; Civljak et al., 2010; Portnoy et al., 2008).
Content of Existing Web-Based Smoking Cessation Interventions
We found that the communication methods used in existing Web-based interventions ranged from a combined approach of Internet, e-mail, and interactive voice response to a single approach. Some studies showed that participants preferred interventions with multiple techniques for presenting the content (Etter, 2006) and that follow-up messages such as e-mails and texts enhanced the effect of an intervention (Lenert, Munoz, Perez, & Bansod, 2004).
The actual elements of different digital smoking cessation interventions vary considerably, and their individual effects could not be determined. The elements included were an electronic library (Bock et al., 2004), biofeedback (Etter, 2006), video (Etter, 2006), e-mails (Lenert et al., 2004), texts (Rodgers et al., 2005), interactive voice response (Brendryen, Drozd, & Kraft, 2008), advice to use nicotine replacement therapy (Bock et al., 2004), diagnostic tools, online professionals, blogs (An et al., 2008; Brandt, Dalum, Skov-Ettrup, & Tolstrup, 2013), relapse prevention, just-in-time therapy (Brendryen et al., 2008), and log-on prompts (Balmford, Borland, & Benda, 2008).
Tailoring of content is suggested to be an important part of successful interventions for smoking cessation (Balmford et al., 2008; Skov-Ettrup et al., 2014; Strecher et al., 2005) and a factor that potentially prevents early dropout (Bock et al., 2004). It is considered to increase consistent use of an intervention (Balmford et al., 2008). Tailoring strategies range from simple personalization, that is, incorporating recognizable aspects of a person in a text with a general content, to individualized information or feedback based on an individual assessment (Hawkins, Kreuter, Resnicow, Fishbein, & Dijkstra, 2008). There was no indication of whether tailoring should be continuous or defined at baseline (Strecher et al., 2005). Tunneling is a tailoring concept that allows program planners to define which messages are delivered to the user at a specific time. It has been recommended that the chronology be similar to the development smokers experience when progressing in smoking cessation (Bock et al., 2004; Brendryen et al., 2008).
“Digital” Behavior of the Target Group
A study of 1,000 Danish respondents showed that both men and women used the Internet for behavior change activities and that the Internet platform is perceived as more useful than other mass media, such as television, radio, or books. Women, people living with children, and people with high socioeconomic status were more likely to use the Internet to improve their health (Voss & Loland, 2007).
In sum, we concluded that (1) the Internet could be a relevant communication channel for reaching a substantial proportion of the approximately 9,00,000 adult daily smokers in Denmark; (2) an Internet- and text-based smoking cessation intervention has the potential to effectively increase long-term quit rates; and (3) compliance, tailoring, and structural factors are important in designing an Internet-based intervention.
Step 2: Program Objectives
The second step in Intervention Mapping is to specify the program objectives. The first task was to break down the general health-promoting goal (quitting smoking) and to define specific subbehaviors or performance objectives that lead to the behavior in question. Performance objectives are the actions the target group must perform to reach the overall behavioral goal. In this step, we carefully analyzed and reformulated the findings of the needs assessment into performance objectives that could be seen as part of smoking cessation process. Once these objectives were specified, we returned to the outcomes of the needs assessment to identify psychosocial behavioral determinants that we deemed relevant for the purpose of our program. Subsequently, we specified program objectives by creating a matrix of change objectives by relating performance objectives to psychosocial correlates. For each cell, one or more change objective was defined, specifying what participants had to change to accomplish the performance objective.
The list of determinants of performance objectives and change objectives was presented to Danish experts and practitioners in smoking cessation research. We not only incorporated the suggestions for new theoretical or practical elements but also modified the matrix to the Danish context. The final performance objectives, determinants, and change objectives are summarized in Table 1.
Matrix of Performance Objectives, Determinants, and Change Objectives
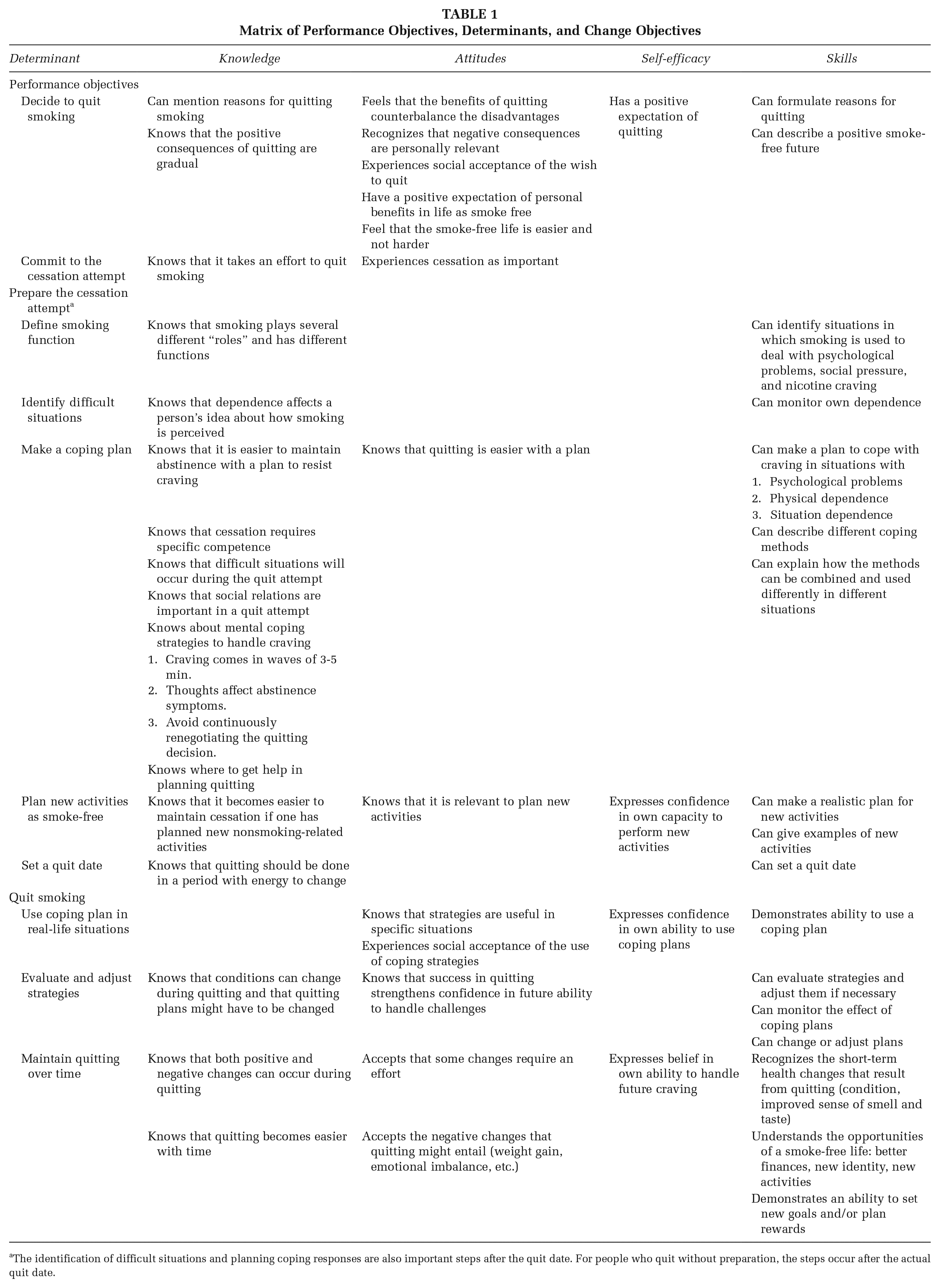
The identification of difficult situations and planning coping responses are also important steps after the quit date. For people who quit without preparation, the steps occur after the actual quit date.
Step 3: Theoretical Methods and Practical Strategies
In the third Intervention Mapping step, change objectives were linked to practical strategies derived from theoretical methods for behavior change. We reviewed the theoretical literature to find appropriate methods for choosing determinants and change objectives from the matrix. We focused on established, well-known methods but also searched for new approaches. We considered whether the method or strategy was adaptable for use on a communication platform and in a digital setting.
We selected self-regulation theory (Clark & Zimmerman, 2014), the transtheoretical model (Prochaska et al., 1992), social cognitive theory (Bandura, 1986), and appreciative inquiry (Kowalski, 2008) for the theoretical backbone of the intervention. The first three were chosen because of their strong focus in our matrix on motivation, self-efficacy, coping, and skills training. In addition, both self-regulation theory and the transtheoretical model state that people go through several stages or phases to reach their health goals, so that these theories are relevant for incorporating elements of timing and tunneling into the intervention. Appreciative inquiry was used to incorporate elements of positive thinking and linking positive expectations to quitting. Experienced counsellors in the field strongly recommended this approach, although there is as yet no evidence for its effectiveness in smoking cessation interventions.
From the general theories, we found that modeling/behavioral journalism (social cognitive theory), feedback (social cognitive theory), coping planning/if-then statements (self-regulation theory), positive imaging (appreciative inquiry), consciousness-raising (transtheoretical model), helping relationships (transtheoretical model), stimulus control (transtheoretical model), and goal-setting (transtheoretical model) were suitable methods for a digital adult smoking cessation intervention. We chose “tailoring” as the overall communication strategy (Hawkins et al., 2008).
Step 4: Program Development
In this step, the actual intervention was designed, produced, and pilot-tested. The planning group created a plan for translating knowledge and input from the previous Intervention Mapping steps into an Internet- and text-based program. All the ideas were evaluated for their appropriateness for the objectives in the matrix and their application for digital media. In parallel, we formed a smoking cessation group with smokers from the target group, who were followed and video-filmed throughout their quitting process. The aim was to obtain real-life role models for the program. We drafted the program in plain language, with detailed descriptions of all elements and functions. A Web-programming company translated the program description into a specification plan. During programming, functionality tests were conducted with members of the planning group to ensure that each element maintained the described aim.
The Intervention
The main platform of the program was the Internet, on which each participant had an individual Web page with the following content: “Profile,” “My page,” “Exercises,” “Blog,” “Videos,” “Urgent assistance,” “My quit plan,” and “Library.”
The program included both passive communication (Web page) and active follow-up, such as e-mails and texts, referred to in the literature as “push messages” (Klasnja & Pratt, 2012). The amount of communication sent over time was approximately bell shaped, reflecting cessation stages: slowly intensifying communication up until the set quit day and the most intensive communication in the first 4 weeks of the quit attempt. In the first period after quitting, participants received up to three messages a day, a new video every day, a new exercise every second day, and so forth (Figure 2). Each participant was followed up until 1 year after quitting. Those who relapsed could set a new quit date and reenter the program with the new date.

Flow of Communication in “Your Digital Quit Program”
When participants signed up for the program, they entered a smoking profile based on the Wisconsin Inventory of Smoking Dependence Motives–68 (WISDM-68) scale (Piper et al., 2004). They answered 68 questions on their smoking habits and were scored on 13 smoking motives. Each profile had a short description, and participants received a text message on the three motives with the highest scores. In addition, five mobile text messages tailored to the three motives were sent to participants during their quit attempt. The feedback was prepared by a trained psychologist with experience in smoking cessation. After registration, participants logged onto “My page” (see Figure 3), which was tailored by personalization, tunneling, and feedback. The page has a small introductory text with the individual’s quit date and a text box giving the number of cigarettes smoked and money spent (before the quit date) and the numbers of cigarettes not smoked and money saved (after the quit date). “My page” also includes an interactive section, in which participants are asked to state their current smoking cessation status (ranked from “Very well” to “I have relapsed”) and then receive feedback on their response. The page also gives new videos, exercises, and activities on the person’s blogs since his or her last log-in.
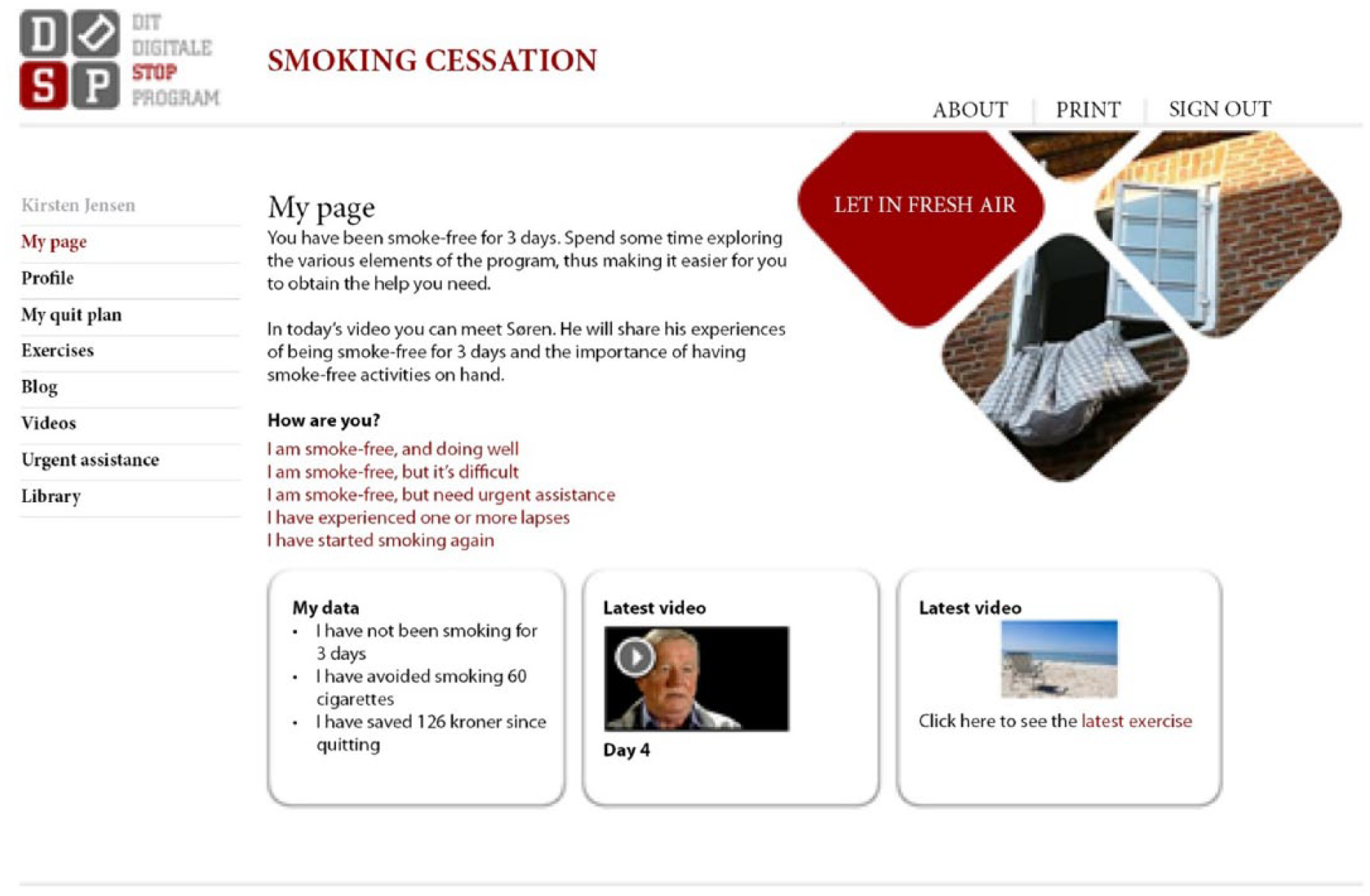
“My Page” Is the Main Page of the Program
The “Exercise” area contains small interactive exercises on diagnostic elements, cessation skills and tools, and positive visualization. The strategies used are positive imaging, consciousness-raising, helping relationships, stimulus control, and goal-setting. For example, in one exercise, the focus is on identifying people in a social network who could support the user during the quit attempt; another exercise defines new activities for a smoke-free life. The exercises are aligned with the quit date, and only exercises relevant to the person’s current stage of change are open.
The “Blog” gives opportunities for social support and feedback from other users of the program. The main strategy is modeling by vicarious learning and feedback.
In the “Video area,” the strategy “modeling/behavioral journalism” is used, with short stories from successful ex-smokers who were followed and interviewed throughout the quitting process. The videos are tailored and tunneled according to the quit date and are revealed day by day during the smoking cessation process.
“Urgent assistance” contains positive imaging, relaxation techniques, and coping planning to help participants cope with immediate craving. The area has four short meditation audio clips with relaxing stories, video clips with ideas on distraction from cigarettes, and suggestions on how to handle immediate craving.
In “My quit plan,” participants plan their coping response using the strategy of “if–then” statements. The area becomes accessible 1 week before the quit date and leads the user through two steps: identifying self-defined danger situations and deciding on specific actions. Users are prompted to take the Fagerstöm test of nicotine dependence (Fagerstrom & Schneider, 1989), and information is provided on the options for medical assistance. If participants decide to use medical products in smoking cessation, the medications they have chosen appear in “My quit plan.”
Finally, the “Library” has a question-and-answer section on smoking cessation, a section on cessation myths, and general information on smoking and smoking cessation.
Testing the Program
We tested the program for 3 months before launching it formally. During this period, the program was online on one of the major Web pages, but we used no marketing or communication about the program in the media. After the official launch of the program, we conducted a qualitative study with users. Nine semistructured interviews were held in February 2010 with men and women aged 23 to 60 years who were ex-smokers and had been enrolled in the Dit Digitale Stop Program (Your digital quitting program) for a minimum of 8 days (Brandt, Dalum, & Thomsen, 2013). The interviews showed that the program created a strong relation between users and the program itself. After about 1 month, however, some participants found that their expectations for communication had not been met, which created frustration, disappointment, and anger toward the program. They expressed frustration when the intensity of communication decreased and felt that the program had “left them on their own.” In contrast, some participants in the last phase of cessation found that texts from the program acted as smoking cues. To incorporate these conflicting views, we decided to maintain the level of follow-up communication but to increase information about when and why the intensity of communication was reduced. We increased the number of feedback messages in the interactive element on “My page” to maintain relevance and new inputs for “heavy users” of the program.
Step 5: Development of an Implementation Plan
Implementation of the program was considered at several levels throughout its development. The program was based on three major national Web pages aimed at smokers, thereby securing a flow of participants. In addition, all health professionals involved in smoking cessation were given information about the program. We encouraged a feeling of ownership of the program by involving the steering committee in its development and secured technical accuracy by involving an experienced Web master in the planning group, who also was responsible for later maintenance and technical assistance.
Step 6: Evaluation of Process and Effect
In Step 6, we finalized the plan for evaluation in a randomized controlled trial of the effectiveness of the program. The trial was conducted in a population-based sample of adult smokers in 2012-2014, and analysis of results is in progress. The control group received a self-help booklet (Lancaster & Stead, 2005). Measurements were conducted 1, 6, and 12 months after cessation. The primary outcome measure was 30-day point prevalence abstinence at 12 months. The 12-month abstinence rate is considered essential, because the long-term effect of Internet-based smoking cessation programs is not well documented (Civljak et al., 2010; Myung, McDonnell, Kazinets, Seo, & Moskowitz, 2009). We also included a number of secondary outcome measures to explore potential working mechanisms of the program: Self-efficacy, motivation, quitting-related expectancy, and use of nonassigned smoking cessation methods such as nicotine replacement were considered potential mediators of effect. In measuring these concepts, we drew on research when possible (Etter, Bergman, Humair, & Perneger, 2000; Hendricks, Wood, Baker, Delucchi, & Hall, 2011). These measures will be analyzed as potential mediators if an effect on abstinence is found. Process evaluation measures were included in the 1-month follow-up questionnaire and included use of the program components, perceived relevance of the program, reasons for nonuse, and whether participants would recommend the program to others.
Discussion
In this article, we describe the use of Intervention Mapping in the development of an Internet-based smoking cessation intervention for adults. The intervention was based on “social cognitive theory,” “the transtheoretical model,” “self-regulation theory,” and “appreciative inquiry.” A combination of strategies all related to specific change objectives were employed (modeling/behavioral journalism, feedback, coping planning/if–then statements, gain frame/positive imaging, consciousness-raising, helping relationships, stimulus control, and goal-setting). In addition, the intervention was tailored according to smoking dependence profile using the WISDM-68 scale, self-selected coping strategies, and “tunneling” was used to tailor communication to smoking cessation stage.
Systematic intervention development processes and detailed descriptions of actual planning are important for full understanding of how program planners can convert research into practice. In addition, clear descriptions create strong link between evidence and actual prevention programs. Detailed program planning and descriptions of planning cannot guarantee an effective program, but they make it possible to explore the mechanisms of the program and to understand why some apparently identical programs work and others do not (Kok & Mesters, 2011). Further precise descriptions of interventions would allow better understanding of the conditions under which they are effective for different target groups or different cultures (Abraham & Michie, 2008).
Although our planning process was guided by intervention mapping, we did not conduct a full review of all determinants of smoking cessation or prioritize them according to “importance” or “changeability.” Instead, we looked at general recommendations for smoking cessation interventions and reviewed the literature on strategies used elsewhere. Therefore, the performance objectives, change objectives, and determinants were selected on the basis of general scientific insights into smoking cessation and consensus among the program planners. This was done for both time restrictions and because smoking cessation is a well-researched field.
We used the WISDM-68 scale to give individual feedback to users. Although the feedback was given by a trained psychologist with experience in smoking cessation, use of the scale in an intervention context is still experimental.
The most important strength of the program development was the existence of a multidisciplinary planning group, who contributed their views during the development process and ensured that both behavioral and communicative aspects were considered throughout. Furthermore, use of Intervention Mapping procedures ensured the transparency of the decisions taken in the development process. For instance, the definition of overall goals, determinants, and performance and change objectives in Step 2 ensured that all partners had a common understanding of the main objective of the program and therefore worked in the same direction (Bartholomew et al., 2006). Such methodological transparency is crucial in deciding on specific outcome or process evaluation measures when planning an evaluation.
Conclusion
The Intervention Mapping method, with a clear link between behavioral goals, theoretical methods, and practical strategies and materials, proved to be useful for systematic development of a digital smoking cessation intervention for adults based on the best available evidence.