
Abstract
Safe in the City, a video intervention for clinic waiting rooms, was previously shown to reduce sexually transmitted disease (STD) incidence. However, little is known about patients’ recall of exposure to the intervention. Using data from a nested study of patients attending clinics during the trial, we assessed whether participants recalled Safe in the City, and, if so, how the intervention affected subsequent attitudes and behaviors. Analyses were restricted to responses to a 3-month follow-up questionnaire among participants who were exposed to the video (n = 708). Impact was measured as participants’ reports of the video’s effect on behaviors and attitudes. Associations were evaluated using multivariable logistic regression. Of participants who were exposed, 685 (97%) recalled viewing the video, and 68% recalled all three vignettes. After watching the video, participants felt more positive about condoms (69%) and comfortable acquiring condoms (56%), were reminded of important information about STDs and condoms (90%), and tried to apply what they learned to their lives (59%). Compared with those who recalled viewing one or two vignettes, participants who recalled viewing all three vignettes reported more positive attitudes toward condoms and peer/provider communication. These findings demonstrate that a low-resource video intervention for waiting rooms can provide sufficient exposure to positively influence STD-related attitudes/behaviors.
Background
Clinic-based interventions incorporating a video offer several advantages for delivering health information, including ease of implementation, consistency of message dissemination, low cost, and high likelihood of being acceptable to both clinic staff and patients (Carey et al., 2015; Carey, Vanable, Senn, Coury-Doniger, & Urban, 2008; Downs et al., 2004; Eakin et al., 1998; C. R. O’Donnell, O’Donnell, San Doval, Duran, & Labes, 1998; Roye, Silverman, & Krauss, 2007; Sweat, O’Donnell, & O’Donnell, 2001; Tuong, Larsen, & Armstrong, 2014; Warner et al., 2008). Stand-alone video interventions further conserve staff time that would be needed to convene groups and lead intervention sessions, thus requiring minimal time for implementation (Downs et al., 2004; Warner et al., 2008).
In sexually transmitted disease (STD) clinic settings, where clinicians may face barriers to educating and counseling patients, inexpensive interventions that are easy to implement offer an effective approach for providing patients with health information and prevention counseling (Eaton et al., 2012; C. R. O’Donnell et al., 1998). One such intervention, Safe in the City, is a 23-minute video intervention designed for STD clinic patients to view while they are in waiting rooms. Safe in the City consists of three vignettes depicting couples negotiating safer sexual behavior, while incorporating key information about condom selection and correct use, and prevention messages (Myint-U et al., 2010; Warner et al., 2008). The intervention used an integrative theoretical approach (Myint-U et al., 2010), combining core constructs from the social cognitive theory (Bandura, 1991), information–motivation–behavior model (Fisher & Fisher, 1996), and the theory of planned behavior (Ajzen, 1991). As part of the intervention, posters in the waiting and examination rooms direct patients’ attention to the video and reinforce key messages. Complete details about the development and content, including the theoretical basis, are described elsewhere (Myint-U et al., 2010). In a multisite controlled trial in which nearly 40,000 STD clinic records of patients were reviewed, the incidence of laboratory-confirmed STDs among patients who attended the clinics during periods when the waiting room video was shown, compared to when it was not, was significantly lower (Warner et al., 2008).
Previous research has found brief video-based interventions can improve knowledge about STDs and influence attitudes and behaviors, including treatment compliance and condom acquisition, among STD clinic patients (Healton & Messeri, 1993; Neumann et al., 2011; C. R. O’Donnell et al., 1998; L. O’Donnell, San Doval, Duran, & O’Donnell, 1995; Solomon & DeJong, 1988, 1989). However, unlike Safe in the City, these interventions typically have included an individual or small-group counseling component, and the administration and evaluation of these interventions have required selecting a sample of patients from the clinic (Healton & Messeri, 1993; Neumann et al., 2011). The Safe in the City trial is unique in that no patients were actually enrolled in the intervention trial that assessed STD outcomes; rather, they were in the clinic waiting room during an interval when the video was or was not showing. Because the trial involved a review of patient clinic records with no actual patient enrollment, little is known about the degree to which patients recalled exposure to the video and its prevention messages. Our analysis was designed to determine, through in-depth surveys with a sample of patients, whether participants recalled viewing the Safe in the City video during their visit and to assess the impact of video exposure on subsequent STD-related attitudes and behaviors.
Method
The main Safe in the City trial was conducted in three publicly funded STD clinics in Denver, Colorado; Long Beach, California; and San Francisco, California, from 2003 to 2005. An alternating treatment assignment scheme based on 4-week intervals was used to systematically assign groups of patients in the waiting room to either the intervention (i.e., Safe in the City video plus accompanying posters) or control condition (i.e., standard waiting room experience). Data for the current analysis were taken from a behavioral study nested within the original Safe in the City trial. Sampling of patients for enrollment in the nested behavioral study was conducted by systematically sampling 1,609 clinic patients in equal proportions from each study arm (810 intervention, 799 control). Participants were asked to complete an audio computer-assisted self-interviewing questionnaire on STD risk behaviors and prevention practices immediately following the initial clinic visit and at 3-month follow-up. For the nested study, participants had to be English-speaking, at least 18 years of age, sexually active in the previous 3 months, not previously exposed to the intervention, and not known to be seriously ill, HIV-positive, or pregnant. They also had to have spent at least 20 minutes in the STD clinic waiting room, which is consistent with the length of the Safe in the City video (23 minutes), could not have been diagnosed with a condition requiring frequent return visits (e.g., genital herpes), and had to have visited the STD clinic during the study enrollment period for a “new problem” (defined as a visit by a patient seeking diagnosis, treatment and/or consultation for signs, symptoms, or likely exposure to an STD that was not previously treated). All patients who participated in the nested behavioral study had to provide written informed consent. The institutional review boards at each study site and the Centers for Disease Control and Prevention reviewed and approved the study protocol.
We analyzed responses of participants who were assigned to the intervention condition of the nested study and completed the 3-month follow-up questionnaire (n = 708). At follow-up, participants potentially exposed to the intervention were asked a series of questions about whether they recalled key components of Safe in the City during their initial clinic visit. Specific exposure measures of interest included viewing (1) a health video in the waiting room, (2) posters in the waiting room, and (3) posters in the examination room. Among participants who recalled viewing the health video, recall of specific aspects was assessed, including whether participants recalled viewing (1) “all” or “most” of the video (vs. “half,” “some,” or “none” of the video), (2) any of the story lines of the vignettes, and (3) 30-second animation segments about condom use.
The video contained three related vignettes featuring young couples of diverse racial/ethnic backgrounds and sexual orientations in different types of relationships: new primary-partner relationships, dating relationships, and one-night stands (Myint-U et al., 2010). In the first vignette, about 10 minutes long, things are getting serious between Paul and Jasmine, but Paul has a sexual encounter with Teresa. After being tested, Teresa informs Paul that she has chlamydia, and Paul, who may have caught chlamydia from her, now has to tell his new girlfriend, Jasmine. In the next, shorter vignette (4.5 minutes long), the same character, Teresa, has recently met Luis and, after her STD scare with Paul, is serious about wanting to use condoms. Initially turned off by her perseverance, Luis eventually runs to a nearby convenience store to buy condoms because Teresa refuses to have sex without one. The third vignette, about 6 minutes long, features Rubén, Tim, and Christina. Rubén’s girlfriend, Christina, does not know about his interest in men. After meeting in a bar, Rubén and Tim have a sexual encounter, and several days later, Rubén has symptoms of an STD. Christina suspects something is wrong and insists on a visit to the STD clinic. In between the vignettes, two 30-second humorous condom animation segments are played. The first animation focuses on the types of condoms available by featuring a phallic-shaped character selecting from a variety of condoms. In the second segment, the character correctly puts on a condom and disposes it after ejaculation (Myint-U et al., 2010). The vignettes and animations in the video can be found at http://www.safeinthecity.org.
The follow-up questionnaire included real and false short summaries of the plots of the vignettes. Participants were asked to indicate whether or not the different story lines were featured in the video playing in the clinic waiting room. We assessed both the percentage of participants who recalled summaries of the three actual story lines described previously and the percentage of participants who recognized two false story lines included in the questionnaire. In the first false story line, a heterosexual woman (Jane) goes to the drugstore with her boyfriend (Brad) to purchase condoms for the first time. In the second, a heterosexual woman (Barbara) thinks she is pregnant because she had unprotected sex with her boyfriend.
Participants who correctly recalled the three true story line vignettes were compared to those who recalled one or two of the vignettes, on a series of measures. Measures compared included responses to statements assessing the video’s effect on subsequent behavior and attitudes, answered using a Likert scale ranging from “strongly disagree” to “strongly agree.” Impact was measured as percentages of participants “agreeing/strongly agreeing” (vs. “strongly disagreeing,” “disagreeing,” “neither agreeing or disagreeing,” or “refusing to answer”) with 11 of the statements: “I picked up a condom during my visit to the clinic because of what I saw in the health video”; “after watching the health video, I felt more comfortable about picking up or buying condoms”; “I felt more positive about condoms in general after watching the health video”; “the health video helped me to talk to my doctor about my risks for HIV or STDs”; “I learned new information about HIV, STDs, and condoms from the health video”; “I was reminded of important information about HIV, STDs, and condoms from the health video”; “I talked to my partner(s) about the health video”; “I talked to my friends about the health video”; “I talked to other people in the waiting room about the health video”; “I have tried to remember and apply in my own life what I learned or gained from the health video”; and “the health video taught me how to use a condom correctly.” Responses to the statements of whether participants talked to their partners or friends were combined for analysis purposes.
Separate multivariable logistic regression models were fitted for each impact measure to evaluate associations between viewing all three story line vignettes, compared with one or two vignettes, adjusting for sex, study site, race/ethnicity, education, and age.
Results
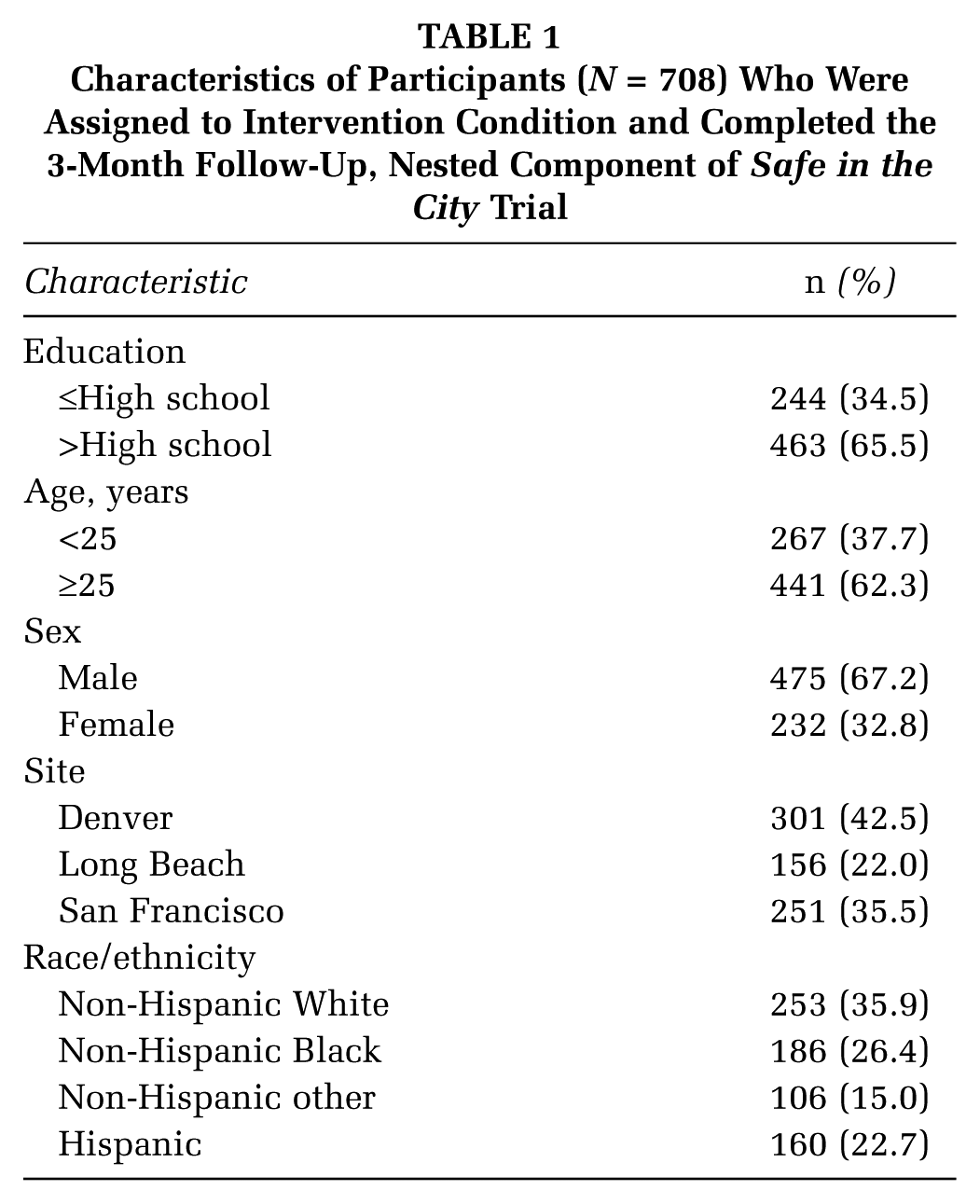
Among the 708 participants who completed the 3-month follow-up questionnaire, more than half were male (67%), non-White (64%), 25 years or older (62%), and had more than a high school education (66%; Table 1). Assessing exposure to the Safe in the City intervention, 685 (97%) of intervention participants recalled viewing a health video in the waiting room at their initial clinic visit. Additionally, 658 (93%) and 503 (71%) reported viewing posters in waiting rooms and examination rooms, respectively (Table 2). Among the 685 participants who recalled viewing a video while in the waiting room, 567 (83%) reported seeing “all” or “most” of the video, whereas 118 (17%) reported seeing “none,” “some,” or “half” of the video. Reported viewership exceeded 80% for each vignette (range per vignette: 81% to 92%), with 467 participants (68%) correctly recalling all three actual story lines.
Characteristics of Participants (N = 708) Who Were Assigned to Intervention Condition and Completed the 3-Month Follow-Up, Nested Component of Safe in the City Trial
Exposure to the Intervention, as Reported by Participants at 3-Month Follow-Up, Nested Component of Safe in the City Trial
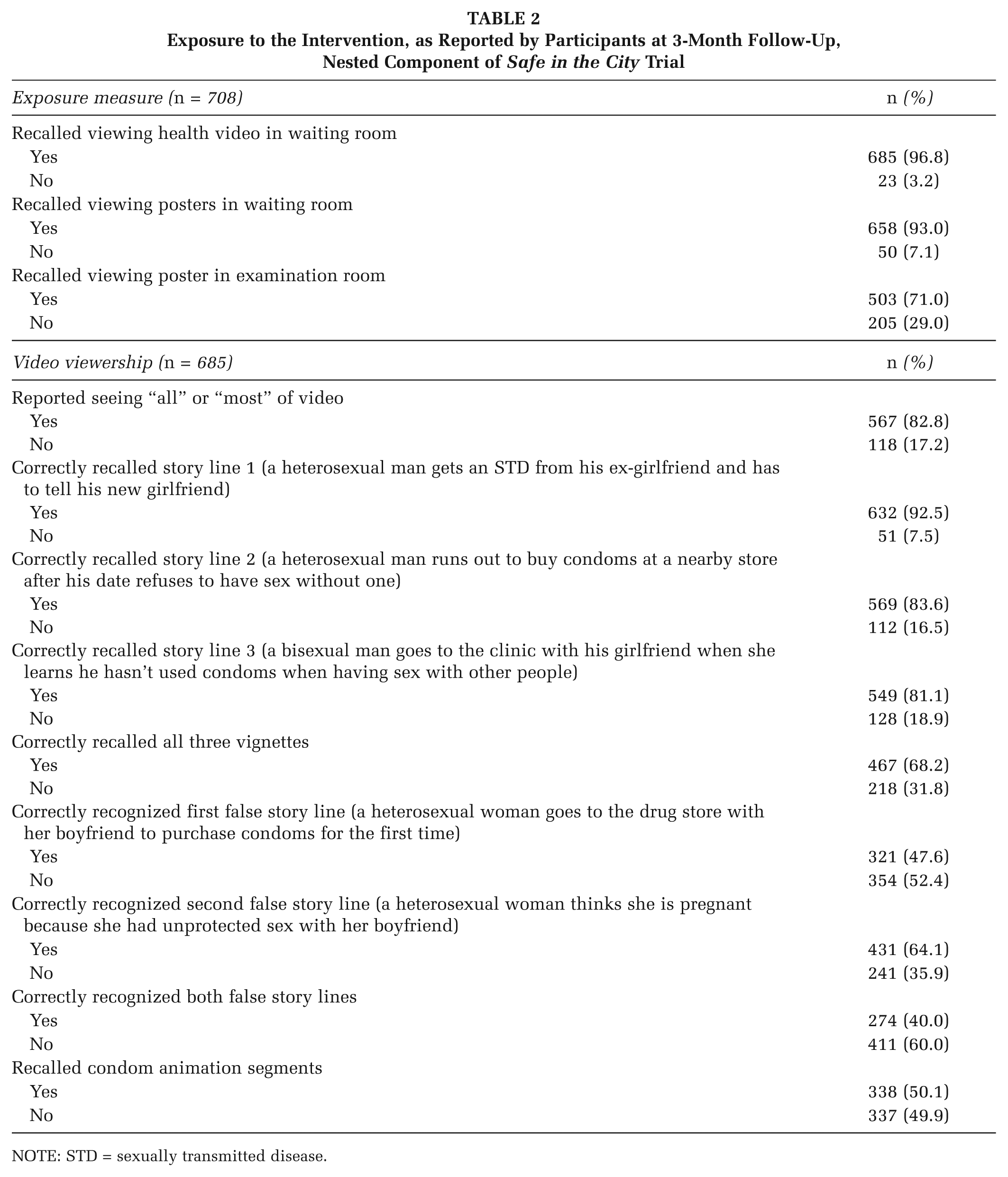
NOTE: STD = sexually transmitted disease.
For the two false story lines, 48% and 64% of participants correctly identified them as being false, respectively, at the follow-up visit. One false story line presented to participants (a heterosexual woman goes to the drug store with her boyfriend to purchase condoms for the first time) was intentionally constructed to be closely related to one of the true story lines in the vignette (a heterosexual man runs out to buy condoms at a nearby store after his date refuses to have sex without one). Despite the similarities of the false and true story lines, 48% of participants nevertheless recognized the story line as being false. Almost a quarter (23%) of participants who recalled viewing a health video correctly identified the three true story lines and recognized both false story lines. When we remove the closely related false vignette, 39% of participants recalled all three story lines and recognized the false vignette in which a heterosexual woman thinks she is pregnant because she had unprotected sex with her boyfriend.
Most of the 685 participants who recalled viewing a health video reported that, based on the video, they felt more comfortable buying or picking up condoms (56%) and more positive about condoms (69%); were reminded of important information about HIV, STDs, and condoms (90%); and tried to remember what they had seen in the video and apply it to their own lives (59%; Table 3). For each measure, a significantly higher proportion of participants who saw all three vignettes reported the attitude/behavior, compared with those who saw one or two vignettes.
Association Between Recall of Video Vignettes and Behavioral and Attitude Measures, Nested Component of Safe in the City Trial a
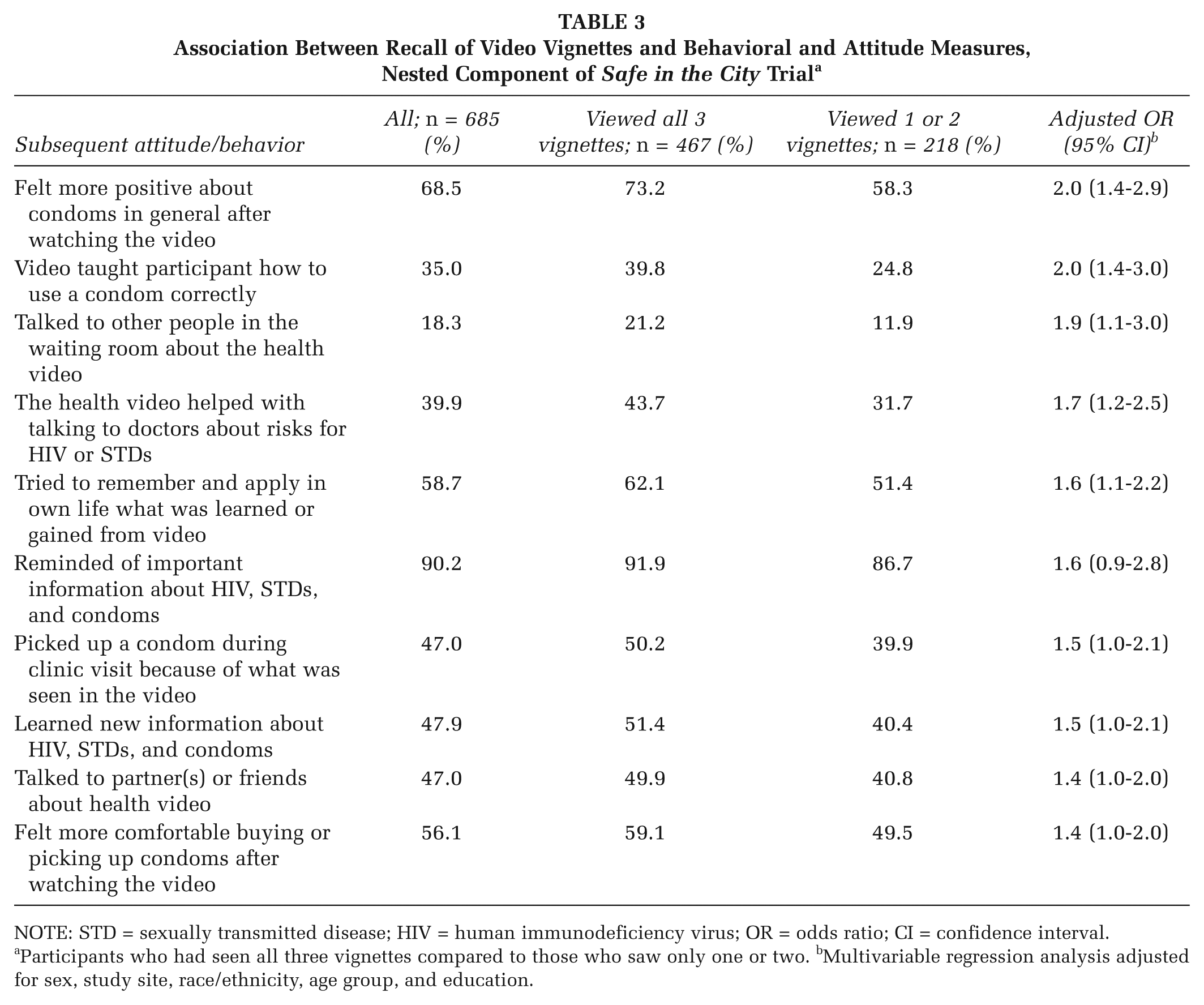
NOTE: STD = sexually transmitted disease; HIV = human immunodeficiency virus; OR = odds ratio; CI = confidence interval.
Participants who had seen all three vignettes compared to those who saw only one or two. bMultivariable regression analysis adjusted for sex, study site, race/ethnicity, age group, and education.
Multivariable analyses revealed that participants viewing all three story line vignettes reported that the video had a more positive impact on attitudes toward condom use compared to participants who viewed only one or two vignettes. Specifically, participants who reported viewing all three vignettes were significantly more likely to feel more positive about condoms in general (73% vs. 58%, adjusted odds ratio [aOR]: 2.0, 95% confidence interval [CI]: 1.4-2.9) and indicated that the video taught them how to use a condom correctly (40% vs. 25%, aOR: 2.0, 95% CI: 1.4-3.0; Table 3). Additionally, participants who reported watching all three vignettes were more likely to talk to other people in the waiting room about the health video (21% vs. 12%, aOR: 1.9, 95% CI:1.1-3.0), indicate the video helped them talk to a clinician about HIV/STD risk (44% vs. 32%, aOR: 1.7, 95% CI: 1.2-2.5), and remember and apply what they learned or gained from the video to their own life (62% vs. 51%, aOR: 1.6, 95% CI: 1.1-2.2). Participants who saw all three vignettes were 40% to 100% more likely than those who saw one or two vignettes to subsequently report the positive attitudes/behaviors asked about (Table 3).
Discussion
Most patients attending STD clinics during the larger Safe in the City Trial who were assigned to the intervention condition recalled being exposed to the intervention in the waiting room. Notably, viewership recall exceeded 80% for each vignette, and approximately two-thirds of participants (68%) recalled all three vignettes, suggesting that simply showing the video in the waiting room in a clinic-based environment can communicate important information about STD prevention to at-risk patients. Of note, participants were able to identify story lines 3 months after their initial clinic visit, well after initial video exposure, suggesting that the story lines of the video were sufficiently engaging to captivate the audience, despite competition for their attention in the waiting room (e.g., cell phone use). Many participants were also able to correctly identify the false story lines in the follow-up questionnaire, despite one of the false story lines being closely related to an actual story line. Higher levels of exposure to the video were associated with positive attitudes about condoms, how to use a condom correctly, increased self-efficacy in discussions with health care providers about STD risk, talking to others in the waiting room about the video, and applying information from the health video to one’s own life.
The findings from this study reinforce results from the larger Safe in the City trial in demonstrating that a low-resource, low-intensity waiting room video can positively influence STD-related attitudes/behaviors of clinic populations. Nonetheless, our analysis has several limitations. Relying on self-reported data could have led to reporting biases. Specifically, social desirability bias may have led to an overreporting of agreeing with impact measures by those who reported they had seen the video. Also, participants may have been more likely to answer affirmatively to the recall questions, as illustrated by the percentages of participants who reported recalling the false story lines. However, the use of audio computer-assisted self-interviewing questionnaires likely reduced the potential for reporting biases compared with being interviewed by a clinician or administrator of the intervention (Roye et al., 2007). Findings may have also been subject to recall bias of specific story lines or engagement in preventive behaviors, given that the follow-up questionnaire was administered 3 months after exposure to the video. Nevertheless, the overwhelming majority of participants reported seeing the video and were able to correctly identify the story lines. Because of the design of the nested study, an additional limitation is that comparisons on the outcome measures were only possible among participants who reported viewing the video. The study population for the nested study was also restricted to participants who reported being in the waiting room at least 20 minutes and thus may have resulted in an overestimate of viewership by excluding patients who may have been in the waiting room for a shorter time. However, during the Safe in the City trial, each site anonymously surveyed approximately 25 patients during each intervention cycle to monitor exposure to the intervention and time spent in the clinic waiting rooms. The level of exposure among patients who spent more than 20 minutes in the waiting room (81%) in the larger trial (Warner et al., 2008) is consistent with the level of exposure to the video in the current study (83%), suggesting similar wait times.
The nested study also has several strengths. As previously noted (Warner et al., 2008), administration of the video intervention took place under actual clinic conditions rather than in a controlled study setting, thus providing more realistic assessment of participant exposure to the intervention. Participants also were not actively enrolled to participate in the intervention and view the video, and those who attended the clinic during the intervention period were asked to recall viewing Safe in the City well after initial exposure. Had the intervention been administered in a controlled study setting or after a shorter duration, the level of video and vignette viewership would likely have been even higher. Another strength is the study included a geographically and racially/ethnically diverse sample of STD clinic patients.
Conclusions
STD clinics, specifically waiting rooms, provide a salient opportunity to educate patients about STDs. Patients who seek services at STD clinics are at risk for subsequent infections, but these settings often face barriers for implementing interventions targeting risk reduction (Healton & Messeri, 1993; Newman, Warner, & Weinstock, 2006; C. R. O’Donnell et al., 1998; Richert et al., 1993). Findings from this study provide evidence that simple, low-intensity, stand-alone, video-based interventions can be provided to patients in high-volume clinic settings with sufficient exposure and can influence subsequent attitudes and preventive behaviors. Specifically, higher levels of exposure to the video intervention were associated with more positive attitudes toward condoms and peer/provider communication. Future research could explore what specific components of a stand-alone video-based intervention resonate most with STD clinic populations and have a long-term impact on subsequent attitudes and preventive behaviors. This would be important to assess, especially among participants who report higher levels of exposure to an intervention, such as Safe in the City, so that when developing similar interventions, the components identified can be incorporated and built upon.
Footnotes
The work contained within this publication was supported by the Centers for Disease Control and Prevention (CDC), where technical assistance was provided through a federal cooperative agreement in the design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review, and approval of the manuscript.
The preparation of this manuscript was done while the primary author was an Association of Schools and Programs of Public Health (ASPPH)/CDC Public Health Fellow supported by Cooperative Agreement Number U36/CCU300430 from the CDC and ASPPH. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of CDC or ASPPH.