
Abstract
Mentoring is commonly used to facilitate professional growth and workforce development in a variety of settings. Organizations can use mentoring to help achieve broader personnel goals including leadership development and succession planning. While mentorship can be incorporated into training programs in public health, there are other examples of structured mentoring, with time commitments ranging from minutes to months or longer. Based on a review of the literature in public health and aggregated personal subject matter expertise of existing programs at the Centers for Disease Control and Prevention, we summarize selected mentoring models that vary primarily by time commitments and meeting frequency and identify specific work situations to which they may be applicable, primarily from the federal job experience point of view. We also suggest specific tasks that mentor–mentee pairs can undertake, including review of writing samples, practice interviews, and development of the mentee’s social media presence. The mentor–mentee relationship should be viewed as a reciprocally beneficial one that can be a source of learning and personal growth for individuals at all levels of professional achievement and across the span of their careers.
Introduction
In order to retain and develop their workforces, public health organizations need to identify and implement strategies that can promote workforce engagement and professional development. Mentoring, defined as teaching or giving help and advice to a less experienced and often younger person over a period of time, is one such strategy. Mentoring has become the subject of research attention in health care settings (Straus, Chatur, & Taylor, 2009; Straus, Johnson, Marquez, & Feldman, 2013; Tracey & Nicholl, 2006; Zerzan, Hess, Schur, Phillips, & Rigotti, 2009). Mentoring can also contribute to leadership succession and career planning, as well as helping develop mentee competencies (Palermo, Hughes, & McCall, 2010; Thacker, Dannenberg, & Hamilton, 2001), and is one of the keys to a successful multigenerational workforce.
In this article, we have amplified the research, drawing on our diverse experiences in private and federal workforce settings to suggest best practices and specific activities that mentors and mentees can incorporate into mentoring relationships.
Method
We conducted a literature review with Medline and Embase databases and used the search terms Public Health AND (mentor* OR professional development OR workforce development). One of the authors (SD) reviewed results of the literature search for public health workforce–related relevance. The literature review yielded 96 abstracts or suggested reference articles. On review, we found six references with relevant content. Most of the content presented here is based on additional materials and expert experience. All authors contributed personal experiences from their own careers and sought published and unpublished reports for individual and group mentoring programs they have been involved with through professional activities.
Mentoring in the Public Health Workplace
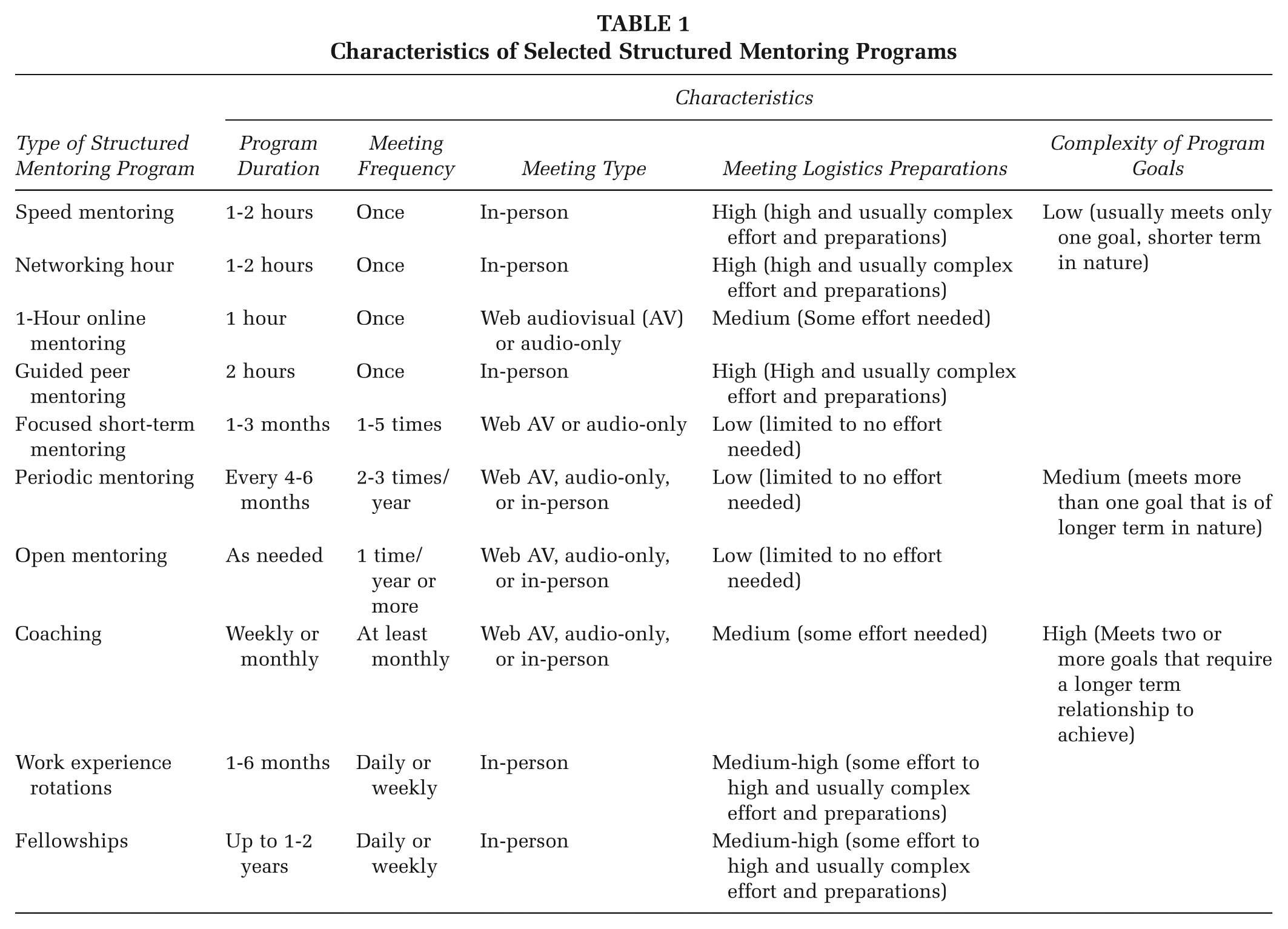
One approach to mentoring is to incorporate it as a feature of postgraduate and student training programs. Fellowships are the most common examples, with multiple successful models in public health settings. Many fellowships, most prominently the Centers for Disease Control and Prevention (CDC) Epidemic Intelligence Service program, have demonstrated benefits of mentorship. One of the authors (JI) established a mentoring relationship with a CDC staff member during an Epidemic Intelligence Service–related student experience at CDC (Buffington, Bellamy, & Dannenberg, 1999) that has resulted in six peer-reviewed articles and one book chapter. Another author (SG) mentored a Kenyan physician for 2 years as part of the Emory University Rollins School of Public Health mentoring program for its graduate students, continuing that mentoring relationship for 2 years when the mentee returned to Kenya. Analogous programs in global health include the Field Epidemiology and Laboratory Training program and the Training Programs in Epidemiology and Public Health Interventions Network (Iblan et al., 2013; Subramanian, Herrera, & Kelly, 2013). Mentor–mentee relationships are also part of newer CDC fellowship programs (www.cdc.gov/fellowships) such as the Public Health Associate Program, CDC Evaluation Fellowship, and the Presidential Management Fellowship. Fellowships can help promote and create long-term mentoring (for 6 months or more) relationships. However, fellowship opportunities are typically only available to recent graduates and are highly competitive (Table 1).
Characteristics of Selected Structured Mentoring Programs
Beyond the scope of training programs, mentoring may be appropriate for employees in specific workplace situations:
Role realignment, such as when an employee returns to a position after obtaining training, certification, or a degree
Leadership development, when an employee desires or is being prepared to advance into a leadership position
Job issues unlikely to be resolved by training, such as challenging interpersonal relationships involving supervisors, subordinates, or colleagues
Mentoring can be a specified or implied supervisory function, which requires active support to ensure trained supervisors are available. Long-term mentoring can be compatible with a supervisor–supervisee relationship, but both parties should be aware that this may involve discussions of alternate career paths or future opportunities.
Outside of the scope of a fellowship program, longer term mentoring programs and relationships require commitment of time and resources that not all public health organizations can support. More recently, structured mentoring programs are stimulating and amplifying professional development for professionals at all levels. These include the following:
Focused short-term mentoring through professional organizations and alumni clubs, matching mentors with mentees for a short number of mentoring sessions with specific, identified goals
Periodic mentoring, meeting with a formal mentor every 4 to 6 months for 30 minutes
Open mentoring though a relationship with a professional coach on an as-needed basis
In our experience, structured mentoring relationships of even shorter duration, for example, 1-hour–long meetings every 2 weeks over a 2-month period, have also received positive evaluations from mentors and mentees.
There are other options for structured mentoring:
Speed mentoring, where groups of mentors and mentees are brought together, and mentees rotate from mentor to mentor every 10 to 15 minutes: The Commissioned Corps of the U.S. Public Health Service (PHS) has used this model at CDC to match junior officer mentees with senior officer mentors. While the mentees all hold current positions within the PHS, they may be seeking new job opportunities or to enhance their promotion potential. Because of the limited time commitment that is required, senior officers at ranks equivalent to that of assistant surgeon general can participate as mentors.
Work experience “rotations,” in which midcareer professionals are temporarily assigned to a different part of their organization: The CDC Office of the Associate Director for Science offers these up to eight times per year to scientists across CDC. The rotation goals are to develop skills in scientific leadership, administration, and review and to broaden rotation participants’ view of both the agency and possible career paths. Several rotation alumni have gone on to attain senior leadership positions at CDC.
Coaching, a formalized professional mentoring relationship, which may be conducted on a fee-for-service, voluntary, or other basis: Coaching is a holistic approach to growth and specifically works to identify barriers to successful goal attainment. Best conducted in face-to-face settings, coaching may also take place via phone or video chat once individual goals have been identified. Initial sessions are usually 1 hour, with follow-up sessions of 30 minutes once focused goals are set. Coaching sessions are often concluded with assignments for the mentee to prepare prior to the follow-up sessions. Coaching is future oriented and comparatively short term, although periodic check-in appointments are common after initial goals are met.
1-hour online mentoring is offered for specific topics such as resume writing or interviewing skills, using remote video options. A Web link is established for reviewers to register, and another link for a mentee to register for review of their curriculum vitae (CV).
A professional organization or alumni “networking hour” provides the opportunity to network and for experienced alumni to pass along professional development advice.
Guided peer mentoring involves two 1-hour sessions where small groups of three to four participants apply didactic information and peer feedback to develop or improve their CV summary paragraphs.
Based on our collective experience, promising practices in structured mentoring include having the mentee define goals for the mentoring, initially without the mentor’s assistance. The mentor then provides feedback, usually in a discussion setting. Mentee-defined goal-setting ensures that the mentoring is appropriately focused. Specific tasks to incorporate into mentoring include reviewing and revising CVs and writing samples; practicing oral communications such as a mock interview, brief oral summary of qualifications, or interest in a specific position or project pitch; and developing a mentee’s Web presence on professional networking sites (e.g., LinkedIn, ResearchGate). A CV should be viewed as both a key writing sample and a record of training, experience, and skills. Mentors should always review the CV of a mentee with whom they establish an ongoing relationship, and mentees should be encouraged to revise their CV at least twice a year. It is useful for the mentor, at the beginning and end of time-limited mentoring relationships, to conduct intake and exit interviews to assess readiness, set expectations and goals, and later assess progress and discuss next steps (Griffey, 2014). This will be particularly beneficial for mentees interested in working toward a specific goal, such as putting forward a competitive application for an upcoming position or developing a specific skill set, such as scientific writing, oral presentations, or message-driven public outreach.
Informal mentoring has long existed in the workplace and includes onetime consultations concerning specific projects or scientific manuscripts. Conversely, for long-established relationships in which the mentor has strong problem-solving and academic skills and the trust of the mentee (Brownson, Samet, & Thacker, 2002), mentors and mentees may wish to periodically review goals, progress, and the structure of the relationship. Less frequent or shorter meetings may be needed as mentees progress in their careers. Mentor–mentee relationships are not intended to substitute for other workforce development activities such as skills training, journal clubs, or formal leadership training.
For organizations wishing to begin or enhance structured mentoring activities, form should follow function. The program’s design should be appropriate to the needs of mentor and mentee and organizational type and setting. Factors to consider include time availability of mentors and mentees, adequacy of the mentor pool, and mentoring program goals. Table 1 summarizes characteristics for the structured mentoring options described here.
Concluding Remarks
Mentoring crosses the career life span, from education and postgraduate training through early-, mid-, and late career phases. Mentoring should be a priority with organizational or agency leadership and may be of particular value to senior professionals who are responsible for staff development within their organizations. No one should consider themselves too senior to have a mentor, coach, or other trusted individual with whom they can consult about career and professional issues. The CDC Director, Dr. Thomas Frieden, has publicly acknowledged the influence of mentors on the development of his career (Schuppe, 2014) and has participated within CDC in a variety of mentoring activities as a mentor.
Individuals at all levels of public health can also join professional organizations and alumni clubs that give them access to mentoring programs that can supplement workplace programs and help professionals demonstrate ongoing career development and growth. Online, there are a wide range of individuals and organizations blogging about mentoring, with some providing additional resources such as tool kits and case studies. Pinterest lends itself to aggregating a variety of information with its many boards labeled “Mentoring.” These boards typically go beyond journal articles to include blog posts, gray literature, infographics, and articles from association and professional e-magazines such as in the example at www.pinterest.com/suego1/mentoring-resources-and-articles/.
In our view, mentoring is an ongoing process that should be mutually beneficial, an assessment supported by the global health literature (Cole et al., 2016). A recent commentary focused on academic medical settings pointed out that mentors may not always have the best interests of mentees at heart (Chopra, Edelson, & Saint, 2016). While this might be true in public health settings as well, in our experience most mentors value the advancement of their mentees. Positive outcomes of mentoring for mentees may include promotion and career progression. Positive outcomes for organizations that encourage mentoring include identification and development of the next generation of leadership.
Footnotes
Acknowledgements
The authors acknowledge Rick Colbert, Stephen B. Thacker CDC Library, for literature search assistance, and Dr. Mary Ari, Centers for Disease Control and Prevention (CDC) Office of the Associate Director for Science, for developing the work experience rotations described in this article. The authors also wish to acknowledge the various mentoring programs (structured and others) and the participants in them that have provided the range or experiences. Mention of specific websites does not imply any endorsement on the part of CDC or the authors. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the CDC.