
Abstract
More than a tenth of the U.S. population (13% = 41 million people) is currently living in poverty. In this population, the socioeconomic, cultural, and environmental conditions have detrimental health effects such as higher rates of chronic diseases, communicable illnesses, health risk behaviors, and premature mortality. People living in poverty are also deprived of social, psychological, and political power, leading to continuation of worsening health and chronic deprivation over generations. The health of individuals living in poverty poses greater challenges from policy, practice, and research standpoints. Public health professionals are poised uniquely to be advocates for the marginalized, be the resource persons for health education, implement health promotion programs, and conduct research to understand health effects of poverty and design tailored and targeted public health interventions. In this article, we summarize the opportunities for public health practice with individuals living in poverty.
Introduction
There is increasing recognition of the significance of social determinants of health (e.g., poverty, education, racial segregation, etc.) on health disparities among various segments of the population. Given the significance of social determinants (“causes of the causes”) of health status, we review income disparities and health impact of poverty across various segments of society and offer suggestions on how health promotion professionals can help reduce financially induced health disparities.
Financial Disparities In Society
The American median household income before taxes in 2016 was $59,039 (includes salary, interest on savings/investments, rent received, etc.). By race/ethnicity, the median incomes in 2016 were as follows: Asian ($81,413), White ($65,041), Hispanic ($47,675), and African American ($39,490; Bricker et al., 2017; Semega, Fontenot, & Kollar, 2017). Earning power is directly related to level of education, and the median incomes for 2016 based on education were as follows: no high school diploma ($26,500), high school diploma ($40,500), some college ($47,700), and college degree ($92,100). Median income differences by gender for full-time workers were $51,640 for men versus $41,554 for women. Using median incomes does not give a complete picture of the population income distribution. For example, almost 60% of African American households earned less than $50,000 in 2016, while 38.9% White households earned less than $50,000. Roughly half of American jobs pay $37,000 or less each year, and about one quarter pay $23,000 or less (Bricker et al., 2017; Kneebone & Holmes, 2016; Semega et al., 2017).
In 2016, there were 40.6 million American people (12.7%) who lived in poverty. Poverty is determined by household size and official monetary thresholds before taxes and may vary by demographic characteristics. For example, poverty rates for race/ethnicity in 2016 were as follows: African Americans (22%, 9.2 million), Hispanics (19.4%, 11.1 million), Asians (10.1%, 1.9 million), and Whites (8.8%, 17.3 million). Age differences for poverty rates were under 18 years of age (18%, 13.3 million), 18 to 64 years of age (11.6%, 22.8 million), and 65 years of age or older (9.3%, 4.6 million). Poverty rates by family structure were married-couple families (5.1%, 3.1 million families), male householders (13.1%, 847,000 families), and female householders (26.6%, 4.1 million families; Kneebone & Holmes, 2016; Semega et al., 2017).
The “very poor” (those under 50% of their poverty threshold) rates in 2016 were as follows: African Americans (10.8%, 4.6 million), Hispanics (7.6%, 4.4 million), Asians (5.2%, 1 million), and Whites (4.1%, 8 million). “Extremely poor” neighborhoods are those where 40% or more of the population lived below the federal poverty levels. In 2010-2014, 14 million Americans lived in such neighborhoods, more than twice as many as in 2000. Based on race, 5.5% of Whites, 17.6% of Hispanics, and 25.1% of African Americans lived in “extremely poor” neighborhoods. The 100 largest metropolitan areas were home to more than 70% of individuals living in extremely poor neighborhoods (Bricker et al., 2017; Kneebone & Holmes, 2016; Semega et al., 2017).
Health Impact Of Poverty
Recent research has found that the difference in life expectancy between the top 1% and bottom 1% of the income distribution of the United States is 15 years for men and 10 years for women. Other researchers have estimated that individual-level poverty caused 133,000 deaths in 2000, income inequity caused 119,000 deaths, and living in area-level poverty 39,000 deaths (Braveman & Gottlieb, 2014; Chetty et al., 2016; Galea, Tracy, Hoggatt, DiMaggio, & Karpati, 2011).
Poverty influences health at each life stage, often resulting in a multiplicative effect creating unhealthy existences, and has a biologically plausible explanation for how it affects health (Figure 1; Galea et al., 2011; Kondo, 2012). Upstream social determinants (distal factors) of health include factors such as poverty, poor education, prejudice/discrimination, access to health care, employment, environmental pollution, government policies, social services, and housing—factors that cannot be changed through an individual acting alone. Whereas downstream behavioral determinants (proximal factors) of health include stress and harmful coping behaviors (health risk factors)—these are under greater control by an individual. Figure 1 is an oversimplification of the complex pathophysiological changes (hypothalamic-pituitary-adrenal axis, sympathetic nervous system, and immune/inflammatory metabolic changes) that occur under acute and chronic stress in the presence of environmental stressors (poor nutrition, pollution, etc.). The result is chronic distress that leads to a variety of emotional and psychological changes (hypervigilance, hostility, depression). Depending on their culture, many will deal with their stress in unhealthy ways (Braveman, Egerter, & Williams, 2011; Braveman & Gottlieb, 2014).
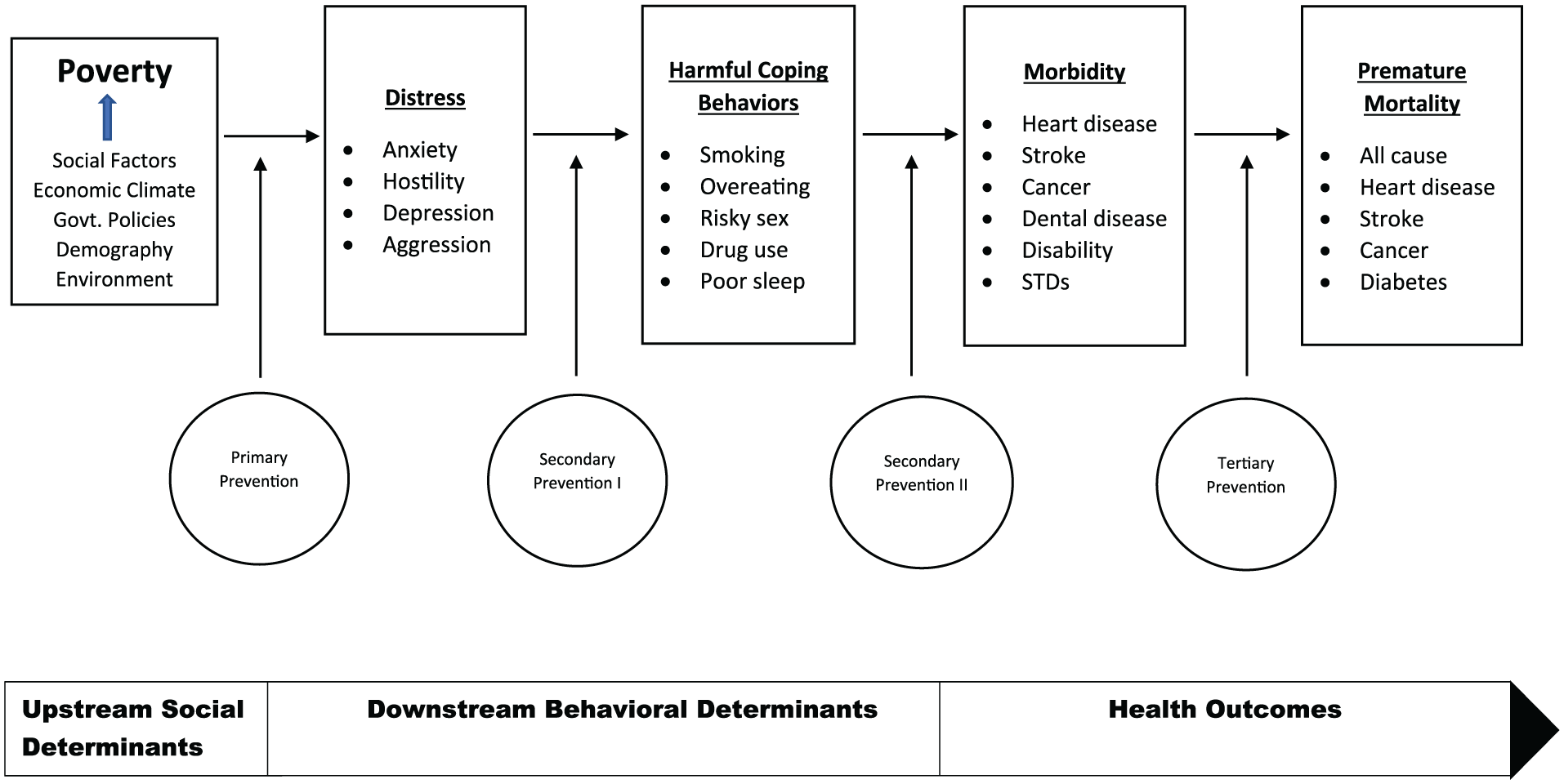
Pathway Linking Poverty to Disease and Premature Mortality
Poverty acts on families not only through the immediate effects of deprivation (lack of housing, food, transportation, etc.) but also through its chronic stress effects, creating an actual pathophysiological change (“wear-and-tear”) in people, referred to as allostatic load. The long-term outcomes of allostatic load and harmful health behaviors are a variety of morbidities, which if not adequately treated, may lead to premature mortality (Braveman & Gottlieb, 2014; Kondo, 2012). Chronic poverty increases the risks of coronary heart disease, hypertension, stroke, obesity, diabetes, respiratory diseases, cancers, substance abuse, HIV/AIDS, disability, dental diseases, and chronic kidney disease (Figure 1). Communities of poverty are more likely to be disorganized and experience higher rates of crime, violence, and environmental stressors (Braveman et al., 2011; Chetty et al., 2016; Stringhini et al., 2010).
Effects of poverty manifest over a lifetime warranting the study of poverty from a life course health development perspective. In the life course health development framework, health is considered to be a consequence of multiple determinants operating in nested genetic, biological, behavioral, and social contexts that change as a person develops—with economic influences having a predominant role in health outcomes (Halfon & Hochstein, 2002). For example, low birth weight in poor infants is associated with a higher risk of diabetes, asthma, heart disease, attention deficit/hyperactivity disorder, infections, and premature mortality. Children in poverty are more likely to experience a greater incidence of acute and chronic psychological stressors, including family conflict, child abuse, single-parent families, and violence. Children from poor families have more emotional and behavioral problems, health risk behaviors, infectious diseases, childhood injuries, and chronic diseases. Children of the working poor (those without paid sick leave) are less likely to receive care, and when they receive care, it is more likely to be of limited quality (Braveman & Gottlieb, 2014; Halfon & Hochstein, 2002).
Advocacy And Policies For Reducing Poverty
Health promotion professionals spend the vast majority of their work in the area of Secondary Prevention II (downstream; Figure 1). Health promotion professionals will not be part of the solution to reduce health disparities that exist between the poor and nonpoor if all of their efforts continue to be rescuing the poor from the stream of economic despair and behavior-induced morbidities. We must spend a commensurate amount of our efforts upstream where the major causes of health disparities are imbedded within the fabric of social determinants of health (Braveman et al., 2011; Braveman &Gottlieb, 2014). The gross economic inequalities that currently exist must be changed, and until they are, we must strive to ensure a strong safety net with few gaps to help ensure that the most vulnerable do not fall through the increasingly large gaps that have formed throughout our current safety net. There are more than 100 government programs that assist poor and low-income Americans, too numerous to review here. However, there are a few major safety net programs that play the biggest role in raising the poor above the poverty line (Table 1; U.S. Government, 2017). The safety net programs raised some 39 million people out of poverty in 2013 and reduced the severity of poverty for millions more; however, because safety net programs (other than the health insurance programs and Social Security) were 9% of the federal budget ($366 billion out of $3.9 trillion in 2011) they are targets for reducing the federal budget (Center on Budget and Policy Priorities, 2017; Rachidi, 2017).
Government Benefits and Actions for Public Health Professionals
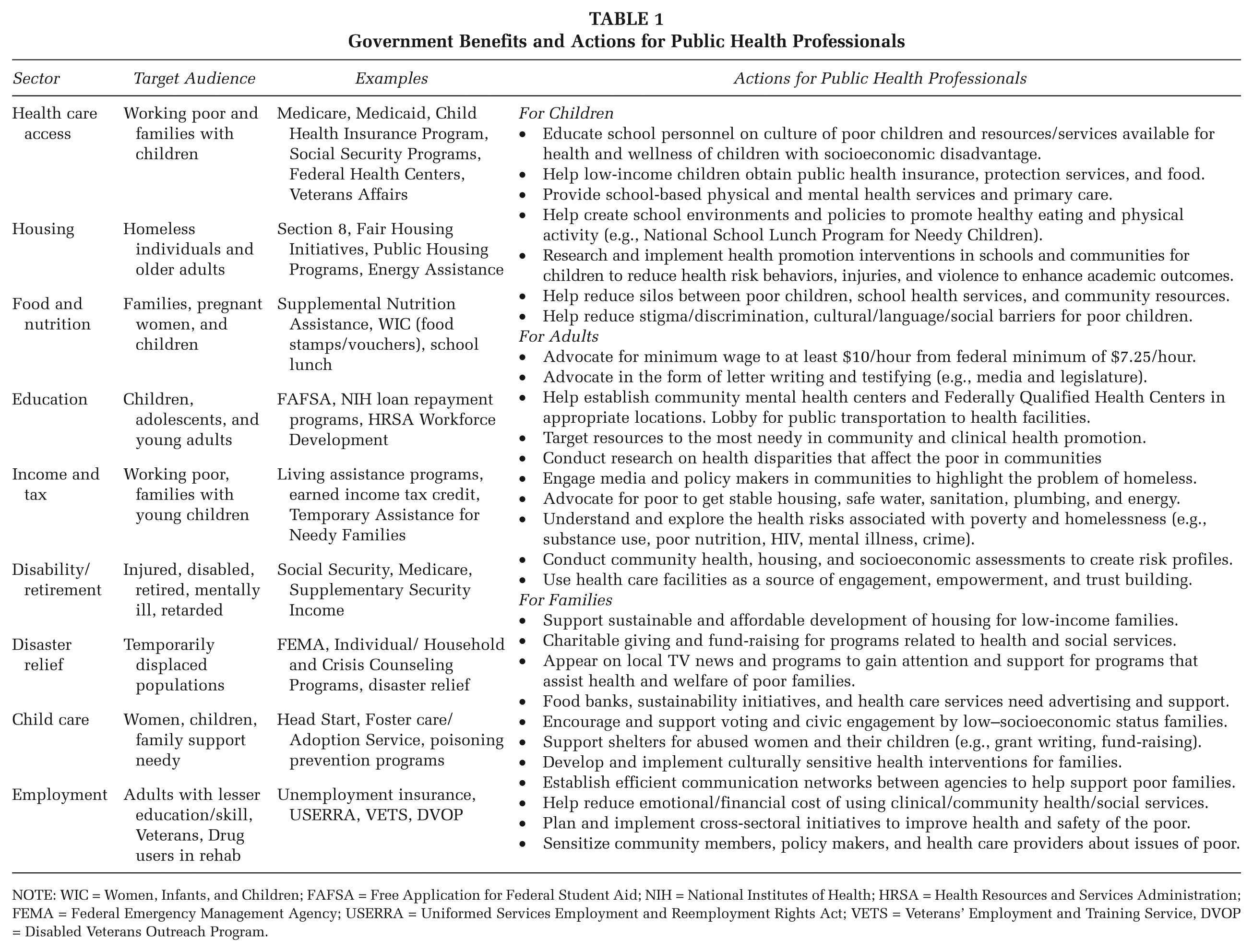
NOTE: WIC = Women, Infants, and Children; FAFSA = Free Application for Federal Student Aid; NIH = National Institutes of Health; HRSA = Health Resources and Services Administration; FEMA = Federal Emergency Management Agency; USERRA = Uniformed Services Employment and Reemployment Rights Act; VETS = Veterans’ Employment and Training Service, DVOP = Disabled Veterans Outreach Program.
Despite the constant pressure or threat of budget cuts, public health professionals can help maximize the use of existing resources and work for additional health and economic resources for the poor. This will require a paradigm shift in our thoughts and actions. We must play a strategic role in the broader social, economic, political, and health care climate of society. Table 1 suggests avenues and practical strategies to empower those who live in poverty. Consistent with our professional responsibilities and competencies, public health educators must (1) assess needs and willingness for those in need to acquire available assistance, (2) become fluent with the existing resources and programs available throughout their communities and serve as a resource person, (3) identify upstream strategies that work to systemically eliminate poverty, and (4) advocate for health and social welfare of the poor (National Commission for Health Education Credentialing, 2017). In addition to assisting individuals to practice healthy behaviors and adequately use health and social services, public health educators must be willing to continue learning about social injustices and differences that negatively affect health and magnify health disparities.
Conclusion
Poverty is detrimental to public health and financial well-being has a substantial protective effect. Therefore, it is not easy to reduce some public health issues until we address upstream disparities. Can public health educators ignore poverty as a critical determinant of public health? If not, what are our roles and responsibilities? What actions do we need to take? Can we still ignore the complex interplay between poverty, unemployment, poor housing, unsustainable communities, lack of access to health care, and individual well-being and public health? This commentary calls for greater intersectoral action, robust public health practice that works with economic and social forces outside the health sector. To alleviate the complex and multilayered impact of poverty on health, public health professionals have the opportunity and skills to advocate for and implement policies and practices through intersectoral mechanisms that are robust, feasible, evidence based, oriented toward outcomes, applied systematically, sustainable, and appropriately resourced.