
Abstract
Background. Nearly 1,300 children in the United States die because of firearm-related injury each year and another 5,790 survive gunshot wounds, making the prevention of firearm-related unintentional injury to children of vital importance to families, health professionals, and policy makers. Objective. To systematically review the evidence on school-based and community-based gun safety programs for children aged 3 to 18 years. Study Design. Systematic review. Method. Twelve databases were searched from their earliest records to December 2016. Interventional and analytic studies were sought, including randomized controlled trials, quasi-experimental studies, as well as before-and-after studies or cohort studies with or without a control that involved an intervention. The low level of evidence, heterogeneity of studies, and lack of consistent outcome measures precluded a pooled estimate of results. A best evidence synthesis was performed. Results. Results support the premise that programs using either knowledge-based or active learning strategies or a combination of these may be insufficient for teaching gun safety skills to children. Conclusions. Gun safety programs do not improve the likelihood that children will not handle firearms in an unsupervised situation. Stronger research designs with larger samples are needed to determine the most effective way to transfer the use of the gun safety skills outside the training session and enable stronger conclusions to be drawn.
Guns are a ubiquitous part of American culture. There are more than 310,000,000 guns in circulation in the United States (Ingraham, 2015). This numerical reality makes the prevention of firearm-related unintentional injury to children and youth of vital importance to parents and families as well as to school, public health and child health professionals, and policy makers. As K. Fowler, Dahlberg, Haileyesus, Gutierrez, and Bacon (2017) report, firearm injuries are the third leading cause of death for all children aged 1 to 17 years. Gun deaths account for twice the number of deaths from cancer, 5 times the deaths from heart disease, and 15 times the deaths from infections (GBD 2013 Mortality and Causes of Death Collaborators, 2014; Palfrey & Palfrey, 2013). Only motor vehicle traffic injuries claim more lives, whose rate fell approximately 50% since 2000, while firearm mortality dropped only 10% in that same time (K. Fowler et al., 2017; Nelson, 2017).
While death is the most egregious result of firearm-related unintentional injury for children, it is not the only serious outcome. Firearm-related injury, in addition to being more frequently fatal, also more frequently requires major surgery as compared to other types of injury. Firearm injury sends thousands of children to the emergency department with open wounds, fractures, brain trauma, and spinal injuries. Overall, nearly 1,300 children in the United States die in shootings each year and another 5,790 survive gunshot wounds (K. Fowler et al., 2017). About 15% of children with a firearm-related injury will sustain traumatic brain injury or an injury to the nerves or spinal cord, necessitating years of often painful, emotionally challenging, and costly rehabilitation (Kalesan, French, Fagan, Fowler, & Galea, 2014).
Beyond direct physical harm, there are also mental health challenges stemming from direct and indirect exposure to a firearm-related injury, making each single firearm injury one that affects many victims. The fear, anxiety, and elevated stress children experience resulting from direct and indirect exposures may have serious psychological health consequences and has been reported as a predictor for the development of posttraumatic stress disorder in children and adolescents (P. J. Fowler, Tompsett, Braciszewski, Jacques-Tiura, & Baltes, 2009; Penn State, 2012). In addition, activating the body’s physiologic stress mechanisms increases risks of serious chronic health conditions, including heart disease and depression.
The economic burden associated with firearm injury is significant. Using injury data from the Centers for Disease Control and Prevention, Miller (2012) estimates annual firearm injury costs average $645 per gun in America. These costs include medical and mental health care costs, criminal justice costs, and the value of pain, suffering, and lost quality of life. Spitzer, Staudenmayer, Tenekoon, and Spain (2017) reported that approximately $730 million dollars annually is spent on the initial hospital admission for gun-related injuries. Government insurance through Medicaid and Medicare covered over 40% of these costs, and another quarter of the costs were borne by uninsured individuals. Spitzer et al.’s (2017) calculations do not include the cost of hospital readmissions, rehabilitation, long-term health care, or emergency department care that does not lead to a hospital admission.
While the American Academy of Pediatrics (2015) notes that the safest home for children is one that does not include the presence of a gun, most unintentional shooting deaths among children do occur in the home with an additional one third occurring at the house of a friend or relative (Luo & McIntire, 2013). Gun safety in the home is complicated by differences in family beliefs, expectations, and actions. Despite parents believing that safe firearm storage is important for child protection and safety, Baxley and Miller (2006) report that 85% of parents did not practice safe gun storage. Jackman, Farah, Kellermann, and Simon (2001) found that 72% of the gun-owning parents believed their child could differentiate a toy gun from a real gun, even though this is an unlikely developmental capability for young children.
One strategy to reduce firearm-related unintentional injury is the development of firearm safety training programs designed to teach children how to respond in the event they encounter a firearm in an unsupervised environment. Their purpose is to eliminate or minimize the risks of unintentional death, injury, or damage caused by improper possession, storage, or handling of firearms.
Three major approaches are used: “just say no” approaches, in which authority figures provide information passively and tell children to stay away from guns (National Rifle Association for Legislative Action, 2001); skills-building or active approaches (Miltenberger et al., 2009), which attempt to teach children skills they can use to resist playing with or touching guns; and knowledge-based approaches (Liller et al., 2003), in which children are passively provided information and printed material about gun safety. These gun safety training programs seek to instill appropriate responses by following specific rules. Children are taught to treat firearms with respect, and they are strongly discouraged from playing or toying with firearms. Yet children in homes where all guns were stored locked away were just as likely as children in homes with firearms stored unlocked to report having handled a gun in the home without adult supervision (Jackman et al., 2001).
Research findings on the effectiveness of interventions to prevent firearm injury are equivocal. Of those programs developed specifically for children, the Eddie Eagle GunSafe program is the most recognized and implemented (National Rifle Association for Legislative Action, 2001). The Eddie Eagle program has educated more than 15 million children since 1988, with an estimated 700,000 children receiving Eddie Eagle firearm injury prevention training each year. The main objective of the Eddie Eagle GunSafe program is to teach children what they should do if they find a firearm, that is, “stop” and do not touch the firearm. In a study comparing the Eddie Eagle GunSafe program of firearm safety with a behavioral training program, it was found that using knowledge-based learning materials was less effective for teaching children desired skills compared with programs incorporating active learning approaches (e.g., modelling, rehearsal, and feedback; Himle, Miltenberger, Gatheridge, & Flessner, 2004).
As well, Jackman et al. (2001) reported that as researchers watched pairs of boys left alone with a concealed inoperative handgun through a one-way mirror, most boys found the gun, handled it, and pulled the trigger. Only one child went to tell an adult about the gun, and he was teased by his peers. In a similar study, Hardy (2003) found that even following gun admonitions, when left alone in a room with a gun, school-aged boys were more likely to touch the gun than other forbidden objects, such as cigarettes. Although systematic reviews exist on the effectiveness of general violence prevention programs, a search of Cochrane, Campbell Collaboration, Joanna Briggs Institute (JBI) Libraries, and PubMed (clinical queries/systematic review) did not reveal any reviews focused on gun safety strategies for use with children.
Objective
Given the health, societal, and economic burden of firearm injuries in children, this review used PICO (participants, interventions, comparisons, outcomes, and study design) to answer the question: “What teaching strategies (I/C) are most effective (S) in teaching children aged 3 to 18 years (P) the skills of gun safety (O)?” The overall intent of this article is to provide practical and actionable information for health promotion practice.
Method
The “Preferred Reporting Items for Systematic Reviews and Meta-Analyses” (PRISMA; 2015) statement, the JBI (2014) method of critical appraisal, and the Agency for Healthcare Research and Quality (2014) guidelines for determining levels of evidence were followed in this review. An a priori protocol was used (Holly, Porter, & Jadotte, 2015).
Search Strategy and Selection Criteria
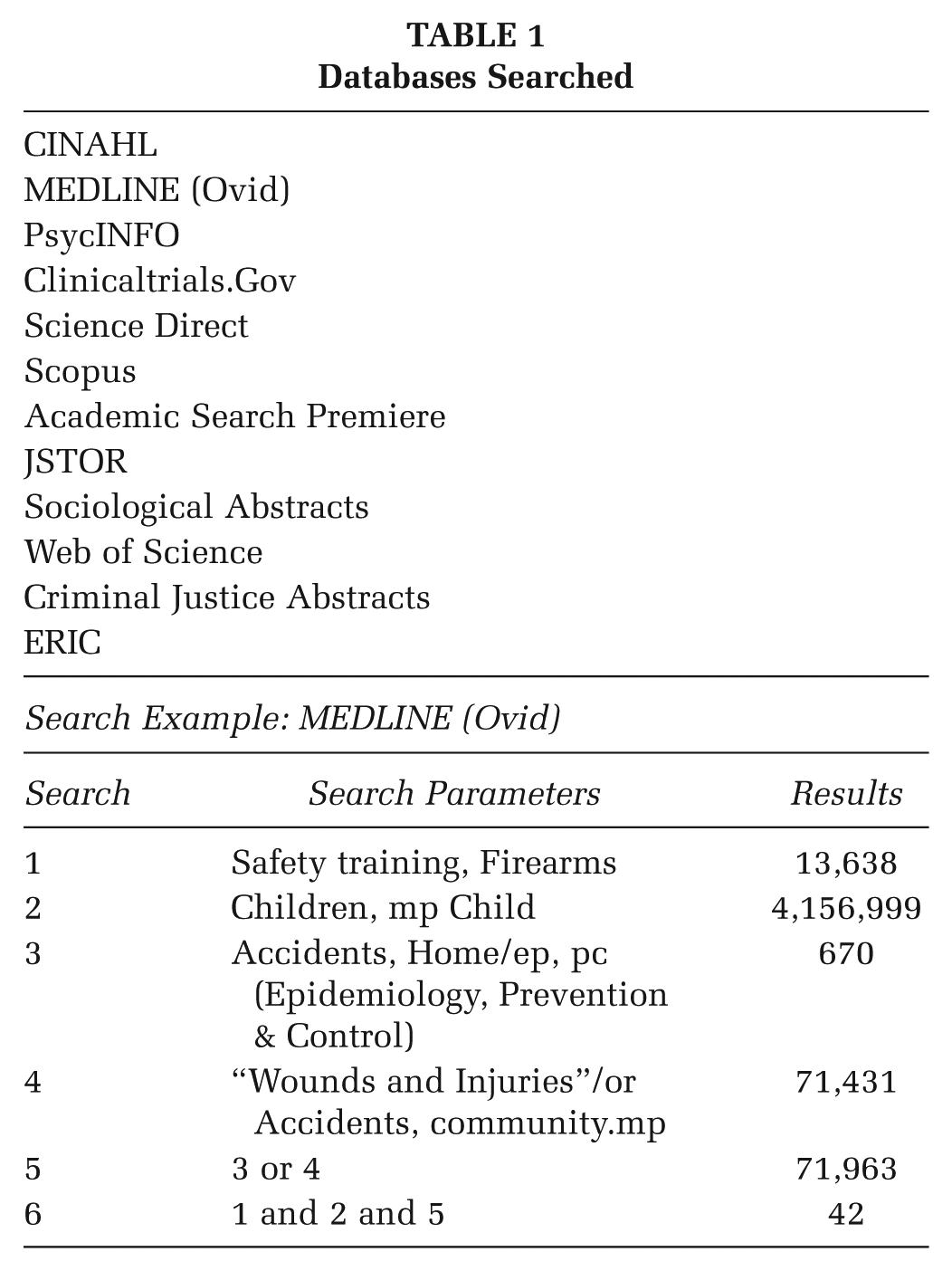
To be included in this review, studies had to be interventional, that is, randomized controlled trials, quasi-randomized controlled trials, or before-and-after studies or cohort studies with or without a control that involved an intervention. The inclusion criteria were (1) the program was targeted to children aged 3 to 18 years; (2) the study focused on knowledge-based and/or skills-based interventions used in school (including after school programs) or community (including the home) programs; (3) a description of the intervention was provided; and (4) outcomes were measured. Studies were further limited to U. S. settings and English language publications. Violence prevention programs not targeted to gun safety and combined safety programs in which the gun safety results could not be differentiated were excluded. To identify studies, using the keywords “gun safety training and children” 12 databases were searched from their inception to December 2016 (see Table 1). Additionally, the reference lists of the identified documents were searched for eligible studies (i.e., ancestry search). An Internet search using Google Scholar was also conducted to identify studies not published in the conventional literature (i.e., grey literature search). Two reviewers screened all articles that were identified by title and abstract against the inclusion criteria.
Databases Searched
The Intervention
Studies were sought that used either a passive, active, or combination teaching strategy intervention. Passive, or information-based strategies, provide children with information about safety threats and safety skills but no opportunity to practice these skills. The focus of this approach is to teach children that guns are not toys and that they should not play with them using discussion, video, or written material.
Active strategies included role modeling, role-play, and specific feedback on behavior. Also called behavioral skills training, this approach to teaching has been used to effectively teach abduction prevention skills (Johnson et al., 2006), poison recognition skills (Dancho, Thompson, & Rhoades, 2008), and pedestrian safety skills (Schwebel et al., 2014). Often an “in situ” or simulated exercise was used that allowed children to practice what they would do in a real-life situation using role-play. Safety skills acquisition are then assessed via observation and video monitor, and the observer goes to the participants’ area once the assessment is completed. Immediate, corrective feedback is provided by the observer if the child failed to use the skills. In some cases, remediation would occur.
A combined approach involves the use of both active and passive strategies. For example, children would attend a lecture/discussion on gun safety, be given written materials on gun safety, and then placed in a simulated situation using role-play and immediate corrective action.
Quality Assessment
Each paper selected for retrieval was assessed for methodological quality using the appropriate critical appraisal instrument based on study design from the JBI (2014). Each team of reviewers compared the results of their review and presented their agreed-on results to the entire team, which made a joint decision to include or exclude the study. Any disagreement between the reviewers was discussed with the entire team until consensus was achieved. The appraisal criteria included questions regarding sample selection, inclusion criteria, assessment of outcomes, sufficiency of the sample description, reliability of outcome measures, and appropriateness of statistical measures used.
Data Extraction
Data were extracted from papers using a de novo data extraction tool. For each study, the following information was extracted: age range of children in the program, sample size, interventions used, place of the program, and outcomes. The collected data were then represented in a table of evidence for comparison and discussion (see Table 2). The low level of evidence, heterogeneity of studies, and lack of consistent outcome measures precluded a pooled estimate of results. Given that the results of heterogeneous studies should be viewed with caution, as bias can be interjected, we took care to detail the search and appraisal process to strengthen the reliability of review findings. The final analysis for this review, therefore, is a best evidence synthesis of intervention characteristics and outcomes based on type of intervention teaching strategy: (1) passive, (2) active, or (3) combination—both active and passive.
Included Studies

Not all studies reported children’s age and gender. bNot all studies reported complete statistical analysis. cFrom Oxford Centre for Evidence-Based Medicine Working Group (2011): Level 1 = systematic review; Level 2 = randomized controlled trial; Level 3 = observational studies, cohort studies nonrandom sample; Level 4 = case series, case control studies.
Results
A total of 298 studies were identified. Of these, 209 were excluded as they were duplicate studies found across databases; 31 were selected for retrieval and 10 were included in this review (see Figure 1). The 21 studies not included were the wrong population (N = 10), not an educational program (N = 5), literature review (N = 2), or not a research study (N = 4; see Figure 1). Of the included studies, one was a randomized controlled trial (Hardy, 2003), and one was a quasi-experimental study (Howard, 2005). The other eight were pretest/posttest studies (Gross, Miltenberger, Knudson, Bosch, & Breitwieser, 2007; Hanratty, Miltengerger, & Florentino, 2016; Liller et al., 2003), posttest only with a control group (Gatheridge et al., 2004; Himle et al., 2004; Kelso, Miltenberger, Waters, Egemo-Helm, & Bagne, 2007; Miltenberger et al., 2009), or posttest only with no control (Jostad, Miltenberger, Kelso, & Knudson, 2008).
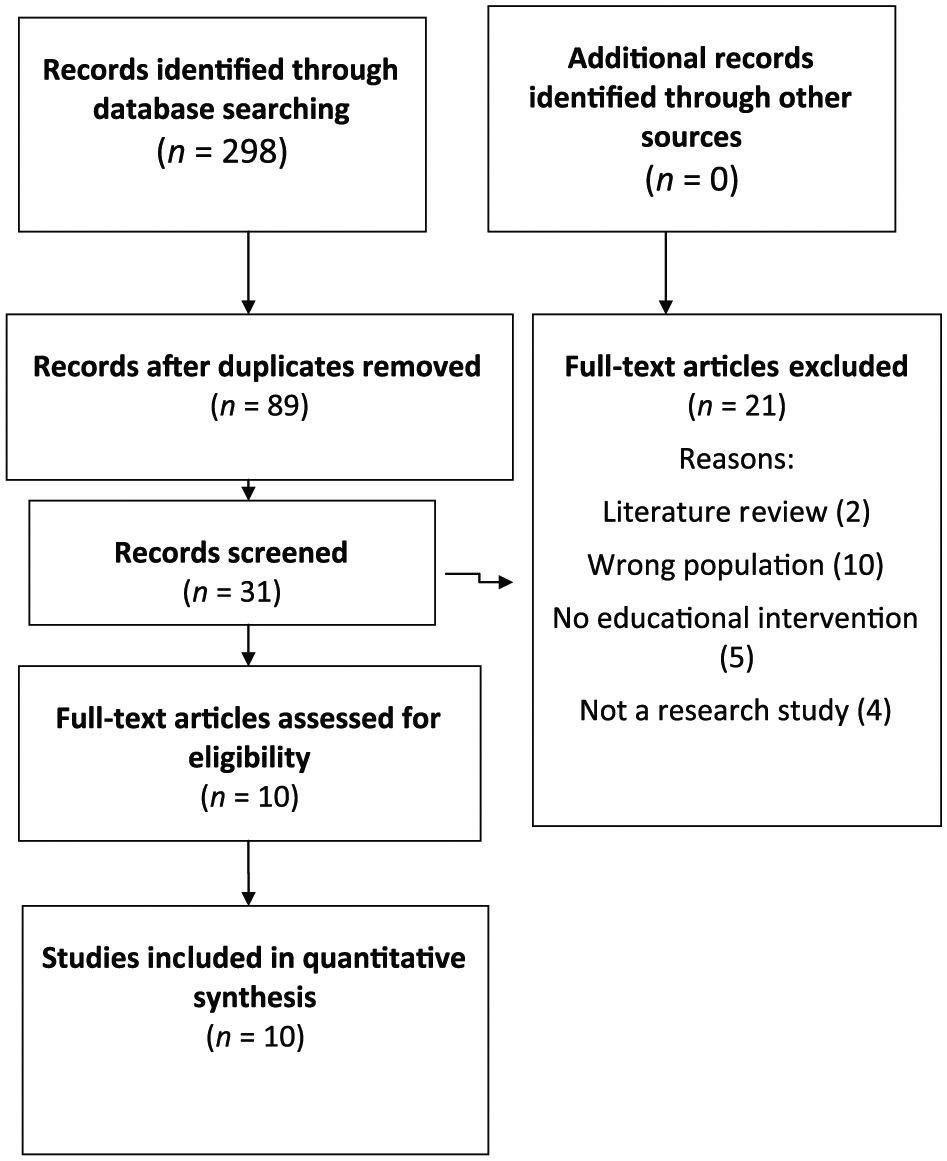
PRISMA Flow Diagram
As noted in Table 2, of the included studies, five used active learning strategies, one used passive learning strategies, and four used a combination of passive and active learning strategies. Four of the studies took place in a school environment and five in the community and one study took place both at home and in the community. Three of the included studies compared the results of using the Eddie Eagle program with the more active behavior skills training program. There were 744 participants across the studies, ranging in age from pre-K/child care to Grade 4, with a median age of approximately 5 years. No studies were located whose participants were middle or upper (high) school students.
Levels of evidence for the included studies are presented in Table 2. Most (N = 8) were either are Level 3 (N = 4) or Level 4 (N = 4) evidence, meaning that the studies were of low quality and health education providers and others should be flexible and cautious in using these results.
Discussion
Unintentional firearm injury among children is a significant public health and social concern. Although firearm injury mortality rates for children declined between 2006 and 2013, an increase accounting for over 10% of all deaths among these ages was seen in 2014 and 2015. Firearm injuries are the third leading cause of death for all children aged 1 to 17 years (K. Fowler et al., 2017). When the age is extended to 19 years, firearm injuries accounted for over 14% of all deaths in 2015, meaning that in one of every seven children aged 1 to 19 years who died, an intentional or nonintentional gunshot wound was the cause (Nelson, 2017). Despite the social and economic burden imposed by firearm injury in the United States, an exhaustive search of the published and grey literature revealed a dearth of high-quality evidence. Only limited evidence (i.e., consistent findings in one or more low-quality studies) was identified (van Tulder, Furlan, Bombardier, Bouter, & Editorial Board of the Cochrane Collaboration Back Review Group, 2003).
Children need to know how to be safe around guns as the relative accessibility of guns in the United States is the highest among developed countries (Branas et al., 2017; World Health Organization, 2014). Increasing a child’s knowledge about how to respond safely when unsupervised access to a gun occurs makes sense. However, an increase in knowledge provides no certainty that children will translate this knowledge to a real-life situation. Using knowledge as the outcome variable, therefore, is insufficient for teaching gun safety skills to children, although some studies in this review reported short-term knowledge gain (Hanratty et al., 2016; Kelso et al., 2007; Liller et al., 2003).
Programs that used active learning strategies (e.g., modeling, simulation, feedback) were somewhat more effective at teaching gun safety skills as assessed by supervised role-play, but the majority still failed to teach the children to use the skills outside the context of the training session. For example, in Hardy (2002), 70 children between the ages of 4 and 7 years were randomly assigned to participate in a weeklong firearm safety program or to the control group. After the program, pairs of children were observed in a structured setting in which they had access to a semiautomatic pistol. A total of 53% of the pairs handled the gun. In other words, the intervention had no effect on children’s likelihood of playing with guns. In another study (Himle et al., 2004), programs were effective for teaching children to repeat the gun safety message and to perform gun safety skills during a supervised role-play, but the skills were not used when the children were assessed via real-life (simulated) assessments. However, Hanratty et al. (2016) did find that while active learning implemented by a teacher was not effective in teaching safety skills to young children, children were able to correctly model behavior with an enhanced component, (i.e., access to preferred activities and escape from further training), suggesting that children may not be fully understanding the significance of gun safety. The very small sample size (N = 5) in this study, however, limits generalizability.
To address active versus passing teaching strategies more closely, three of the studies in this review compared the passive learning Eddie Eagle program with the more active behavior skills training program. In two of these studies (Himle et al., 2004; Kelso et al., 2007), contrary to what was predicted, children in the Eddie Eagle and the active learning conditions did not differ during the in situ (simulated) assessment, suggesting that the programs did not differ in teaching children to perform the target skills in a realistic situation, although verbally all children demonstrated increased knowledge. In the Gatheridge et al. (2004) study, when children were not aware they were being assessed in a naturalistic setting, children in the skills training group were more likely to perform the desired skills than were children in the Eddie Eagle group, H(1, n = 30) = 8,65, p < .01.
The instructor who taught the gun safety skills lessons varied across the studies and included peer tutors, parents, teachers, and a nurse as well as the researchers conducting the studies. There was little variation across the studies in terms of outcomes.
In addition, although our search strategy looked for studies involving children aged 3 to 18 years, the 10 included studies only addressed children aged 4 to 9 years. This is a significant gap as the Youth Risk Behavior Surveillance System (Centers for Disease Control and Prevention, 2016) reported that 5.3% (N = 13,263; confidence interval [CI: 4.6, 6.1]) of the high school respondents reported carrying a gun at least once during the 30-day period preceding the survey and 4.1% (3.5% to 4.7%), 15,468 reported carrying a gun on school property.
This is important on two fronts—development and research gaps. From a child and adolescent development perspective, what works and matters with the younger child is often different from what works with an adolescent. Certainly, the developmental abilities of a 4-year-old are different in the cognitive and motor domains compared to a 17-year-old, and even to a 7-year-old. Even within the adolescent age-group, there are cognitive development variations along the age trajectory. So, as always in child health and safety, it is important to consider the child’s age and developmental abilities.
Gun-related injuries and deaths are a significant issue for adolescents. Little is known about the health and well-being of those who witness or survive unanticipated episodes of gun violence, which creates situations of traumatic loss and grief. Developmentally appropriate learning strategies to prevent and limit adolescent gun-related injury need more attention. Prevention strategies for unintentional gun-related injuries for the younger adolescent male population may be of special importance (Institute of Medicine & National Research Council, 2013).
Transferability of learned material among different contexts (i.e., home vs. school, home vs. friend/relative home) needs consideration. With most unintentional gun injuries and deaths occurring in the family, relative, or neighbor’s home, skills learned in the school setting need applicability to the home setting. In the same vein, gun safety advocates need to reinvigorate their efforts targeted toward parents, grandparents, and other adult caregivers. Optimal safe gun storage may still be the preferred choice to keep children and adolescents safe from unintentional gun injury.
Conclusion
Gun safety programs do not appear to reduce the likelihood that children will safely handle firearms. The studies located and included in this review are of limited evidence (primarily Levels 3 and 4) due to small sample sizes, minimal statistical analysis, and lack of randomization, making a determination of effect size not possible; therefore, an evidence synthesis of study findings was done. More research is needed to determine the most effective way to transfer the use of the skills outside the training session and to ensure that those skills are sustainable. Rigorous, large-scale, and age- and developmentally appropriate studies are needed.