
Abstract
Kentucky youth (14.3%) smoke more cigarettes as compared to the U.S. average (8.8%), and Appalachian communities suffer disproportionately from tobacco-related diseases such as lung cancer. Training youth to become advocates is an effective strategy to improve health equity. This article describes the development and impact of a youth advocacy program to promote tobacco control policies in Appalachian Kentucky. Phase I (2017-2018): two ½-day trainings followed by monthly meetings with one high school (n = 20 youth). Trainings provided information on tobacco use, consequences, industry tactics, evidence-based tobacco control, and advocacy skills. Results provided support for expansion to Phase II (2018-20119): A 1-day training followed by monthly information sharing implemented in three counties (N = 80). Youth were surveyed before and 6-months posttraining during both phases. Phase I: At posttraining, 85% of youth believed they could reduce the amount of tobacco use in their community versus 66% at baseline. More students tried at least once to convince school or government officials to be more concerned about tobacco use (77% vs. 47%). Phase II: More students supported tobacco policies at posttraining survey and realized policies are an effective strategy to reduce tobacco use. At posttraining survey, students reported greater interpersonal confidence talking with others about tobacco-related issues, with a 24% increase in confidence talking with adults in their communities, as well as greater advocacy self-efficacy. Youth in Appalachia demonstrate desire to influence tobacco use and policy to improve health equity. Findings reinforce the need for collaborative public health interventions to promote ongoing training and support for youth living in high-risk communities.
Background
Although tobacco control efforts have made great strides since the Surgeon General’s report on tobacco over 50 years ago, tobacco continues to disproportionately affect lower income and less educated individuals, particularly those living in rural, Appalachian communities (American Lung Association [ALA], 2015; U.S. Department of Health and Human Services, 2014). Nationally, prevalence of cigarette smoking among U.S. adults is highest among those living in rural areas (28.5%) compared to urban (25.1%), small (22%), and large metropolitan areas (18.4%; ALA, 2015). Individuals living in Appalachian communities also report much higher rates of tobacco use than those in the non-Appalachian United States (Marshall et al., 2017), particularly those living in Central Appalachia, which includes almost half of Kentucky’s 120 counties. In fact, women and men from Appalachian Kentucky smoke at rates 1.8 and 1.6 times higher, respectively, than U.S. adults (Schoenberg, Huang, Seshadri, & Tucker, 2015). Tobacco use also has a greater impact on the health of individuals living in Appalachian communities. Deaths from three of the four leading causes of death in the United States (heart disease, cancer, and chronic lower respiratory disease) occur more frequently in Appalachia (Beatty et al., 2019). For example, chronic obstructive pulmonary disease–related death in Central Appalachia is twice that of the non-Appalachian United States, with the highest mortality rates among those living in the Appalachian counties of Kentucky (Beatty et al., 2019). These higher prevalence rates and tobacco-related health issues are in part due to socioeconomic factors, culture, and lack of tobacco policies (ALA, 2015). Both community- and policy-based strategies can help prevent tobacco use among individuals in Appalachia (U.S. Department of Health and Human Services, 2014).
Evidence-based methods to reduce tobacco use reinforce the importance of policy change, including smoke-free workplace laws and tobacco-free schools (Centers for Disease Control and Prevention [CDC], 2014; Fichtenberg & Glantz, 2002; Hahn, Rayens, Langley, Darville, & Dignan, 2009; Wakefield, Kaufman, Orleans, Barker, & Ruel, 2000). Tobacco policies, which take a population-based approach to improving health, have the potential to reach groups disproportionately affected by tobacco-related disparities (Beatty et al., 2019). While many states have succeeded in implementing evidence-based tobacco policies, others, particularly those serving Appalachian communities, lag behind in this effort (ALA, 2018). Kentucky, located in the Central Appalachian region, received an “F” grade in implementing smoke-free air laws and tobacco taxes (ALA, 2018), reinforcing the need to support advocacy efforts for evidence-based tobacco control in at-risk Appalachian communities.
The Office on Smoking and Health’s Best Practices in Tobacco Control reinforces the importance of engaging youth in tobacco control efforts (CDC, 2014). Training youth to become advocates for public health issues in their communities is an effective strategy to improve the health of a community (Klindera, 2001). Moreover, engaging youth to advocate for strong school, community, and statewide tobacco policies, especially in high-risk regions like Appalachia, can promote health equity (CDC, 2014). Building a cadre of youth advocates in traditionally underserved communities facing health-related disparities due to the consequences of tobacco use can strengthen the reach of evidence-based tobacco policies (CDC, 2014).
However, little is known about the best approach to train youth in tobacco control, particularly in rural Appalachian communities. Youth in Appalachian communities describe a deeply entrenched tobacco culture, reinforced by family and community surroundings, and many perceive that their communities are resistant to change (Hart et al., 2018). While much is known about enhancing self-efficacy to resist peer pressure to use tobacco, less is known about supporting youth self-efficacy to advocate for tobacco control. According to the Youth Empowerment Theory (Zimmerman, 1995), engaging youth in meaningful community activities helps youth gain the vital skills, responsibilities, and confidence necessary to become productive and healthy adults. According to Zimmerman (1995), “Empowerment theory connects individual well-being with the larger social and political environment, and suggests that people need opportunities to become active in community decision making in order to improve their lives, organizations, and communities” (p. 582). Within the tobacco control context, youth need to be not only empowered to believe that policy is an effective and appropriate tobacco use prevention strategy to reduce tobacco-related disparities in their communities (Ribisl et al., 2004) but also given the opportunity to participate in skills-based training to support self-efficacy to participate in advocacy activities.
Given the lack of research among youth in Appalachian communities, planning, implementing, and evaluating an intervention to help build capacity for comprehensive tobacco policy is warranted. This article describes the development and impact of an advocacy program on youth self-efficacy and efforts to promote tobacco control policies in underserved Appalachian Kentucky. While there have been other studies on youth empowerment and tobacco control, our study focuses on rural Appalachia in a tobacco-growing state with high tobacco use rates and weak tobacco control policies.
Method
The Youth Tobacco Advocacy Training (YTAT) program was initially developed and piloted in one rural Appalachian high school in academic year (AY) 2017-2018 (Phase I) and, with the support of the state, scaled up in AY 2018-2019 (Phase II) to include three counties in rural Appalachia serving middle and high school youth. All phases of the study were approved by the university’s institutional review board. Parental consent and youth assent were obtained prior to data collection during each phase. Letters were sent home to parents of participating youth via existing school protocols: Passive consent was employed, thus parents not wanting their child to participate were asked to return the signed form. Youth were given an assent form 1 to 2 weeks prior to the training and asked to return it the day of the training if they agreed to participate in the study. Students were able to participate in the training opportunity regardless of their desire to take part in the research. Evaluation data were collected for each phase, with refinement of data collection methods and instruments occurring after piloting measures in Phase I. Methods for program development and implementation, program description, and evaluation for both Phase I and Phase II are described below.
Phase I. Pilot Youth Tobacco Advocacy Training Program
Program Development and Implementation
One year before the pilot YTAT program began (AY 2016-2017), a subset of our research team met with community advocates, school officials, and adult mentors from a rural, Appalachian Kentucky county to gauge interest in tobacco control, identify adult champions, and better understand community needs and assets. The adult mentor of a high school student leadership group (N = 20) agreed for the leadership group to incorporate youth advocacy into their strategic plan and participate in Phase I (AY 2017-2018).
Program Description
The program was planned using the previously described youth empowerment theory as the conceptual framework (Zimmerman, 1995), which has also been operationalized for youth involvement in tobacco control (Holden, Evans, Crankshaw, & Ben-Davies, 2004). Phase I empowerment training emphasized changing attitudes, beliefs, and knowledge and provided the opportunity to obtain skills to enact change (Zimmerman, 1995). This included skill building for policy advocacy as a strategy aimed at affecting health equity and the health of participating communities (CDC, 2014; Klindera, 2001).
Students attended two ½-day advocacy trainings followed by monthly in-school meetings (AY 2017-2018). Training I was conducted in September by members of the research team, a college student studying public health, and community partners working in youth advocacy. Training I provided information on tobacco use and consequences, industry tactics to target youth and specifically those in rural communities, and local tobacco policies and an introduction to advocacy. Our team tailored the Taking Down Tobacco 101 training module offered online by Campaign for Tobacco-Free Kids (CTFK) to be appropriate for youth in the Appalachian community. We included Kentucky-specific data, made sure information was culturally appropriate by giving relevant examples and including pictures that would resonate with these youth, discussed community norms around tobacco use, and reinforced how influential the tobacco industry has been in rural Kentucky communities. As a follow-up skill-building exercise, youth were asked to complete a community tobacco assessment (King Ledford, Lucas, Dairaghi, & Ravelli, 2013) before Training II to help them identify areas of strength and need in their own community. Representatives from North Carolina’s YES (King Ledford et al., 2013), including two high school students and one adult facilitator, were contracted to implement Training II. Students learned about systems change, discussed findings of their community assessments, and developed policy advocacy skills. All content was framed with a youth empowerment lens, with the trained YES high school students responsible for implementing the majority of the content. The culminating experience was for youth to develop and present a stakeholder elevator speech related to tobacco policy in their community. Booster trainings were conducted during monthly in-school meetings, with topics ranging from e-cigarette education to developing effective media messaging. Biweekly communication was maintained by the principal investigator with the adult mentor to answer any questions, share resources, and provide support. All participating youth received promotional items during the training (e.g., pens, buttons, bracelets). Additional incentives were not provided for participating in the evaluation.
Evaluation
Phase I impact evaluation
Phase I participants were surveyed before (September 2017) and 7 months after both training sessions (April 2018) through paper-based surveys. The Phase I baseline survey was distributed during the first 15 minutes of Training I prior to any content being shared, and the Phase I post survey was distributed during the last monthly student group meeting. Phase I impact measures were developed based on the youth empowerment theory and its use with tobacco control efforts (Holden et al., 2004). Changes in youth attitudes and beliefs, knowledge, and skills in acting as effective social change agents are appropriate measures related to youth empowerment (Holden et al., 2004). Included subscales are summarized below.
Tobacco Policy Attitudes: This five-item instrument assessed degree of opposition or support towards tobacco control policies (Kentucky Health Issues Poll, 2018), with a four-choice response set ranging from strongly oppose to strongly support. The items were summed to create a total Tobacco Policy Attitudes score, with a potential range of 5 to 25 and higher scores indicating greater support. Sample items included, “Do you oppose or support laws to prohibit selling tobacco to minors?” and “Do you oppose or support laws making it illegal to buy tobacco until age 21?”
Group Efficacy: Three items were used to measure perception of the efficacy of their advocacy group relative to tobacco policy development (Holden et al., 2004). The items were rated on 4-point scale ranging from strongly disagree to strongly agree, and the items were added together to obtain the Group Efficacy score; the potential range was from 3 to 12, with higher values indicating a more positive perception of the group’s ability to advocate for policy. Sample items included, “This group can influence how adults in this community feel about tobacco”’ and “This group can reduce the amount of tobacco use in our community.”
Interpersonal Confidence: This instrument measured the confidence the participant has in their ability to convince others not to use tobacco, with separate items for family, teachers, and friends (Holden et al., 2004). The items were scored on a 6-point response option, with five of the choices ranging from I cannot do it to I definitely can do it; a sixth response option was that it was not applicable because no one in that particular group (family, teachers, or friends) used tobacco. A sample item is, “How sure are you that you can convince family members not to smoke or use tobacco?” This instrument was scored only for those who did not chose a not applicable response to one or more of the items and was the sum of the responses given, with higher scores indicating greater confidence to convince others not to use tobacco. The range of potential scores was from 3 to 15.
Industry Self-Efficacy: A single item (“How confident are you that you can work effectively against the tobacco industry?”) was used to measure industry self-efficacy, with the five-choice response set ranging from I cannot do it to I definitely can do it, with a higher score indicating greater self-efficacy in this area (Holden et al., 2004). The range of scores was from 1 to 5.
Advocacy: Advocacy for tobacco policy was measured with a two-item instrument that reflected advocacy with “other students, family or friends” and institutions on the topic of concern about tobacco use (Holden et al., 2004). The institutions question was, “In the past year, how many times have you tried to convince school officials, local businesses, community agencies, or government officials to be more concerned about tobacco use?” and the family/friends item was worded similarly. The five response options ranged from neve’ to six or more times. The total advocacy score was the sum of the two items, with higher scores indicating greater advocacy actions; the potential range was from 2 to 10.
Phase I data analysis
Data were summarized descriptively using means and standard deviations or frequency distributions. The percentage of the maximum possible score that the mean represents was calculated as an objective way of quantifying how close the participants were to this value, on average. Comparison of baseline and posttraining scores for the aforementioned subscales was accomplished using mixed modeling for repeated measures. This strategy was chosen to allow the retention of participants in the analysis even if they did not complete the posttraining survey, since mixed modeling allows the retention of all participants who complete at least one survey. In addition, the goal of the longitudinal comparison of summary scores (rather than evaluation of changes in individual items) was to provide a broad overview of the outcomes most likely to be affected by the training, with planned focus on item-specific changes in Phase II. An alpha of .05 was used for the mixed modeling.
Phase I process evaluation
At the conclusion of the project, students answered additional open-ended questions on the posttraining survey to assess things they liked and things that could be improved with regard to the youth advocacy training and their participation in the youth advocacy program throughout the school year. In addition, an informal interview was conducted with the adult mentors to determine their perceptions on the experience, lessons learned involving youth in advocacy, and if they would be interested in participating in a similar program in the future. Qualitative data were analyzed by one member of the research team for common themes within each question.
Phase II: Youth Tobacco Advocacy Training Program
Program Development and Implementation
Based on lessons learned from Phase I, the state health department hosted the YTAT program (AY 2018-2019) with students from a total of three Appalachian Kentucky counties (N = 80). Returning members of the Phase I high school student group and two other high schools in the same county were invited to participate (County P). The two additional schools in County P had not previously worked on tobacco control nor did they have existing student tobacco advocacy groups. Two additional rural, Appalachian Kentucky counties were also included in Phase II (County A and County C). Counties A and C had active youth groups working on tobacco control through the middle and high schools, and the adult mentors agreed to participate to support their existing advocacy efforts. During Phase II, the researchers aimed to build more autonomy with participating adult mentors and youth, to support sustainability efforts.
Program Description
October 2018, two regional 1-day interactive trainings were conducted by members of the research team in collaboration with two near-peer college students, CTFK, and partners from the local and state health departments. The training provided breakout sessions on the following topics: tobacco use and consequences, the impact of tobacco policies, developing effective messaging, e-cigarettes and the link to school and community policies, and policy advocacy skills. Resources from CTFK’s online training modules were used to supplement tailored training materials developed by the research team. As a culminating experience, youth initiated development of an action plan to work on tobacco policy advocacy in their schools or communities during the upcoming school year (AY 2018-2019).
Adult mentors in the three counties agreed to support the youth to work on tobacco prevention and youth advocacy efforts outlined in the action plan throughout the school year. Adult mentors were also asked to carry out additional booster trainings throughout the school year, with resources and regular check-ins provided by the research team. Resources provided information on e-cigarettes, how to plan and implement a school and/or community event, how to maintain youth engagement, communicating with elected officials around tobacco policy, and upcoming statewide advocacy events and training opportunities. A statewide tobacco control newsletter was also developed by the researchers and shared with the adult mentors. All participating youth received promotional items during the training (e.g., pens, buttons, sunglasses). Additional incentives were not provided for participating in the evaluation.
Evaluation
Scaling up on the preliminary work done in Phase I, researchers collected both process and impact evaluation data in Phase II. In addition, since there was a larger sample in Phase II, the state wanted to look more closely at individual responses to the subscale items rather than summary scores for this Phase of the study.
Phase II impact evaluation
Phase II participants were surveyed before (September 2018) and 7 months after both training sessions (April 2019) through paper-based or online surveys (at the preference of the adult mentor). The Phase II baseline survey was distributed prior to the training during a collective student group meeting time with each respective group. The Phase II posttraining survey was distributed in a similar manner. Based on lessons learned in Phase I, researchers modified the baseline and post impact survey utilized in Phase I to more clearly measure specific project outcomes, particularly those linked to youth empowerment and policy advocacy (Holden et al., 2004). Because feedback from the Phase I study included criticism about the length of the survey and the lack of alignment between project goals and survey questions, the survey was condensed and pilot tested with a group of college students who assessed item clarity and readability for the population of interest. Additionally, items were reviewed by experts in the field and aligned with training objectives. Included subscales for Phase II are summarized below.
Tobacco Policy Attitudes: Five items measured the degree an individual supports tobacco policies and two additional items assessed the perceived effectiveness of education versus tobacco policy (Table 1), using a 5-point scale from strongly disagree to strongly agree. The tobacco policy items were adapted for the adolescent population from the Kentucky Health Issues Poll (2018), and based on feedback that the “opposition” and “support” language from Phase I was confusing.
Interpersonal Confidence: Six items assessed individuals’ belief in their ability to influence different groups’ tobacco use behaviors, and the 5-point response options ranged from strongly disagree to strongly agree. A sample item is, “I am confident in my ability to influence [e.g., adults in my community] to be concerned about tobacco-related issues.” These items were drawn from several domains in the Attributes of Psychological Empowerment scale (Holden et al., 2004).
Advocacy Self-Efficacy: Three items assessed confidence in ability to advocate for policies to lower tobacco use, select effective advocacy strategies, and develop an advocacy action plan, with responses on the 5-choice scale ranging from strongly disagree to strongly agree. These items were also drawn from Holden et al.’s (2004) Attributes of Psychological Empowerment scale, specifically from the Interactional domain. These items measured the degree to which participants believed they had the tools and strategies to be effective advocates. Phase I measures did not include specific advocacy skills, so this subscale was added to align with training objectives for Phase II.
Self-Reported Advocacy: Seven items measured the efforts made by the individual to build support for tobacco policies. “In the past 6 months, how many times have you tried to convince [e.g., family, friends, government officials] to be more concerned about tobacco-related issues?” (never, 1-3 times, and 6 or more times), with a separate item for each type of individual or institution targeted by advocacy. These items mirror those from Ribisl et al. (2004) but were expanded from the Phase I measures, given feedback from youth who said there was a difference when participating in advocacy with the various represented groups.
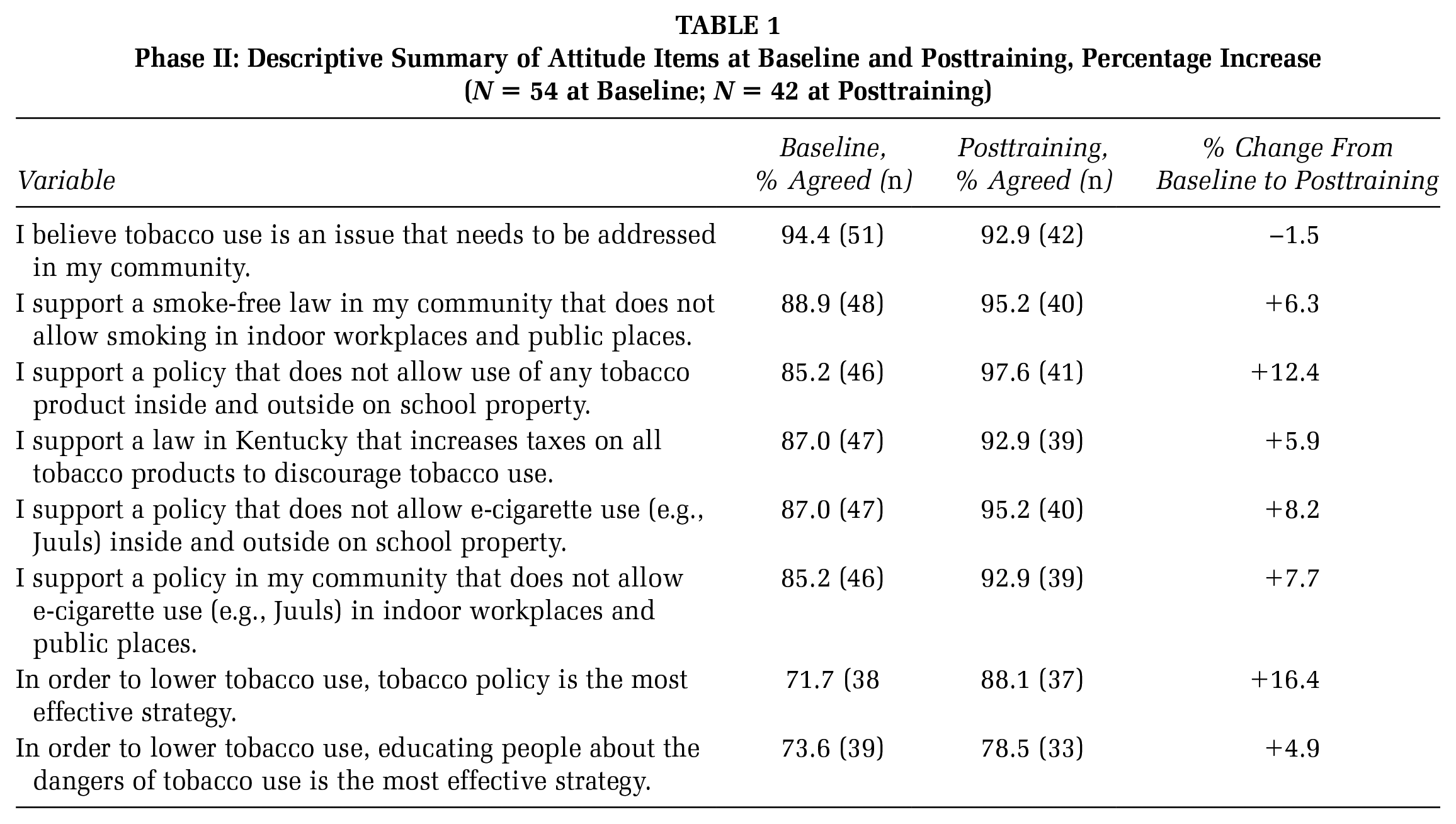
Phase II: Descriptive Summary of Attitude Items at Baseline and Posttraining, Percentage Increase (N = 54 at Baseline; N = 42 at Posttraining)
Phase II data analysis
The data were summarized descriptively using means and standard deviations or frequency distributions. To compare Likert-type subscales, those who chose either strongly agree or agree were included in the “percentage agreed” category as is referenced in Tables 1 through 4. Phase II data analysis focused on item-specific changes over time from baseline to posttraining.
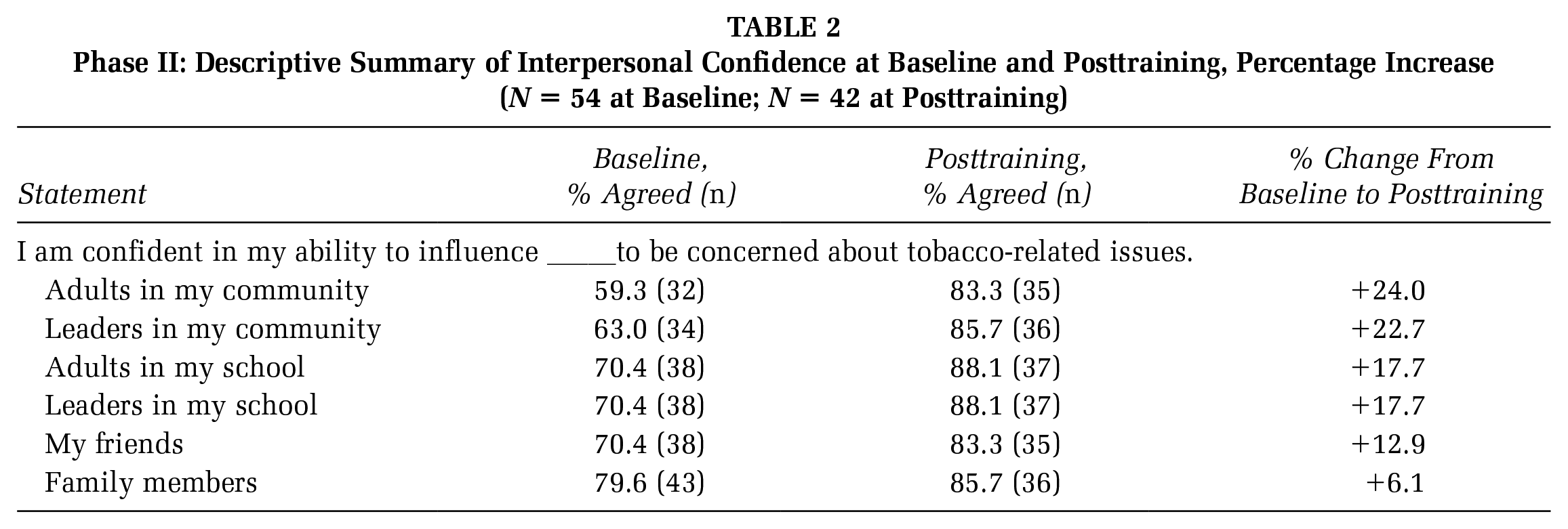
Phase II: Descriptive Summary of Interpersonal Confidence at Baseline and Posttraining, Percentage Increase (N = 54 at Baseline; N = 42 at Posttraining)
Phase II: Descriptive Summary of Advocacy Self-Efficacy and Self-Reported Advocacy at Baseline and Posttraining, Percentage Increase (N = 53 at Baseline; N = 42 at Posttraining)

Phase II: Descriptive Summary of Process Evaluation Items Posttraining (N = 67)

Phase II process evaluation
Participants completed paper-based satisfaction surveys immediately following the September training. At the conclusion of the project, participants answered additional open-ended questions on the post survey. Process and satisfaction survey questions were adapted from surveys described in the Youth Empowerment Solutions Evaluation Guide (Zimmerman, Morrel-Samuels, & University of Michigan School of Public Health, 2017) to align with training goals. Items were developed to assess (1) perception of how well YTAT prepared them to address tobacco-related issues, (2) satisfaction with YTAT implementation, and (3) strengths and weaknesses of YTAT. Quantitative data were analyzed with descriptive statistics. Qualitative data collected at post were analyzed by one member of the research team for common themes within each question.
Results
Phase I: Impact Evaluation
Youth were surveyed at baseline (pretraining) and then again 7 months posttraining. Of the 20 students (70% female, 60% high school freshmen) who completed the baseline survey, 14 completed the posttraining survey (70% retention rate).
For most outcomes, scores tended to increase from baseline to posttraining (Table 5). There was a 39% increase in self-reported advocacy and a 12% increase in group efficacy. Postintervention, 85% of respondents believed they could reduce the amount of tobacco use in the community; all respondents reported they could start discussions with others about tobacco-related issues. All respondents had tried at least once to convince peers, family, and friends to be more concerned about tobacco issues at postintervention compared to baseline (67%). Similarly, more respondents had tried at least once to convince school officials, local businesses, community agencies, or government officials to be more concerned about tobacco use (77%) than at baseline (47%).
Phase I: Descriptive Summary of Scale Scores at Baseline and Posttraining, Average Percentage Increase, and p Value for the Mixed-Model Time Effect (N = 20)

Phase I: Process Evaluation
Posttraining, students exhibited a sense of empowerment, “It made me believe I was working towards an important bigger picture that means something.” Nearly all respondents mentioned that the experience provided skills they need to be an effective advocate. Many of the youth were not comfortable at first talking about tobacco-related issues given the negative response they expected. Similarly, they had never thought about tobacco policy as a way to improve health outcomes in their community. Youth were eager to talk about tobacco and the benefits of evidence-based tobacco policies.
Based on information provided during the informal interview with the adult mentor, students hosted and participated in a variety of school- and community-based activities to make their voices heard. They developed communication materials to share with peers, teachers, and school administrators. They also encouraged others to support being “tobacco-free” through petitions, signing and displaying a banner in the school, and distributing bracelets, branding the movement, and creating a presence in their school. Youth also visited the State Capitol to talk with elected officials and presented at state and regional conferences.
The adult mentor also realized the positive impact on the youth: “We sometimes underestimate the role students play in solving real-world problems. By empowering our students with information and giving them a voice in this issue, we are providing opportunities for leadership in their school and community.”
Youth suggested more group meetings and encouraged getting more youth involved. They also wanted additional opportunities to interact with other youth working on advocacy efforts and wanted additional training on specific policies as well as advocacy skills.
Phase II: Impact Evaluation
The Phase II baseline survey was fully completed by 54 students. Of the participating students, 65% were from County P, 25% from County A, and 11% from County C. The majority were high school students, 70% were female, and 80% White. The post survey was fully completed by 42 students (a 78% retention rate). Half of post survey respondents were from County P, 36% from County C, and 14% from County A. More than half were high school students compared to 38% late elementary and middle school students. Three fourths were female and 88% White.
At baseline, less than half of the participating students had received tobacco- or advocacy-related training in the past year. Participating students were asked to complete the online Taking Down Tobacco training by CTFK prior to the in-person training; only 10% of them had completed the Taking Down Tobacco training at baseline compared to 85% at post.
Nearly all respondents agreed that tobacco use is an issue that needs to be addressed in their community at both time points (94% pre- vs. 93% posttraining). There was an increase in support for tobacco policies over time, particularly with tobacco-free schools (12% increase). At follow-up, a higher proportion of students (88%) agreed that tobacco policy was the most effective strategy compared to tobacco education (79%). Additional policy attitudes are summarized in Table 1.
Most students agreed at baseline that they were confident they could influence others (Table 2). The percentage who agreed that they could influence others increased for each of the specific groups to be influenced from baseline to posttraining, with confidence in their ability to influence adults and leaders in their community increasing the most (percentage change = 24% and 23%, respectively).
Nearly all students agreed that there are things they can do to make their communities a better place at both time points (98% baseline vs. 95% posttraining). Similarly, nearly all students agreed that their participation in group efforts to influence public opinion and policy makes a difference in their communities (90% baseline vs. 93% posttraining).
At baseline, almost three quarters of students demonstrated confidence in their abilities to advocate for tobacco policies in their community versus 91% at posttraining (Table 3). Confidence in specific skills related to advocacy, including selecting effective advocacy strategies and developing an action plan improved the most between baseline and post-training (percentage change: 25% and 21%, respectively).
At baseline, when asked about their advocacy activities, many students indicated they had attempted to influence family, friends, and other students to be concerned about tobacco-related issues; however, few students had attempted to influence school administrators, local businesses, community agencies, or government/elected officials (Table 3). At posttraining, the percentage who “never” tried to convince decreased for all advocacy targets with the exception of friends. For the other six target groups or institutions, the smallest change was for other students (a decrease in never from 26% to 12%) while the greatest was for community agencies (a decrease in never from 85% to 5%).
Phase II: Process Evaluation
Of the 80 youth who participated in the training, 67 students participated in and completed process surveys immediately following the training. Overall, students were satisfied and found the training useful. Students felt the most prepared by the following breakout sessions: Advocacy 101, Juul in Your School, and Say YES to Tobacco Policies. While these three sessions were perceived as the most beneficial, the majority of students reported benefiting from all sessions (Table 4). Nearly all participants reported overall satisfaction with training. Students believed the training was organized and of high quality. Nearly all (90%) students indicated they would recommend the training to a friend.
Students also reported feeling empowered by receiving advocacy skills at the training: “I was empowered to make a change within my community,” and gained skills to use in the future: “I learned how to write a speech and information about Juuls that will help our campaign in the future.” Based on these training, students reported feeling ready to advocate for tobacco policies and felt equipped with the tools to do so. Students reported willingness to talk to not only their friends and families about tobacco issues but also individuals at school and in the community: “If I see someone at school using tobacco, I will ask them nicely to put it away on school grounds.”
Students reported an interest in learning more practical skills to apply their advocacy training and more general information about tobacco policies. Students also reported wanting additional hands-on and interactive activities. Students reported a desire to have more support from their school, more events in which to practice advocacy, and more tools to communicate with lawmakers. Other suggestions included the desire to build more confidence, spend more time on training activities, more guest speakers, reminders on skills they were introduced to, and more student participants. Students overwhelmingly reported a desire to learn more communication tools to assist them with advocacy, and they wanted more examples of successful advocacy.
Discussion
While there is support to engage youth in tobacco policy advocacy efforts (CDC, 2014), there is a lack of research on the impact of advocacy programs to promote tobacco control policies in underserved Appalachian communities. Our study reinforces the numerous benefits reported among participating youth living in rural, Appalachian Kentucky whose communities are disproportionately burdened by tobacco-related morbidity and mortality (Marshall et al., 2017) and where tobacco control lags behind the rest of the nation (ALA, 2018). During both phases, students participating in the youth advocacy training program overwhelmingly agreed tobacco use is an issue that needs to be addressed in their community. Youth also believe there are things they can do to make their communities a better place. Empowering youth as advocates in high-risk regions like Appalachia is a promising strategy to promote health equity by investing in an infrastructure to strengthen existing evidence-based tobacco policies (CDC, 2014).
During Phase II, more youth agreed that tobacco policy is the most effective strategy to decrease tobacco use in their communities. Regardless of the type of advocacy training, youth must believe that policy is an effective approach to tobacco prevention (Ribisl et al., 2004). Interestingly, during Phase I, support for evidence-based tobacco policies decreased slightly among participating youth, whereas there was an increase in support for all tobacco policies over time during Phase II. Policy support is strongly associated with the likelihood of participating in advocacy-related actions among high school students (Unger, Howard, Boley, Johnson, & Chen, 1999), so this should be an important component of advocacy trainings. During Phase II, the training further reinforced the importance of various evidence-based toacco policies, giving specific examples within each community, and relating back to the lack of statewide policies in Kentucky (ALA, 2018). Youth participating in these trainings seemed particularly interested in ensuring existing tobacco-free school policies are enforced and that policies include staff, administrators, and visitors. During Phase II, statewide legislation for tobacco-free schools was introduced during the legislative session, so this was certainly a topic of interest in the participating communities. Media releases and social media links were shared with the adult mentors to share with their youth groups, which could have specifically influenced greater support for tobacco-free schools. Future research may want to focus on particular policy advocacy targets so training can be tailored and aligned with the policy the community is most ready to implement.
Interpersonal confidence increased during both Phase I and Phase II. While most students agreed at baseline that they were confident they could influence others, during Phase II, confidence in the youths’ ability to influence adults and leaders in their community increased the most (24% and 23%, respectively). Given the deeply entrenched tobacco culture in many Appalachian communities (Hart et al., 2018), talking with others in the community about this topic may be challenging, so improvement on these outcomes is promising. Training content primarily focused on youth talking with elected officials and adults in their communities. Different strategies may be needed to specifically encourage youth to influence their peers and family members. There is a need to explore effective strategies to engage youth with these targeted groups since both family and peers are extremely influential.
Students also demonstrated confidence in their abilities to advocate for tobacco policies in their community. Phase II measures included individual advocacy self-efficacy, realizing that perceptions of group efficacy may be different than their own individual skill set. Confidence in advocacy-related skills, including selecting effective advocacy strategies and developing an action plan improved by over 20% between baseline and posttraining during Phase II. At post all students agreed they were able to select effective advocacy strategies, which is a unique and specific skill that is necessary for policy advocates to be successful (Ribisl et al., 2004). It is clear that the training helped youth gain confidence in these skills, similar to other research among Kentucky youth (King et al., 2015). However, it is important to note that continued training is necessary. In fact, youth elicited a desire for more training to help put the skills into action. Long-term booster trainings and follow-up are warranted, particularly given the complexity of policy change. This reinforces the need for adequate resources and infrastructure to sustain youth advocacy efforts.
Self-reported advocacy increased during Phase I and Phase II evaluation. During Phase I, all respondents had tried at least once to convince peers, family, and/or friends to be more concerned about tobacco issues at postintervention compared to 67% at baseline. While there was an improvement in advocacy during Phase I, during Phase II, it was important to distinguish individual advocacy activities among various groups (e.g., family, friends, school administrators, local businesses, community agencies, or government/elected officials) in order to further improve training content and follow-up with adult mentors. During Phase II, the percentage who never participated in advocacy efforts decreased for all advocacy targets with the exception of friends. The greatest change was for community agencies (a decrease in never from 85% to 5%). The training focused on talking with adults, elected officials, and community stakeholders. However, there is a need to integrate additional training content to ensure youth are well equipped with strategies and talking points for various policies and target groups. Previous studies highlight the frustrations that can occur among youth when talking with community stakeholders (Ribisl et al., 2004). Youth in our study also mentioned potentially being discouraged by a lack of results. Not only does follow-up trainings need to help prepare youth to face the opposition, but also it is imperative to reinforce that youth have been instrumental in policy changes in similar communities, and set them up for success by setting short-term subgoals and milestones.
Strengths and Limitations
Strengths of this study include the inclusion of students from several rural, Appalachian communities. We were also able to build lessons learned from Phase I into Phase II to help improve measured outcomes, design of the training, and communication with adult mentors. The sample size is a limitation, but participation in both baseline and post surveys was relatively high for those attending the training. Students who were already interested in these efforts may have been more engaged than the general population of students in the state, so results may not be generalizable to all youth. This reinforces the need to conduct a randomized controlled trial to determine if this intervention truly leads to change in advocacy impact over time. Evaluation with youth across different Appalachian communities spread out across the state was challenging given the varied meeting times of each group and the varied involvement of the adult mentors. However, the adult mentors who were engaged were able to assist with continued youth participation throughout the school year. Further quantifying participation in duration and dosage of interaction with adult mentors during Phase II would be beneficial. In addition, quantifying advocacy efforts would be useful to determine an additional impact of the training and correlate with policy outcomes over time.
Implications for Practice and/or Policy and Research
Tobacco policies provide an opportunity to reach groups disproportionately affected by tobacco-related disparities (Beatty et al., 2019), including those living in rural and Appalachian communities. Youth in Appalachia demonstrated a desire to influence tobacco use and policy in their communities. Improvements were observed in attitudes, interpersonal confidence, advocacy self-efficacy, and self-reported advocacy over time with youth who participated in the tobacco advocacy policy training. Lessons shared regarding practical application and implementation of a youth advocacy program may benefit health promotion and community health professionals, particularly given the benefits of engaging youth in advocacy (CDC, 2014). Youth enjoyed participation in the tobacco advocacy training and wanted to make a difference in their community. While working towards tobacco policies can be challenging in a community with high tobacco use rates and a tobacco-growing heritage (CTFK, 2018), engaging youth in tobacco advocacy can help build a foundation for future tobacco control efforts. Because policy change takes time, it may be helpful to continue to track the progress of these youth during the next few years, and also monitor community-engaged work and ultimately tobacco policy change.
Building a relationship with community advocates, school officials, and adult mentors is instrumental in successfully engaging youth to work on advocacy; it also helps with sustainability. While it was not the focus of this study, additional research is needed to evaluate the role of the adult mentor in relation to youth outcomes. In addition, resources are necessary to build capacity and infrastructure to support tobacco policy advocacy, particularly in states with a lack of evidence-based tobacco control policies. Our findings reinforce the need for continued collaborative health promotion interventions to promote tobacco policy advocacy and support for youth living in high-risk communities.
Footnotes
Authors’ Note:
The authors would like to thank the community and school stakeholders who made this program possible. In addition, we are most appreciative of the youth who participated in the program. This work was supported by the Kentucky Department for Public Health, Tobacco Prevention and Cessation Program, and the CVS Health Foundation.
Supplement Note:
This article is part of the Health Promotion Practice supplement, “Tobacco and Health Equity: Interventions, Research, and Strategies to Address Tobacco Use Among Diverse Populations,” developed under the guidance of the Society for Public Health Education (SOPHE). SOPHE received funding from the Food and Drug Administration’s Office of Minority Health and Health Equity (Grant number HHSF223201820377A) to support printing and open access dissemination. The views and findings expressed in these manuscripts are those of the authors and do not imply endorsement or reflect the views and policies of the U.S. Government. The entire supplement issue is available open access at ![]() .
.