
Abstract
The community readiness model (CRM) was used to assess changes in community readiness across four counties in Georgia that were targeted as part of a 3-year Childhood Obesity Prevention Program. Key respondent interviews were conducted with community stakeholders in 2012 (n = 20) and 2017 (n = 18) using a semistructured questionnaire assessing six dimensions of community readiness (i.e., community efforts, community knowledge of efforts, leadership, community climate, community knowledge about the issue, and resources available to support efforts). Interviews were analyzed using the CRM scoring protocol and qualitative methods. Paired t tests were used to compare mean score differences between baseline and follow-up assessments. At baseline, overall mean readiness scores for the four counties ranged from 4.52 to 5.05 on the CRM 9-point scale. At follow-up, overall readiness scores ranged from 6.01 to 6.97 out of 9.00. Data revealed a statistically significant improvement in scores across all communities (+1.70, p = .007; 95% confidence interval [0.87, 2.51]). Data also revealed statistically significant improvements in every dimension of readiness, except community knowledge of the issue. Information gleaned from interviews suggested that investing in staff to support efforts, building awareness to shift the community climate, and cross sector collaboration contributed to improved community readiness among the study communities. The provision of technical assistance, peer learning opportunities, and financial support as part of a cooperative grant initiative holds promise for increasing the capacity of community coalitions to advance childhood obesity prevention efforts in their local communities.
Despite recent declines among children nationally, childhood obesity remains a major threat to public health in the United States (Ogden et al., 2016; World Health Organization, 2014). Childhood obesity is the result of myriad factors, though poor nutrition, physical inactivity, and obesogenic environments have been identified as primary drivers (Ogden et al., 2016). Community-based approaches utilizing policy, systems, and environmental (PSE) strategies to address multiple factors driving childhood obesity have become increasingly prevalent (Bunnell et al., 2012; Keener et al., 2009; Mantziki et al., 2018). Community-based interventions can support programs and PSE changes that address both individual health behaviors and the social and physical environments that affect health. Assessing a community’s readiness prior to the implementation of a community-based intervention allows for tailoring of the approach to the community context (Bhuiya et al., 2017; Oetting et al., 1995; Sliwa et al., 2011).
The community readiness model (CRM) is a method for assessing community readiness developed by the Tri-Ethnic Center for Prevention Research at Colorado State University (Plested et al., 2006). The CRM defines community readiness as the capacity or ability of a community to take action to address an issue of interest. Six dimensions of readiness are assessed, including existing community efforts, community knowledge of efforts, leadership, community climate, community knowledge about the issue, and resources available to support efforts (Plested et al., 2006). Based on the transtheoretical model of behavior change (Prochaska & DiClemente, 2005), the model scores each of the six dimensions along nine stages of readiness, ranging from a score of 1.00 (no awareness of the issue) to 9.00 (a high level of community ownership; Edwards et al., 2000; Plested et al., 2006). Refer to Table 1 for an overview of the nine stages of community readiness.
Nine Stages of Community Readiness
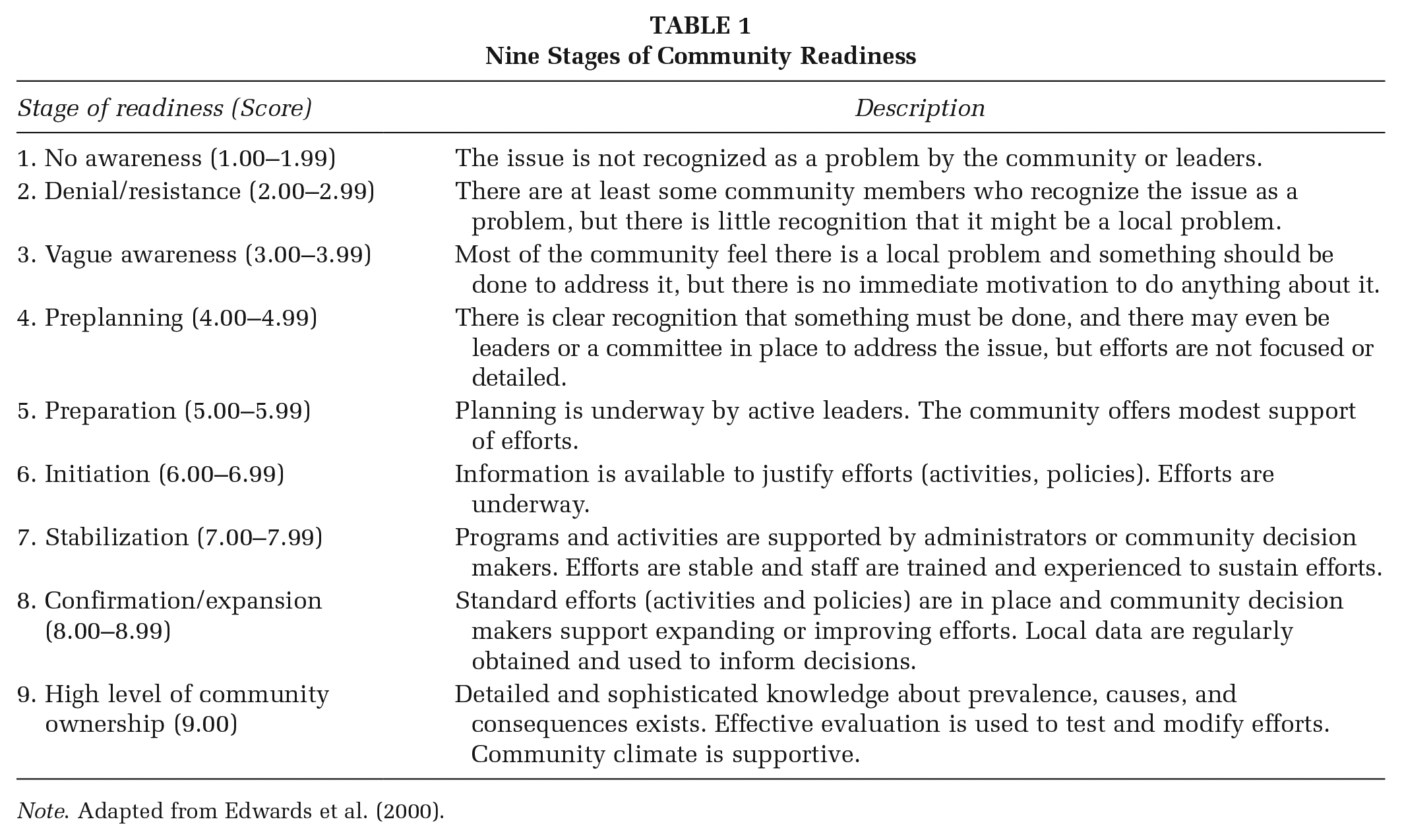
Note. Adapted from Edwards et al. (2000).
The CRM results can be used to help communities select prevention strategies that are appropriate to their local context. For each stage of readiness, the CRM guides the development of goals and strategies that increase readiness for action. For example, communities scoring in the lower stages of readiness in leadership on childhood obesity may have local leaders who do not recognize obesity as problem or indicate any motivation to take action. In such a case, the CRM would guide the community’s focus toward educational efforts on childhood obesity among its leaders (Edwards et al., 2000; Sheldon et al., 2016; Sliwa et al., 2011), which would support increased readiness to consider and implement evidence-based prevention strategies for childhood obesity.
Childhood Obesity Prevention Program
In 2012, Georgia State University School of Public Health (GSU-SPH) conducted a statewide assessment to identify community coalitions in Georgia with existing capacity and interest in expanding childhood obesity prevention efforts. Fifteen active coalitions were identified and community readiness assessments were conducted in their respective counties. Sheldon et al. (2016) describe findings from that study.
Subsequently, the Healthcare Georgia Foundation invited 14 coalitions from this study to apply to a 3-year grant initiative—the Childhood Obesity Prevention Program (COPP)—with the aim of advancing childhood obesity prevention efforts (Healthcare Georgia Foundation, 2017). Based on a competitive funding announcement, four coalitions received financial support and technical assistance (TA) from 2013 to 2016. GSU-SPH collaborated with the GSU Georgia Health Policy Center and Georgia Family Connection Partnership to provide planning, implementation, and PSE change TA. TA included assignment of a TA provider, regular check-ins, site visits, action planning support, meeting facilitation, staff capacity building, consortium and partner development, sustainability planning, and resource sharing. FHI360 provided communications support and ICF Inc. provided evaluation TA (Healthcare Georgia Foundation, 2017). The TA providers worked collaboratively to coordinate peer learning opportunities, webinars, and workshops. During the 3-year initiative, the coalitions accomplished a number of organizational, programmatic, and policy achievements summarized in Table 2.
Coalition Accomplishments During the Childhood Obesity Prevention Program Grant
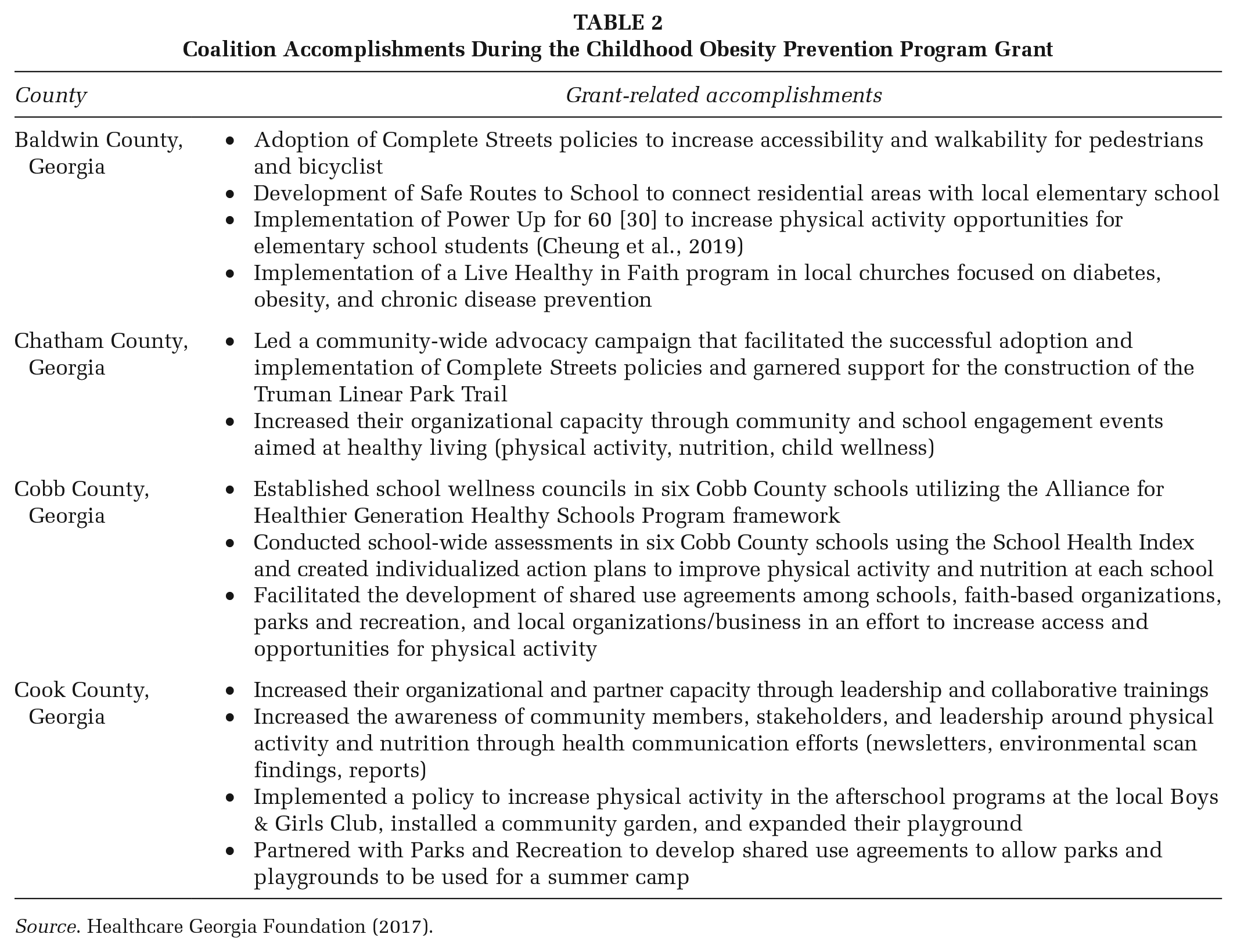
Source. Healthcare Georgia Foundation (2017).
This study focused on community readiness at the county level, where the coalitions that were part of the COPP initiative were operating. The purpose of this study was to assess changes in community readiness between 2012 and 2017 in the four Georgia counties. In addition, this study sought to understand the factors that may have contributed to changes in the readiness dimension scores.
Method
Sample and Design
The identification process for the selection of counties and the baseline community readiness assessments are detailed by Sheldon et al. (2016). In the initial study, an environmental scan identified active coalitions in Georgia (n = 15) that were addressing childhood obesity. Key respondent interviews were conducted with community stakeholders in each county (n = 79), and community readiness was calculated. The four counties with coalitions that were part of the COPP initiative were included in a follow-up assessment of community readiness. Sociodemographic characteristics for the study counties are presented in Table 3.
Sociodemographic Characteristics of the Study Counties
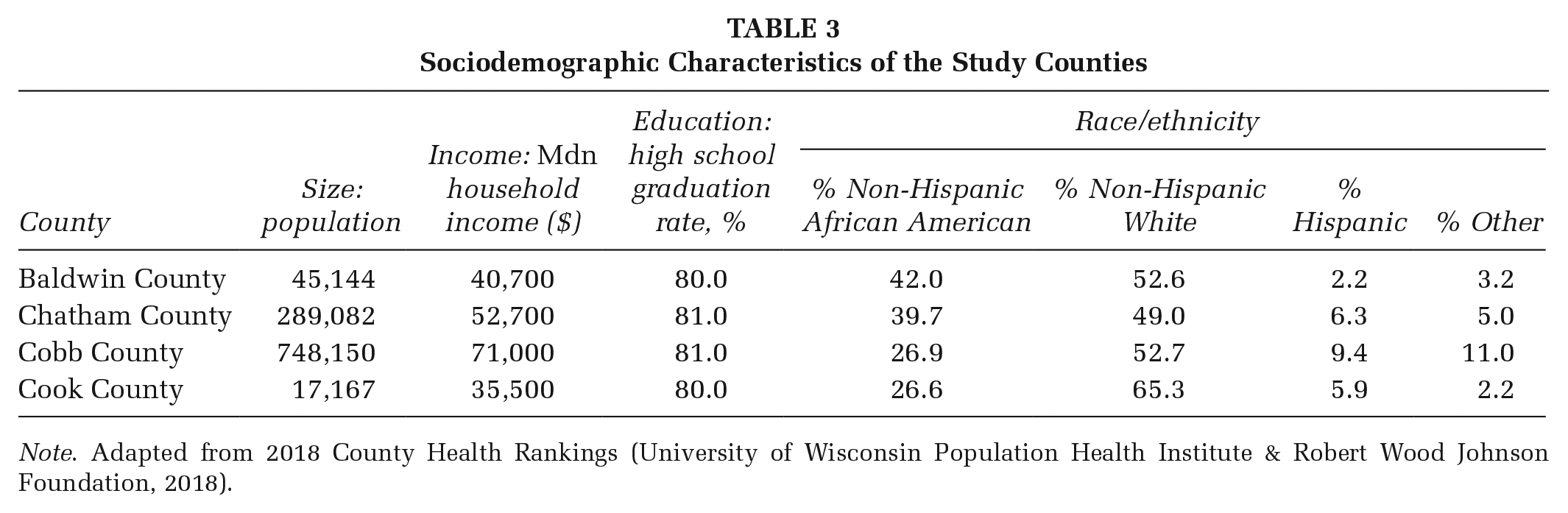
Note. Adapted from 2018 County Health Rankings (University of Wisconsin Population Health Institute & Robert Wood Johnson Foundation, 2018).
Key respondents were identified in each county and invited to participate in a phone interview using the CRM interview guide. The CRM defines key respondents as individuals in the community who can provide insight as to what is going on locally around an issue and should represent different sectors within the community to allow for the collection of information from several perspectives (Plested et al., 2006). Key respondents included individuals in the community who had knowledge about the people, processes, or happenings in childhood obesity prevention efforts. Respondents from the 2012 study were initially contacted to participate in the follow-up assessment. Individuals who were no longer able to provide insight about childhood obesity prevention efforts in the study counties were not included, and a comparable replacement was identified and invited to participate using convenience sampling methods.
Twenty baseline key respondent interviews (Baldwin County: n = 4; Chatham County: n = 6; Cobb County: n = 5; Cook County: n = 5) and 18 follow-up interviews (Baldwin County: n = 4; Chatham County: n = 6; Cobb County: n = 4; Cook County: n = 4) were conducted. Six respondents participated in both baseline and follow-up assessments. Respondents represented different community sectors, including city and county governments, schools, academia, local businesses, local nonprofits or community organizations, and public health.
Procedures
The CRM interview guide included 36 open-ended questions related to six dimensions of readiness (Plested et al., 2006). Interviews were conducted over the telephone by a trained researcher, audio recorded, and lasted approximately 60 minutes. Informed consent was obtained from respondents prior to their interview using an approved protocol from the institutional review board at GSU.
Analysis
Interviews were transcribed and analyzed using NVivo11 (QSR International, 2011). Two trained researchers independently scored and coded all interviews. The CRM provides an anchored 9.0 rating scale with specific statements corresponding to the stages of readiness for each of the six dimensions. Every interview was scored based on the lowest rating statement for each dimension; if the interview supported the statement, the scorer would move to the next statement. This process was repeated until a rating statement was no longer supported. Researchers discussed scoring differences and referred to the scoring guide to achieve consensus on all readiness scores. The interrater reliability between scorers was 92%. An overall mean community readiness score was calculated as the average across all dimensions for each county. Per CRM scoring protocol, the overall readiness scores were rounded down to a whole number corresponding with a specific stage of readiness (Plested et al., 2006). Readiness scores were analyzed in SPSS (IBM SPSS Statistics Version 25, 2018) using paired t tests to compare mean differences between the baseline scores and the follow-up scores for the four counties. The significance level was set at .05.
In addition, thematic analysis techniques were used to understand changes in the readiness scores. The researchers read each interview and identified emergent characteristics in the responses that could speak to changes in readiness scores including facilitators, barriers, and lessons learned. The characteristics were coded and similar codes were refined and condensed into themes (Braun & Clarke, 2006). Any coding discrepancies were discussed among the researchers until consensus was reached.
Results
Pre-COPP Readiness Scores (2012 Findings)
At baseline, readiness scores for the four counties ranged from 4.52 to 5.05 on the CRM 9-point scale. Three counties (Baldwin County: M = 4.98, SD = 0.30; Chatham County: M = 4.52, SD = 0.21; Cobb County: M = 4.54, SD = 0.30) scored in the preplanning stage and one county (Cook County: M = 5.05, SD = 0.99) scored in the preparation stage of readiness. The overall mean readiness score in 2012 was 4.77 (SD = 0.28), corresponding with the preparation stage of readiness. The dimension exhibiting the highest mean score was existing community efforts (M = 6.40, SD = 0.19; initiation stage). The lowest scoring dimension was community climate (M = 3.63, SD = 0.45; vague awareness stage).
Post-COPP Readiness Scores (2017 Findings)
At follow-up, overall readiness scores ranged from 6.01 to 6.97 out of 9.00; every county scored in the initiation stage (Baldwin County: M = 6.56, SD = 0.26; Chatham County: M = 6.97, SD = 0.46; Cobb County: M = 6.01, SD = 0.60; Cook County: M = 6.33, SD = 0.42). The overall mean score in 2017 was 6.47 (SD = 0.40). The dimension exhibiting the highest mean score was community efforts (M = 7.66; SD = 0.27; stabilization stage). The lowest scoring dimension was community knowledge of the issue (M = 5.04, SD = 0.54; preparation stage).
Changes in Readiness Scores Over Time Across Counties
Data were analyzed using paired t tests to compare mean differences between the overall 2012 scores and the 2017 scores for the study counties. Analysis revealed a significant improvement in scores across all counties (p = .007). Data also revealed statistically significant improvements in every dimension of readiness, with the exception of community knowledge of the issue. Table 4 includes an overview of the average scores in 2012 and 2017.
Overall Mean Readiness Score Differences Between 2012 and 2017 by Dimension
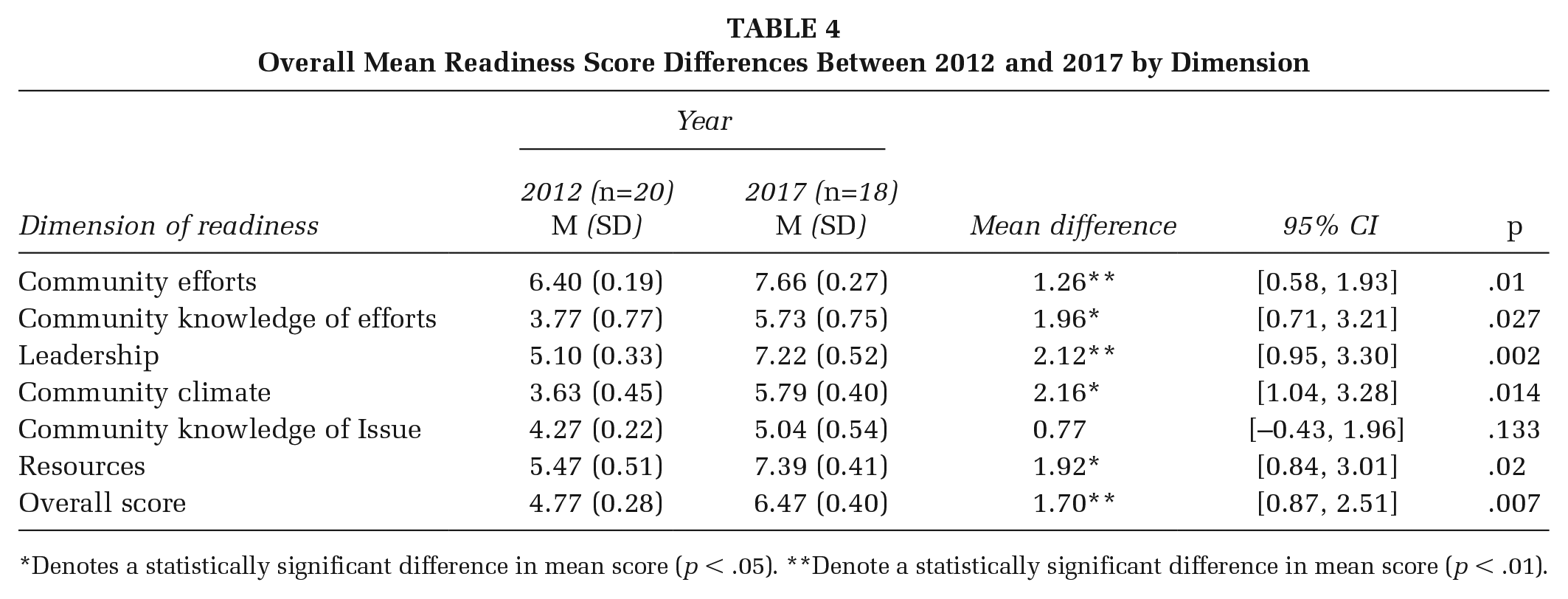
Denotes a statistically significant difference in mean score (p < .05). **Denote a statistically significant difference in mean score (p < .01).
Mean Readiness Scores by County
Paired t tests were conducted to compare the overall mean community readiness scores in 2012 and 2017 by county. There were significant increases in the overall mean readiness scores from 2012 to 2017 for all counties: Baldwin County (+1.58, SD = 0.64, 95% confidence interval [CI: 0.40, 1.56], p = .002), Chatham County (+2.45, SD = 0.64, 95% CI [0.40, 1.58], p = .002), Cobb County (+1.47, SD = 1.07, 95% CI [0.67, 2.63], p = .020), and Cook County (+1.29, SD = 0.22, 95% CI [0.14, 0.55], p < .001).
Qualitative Findings
The key respondent interviews highlighted several important findings: (1) People [staff] were considered one of the most valuable investments for advancing local efforts; (2) building awareness among community members and leaders was important in creating a more supportive environment for childhood obesity prevention efforts; and (3) cross sector collaboration enabled diverse groups within the community to coalesce behind a common agenda. Each finding is described in more detail below.
Investments in People
According to respondents, many local efforts targeting physical activity and nutrition were occurring in the counties between baseline and follow-up assessments. As told by the respondents, one critical piece that made the difference between 2012 and 2017 was that the county coalitions and their partners received funding to support staff to help connect prevention efforts to the local community. Some COPP grant funding was used to support full-time and part-time staff to help coordinate activities, convene meetings, and host trainings and other events. For example, one respondent shared,
Well, I would say that our heyday was when we were in the first couple of years of funding and we had enough funds to support staff members. Our best progress was made when we had a full-time director of community programs. When you’ve got somebody that’s 100 percent devoted to connecting things in the community . . . that makes a big difference.
Funding from the COPP allowed county coalitions to adequately staff their efforts to ensure day-to-day activities were carried out. One respondent indicated, “Our people are our best assets. They provide that face time. They get out there and champion our efforts, connect with families and the kids. . . . They get people interested in what we’re doing and involved.” Another respondent stated, “Through some of our after school programs, they actually hired people whose sole focus is around how to increase physical activity in their programs,” they continued, “The people make all the difference, and I would always put money into people as opposed to programs and things like that . . .”
Other respondents suggested that investing in project staff helped to educate community members and leaders by promoting different health efforts that were going on locally. One respondent shared, “Our staff are our community champions and we rely on them for getting the word out on what we are doing and they know who to talk to in the community, to get a dialogue started . . .”
Building Awareness to Shift the Community Climate
As interviewees shared insight about their communities, many highlighted the importance of community efforts focused on education and building awareness. According to one respondent, “I think people, in my experience, especially from teaching the nutrition classes, really want to learn and they’re so appreciative of all the information that you give them . . .” She added, “It’s really just basic stuff, like reading a food label. They just are so happy that I came and taught them these things and they want to learn more.” Another respondent shared, “I think we’re definitely moving in a good direction. People are interested in what we’re doing. . . . It’s going to take a while to see the complete shift but at least it’s starting.”
All COPP coalitions reported COPP activities that engaged community members in their efforts and shared data and evaluation results with the local community. Many respondents suggested that sharing data helped make a case for their efforts. One respondent indicated, “We’ve been sharing obesity statistics for a long time. One in three in the county is overweight or obese. When you say that, people can actually see that. So they’re aware our work’s important.”
Another respondent shared that building the awareness about childhood obesity took some time but now community leaders and residents can actually see the problem locally. The interviewee said,
Back in the early 2000s, it probably wasn’t on anybody’s radar screen, but then people started to talk about it and you could see the health risks, in terms of kids becoming type 2 diabetics and people started to get the message. It was a pretty easy sell when I went around to partner organizations to try to pitch being part of the initiative [COPP], people seemed to be aware of the importance at that time. So I think we’ve definitely made some headway there.
Although many respondents believed progress has been made in terms of education, there is still a challenge with social culture. One respondent, who worked in a school system, indicated, “What we’re up against is a complete societal shift about what we eat, when we eat, when we exercise or not, all of these things are just sort of generationally engrained into what we do.” She suggested that more recent education efforts are starting to change the way children think about nutrition and physical activity and they are becoming much “more receptive” to healthy behaviors.
Other respondents believe that childhood obesity is an issue that many community members and leaders can now get behind; one respondent stated, “Childhood obesity prevention is really one of my easier sells now when it comes to trying to find funding.”
Cross Sector Collaboration
Another emergent theme was the collaboration between prominent coalitions and workgroups that existed to address childhood obesity. As respondents described these groups, most stated the community coalitions contained members from different sectors in their communities. One respondent shared, “We have implementation workgroups with different people across the community to participate in. This is something we really focused on creating.” They added, “We also have done focus groups where people will come and give us their feedback or we’ve done online surveys.” Respondents indicate that this approach allows the coalition to engage community members in their childhood obesity efforts.
When asked about how community coalitions will sustain efforts, many respondents spoke to the diversity of their coalitions and community workgroups. One interviewee said, “We have different agencies or businesses outside of leadership in the community that step up and kick in some money and support for things the community needs.” Another respondent suggested that while they are still seeking grant money, partners are beginning to “put their own skin in the game.” For example,
A lot of the initial funding came from grants. Whether or not we’ll receive the funding, that’s sometimes yes and sometimes no, but the hospital and school system are now a part of this. . . . It’s part of their own budget. That’s going to be a long-term kind of thing. And, then having this sort of community partner initiative is—that’s a long-term kind of thing, too. Now that we’re actually working together and putting it together, it’s creating more sustainability for the future.
Specifically, one respondent acknowledged the role that TA played in implementing efforts; they shared, “The TA we received over the past 6 years or so, first with RWJF [Robert Wood Johnson Foundation] and then with Healthcare Georgia, has really helped organize and mobilize our coalition to do this work and build on it.” They also stated that during the COPP grant,
We had a lot of efforts focused on infrastructure so we worked with transportation, the city, agencies, and residents on connecting trails around the county to connect with all these other programs our partners were doing. They’re still all involved.
Discussion
At present, childhood obesity is considered an epidemic in the United States. Community coalitions have been identified as central stakeholders in childhood obesity prevention (Glickman et al., 2012). Developing an understanding of community readiness to adopt childhood obesity strategies is an important step forward. A pre–post assessment of community readiness in four Georgia counties enabled local community coalitions to engage stakeholders and tailor interventions or strategies according to what the community was ready and willing to support and invest in.
Findings from our study suggest that a cooperative grant strategy that included fiscal support and the provision of TA shows promise for increasing the readiness of communities in the preplanning and preparation stages of readiness. The COPP grant strategy utilized a capacity-building TA model, which provided support to local coalitions around leadership capacity and education, awareness building, communication efforts, partnership/consortium development, and policy and program implementation. The COPP initiative used TA to support the development of evidence-based interventions and build organizational, workforce, and leadership capacity to implement and evaluate these strategies successfully. Brownson et al. (2014) conducted a study highlighting the need to support administrative evidence-based practices (A-EBP) that increase knowledge skills and capacity to implement evidence-based public health strategies. A-EBP approaches include TA, workforce development, leadership capacity building, and partnership and relationship development (Brownson et al., 2014). Researchers found that in order to implement evidence-based public health strategies effectively, organizations need to improve practices that increase organizational and leadership capacity (Brownson et al., 2014; Eyler et al., 2018). These approaches are consistent with the supports provided to the community coalitions during the COPP initiative.
At baseline, findings revealed that the communities recognized that childhood obesity was a problem locally and some activities were being developed and implemented to address it, but interviews highlighted the need for education and awareness, leadership and staff capacity building, and collaboration across multiple stakeholders. According to the CRM (Edwards et al., 2000), communities in the preplanning stage of readiness should focus their efforts on increasing awareness about the issue and increasing awareness about the different strategies the community can implement to address the issue, which is consistent with the scores and needs identified in our baseline assessment.
Data at follow-up revealed significant improvement across every readiness dimension for each county. While observed improvements cannot be directly attributed to the COPP grant, it is reasonable to view COPP as a likely (potentially significant) contributor. The mission and objectives of the COPP grant initiative aligned well with the improvements experienced in each county (i.e., knowledge, leadership, community climate). As part of the COPP, the coalitions worked with their TA providers to develop specific community action plans, which expanded beyond awareness building and focused on the implementation and evaluation of evidence-based policy and environmental strategies (e.g., Complete Streets, Safe Routes to School, trail/built environment construction, community gardens, and physical activity programs). The TA providers guided coalitions toward evidence-based prevention practices that were appropriate and relevant for each community.
Some study limitations exist. We were not able to assess all 15 counties from the initial study to determine differences between those communities that participated in the COPP and those that did not. Future research could examine all counties to gain a better understanding of changes in community readiness across the state and the activities that have occurred since the last assessment. Examining community readiness prior to implementation of new prevention initiatives can be helpful in tailoring TA and implementation strategies to the local context. This study suggests that such an approach may help communities increase their readiness and implement recommended intervention strategies. The implications for practice are summarized in Table 5.
Implications for Practice
Conclusion
Improvements were reported across all counties for every dimension of readiness examined. In this study, investment in people as well as in cross sector collaboration contributed to improved community readiness, through increased leadership, knowledge, and skills and awareness of childhood obesity, which helped promote local efforts. The provision of TA, in addition to financial support, as part of a cooperative grant strategy holds promise for increasing the capacity of coalitions to address childhood obesity in their local communities.