
Abstract
Background. Uncontrolled hypertension is the primary risk factor for the development of cardiovascular complications and particularly burdens racial/ethnic minority populations. Aim. To determine the effectiveness of a community hypertension screening, education, and empowerment intervention on blood pressure (BP) improvement. Method. We screened 152 participants across four churches in predominantly racial/ethnic minority neighborhoods for elevated BP. During this visit, those with BP ≥ 140/90 mmHg were enrolled in the study and completed interventions. Individuals with moderately elevated BP (≥140/90 and <160/100 mmHg; Group 1) viewed a 3-minute hypertension education video. Individuals with severely elevated BP (≥160/100 mmHg; Group 2) additionally viewed echocardiograms images with subclinical changes from uncontrolled hypertension and had a brief on-site medication review with a pharmacist. Both groups received automated BP monitors and information on neighborhood federally qualified health centers for primary care. Participants returned to each church for follow-up 3 months later. We analyzed BP difference at 3 months and percentage with controlled BP for each group. Results. For Group 1, mean baseline and follow-up BPs were 143.5/88.0 mmHg and 138.5/85.8 mmHg, respectively. For Group 2, BPs significantly decreased from 165.4/98.3 mmHg to 150.4/90.8 mmHg. After the intervention, participants with controlled BP for Groups 1 and 2 were 35.5% and 55.2%, respectively. Discussion. Participants in both groups had BP improvements. Greater improvements were in individuals at higher cardiovascular risk due to severely elevated BPs (≥160/100 mmHg). Conclusion. This pilot highlights the impact that streamlined empowerment interventions with dedicated health personnel can have in high-risk communities with elevated BPs.
Keywords
Background
About 32% of U.S. adults have hypertension (Benjamin et al., 2019), of whom 16% are unaware of their condition (Paulose-Ram et al., 2017). Every 10-mmHg reduction in blood pressure (BP) reduces risk of major cardiovascular events, coronary heart disease, stroke, and heart failure, leading to a 13% reduction in all-cause mortality (Ettehad et al., 2016). Patients with severely elevated BP (≥160/100 mmHg) are at the highest risk for developing secondary cardiovascular complications as a result of their uncontrolled hypertension (Gu et al., 2008). The continued high prevalence and inadequate control of hypertension are troubling given the consensus among researchers and the clinical community regarding the importance of evaluation, pharmacologic treatment, and overall management of these patients in prevention of secondary cardiovascular complications.
In the United States, racial/ethnic minority populations are particularly burdened, and significant disparities exist in hypertension treatment and outcomes (Carnethon et al., 2017). In Chicago, the highest rates of uncontrolled hypertension are seen in predominantly racial/ethnic minority communities, with rates as high as 54% in some communities in the South and West Side (Cohen et al., 2016). Higher rates of morbidity and mortality due to kidney failure, heart disease, and other secondary complications from uncontrolled hypertension are also more prevalent in these communities (Cohen et al., 2016).
Faith-based organizations remain a unifying force in racial/ethnic minority communities encouraging participation in interventions, and networks of support and accountability among intervention participants (Goldstein et al., 2008). Public health professionals and faith-based organizations often have a shared goal of improving community health, so partnerships can have great potential (Brewer & Williams, 2019). Previous studies have demonstrated that interventions introduced in the community are effective in reducing the risk of cardiovascular disease among individuals who might otherwise face barriers to care (Ferdinand et al., 2012; Morisky et al., 2002; Oexmann et al., 2001; Schoenthaler et al., 2018).
Aim
To address the disproportionate rates of uncontrolled hypertension and associated morbidity and mortality among racial/ethnic minority communities in Chicago, we designed the Community Targeting of Uncontrolled Hypertension (CTOUCH) pilot study. The pilot was designed to determine participant acceptability and overall impact of a community-based Screening, Brief Intervention, and Referral for Treatment program for hypertension (SBIRT-HTN) on BP improvement /control through patient empowerment and access to primary care follow-up. A previous study by the authors, called A Hypertension Emergency Department Intervention Aimed at Decreasing Disparities, has shown that eliminating traditional barriers to follow-up care through an SBIRT-HTN intervention will improve treatment adherence among an urban population with elevated BP in the emergency department (Prendergast et al., 2018). CTOUCH was implemented to determine if the intervention could prove successful in a community-based setting. Previous studies have focused on interventions in African American churches, whereas our study also includes Hispanic churches (Brewer et al., 2017; Schoenthaler et al., 2018).
Method
Study Sample
Four churches in predominantly racial/ethnic minority communities in Chicago, Illinois (Austin, Pilsen, Bronzeville, and Humboldt Park), were selected for participation in this pilot in 2017. Two BP screening events were organized at each congregation to accommodate the different worship services. Information about the screening events was communicated to members of each congregation through bulletin announcements, local flyers, and reminders provided by church leaders at the conclusion of services.
Prior to participating in BP measurement on the day of the screening, all participants were shown a 5-minute standardized consent video explaining all study procedures and provided with an opportunity to ask questions before signing a consent form. Inclusion criteria was adults (≥18 years) and verbal fluency in English or Spanish. People were excluded if they were unable to verbalize comprehension of the study or exhibited impaired decision making (e.g., dementia), lived outside of Chicago communities, or planned to move from Chicago area within the next 3 months (due to the study’s 3-month follow-up). This study was approved by the Institutional Review Board of the University of Illinois at Chicago (Protocol No. 2016-119).
The CTOUCH study team, composed of emergency department physicians, pharmacists, researchers, and students, screened 152 community participants across the four churches. Only individuals with moderately (≥140/90 and <160/100 mmHg; Group 1) or severely elevated BP (≥160/100 mmHg; Group 2) participated in the study interventions. Participants with normal BP (<140/90 mmHg) on initial screening were congratulated on their BPs and received a pedometer and materials on healthy nutrition and exercise. This initial screening concluded their participation in the study.
Intervention
The study intervention consisted of a culturally appropriate video on “What Is High Blood Pressure?.” The video educated viewers on high BP, how it is diagnosed, and the importance of treatment to prevent secondary complications. The 3-minute video was animated and available in both English and Spanish. Through pilot testing and prior studies, the video has been tested on patients with similar demographics as study participants, and it was well-received (Prendergast et al., 2018).
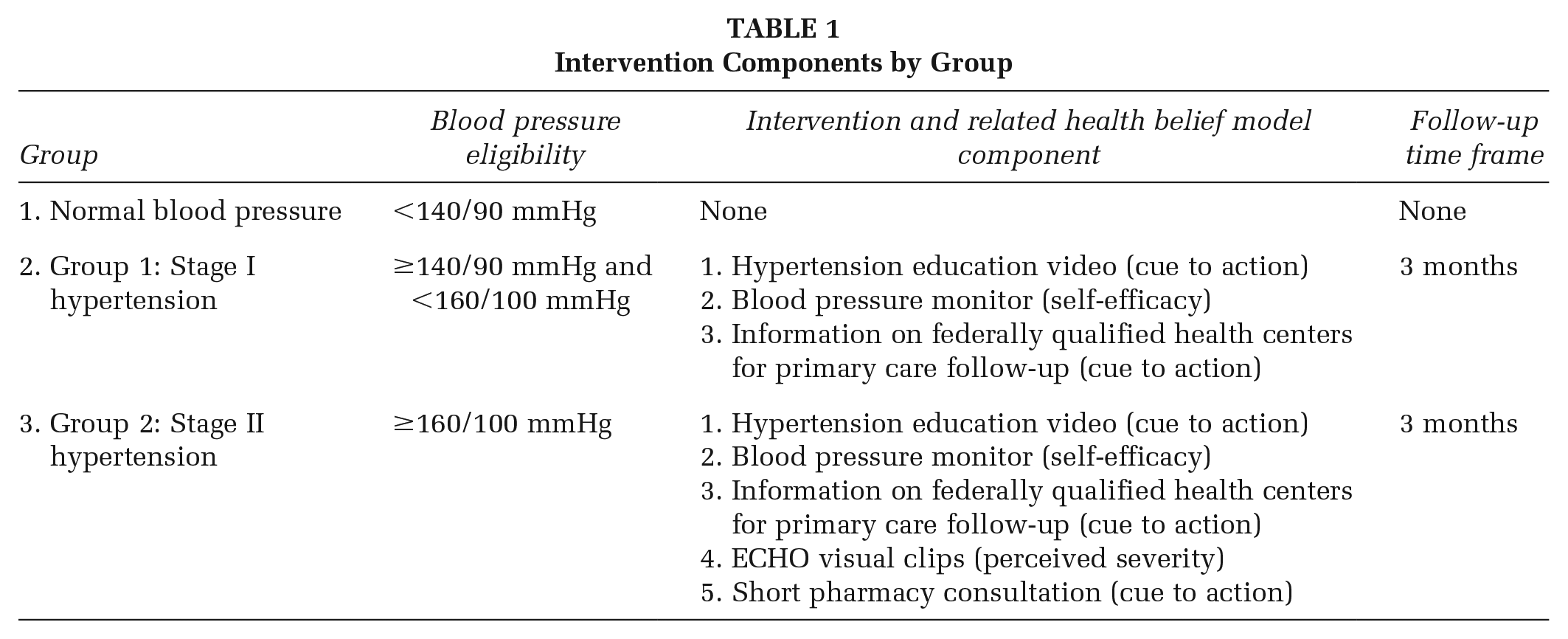
Individuals with severely elevated BPs (≥160/100 mmHg) additionally viewed a brief collection of echocardiogram images showing early but reversible subclinical changes due to uncontrolled hypertension and had a brief on-site consultation with a clinical pharmacist. Following completion of the intervention, all participants received automated BP monitors (with training on how to use them) and information on federally qualified health centers (FQHCs) located in their respective geographic location for ongoing primary care. Intervention components by group is displayed in Table 1.
Intervention Components by Group
Details of Screening and Intervention Components
Components of Screening (N = 152)
Screening and demographic survey: There were six questions focused on sociodemographic data. Data collected included BP, age, gender, self-reported race and ethnicity, and current home address.
Modified health care access survey: There were four questions related to presence or absence of health care coverage, established primary care, and date of most recent primary care physician visit.
Modified heart disease and stroke risk community screening form: There were seven questions related to presence or absence of cardiovascular risk factors, hypertension, tobacco use, diabetes, and obesity.
Components of Intervention (Groups 1 and 2, N = 89)
Hypertension educational video: Participants viewed a 3-minute video on hypertension aimed at educating study participants about high BP and the importance of treatment to prevent secondary complications. Videos are bilingual and culturally sensitive.
FQHC resource: A systematic review of hypertension screening in communities found that only 16% of studies reported referral to primary care after screening, and recommended that studies with good follow-up of patients to definitive hypertension diagnosis are needed (Fleming et al., 2015). In our study, participants received a one-page handout with addresses and phone numbers to the nearest FQHC in their community, so that they could connect with primary care for follow-up if they did not have a primary care provider.
Home BP monitoring (HBPM) kit: All participants received an HBPM kit containing an automatic BP monitor (Omron 5-Series HEM-7131-Z) and self-reporting logbook. Participants were shown how to use the BP monitors prior to leaving the community church. The patient-centered benefit of HBPM has been repeatedly demonstrated and is recommended as an important component of hypertension management (Jaffe et al., 2013). HBPM has been shown to improve adherence to medications, promote healthy lifestyle changes, and aid in the optimization of treatment.
Additional Components of Intervention (Group 2, N = 43)
Visual echocardiogram image clips: Visual images of echocardiograms demonstrating normal and abnormal cardiac ultrasounds with early subclinical changes attributed to uncontrolled hypertension were viewed by participants as an empowerment tool to educate and motivate participants to improve their BP. An emergency medicine physician provided these images in a simplified way that could be easily understood, especially for participants who may have low health literacy levels (see Figure 1 for example image). Participants also had the opportunity to ask questions to the physician.
We found that the real-time visualization of cardiac ultrasound images was a significant patient motivator and empowerment tool in a previous pilot study (Prendergast et al., 2015).
On-site brief consultation with clinical pharmacists: Participants with severely elevated BPs (Group 2) had a 10- to 15-minute consultation with a clinical pharmacist. The sessions included medication review, potential drug interactions, medication adherence assessment, BP goals and monitoring frequency, and basic hypertension education (complications, diet, exercise).

Visual Echocardiogram Image Clip Example
Assessments for Groups 1 and 2
Hypertension knowledge assessment: There were 10 questions to assess respondents’ knowledge in defining hypertension, lifestyle, and behaviors that may affect BP, and their understanding of long-term consequences of hypertension. The survey has been previously validated within urban populations with high proportion of Black and Latino patients. Scores are categorized into tertiles that indicate low (≤7), medium (8), or high (9–10) levels of hypertension knowledge (Sanne et al., 2008).
Modified Morisky Scale health survey: The modified Morisky scale is a previously validated four-item instrument to assess self-reported patient adherence related to antihypertensive medication. The modified Morisky scale provides a total score with a range of 0 to 4, with higher scores indicating lower adherence to medication. The scores of the modified Morisky scale can be classified as low compliers (3–4), medium compliers (1–2), and high compliers (0; Morisky et al., 1986).
Patient Activation Measurement survey: This is a previously validated 10-item instrument that measures level of engagement (activation) and has been used in hypertension interventions with higher scores indicating better self-care behaviors (Hibbard et al., 2005).
Conceptual Model
Hypertension screening identifies people at higher risk for stroke, heart attacks, and renal failure (due to their BP) but who may not have experienced symptoms. Because hypertension is largely asymptomatic until often irreversible damage has occurred, many patients do not follow instructions to start a prescribed medicine or change their diet. The health belief model (Rosenstock, 1974) informed our intervention to deal with noncompliance in such situations. According to the health belief model, asymptomatic patients will not follow prescribed treatment regimens or adopt behavior change unless they accept that although they have no symptoms, they do in fact have hypertension and that this puts them at risk for irreversible cardiovascular injury (perceived susceptibility). They must understand that uncontrolled hypertension can lead to heart attacks, renal failure, and strokes (perceived severity). By watching the echocardiogram image clips, the intervention group can visualize the severity of early subclinical changes within one’s body as a result of uncontrolled hypertension. Patients must understand that taking prescribed medication or following a recommended dietary regimen can prevent progression of and sometimes reverse the damage caused by hypertension (perceived benefits) without excessive difficulty (perceived barriers). Educational videos and a collaborative discussion with an emergency department–based pharmacist/advanced practice nurse might encourage people to consistently follow medication regimens and dietary recommendations (cues to action). By arming all participants with a list of nearby FQHCs in their community and giving them HBPM kits, we hope that we build their confidence in taking control of their BP (self-efficacy).
Measures/Assessment of Outcomes
Following the initial screening and education visit, there was one additional in-person visit at 3-months for BP reassessment. All intervention participants received phone calls for verification of contact information at 1 and 2 months. During the final visit, study participants completed an exit survey and assessment of medication adherence. Study personnel conducting the BP reassessments were blinded to the initial BP readings for all study participants. On completion of final study assessments, participants received a $25 gift card from Subway restaurant as compensation for their participation. Participants were offered an opportunity to participate in a voluntary focus-group regarding the study. Analysis of the focus group will be reported as part of a separate manuscript.
Clinical outcomes were assessed at two time points (0 and 3 months). Baseline and follow-up BP measurements were recorded on seated participants by trained research assistants using digital Omron HEM-7131-Z and LifeSource UA-789AC BP monitors. The primary outcome was mean BP differences at 3 months. Secondary outcome was the percentage of participants with controlled BP (<140/90 mmHg for Group 1 and <160/100 mmHg for Group 2) at the study completion.
Statistical Analysis
The unit of analysis was the individual. Summary statistics of sociodemographic characteristics (age, sex, self-reported race and ethnicity), tobacco use, and medical history were calculated for all groups—normal BP, Stage I BP, and Stage II BP. We compared this information among the three groups using analysis of variance for continuous variables and chi-square tests for categorical variables. Paired t test was employed to identify significant overall difference between pre- and postintervention measurements within each group for Group 1 and Group 2. Analysis was completed using Stata Version SE 15 (College Station, TX: StataCorp LP).
Results
Participant Characteristics
A total of 152 participants completed the BP screening across the four community churches with 59% (n = 89) of participants screening positive for hypertension (BP ≥ 140/90 mmHg). Table 2 shows the baseline characteristics of study participants by group.
Baseline Characteristics of All Three Groups—Normal Blood Pressure, Group 1, and Group 2

NOTE: N/A = not applicable.
There were several characteristics that varied across the groups. Age was highest for Group 2, then Group 1, then the normal BP group. Proportion of Black participants was highest for Group 1 and lowest for the normal BP group, and proportion of Hispanic participants was highest in the normal BP group and lowest in Group 1. A higher proportion of people in Group 2 had been told that they had high BP than in any other group. Group 2 also had a significantly higher proportion of <30 minutes of physical activity on most days than the other groups. While not statistically significant, the percentage who were smokers or lived with smokers was lowest for normal BP and highest for Group 2. Similarly, having a family member with a heart attack before 55 and being overweight were lowest for the normal BP group and highest for Group 2. Access to care was not significantly different across the three groups, although health care coverage was most prevalent for Group 2 and least prevalent for people with normal BP. Also, hypertension knowledge was not significantly different between Group 1 and Group 2.
Moderately Elevated BP (Stage I: Intervention Group 1)
Table 3 shows that mean BP decreased overall (−5.0 mmHg for systolic blood pressure [SBP] and −2.2 mmHg for diastolic blood pressure [DBP]) for Group 1 at 3 months following the intervention; however, changes in neither SBP nor DBP were statistically significant (p = .109 and p = .209, respectively). Of 31 participants who followed up at 3-months, 36% (n = 11) had improvement of both SBP and DBP into normal range. Fifty-five percent (n = 17) had improvement to a normal SBP and 65% (n = 20) had improvement to a normal DBP (not shown). The percentage with an active prescription for an antihypertensive medication increased from 43% to 47% (p = .326). Of those on a medication, medication adherence improved significantly (p = .012).
Change in Blood Pressure and Medication Adherence for Those Who Completed Follow-Up: Baseline to 3-Month Follow-Up

Of those on a medication. bLower is more adherent.
Severely Elevated BP (Stage II: Intervention Group 2)
Table 3 also shows that, for Group 2, mean BP for those who followed up at 3-months changed by −15.0 mmHg for SBP and −7.5 mmHg for DBP. Reductions in both SBP (p value = .001) and DBP (p value = .001) were statistically significant. Of the 29 participants who completed their follow-up at 3 months, 55% (n = 16) had a decrease in both SBP and DBP to the moderately elevated range and 31% (n = 9) had BP in the normal range (not shown). The percentage of participants with an antihypertensive medication prescription increased from 64% to 68% (p = .573). Medication adherence remained constant for Group 2 from baseline to follow-up (p = .817).
Discussion
In our study, participants with moderately elevated BP (Group 1) showed a decrease in mean BP from 143.5/88.0 mmHg at baseline to 138.5/85.8 mmHg at 3 months follow-up; however, the change was not significant. For those with severely elevated BP (Group 2), there was a significant decrease from 165.4/98.3 mmHg to 150.4/90.8 mmHg. After the intervention, participants with controlled BP for Groups 1 and 2 were 35.5% and 55.2%, respectively.
Uncontrolled hypertension is a major public health problem particularly among racial/ethnic minority populations, leading to higher prevalence of secondary cardiovascular complications such as heart failure, stroke, myocardial infarction, and end-stage renal disease as compared to other nonminority groups (Wilson et al., 2002). Among racial/ethnic minority populations, racial disparities in awareness and treatment of hypertension continue to exist (Bennett et al., 2016).
As demonstrated in our study, the majority of individuals screened had at least moderately elevated BP (59%), which is significantly higher than the national average-estimated by the Centers for Disease Control and Prevention to be approximately 33.2% for adults aged 20 or older. In addition, there were a sizable number of participants who were unaware of their elevated BP (44% in Group 1 and 30% in Group 2). Again, these numbers are much higher than the national average of 16% (Paulose-Ram et al., 2017). Two churches in the study were predominately Latino, and previous studies suggest that Latinos tend to have higher rates of undiagnosed hypertension due to lack of awareness of their hypertension as compared to nonminority groups (Centers for Disease Control and Prevention, 2017; Guzman, 2012). National estimates show that 30% of uninsured adults were unaware of their hypertension compared to 14% of insured adults, and as health care visits increased, the percentage of adults unaware of their hypertension status decreased (Paulose-Ram et al., 2017). These findings suggest a need to intervene in groups who lack access to health care. Given the importance of early diagnosis and treatment in order to prevent secondary cardiovascular complications, educational and empowerment BP screenings in partnership with community-based organizations, such as churches, may be cost-effective, efficient, and favorable to affect the health disparities associated with cardiovascular complications in racial/ethnic minority populations.
Identification and removal of perceived barriers to hypertension control among racial/ethnic minority populations remain unsolved public health problems (Wilson et al., 2002). Most individuals in our pilot indicated no significant access to care barriers and reported having visited a primary care physician within the past 12 months, suggesting that presence of other factors, such as education and empowerment, contributing to lack of BP control. Our previous studies in predominantly racial/ethnic minority populations with uncontrolled hypertension found that education coupled with empowerment was a significant patient motivator in controlling BP. The interventions conducted in the pilot were centered around these concepts of education (hypertension video) and empowerment (echocardiograms showing subclinical heart changes due to uncontrolled hypertension, on-site pharmacist consultation, HBP monitors, and information on local FQHCs for primary care follow-up).
Previous studies have demonstrated the effectiveness of hypertension interventions initiated in the community for vulnerable patient populations, with improvements in BP control and increased linkages and follow-up rates at primary care facilities (Levine et al., 2003; Walton-Moss et al., 2014; Ward et al., 2000). Meta-analysis of community interventions to manage hypertension among predominantly racial/ethnic minority groups found that hypertension education combined with individualized support for self-management of hypertension were associated with reductions in BP levels and improvements in BP control (Connell et al., 2008). One study explored the nontraditional health care setting of barber shops to target African American men with uncontrolled hypertension. Health promotion by barbers, along with medication management by specialty-trained pharmacists, showed large and sustained BP reduction after 6 and 12 months (Victor et al., 2018; Victor et al., 2019).
We were able to demonstrate effectiveness using not only educational techniques but also a multi-pronged empowerment approach (visual echocardiogram images and personalized pharmacy consultations). By utilizing a group setting with individualized support, study participants were engaged in a familiar/safe environment. Similarly to findings from the Community-Based Hypertension Control Project for an ethnically diverse population study that demonstrated that individualized counseling and home visits resulted in significant, sustained improvements in BP control, our study demonstrated greater BP improvements in those participants who had the pharmacist consultation at a 3-month observation period (Morisky et al., 2002).
Limitations
There were some limitations to this study. The greatest limitation was the small sample size of participants (N = 89), which limits generalizability of our results. Second, there was loss to follow-up for 15 participants (32.6%) in Group 1 and 14 participants (32.6%) in Group 2. Ideally, we would have liked to have 100% participant follow-up, and more participant engagement during the 3-month postintervention period may have helped alleviate this problem. Given that this was a pilot study, future renditions of this intervention will include implementations of lessons learned, larger number of participants, and more churches. Additionally, there were variations in participant characteristics between the study groups, such as mean age. Finally, physician leadership on the study was limited to emergency medicine physicians. Inclusion of primary care physicians and/or cardiologists in future similar studies may be helpful for better longitudinal outpatient follow-up care.
Implications for Practice, Policy, and Research
Hypertension is one of the most important modifiable risk factors for cardiovascular disease and stroke. Given the significant health disparity associated with uncontrolled hypertension, particularly among racial/ethnic minority populations, it is imperative that new models of community-based screening be evaluated. We found that expanding on traditional educational formats with empowerment opportunities was an effective means of engaging study participants.
A significant percentage of participants had improvements in their overall BP and the classification of BP category (improvement from severely to moderately elevated and from moderately to mildly elevated). The greatest improvements were seen in those individuals at higher cardiovascular risk due to severely elevated BPs (≥160/100 mmHg). This pilot highlights the impact that streamlined empowerment interventions with dedicated health personnel can have in high-risk community populations with elevated BPs. Future work can expand this model in more communities throughout Chicago and the nation.