
Abstract
Future control of the coronavirus disease 2019 (COVID-19) pandemic is dependent on the uptake of the COVID-19 vaccine. Many factors have swayed the public’s perception of this coronavirus and the new vaccinations, including misinformation, heightened emotions, and the divisive and tumultuous partisan climate. As such, vaccine hesitancy may be more prevalent for the COVID-19 vaccine than others. Healthcare workers are trusted sources of information and have the opportunity to influence an individual’s choice to take the vaccine. For those who initially present as unwilling to be vaccinated, trying to persuade them with facts and scare tactics may cause more resistance. By using the communication approach of motivational interviewing, practitioners can support autonomy to reduce defensiveness, use a guiding style to elicit ambivalence and provide information, address personal agency to ensure that their patients understand that their efforts can reduce risk, and evoke a person’s own argument for vaccination to decrease vaccine hesitancy.
Behaviors such as good hygiene, social distancing, and mask wearing are proven ways to slow the spread of coronavirus disease 2019 (COVID-19); however, there has been less than optimal adherence in the United States (Chou & Budenz, 2020). With the emergence and mobilization of multiple vaccinations approved for the general public, effective and timely control of the pandemic will be contingent on a majority of people agreeing to be vaccinated (Chou & Budenz, 2020). Vaccinations of all types have increasingly become an emotionally charged issue, resulting in “vaccine hesitancy” (Chou & Budenz, 2020; Puri et al., 2020).
Vaccine hesitancy is described by the World Health Organization as a “delay in acceptance or refusal of vaccines despite availability of vaccination services” and spans across a continuum from high vaccine demand to complete vaccine refusal (MacDonald, 2015). Vaccine hesitancy is complex with numerous factors influencing an individual’s acceptance including, but not limited to, misinformation about vaccines, distrust of the healthcare system or providers, negative experiences with a past vaccine, and beliefs and attitudes about health and prevention (Tustin et al., 2018). Fundamentally, people make decisions based on what feels most emotionally compelling and relevant in the moment—their concerns related to perceived risk versus perceived benefits of the vaccine (MacDonald et al., 2018).
The public’s perception of the COVID-19 pandemic has been specifically influenced by misinformation and unsubstantiated rumors that emerged on social media platforms and selected news programs and have subsequently been directed toward the COVID-19 vaccine (MacDonald et al., 2018; Puri et al., 2020). Furthermore, heightened and sustained emotions due to the pandemic, such as loneliness, uncertainty, isolation, fear, and anxiety, have led to negative affect and, for some, eroded their sense of agency that individual actions could and would make a difference (Chou & Budenz, 2020; Miller & Rollnick, 2013; Puri et al., 2020). Moreover, the current divisive and tumultuous partisan climate has resulted in a wide split among self-identified political party affiliation in their belief about the value of preventative COVID-19 measures and their willingness to receive the vaccine (Suffolk University Political Research Center, 2020). Finally, COVID-19 has disproportionately affected some racial and ethnic minority groups who may also be more hesitant to trust scientists, medical professionals, or new medical treatments (Funk et al., 2020; Shen et al., 2021).
By itself, information does not change entrenched behaviors and is not an effective stand-alone intervention, especially when facing a divisive issue such as vaccination (Gagneur, 2020; Miller & Rollnick, 2013). Addressing vaccine hesitancy is most effective when using a multipronged approach. Strategies include using consistent public health messaging, leveraging social media, highlighting endorsements by trusted public figures, detecting and addressing hesitancy in identified high-risk populations, ensuring all healthcare workers (HCWs) are providing consistent information and recommendations, using effective communication to engage and explore the issue, and employing evidence-based behavior change strategies (Chou & Budenz, 2020; MacDonald et al., 2018; Puri et al., 2020). This article will focus on presenting best practice for HCWs in using an evidence-based communication approach and effective behavior change strategies to assist their patients in making the best healthcare decision for their family and themselves.
Motivational Interviewing: A Best Practice Communication Approach
Motivational interviewing (MI) is a patient education or health coaching approach that is fully standardized and consistently demonstrated as causally and independently associated with positive behavioral outcomes (Frey et al., 2020; Miller & Rollnick, 2013). There is strong evidence and support for the use of MI by HCWs across a wide range of challenging behaviors, including treatment adherence and vaccine hesitancy (Frey et al., 2020; Gagneur, 2020; Houck et al., 2013). MI is “a collaborative conversational style for strengthening a person’s own motivation and commitment to change” (Miller & Rollnick, 2013, p. 12). The approach is grounded in social–psychological theory, including cognitive dissonance, self-efficacy, and self-perception; indeed, it is congruent with the leading behavior change theories and models, including the transtheoretic model, the health belief model, the social cognitive theory, and cognitive dissonance theory (Houck et al., 2013). Core elements of MI have been well-described in the literature and include the spirit of MI, core communication skills, attending to the language of change, and utilizing the structure of four processes to guide an individual through the intervention (Miller & Rollnick, 2013). We will focus on how MI principles and strategies can be leveraged to address vaccine hesitancy.
Using MI to Address Vaccine Hesitancy
MI embraces multiple strategies that relate specifically to the issues that contribute to COVID-19 vaccine hesitancy (Gagneur, 2020). First, it reduces defensiveness and allows the HCW to engage and build trust and rapport. The “worst-case scenario” in healthcare conversations is when a HCW is arguing for the targeted behavior (in this case, the vaccination) and the individual is arguing against it (Miller & Rollnick, 2013). In a more traditional or directive approach (often the norm in many healthcare settings), the HCW’s agenda and recommendations are prioritized, which results in this worst-case scenario and the resulting effects—patient defensiveness, the presentation of arguments for only one side of their ambivalence, and the inevitable outcome of the patient disengaging or shutting down. The MI approach avoids this scenario by employing reflective listening to draw out the patient’s views about vaccination and validating their concerns. Of note, the HCW’s perception about role and agenda drives their intentions going into the interaction which, in turn, determines their strategies. For a direct comparison between the traditional and MI approach, see Table 1.
Comparison of Perceived Role and Agenda by HCW
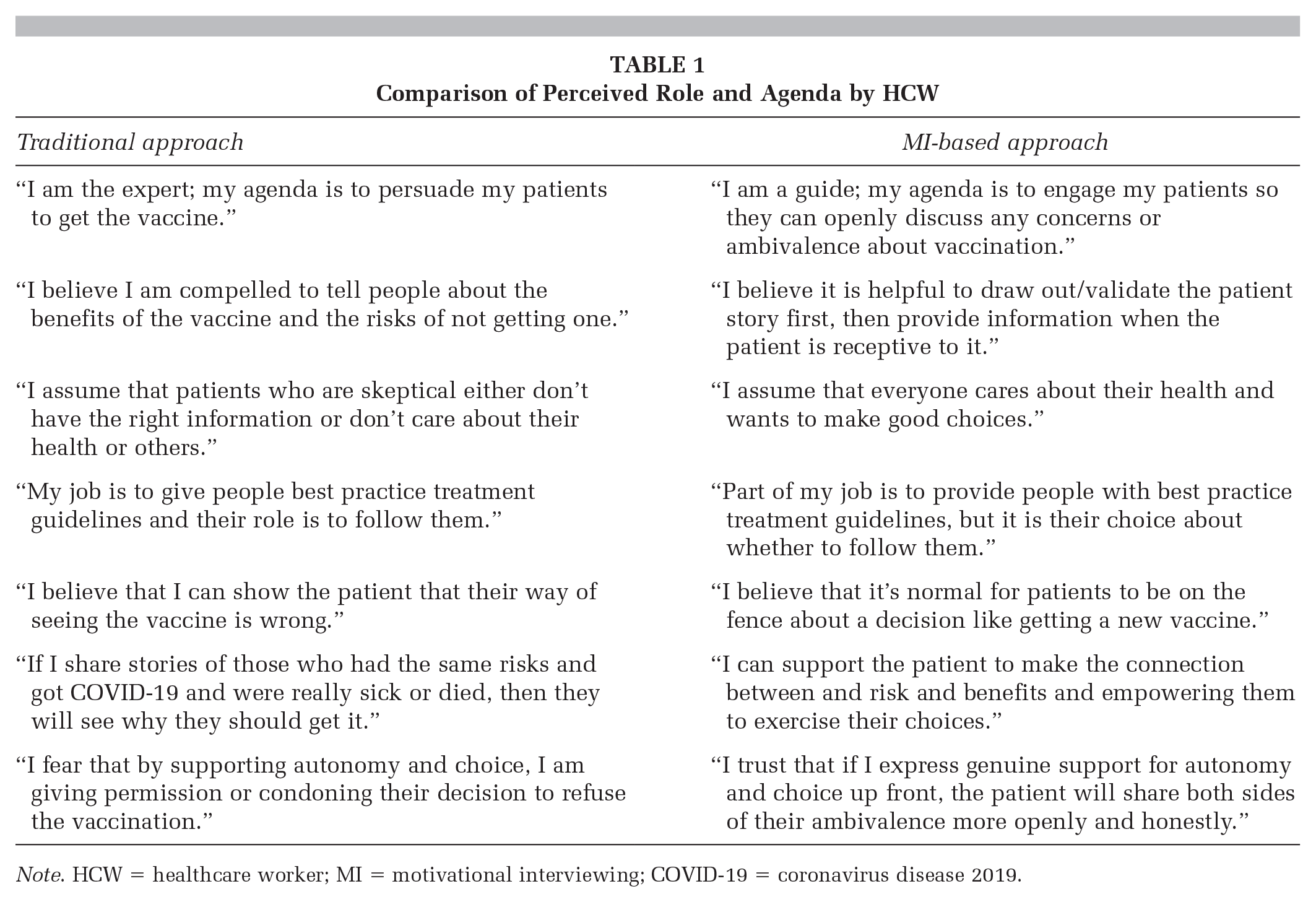
Note. HCW = healthcare worker; MI = motivational interviewing; COVID-19 = coronavirus disease 2019.
Additionally, genuine support for autonomy and choice is offered up front, which allows patients to feel respected. In response, their shoulders go down, making it more likely that they will share their concerns more openly and honestly. Once trust and rapport have been established (which can happen very quickly), the HCW now has the opportunity to introduce some of their own perspectives and information, and possibly influence decisions.
Second, MI favors a guiding style (vs. a directing or following one) to help people share and work through their ambivalence after they have been engaged by the HCW. (Note: In the traditional or directive approach, if the worst-case scenario has developed, the patient will not generally share their ambivalence; thus it appears as if there is none.) This is done by exploring and evoking the patient’s own arguments in favor of the targeted behavior (getting the vaccine), even if only eliciting what others have shared about the possible benefits. This is known as the “best-case scenario” in a healthcare conversation—one in which HCWs evoke and reflect what is called “change talk” from the patient. In the case of vaccine hesitancy, initial change talk is the patient’s possible desire, ability, reasons, and need to get vaccinated, even if their list is brief. Multiple research studies have shown a positive correlation between change talk and commitment strength to the targeted behavior, followed by increased treatment adherence (Frey et al., 2020; Gagneur, 2020; Houck et al., 2013). Once change talk has emerged, the skillful MI practitioner strengthens it by asking for elaboration, reflecting it, affirming it, or summarizing it.
Moreover, the MI approach encourages HCWs to identify patient concerns, fears, and misconceptions; thus, they are able to provide relevant and tailored information to the patient when they are receptive to it. Generally, after rapport has been established and change talk has been evoked, the practitioner can readily ask what the patient knows about an aspect of the issue at hand; for example, what does the patient know about current risks of infection, what do they know about the approval process of the vaccine, or what do they know about the rate and type of side effects experienced from the vaccine? Once they have responded, the HCW can affirm their knowledge and then ask for permission to share some information or an alternative perspective. Depending on the patient’s stance, it may be helpful to again support autonomy at this time. After providing the information, an essential component of this information exchange process is asking what the person thinks about the information that was offered (Miller & Rollnick, 2013).
Last, the MI approach does significantly more than enable information to be shared. It can support and enhance one’s sense of personal agency—the belief that one’s actions can make a difference. By neutralizing the emotional vortex, the HCW creates a safe space and can guide people into more objective discussions about the pros and cons of status quo versus getting vaccinated. This also allows the HCW the opportunity to affirm their patients’ insights that empowers them to independently exercise their choice to protect or promote their health. The optimal result is that initial skeptics become at least open to the consideration that using preventative measures such as masks, social distancing, and vaccination can lower their risks and have a positive impact on their own and loved ones’ lives. This increase in agency can be far-reaching as it crosses over into other self-management and health-promoting behaviors.
Applications to Health Promotion
The MI approach is not without its drawbacks; the major one being the time, effort, and resources that it demands to train HCWs to a competent level commensurate with the outcomes found in the literature. Typically, organizations that do provide training in MI rely on a traditional “one-and-done” training model. Thus, their staff do not significantly improve their skills, much less reach MI proficiency. Research is clear that HCWs only develop competency when the following conditions are met: (1) There is management support for the skill-set acquisition, as reflected in job description, acknowledgment of competency achievement, reduction in workload during the training period, and inclusion of the skill-set reflected in quality assurance and job performance reviews; (2) staff receive an interactive and comprehensive introductory training (12–14 hours) in an in-person or online format; and (3) staff receive ongoing competency assessment and concrete feedback from actual patient sessions, accompanied by mentoring and skill-building sessions (Miller & Rollnick, 2013).
Another drawback of the approach is a pervasive misunderstanding about the full complexity of MI and the common assumption that it is interchangeable with other patient-centered communication approaches. Although the use of communication micro skills—open questions, affirmations, reflections, and summaries—are encouraged when using MI, these are merely building blocks in the early stages of competency development. MI prizes engagement, rapport building, goal setting, and other evidence-based behavior change strategies as well. However, after full proficiency is reached, what differentiates MI from other approaches is the intentional goal of activating the patient through the evocation of change talk and empowering them by addressing their self-efficacy and/or personal agency. This intention is based on values, assumptions, and science: (1) the value of supporting autonomy; (2) the assumption that people do care about their health and will make good decisions with the right support and guidance; (3) the belief that the patient should be a full partner and primary driver in the health coaching process rather than a passive recipient of information; and (4) the knowledge of brain imagery science that elucidates how people work through ambivalence to determine their stance on future behaviors, as supported by the self-perception theory (Frey et al., 2020; Houck et al., 2013; Miller & Rollnick, 2013). As an ambivalent person hears themselves verbalize the benefits of being vaccinated, the part of the brain that is linked with self-perception is activated, leaving the person feeling more strongly about that side of their ambivalence (Houck et al., 2013).
HCWs have a significant opportunity to support individuals in making decisions about receiving the COVID-19 vaccine. Along with other population management strategies, MI can be an effective and useful communication approach to help reduce vaccine hesitancy. By reducing defensiveness, increasing engagement, evoking change talk, and sharing relevant information at the right time, HCWs can empower people to make informed decisions about their health.
Finally, while the focus of our article is on strategies to support increased vaccine uptake, ensuring that all people—especially those at higher risk of infection and death—have resources and support in making vaccination decisions is an integral component of vaccine equity (Phelan et al., 2020). By adopting an MI approach, we ensure that people are treated with respect and have the opportunity to consider the COVID-19 vaccine as a public health priority for all. As such, it is critical to recognize and highlight the larger context and ecosystem in which people have the opportunity to make decisions about vaccination. Community-based organizations, including community centers, faith-based organizations, universities, pharmacies, schools, and their staff, can play a large role in providing outreach, education, and equitable access to the COVID-19 vaccine (Phelan et al., 2020). For more information on MI, visit our Supplemental Material for more description, examples, and resources.
Supplemental Material
sj-pdf-1-hpp-10.1177_15248399211016463 – Supplemental material for Using Best Practices to Address COVID-19 Vaccine Hesitancy: The Case for the Motivational Interviewing Approach
Supplemental material, sj-pdf-1-hpp-10.1177_15248399211016463 for Using Best Practices to Address COVID-19 Vaccine Hesitancy: The Case for the Motivational Interviewing Approach by Amanda Gabarda and Susan W. Butterworth in Health Promotion Practice
Footnotes
Authors’ Note:
Amanda Gabarda declares that she has no conflict of interest. Susan Butterworth owns Q-consult, LLC, a consulting firm that provides motivational interviewing training services. She has an approved plan for managing any potential conflicts arising from her consulting activities. There was no external funding to support this work.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.