
Abstract
HIV-related stigma remains a considerable barrier to engaging at-risk populations in HIV testing and prevention programs. We assessed the moderating role of HIV-related stigma on the relation between perceived susceptibility to HIV and HIV testing intention among college students. We hypothesized that the moderating role of HIV-related stigma would be differential between heterosexual and sexual minority college students. We administered a survey focused on HIV-related knowledge, attitudes, and behaviors in spring 2016 (N = 2,159). We used multigroup path analysis to analyze the hypothesized moderation. HIV-related stigma moderated the relation between perceived susceptibility and testing intention for heterosexual but not sexual minority college students. Specifically, higher HIV-related stigma decreased the association between perceived susceptibility and testing intention. These results demonstrate the importance of priority population segmentation for HIV testing campaigns.
Approximately 1.2 million people in the United States are living with HIV (PLWH). Within this population, an estimated 14% are unaware of their HIV status (Centers for Disease Control and Prevention [CDC], 2020). Young people and young adults (aged 13–24 years) are particularly affected by HIV, accounting for 21% of all new HIV diagnoses (CDC, 2020). While young people and young adults are grouped in the 13- to 24-year age range, not all young people encounter similar risk (CDC, 2020). College students in this age-group exhibit specific factors placing them at higher risk of HIV transmission, including new independence, peer pressure to experiment sexually, potentially inadequate knowledge, and variable HIV-related stigma and testing beliefs. Research has documented that college students frequently engage in condomless sex and engage with multiple partners, yet only 28.5% of students report that they have been tested for HIV (American College Health Association, 2020). Therefore, additional research on how to increase HIV testing engagement among college students is necessary to meet the public health priority of reducing HIV risk and transmission.
Theories of health behavior provide frameworks to examine HIV transmission risk and testing uptake. Self-perceived susceptibility and risk are constructs that can be used to explain individuals’ perceived HIV exposure risk and to enhance uptake of self-protective behaviors like condom usage. These constructs align with common health behavior theories such as the health belief model (HBM; Glanz et al., 2015), which has been used as a framework to describe perceived risk of HIV transmission among higher risk populations. Theory informs us that people with higher perceived susceptibility, in the presence of available services and cues to action, will have higher testing intention. However, the presence of psychosocial barriers such as stigma may reduce intention to get tested. HIV-related stigma remains a large barrier to HIV testing engagement among at-risk populations (Earnshaw et al., 2012). Therefore, assessing the impact of HIV-related stigma on the relation between perceived susceptibility and testing intention is key to developing appropriate interventions and theories for research and practice.
In positing a role for HIV-related stigma in value-expectancy theories (like the HBM), it is crucial to recognize that stigmatizing beliefs vary across populations. There is a rising consensus that sexual health education be comprehensive and inclusive of lesbian, gay, bisexual, transgender, and questioning students (LGBTQ+) and intersectionality within this community. Additionally, HIV testing campaigns have been explicitly prioritizing sexual and gender minority populations for decades (e.g., Noar et al., 2009). There have also been a multitude of HIV-related stigma interventions with the intention to reduce HIV-related stigma and cultivate more interest in HIV treatment, care, and support, specifically prioritizing the LGBTQ+ population (Stangl et al., 2013). These health promotion programs are a likely contributor to the relatively lower HIV-related stigma observed among sexual minority (LGBQ+) communities in comparison with their heterosexual counterparts (Beaulieu et al., 2014; James et al., 2021).
Despite a theorization of the role of stigma and perceived susceptibility in the development of testing intentions, it is unclear if HIV-related stigma moderates the relation between perceived susceptibility and testing intention. Based on previous literature (e.g., Gamarel et al., 2018; Golub & Gamarel, 2013), we hypothesize that HIV-related stigma will moderate the relationship between these health behavior constructs. Due to the historical prioritization of sexual minorities in health communication messaging and the (relatively) lower stigmatizing beliefs regarding HIV observed in sexual minority populations, we also hypothesize that the moderating role of stigma will be differential based on the experiences of being LGBQ+ (i.e., the moderating role of stigma will be weaker among sexual minorities).
Methods
Procedure and Sample
This project is a secondary analysis of survey data collected among college students between January and February 2016. This study was declared exempt by the University of Florida Institutional Review Board. Students were recruited from a large university in the Southeastern United States through a random sampling (without replacement) strategy conducted by the University Registrar’s Office: 10,000 students were contacted. A total of 3,162 responded to the survey; however, only 2,343 completed the questionnaire. Our analytic sample for the present study included 2,159 students who completed the sexual orientation item. The majority of students in our sample were heterosexual, female, White, and sexually active (see Table 1).
Sample Characteristics
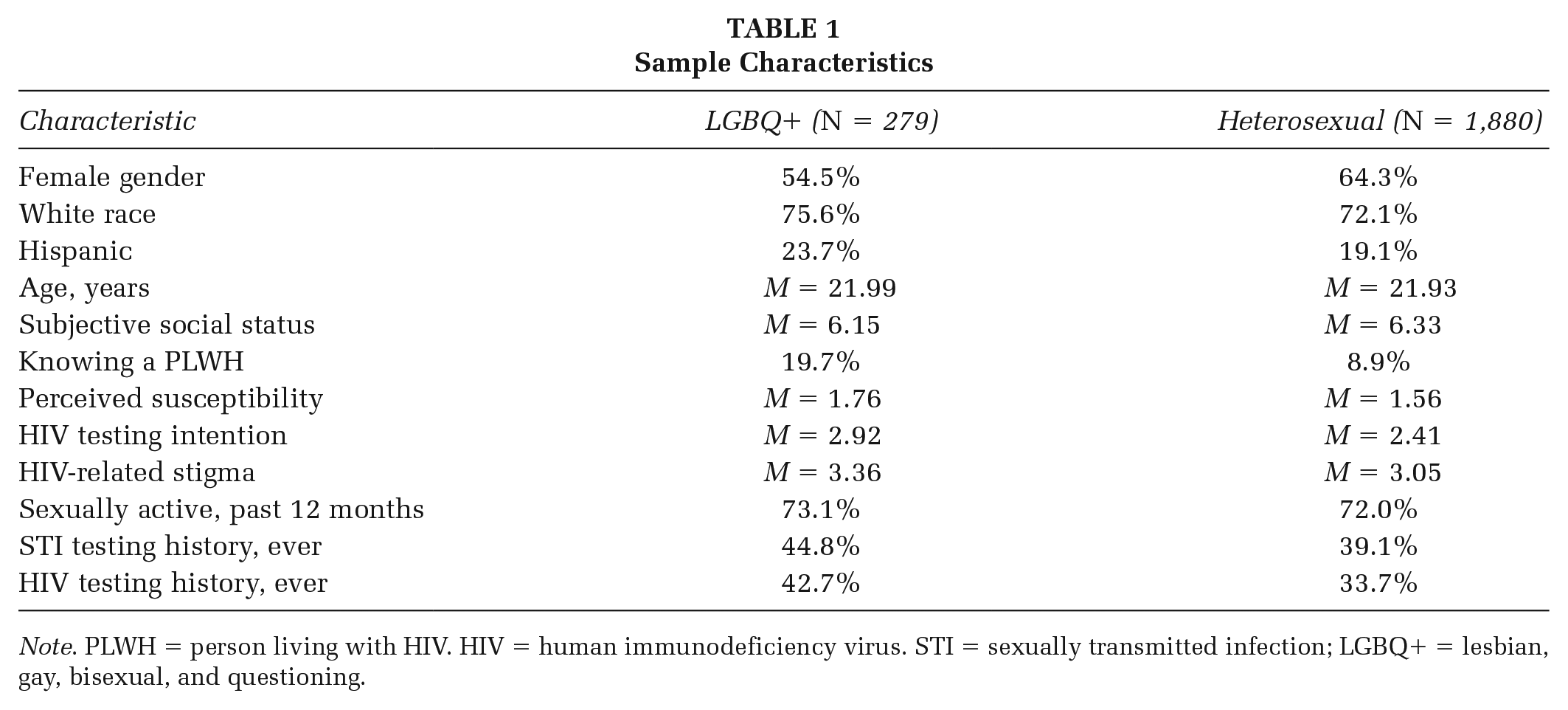
Note. PLWH = person living with HIV. HIV = human immunodeficiency virus. STI = sexually transmitted infection; LGBQ+ = lesbian, gay, bisexual, and questioning.
Measures
HIV-Related Stigma
Our conceptualization of HIV-related stigma in the HBM is that of a modifying factor. HIV-related stigma was measured using a revised version of the Stigmatizing Attitudes Towards People Living with HIV/AIDS Scale (SAT-PLWHA-S; Beaulieu et al., 2014). The revised SAT-PLWHA-S is a six-factor, 26-item scale that measures prejudice, discrimination, and stereotyping attitudes toward PLWH (James et al., 2021). Certain items are reverse coded (Beaulieu et al., 2014); then, item responses are averaged to calculate stigma scores. Scores range from 1 to 4, with lower scores indicating more stigmatizing (i.e., less positive) views of PLHIV.
Antecedents
Perceived susceptibility and HIV testing intention are the behavioral antecedents conceptualized in the HBM, and independent and outcome variables in this study. Perceived susceptibility was measured by asking students their perceived likelihood of being infected with HIV; response options were “none,” “small,” “moderate,” and “large.” HIV testing intention was measured using a 5-point Likert-type item: “How likely is it that you will be tested for HIV within the next 12 months?” with response options “very unlikely,” “unlikely,” “unsure,” “likely,” and “very likely.”
Covariates
Covariates in our analysis were chosen based on previous empirical and theoretical research on HIV testing intention and utilization (Anwuri et al., 2017; Glanz et al., 2015) and are conceptualized as modifying factors in the HBM. As this is a secondary analysis, we are limited to the covariates originally measured. We included demographic, social network, and behavioral covariates. Demographic characteristics included were self-reported gender, racial identity (dichotomized to White vs. non-White), Hispanic ethnicity, and age. Subjective social position was measured using the MacArthur Scale of Subjective Social Status, where respondents selected the “rung” of their perceived location on a ladder in comparison with other people in the United States; scores range from 1 to 10, with higher scores indicating higher perceived social status. The MacArthur Scale has demonstrated convergent validity with both sociofinancial indicators of social position and health status (Cundiff et al., 2013). Social network status was measured by one variable: having a friend, family member, or colleague who was a PLWH. Behavioral covariates included (1) being sexually active (i.e., oral, anal, or vaginal intercourse during the past 12 months), (2) ever being tested for an STI, and (3) ever being tested for HIV.
Data Analysis
We used MPLUS version 8 for all analyses using a maximum likelihood estimator with robust standard errors (MLR; appropriate for non-normally distributed outcomes). First, we conducted a path analysis model using the full, ungrouped sample to identify if HIV-related stigma moderated the relation between perceived susceptibility and HIV testing intention. Moderation was tested as an interaction term (i.e., centered perceived susceptibility * centered HIV-related stigma), and criteria for evidence of moderation was a significant interaction term. We then constructed a multigroup path analysis model to test our primary hypothesis—that is, the moderating effect of HIV-related stigma differs between heterosexual and nonheterosexual college students. To test this hypothesis, we estimated an (1) unconstrained, full-comparison model and (2) a model constraining the main effects of perceived susceptibility and stigma, and the interaction term. We used Muthén and Muthén’s (n.d.) procedures for chi-square difference testing using loglikelihood values estimated using MLR to discern if the constrained model fit better than the unconstrained model.
Results
First, we ran a full-sample model to assess the moderating effect of HIV-related stigma between perceived susceptibility and HIV testing intention. The main effect of perceived susceptibility was significant (β = 0.220, p < .001), but the main effect of HIV-related stigma and the interaction between stigma and perceived susceptibility were not significant (see Table 2). We then estimated an unconstrained two-group path model where all paths were freely estimated and a model where the effects of interest (i.e., main effect and interaction term) were constrained across groups. The unconstrained, freely estimated, model had a significantly better model fit than the constrained model, indicating varying effects of the independent and interaction variables between sexual minority and heterosexual students.
Standardized Path Coefficients Testing the Moderating Effect of HIV-Related Stigma on the Relation Between Perceived Susceptibility and Testing Intention
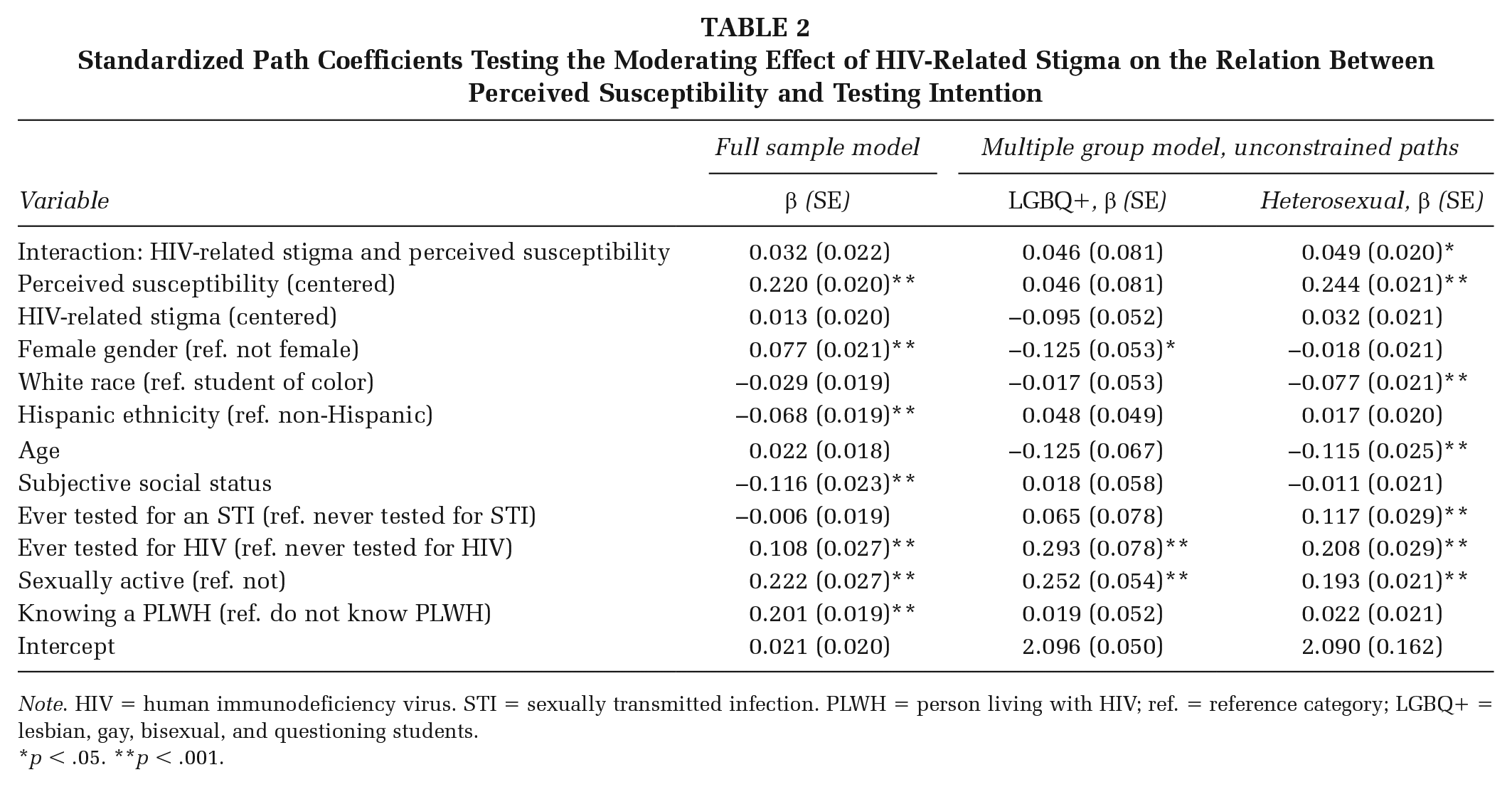
Note. HIV = human immunodeficiency virus. STI = sexually transmitted infection. PLWH = person living with HIV; ref. = reference category; LGBQ+ = lesbian, gay, bisexual, and questioning students.
p < .05. **p < .001.
Among heterosexual college students, the main effect of perceived susceptibility to HIV infection was significant and had the highest standardized coefficient (β = 0.244, p < .001). Higher HIV testing intention was observed for students who had higher than average susceptibility, those who were sexually active, and students who had previously been tested for STIs and HIV. Among sexual minorities, the only significant covariates associated with higher testing intent were HIV testing history and being sexually active (β = 0.293 and 0.252, respectively; ps < .001). Lower HIV testing intention was observed for students who were White and for younger heterosexual students. The interaction effect of stigma on the relation between perceived susceptibility and intention was significant for heterosexual (β = 0.049, p < .017) but not sexual minority students (β = 0.293, p = .568). The pattern of the interaction plots indicated that as our measured variable of HIV-related stigma increased, the effect of perceived susceptibility on HIV testing intention also increased.
Discussion
The HBM is one of the most widely taught and applied theories in health promotion practice, and additional research is needed to understand the role of psychosocial moderating/modifying variables on primary constructs and health behavior outcomes (Glanz et al., 2015). Globally, research findings on the relationship between perceived susceptibility to HIV testing and HIV testing intention are equivocal and, in many cases, found to be insignificant (Evangeli et al., 2016). However, in a sample of community college students in the United Stataes, heightened risk perception was associated with increased intention to get tested (Anwuri et al., 2017). In the full ungrouped analysis, perceived susceptibility was associated with greater intention to get tested, but the effect of HIV-related stigma was not significant. Although HIV-related stigma did not moderate the relation between perceived susceptibility and HIV testing intention in the full sample, moderation did occur in subgroup analyses: higher stigma decreases the effect of perceived susceptibility on HIV testing intention among heterosexual but not sexual minority, college students. As such, HIV-related stigma may be conceptualized as a barrier to HIV testing intention, with differential effects between sexual orientation groups.
Limitations
The findings of this study should be interpreted with respect to the limitations of the study. Data were collected from students at a single, large university via a self-report cross-sectional survey. Therefore, we are unable to ascertain temporality necessary to infer a causal relation between perceived susceptibility and HIV testing intention. In addition, the self-reported measures lead to potential recall and social desirability bias. An additional limitation is the measurement of perceived susceptibility and HIV testing intention. Both constructs were measured by a single item that had relatively few Likert-type response options. Future research should expand construct coverage when measuring perceived susceptibility and HIV testing intention, consider a longitudinal measure of receiving an HIV test, and increase the sample size of the sexual minority population.
Implications for Health Promotion Practice and Research
Our results indicate that heterosexual college students who hold stigmatizing beliefs about HIV have lower HIV testing intention compared with their peers with the same level of perceived susceptibility but fewer stigmatizing beliefs. Our results underscore the importance of audience segmentation in health communication and social marketing campaigns. Specifically, our findings point to the importance of tailoring HIV testing campaigns to meet the unique perceived psychosocial barriers of the priority population—in this case, addressing HIV-related stigma among heterosexual college students. Furthermore, these results have implications for clinical care. Among college students using university health centers, sexual minority college students may be more likely to experience discrimination and stigma stemming from their sexual minority status (e.g., Reeves et al., 2021). Reducing these negative clinical experiences is crucial to further promote patient engagement in sexual health services, particularly for individuals who may not self-identify as a sexual minority but may be engaging in same-sex intercourse.
Our study also introduces several new questions to extend research in health behavior theory and HIV testing service utilization. First, there is limited research on the role of stigma within the HBM. Addressing this gap in the literature should be of central focus to further advance and refine health behavior theory. In addition, one interest of the present study was to consider differences across sexual orientation and across gender groups. Due to the small sample size of the sexual minority group in our study, this was not possible; however, it is conceivable that there are differential effects of HIV-related stigma across sexual orientation and gender categories (e.g., lesbian women, straight men, etc.), which merit further research.
Footnotes
Authors’ Note:
This study was funded by the University Scholars Program, Center for Undergraduate Research, at the University of Florida awarded to Tyler G. James and Sadie J. Ryan.
Author Contributions
Alyssa Berger: Conceptualization, methodology, writing—original draft, writing—review and editing. Tyler G. James: Conceptualization, methodology, formal analysis, investigation, writing—original draft, writing—review and editing, funding acquisition. Sadie J. Ryan: Methodology, investigation, resources, writing—review and editing, supervision, funding acquisition.