
Abstract
Some patients experience negative interactions with health care providers, such as when they perceive that their concerns are ignored by providers. The present study, guided by patient-centered communication, examined health care provider communication behaviors that resulted in patients feeling dismissed, and whether there were differences in providers who dismissed being perceived as (dis)similar to the patients in gender, race/ethnicity, or age. U.S. adults claiming they felt dismissed by a provider were asked to recall demographic information they perceived about the provider and what the provider said that was dismissive. Responses were coded for emergent themes. Results revealed that younger, female, and non-White participants most frequently reported being dismissed by a dissimilar provider. Patients felt dismissed when they perceived that providers were rude or did not take action, provided poor information, did not believe patients, rushed the visit, or were uninformed. Providers may want to avoid these behaviors and could consider obtaining training in supportive communication behaviors such as providing validation to patients and listening to patients in order to enhance patient satisfaction. Patients can also receive communication training to take a more active role in their medical encounters by learning to effectively ask questions, express preferences, and speak up for themselves.
In the media, some recent attention is being paid to patients feeling dismissed by health care providers. NBC Today’s (2020) “Dismissed” is a series wherein women share stories in which they felt their health issues were not taken seriously by providers. Today (2019) also conducted a survey with a national sample of almost 4,000 U.S. adults with chronic health conditions and discovered that 26% of women and 18% of men surveyed perceived that their symptoms were ignored by a health care provider. Similarly, the National Pain Report (Anson, 2014), which evaluated perceptions of interactions with health care providers among women with chronic pain, indicated that 45% of participants expressed that a doctor had told them that they were imagining their pain.
Patients perceiving that they were dismissed by a health care provider can result in negative outcomes. First, some errors in diagnosis are a result of physicians ignoring information patients provide, not listening to patients, and not taking patients’ concerns seriously (Giardina et al., 2018). Second, patients may experience distress, anger, anxiety, or uncertainty, and decide to treat their health conditions on their own if providers do not validate their experiences (Braeuninger-Weimer et al., 2019; Street et al., 2018). Providers dismissing patients can also result in decreased continuity of care because patients visit other providers for a second opinion when they feel dismissed (Braeuninger-Weimer et al., 2019). Visiting multiple providers can result in expensive, needless tests (Burke, 2019). Continuity of care is important because it results in fewer visits to the hospital and fewer expenses (Bazemore et al., 2018). Thus, it is important for providers to communicate in a way that will promote continuity of care with their patients.
The present study, utilizing patient-centered communication (PCC) as a framework, sought to understand what providers say and do that is perceived by U.S. adult patients as being dismissive. Such research could provide an understanding of specific communication behaviors providers should avoid when interacting with patients, which could inform clinician communication training and promote health equity. When providers engage in equity-focused health care in a primary care context, this can increase patients’ confidence in their health care and abilities to take care of their health, which results in improved health outcomes (Ford-Gilboe et al., 2018).
Patient-Centered Communication
PCC is a framework that helps describe interaction between health care providers and patients; takes the beliefs, attitudes, and needs of individual patients into account; and emphasizes patients’ perspectives when engaging in health-related decision making (Institute of Medicine, 2001). PCC has several components, including obtaining the patient’s viewpoint, exchanging information, attending to the patient’s emotions (Epstein & Street, 2007), and ensuring patients understand health information (Epstein et al., 2005). Specific provider communication behaviors that demonstrate PCC include reassuring or encouraging patients, as well as nonverbal behaviors such as maintaining eye contact, leaning forward, and nodding (Epstein & Street, 2007). PCC is important because it is associated with positive outcomes, including increased patient satisfaction, recall, and treatment adherence (King & Hoppe, 2013). PCC is also associated with less patient anxiety and greater trust in physicians (Zwingmann et al., 2017). Patients desire PCC when interacting with providers by wanting their providers to consider patients’ ideas, explain things in an easy to understand manner, and generate a positive relationship with patients (King & Hoppe, 2013). When providers do not acknowledge patients’ perspectives, patients likely feel dismissed.
Patients Feeling Dismissed by Providers
If patients feel dismissed by their providers, this might indicate these providers are not communicating in ways that align with PCC. For instance, physicians sometimes tell patients that illnesses are “all in their heads” if the providers do not know what is wrong, causing them to feel dismissed and distressed (Burke, 2019). Cancer survivors who experienced a lack of PCC with providers also indicated this perception was a result of providers not giving them information they desired, not listening, or not attending to patients’ concerns and/or emotions (Street et al., 2018). These behaviors demonstrating a lack of PCC are similar to provider behaviors mentioned among patients with particular health issues who reported feeling dismissed.
Provider Dissimilarity and Dismissal
Patients may have increased perceptions of dismissal from providers if they are different from their providers or have certain characteristics. The National Pain Report (Anson, 2014) indicates that 65% of participants believed that physicians gave their pain less attention because of being female. Similarly, Today’s (2019) poll indicated that 31% of women with chronic conditions compared with only 19% of men surveyed perceived they had to provide evidence for their symptoms to a medical professional. Younger women tended to report feeling most dismissed, with 49% of women aged 18 to 24 years perceiving that they had to provide evidence for their symptoms (Today, 2019). Additionally, some racial and ethnic minorities experience racism in encounters with providers (Gonzalez et al., 2018). Racism could be operating through implicit bias, in which providers unconsciously allow negative attitudes toward groups of individuals to harm their interactions with those individuals (Hall et al., 2015). A systematic review of 15 studies reported that implicit bias is common among health care providers and can be problematic because it can result in negative clinician–patient communication and negative mental health outcomes among patients (Hall et al., 2015). For instance, when non-Black oncologists had higher implicit racial bias, observers and Black patients perceived them to demonstrate less encouraging communication and less PCC (Penner et al., 2016). Findings from previous literature suggest that patients may be more likely to report feeling dismissed by providers who are demographically different from them.
Health Care Provider Dismissive Communication
Many patients report feeling dismissed by providers, expressing particular provider communication behaviors that the patients perceived negatively. For instance, among women experiencing pain during sexual intercourse, many felt invalidated by health care providers (Braksmajer, 2018), while some patients with nonepileptic seizures experienced providers blaming and stigmatizing them (Robson & Lian, 2017). Among patients with chronic pain, many felt their providers did not want to discuss pain, felt they did not have enough time with the providers, or felt stereotyped by the providers (Bergman et al., 2013). For individuals from Norway with medically unexplained symptoms, they perceived that providers disregarded their perspectives, tried to attribute their symptoms to psychological causes, or provided poor suggestions (Lian & Robson, 2017). Among patients with a neuroimmune condition and chronic fatigue syndrome, almost 90% reported feeling dismissed by a health care provider, with providers giving inappropriate causes and treatments for the health issue, not believing patients, not adequately understanding the health issue, or being insensitive (McManimen et al., 2019).
Previous research tends to investigate patients feeling dismissed by clinicians within the context of one singular and specific health issue at a time, or with one type of provider at a time (i.e., physicians). There is little research on patients with different types of health issues or symptoms that more globally explores feeling dismissed by health care providers. Therefore, this study seeks to understand the experiences of U.S. adult patients with a multitude of health issues feeling dismissed, in order to determine whether there are patterns of dismissal behaviors among a wider range of health care providers and patients. We hypothesized that a greater percentage of individuals with a provider who is perceived as dissimilar to them in gender, age, or race/ethnicity will perceive that they have been dismissed than individuals with a provider who is perceived as similar to them. We also asked what health care providers say and do that is perceived by patients as being dismissive.
Method
An online survey approved by the university’s institutional review board was distributed on Amazon Mechanical Turk in Fall 2019. The main purpose of the survey was to conduct an experiment to analyze participant responses to doctor communication. However, additional items were added to the end of the survey to test this study’s hypothesis and research question.
Survey Questions
To answer our hypothesis and research question, participants were asked if they ever felt they had a health problem that was dismissed or ignored by a health care provider, with response options of “Yes” or “No.” For participants who answered “Yes,” they were asked to indicate whether they perceived that the provider was the same or different gender and race/ethnicity as them, and whether the provider was perceived as younger, around the same age, or older. They were also asked to describe what the health care provider said and what happened within the dismissal interaction.
Open-Ended Data Analysis
A coding scheme was developed to analyze the open-ended responses using a thematic analysis approach (Braun & Clarke, 2006). The first author (GH) identified themes that emerged from the responses and developed a coding scheme. Then the first author trained a coauthor (RR) in how to use the coding scheme. The coders conducted four rounds of training with 50 responses each, and then they coded the rest of the responses. Intercoder reliability for the final round of coding was adequate among the five categories (κ ≥ .68; 85%–97% agreement; however, for the “Uninformed” category—95% agreement—only the percent agreement is reported because the code occurred so infrequently). The coders met to resolve all disagreements after all rounds of coding until 100% agreement was obtained.
Results
Participants
Data were obtained from U.S. adult participants recruited from Amazon Mechanical Turk. Participants were paid 75 cents for completing the survey. A total of 2,027 responses were collected. However, responses were removed if they were duplicates based on IP (internet protocol) address (n = 93), had more than half missing data (n = 45), or failed an attention check (n = 174). This left 1,715 responses. Among these participants, over half of them indicated that they had a health problem dismissed by a health care provider (51.5%; n = 882). Among participants indicating that they had been dismissed, 871 completed the open-ended question asking what the provider said or did that was perceived as dismissive. Seventy-four responses were removed due to being irrelevant (e.g., “Health problem” or “Yes”). The 797 remaining relevant responses were coded.
Among participants whose open-ended responses were analyzed, 69.2% identified as female (n = 550), 29.6% as male (n = 235), 0.8% as transgender (n = 6), and the rest stated “Other” or preferred not to respond. Participants ranged in age from 18 to 83 years (M = 38.74 years, SD = 12.64). A majority of respondents classified themselves as White (79.5%, n = 632), followed by African American (6.8%, n = 54), Asian (6.7%, n = 53), Hispanic (4.4%, n = 35), Native American (0.4%, n = 3), or selected Other (2.2%, n = 18). Regarding education level, 0.6% of participants did not complete high school (n = 5), 23.6% completed high school/GED (n = 188), 20.2% had a 2-year college degree (n = 161), 38.2% had a 4-year college degree (n = 304), and 17.3% had an advanced college degree (n = 138).
Dismissal From Providers Perceived as Demographically Different
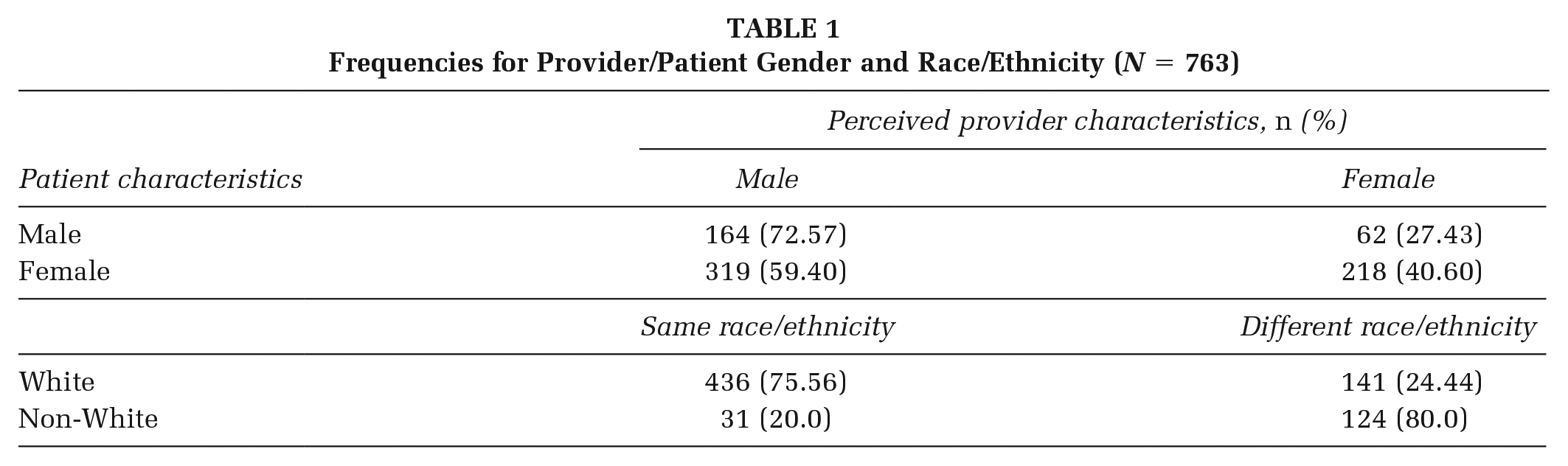
The hypothesis predicted that more participants would report being dismissed from providers who were perceived as demographically different from them (gender, race/ethnicity, and age) than similar. A two-way chi-square was conducted for gender (male or female patient, male or female provider). Results indicated a significant effect: χ2(1) = 65.03, p < .001, Φ = .29 (see Table 1). More female participants perceived they were dismissed by a male provider (59.40%, n = 319 out of 537) than male participants perceived they were dismissed by a female provider (27.43%, n = 62 out of 226). For age, a one-way chi-square was conducted (provider was older, same age, or younger). There was a significant effect: χ2(2) = 425.87, p < .001; 67.76% of participants (n = 538) perceived they were dismissed by a provider who was older than them, 18.39% by someone near the same age (n = 146), and 13.85% by a provider who was younger (n = 110). For race/ethnicity, a two-way chi-square was conducted (White or non-White patient, provider same or different race/ethnicity). There was also a significant effect: χ2(1) = 163.32, p < .001, Φ = .47; 24.44% (n = 141 out of 577) of White participants perceived they were dismissed by a provider of a different race/ethnicity, while 80.0% (n = 124 out of 155) of non-White participants perceived they were dismissed by a provider of a different race/ethnicity. The hypothesis was supported for younger, female, and non-White participants.
Frequencies for Provider/Patient Gender and Race/Ethnicity (N = 763)
Providers’ Dismissive Communication Messages
The research question asked what participants perceived providers said or did that was dismissive. Five themes emerged from the responses (see Table 2).
Themes for Patients Feeling Dismissed by Health Care Providers (N = 797)

Note. MCL = medial collateral ligament; ER = emergency room.
Inappropriate/Lack of Response
The most common theme among participants (59.72%) was perceiving that a provider displayed inappropriate behavior such as being rude, condescending, or laughing at the patient. For instance, “They scoffed and mocked me when I described the problem. I never went back.” This theme also included patients perceiving that providers were not listening. A sample comment included, “She was distracted looking at her laptop, not looking at me.” Finally, some patients perceived providers were not doing enough to address the health issue. For example, “The doctor was unwilling to order a test that I considered necessary to rule out, based on my symptoms.”
Bad Information
Many participants perceived that a provider gave poor diagnosis or treatment information (57.97%). Example comments were “The health care provider said that I was most likely feeling dizzy because of how tall I am, which sounds improbable”; “When I told my doctor that my heart was beating irregularly, my doctor insisted that my symptoms were definitely from anxiety”; and “They just give me aspirin and tell me to sleep a lot.”
Do Not Believe
Some respondents felt as though a provider did not believe that they had anything wrong or denied that they had a particular health issue (15.81%). For instance, “They dismissed my walking pneumonia as me being a hypochondriac.” This theme also included patients perceiving providers thought that they were faking or exaggerating their symptoms or that they wanted something. For example: “The nurse thought I was drug seeking and faking pain.”
Time
A less frequently occurring theme mentioned by some of the participants was that a provider did not spend enough time with them, was rushing the appointment, or limited the number of health issues discussed (7.03%). Comments representing this theme included, “When I started to tell her some of my problems she said she could only deal with a couple of my problems today” and “When I was pregnant, the OB always asked if I had any questions as his hand was on the doorknob to leave.”
Uninformed
Finally, a perception that a provider did not know what was wrong, did not know what they were doing, or could not do anything to help was mentioned by several participants (5.14%). Example responses representing this theme included, “Idiot doctor” and “They had never heard of a particular symptom I was having.”
Discussion
Our findings indicate that many participants experienced feeling dismissed by a health care provider. While previous research has examined patients’ recollections of providers’ dismissive messages among patients with the same health issue (Bergman et al., 2013; Braksmajer, 2018; Lian & Robson, 2017; McManimen et al., 2019; Robson & Lian, 2017), the present study sought to include a variety of health issues and patients across a general population sample. For those participants who felt dismissed, a greater percentage of participants who were younger (67.76%), female (59.40%), and non-White (80%) perceived they were dismissed by a dissimilar provider than older (13.85%), male (27.43%), or White (24.44%) participants. Some of these participants may have experienced implicit bias from their providers, as it is associated with a lower quality of care based on race/ethnicity, gender, socioeconomic status, age, or other characteristics (FitzGerald & Hurst, 2017). To combat implicit bias, providers can equally acknowledge their patients, be respectful, and work to establish rapport with all patients (Gonzalez et al., 2018). Marcelin et al. (2019) suggest that health care providers reflect on stereotypes and biases they may have and consider how these stereotypes and biases could affect interaction with individual patients before interacting with them; then, they can make a conscious effort to avoid any potential negative behaviors. Providers consciously making an effort to improve communication with every patient aligns with health equity and could promote health among all patients.
Provider Dismissal Behaviors
Patients with a variety of health issues tended to experience similar feelings of dismissal from providers. Specifically, they felt certain providers were insensitive, did not listen, did not take action, provided poor information, did not believe them, rushed the interaction, or were uninformed. Previous research indicates similar results among particular patients. For instance, patients in the United Kingdom who complained about interactions with doctors indicated that the doctors did not adequately maintain eye contact, did not listen, or were rude (Kee et al., 2018). Patients with an autoimmune disease and chronic fatigue syndrome felt some providers gave inappropriate causes and treatments for health issues, did not believe them, had a lack of knowledge, or were tactless (McManimen et al., 2019). Finally, patients with chronic pain did not appreciate when their primary care providers rushed the interaction (Bergman et al., 2013).
Implications for Practice: Positive Communication Behaviors
To combat the issue of patients feeling dismissed, providers can attempt to avoid the behaviors patients perceive as dismissive and engage in positive communication behaviors. One idea is to provide clear justification to patients for why providers are making decisions. Another strategy is for providers to validate their patients, which may enhance provider–patient interaction and patient satisfaction (Edmond & Keefe, 2015). Providers can also engage in active listening when interacting with patients. For instance, patients with chronic musculoskeletal low back pain want their health care providers to listen to them (Braeuninger-Weimer et al., 2019). In addition, providers can enhance their PCC skills, since PCC emphasizes providers considering patients’ emotions, perceptions, and desires regarding their health issues (Hashim, 2017). Providers should be trained to engage in supportive communication behaviors to improve their communication skills. Medical school faculty or communication scholars could train medical students by incorporating effective communication strategies into the medical school curriculum. One idea is to train providers in reflexivity, such that they consider their communication when interacting with patients who are different from them, and make adjustments if needed, in order to address potential implicit bias (Alexander et al., 2020).
In addition to enhancing provider communication, patients can also be trained in how to effectively communicate with health care providers. Patients could be trained by local researchers and/or health care providers who could design research projects grounded in health promotion. They could obtain funding specifically for creating communication training for patients within a particular community, which would allow for a targeted approach. Relevant PCC behaviors for patients include patients asking questions about diagnosis or treatment information (Epstein & Street, 2007) or mentioning a treatment preference (Robinson et al., 2013). Patients could also be trained to speak up for themselves if they perceive that they are being dismissed. For instance, SpeakENDO (2020), a campaign for endometriosis, encourages patients to openly discuss their pain when meeting with gynecologists to convince them to take their pain seriously.
Limitations and Implications for Future Research
Because participants were asked to recall information that happened in the past, it is possible some of the participants did not accurately recall all of the details of the interactions in which they felt dismissed. Relatedly, while participants were asked to speculate the biological sex, race/ethnicity, and age of the health care providers, the participants could not know this demographic information with certainty. Our sample was fairly young, female, and White, so the results may not be generalizable to other individuals. Therefore, future studies could utilize a more diverse sample to better explore racial/ethnic differences. Additionally, we only obtained the patients’ perspectives on the interactions, and not the perspectives of the health care providers. Future research could evaluate the providers’ viewpoints on interactions in which patients felt dismissed. Because the data were collected using a survey, the researchers could not use probing questions to obtain more details on the interactions. Other studies could utilize interviews and/or focus groups to gain a more in-depth understanding of these interactions. Future studies could also examine results based on the types of health issues participants described, to see if there are any patterns that arise. Finally, an experiment could be conducted to determine whether patients perceive types of dismissal as an expectancy violation or not.
Conclusion
Just over half of the participants surveyed in this research indicated they felt dismissed by a health care provider at some point in the past. Among those who felt dismissed, a majority perceived that providers communicated inappropriately and/or provided bad information during the interaction. Findings from this study could be useful to guide communication training for providers in terms of communication behaviors they should try to avoid when interacting with patients. As well as avoiding dismissal behaviors, providers can be trained in supportive communication behaviors such as listening, validating, and providing clear explanations. Patients can also be trained in PCC skills such as mentioning preferences related to treatment. By encouraging providers to engage in supportive communication behaviors, this may promote a positive provider–patient relationship, health equity, continuity of care, and patients’ health.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.