
Abstract
Background. Chronic stress and depression disproportionately affect families experiencing poverty, and likely contribute to disparities in early childhood developmental outcomes. Developing strategies to address chronic stress and depression may help mitigate these disparities. Early Head Start (EHS) and Head Start (HS) programs provide an important platform to address the disproportionate burden of stress and mental health issues experienced by EHS/HS families. However, few low-literacy, broad, scalable interventions improve parents’ knowledge and attitudes around these topics. Objectives. We examined parents’ knowledge and attitudes regarding stress and depression before and after a train-the-trainer (TTT) intervention delivered to 28 EHS/HS agencies across the United States. Methods. Following a TTT workshop, 18 agencies chose to deliver the stress training to 1,089 parents and 5 chose to deliver the depression training to 670 parents. Participating parents completed paper assessments at baseline and 3 months following the training. Paired T-tests and chi-square analyses tested whether responses significantly improved over time. Results. At baseline, 37.2% of parents reported feeling stressed most of the time and 13.4% reported feeling depressed most of the time. Following the trainings and reinforcement activities, parents’ knowledge, attitudes and self-reported behaviors significantly improved, including willingness to seek help for depression, avoidance of negative health-risk behaviors and utilization of healthy stress management practices. At follow up, 18.6% of parents reported feeling stressed most of the time and 11% reported feeling depressed. Conclusion. Findings suggest this low-literacy TTT approach is potentially a promising health promotion intervention with broad dissemination potential.
Keywords
Chronic stress is highly prevalent among Americans, impacting one in two adults in the United States (US) (Halonen et al., 2020), and is thought to be one of the root causes of mental health problems, including depression (Stefanaki et al., 2018). The high prevalence of chronic stress and depression has important social, economic, and health implications for affected individuals and their families (Bermudez-Millan et al., 2016; Dalton et al., 2016; Snow & Abrams, 2016). Untreated depression can lead to lower educational attainment, unemployment, high work absenteeism and disability, increased risk of substance abuse and teen pregnancy, and high mental and medical care costs. (Chow et al., 2019; Konig et al., 2019). High levels of stress and depressive symptoms among adults with children also have indirect societal, economic, educational, and health costs. Parental depression may adversely impact child development and health through harsh parenting, child abuse and neglect, and parent-child attachment problems that can lead to poor cognitive and social-emotional development, behavioral problems, poor sleep, obesity, and later adult onset of poor health, unemployment, poverty, and increased risk of criminal justice involvement. (Baker et al., 2020; Beeber et al., 2014; Cherry et al., 2019; Erickson et al., 2019).
The direct and indirect impacts of stress and depression likely contribute to their disproportionate prevalence among individuals and families experiencing poverty. Studies estimate that up to 50% of low-income mothers experience depressive symptoms compared to 10% to 30% of mothers in the general population which may further exacerbate disparities in parental and child health (Justice et al., 2019; Li et al., 2017; Palmer Molina et al., 2020). The possibility for households to be affected by both poverty and adult depression, and the associated direct and indirect (i.e., child) costs, make it imperative to address the management and prevention of depression among low-income households with children. Strategies to address chronic stress and depression among parents of young children living in low-income communities may help mitigate these disparities.
Several key safety-net federal programs such as Early Head Start (EHS) and Head Start (HS) are specifically focused on supporting families with young children to mitigate the negative health and developmental consequences of early adversity. EHS/HS programs provide early childhood educational interventions and comprehensive services for both the child and parent such as parenting support and community resources for food, job training, housing, and continuing education. The majority of EHS/HS children reside in households with a single parent and experience food insecurity, unemployment, and economic hardship (Administration for Children and Families, 2015). Not surprisingly, issues of chronic parental stress and depression are highly prevalent among EHS/HS families (Arlinghaus et al., 2020; Hustedt et al., 2017). Studies indicate that up to one in two mothers whose children attend either EHS or HS experience significant levels of depressive symptoms (Administration for Children and Families, 2015; Baker, 2018; Silverstein et al., 2017).
As a trusted community program and resource broker for low-income families with young children, EHS/HS programs provide an important platform and opportunity to be highly responsive to the disproportionate burden of stress and mental health issues experienced by EHS/HS families (Small, 2006; Small & Gose, 2020; Wesson & Kitzman, 2018). EHS/HS agencies thus have the opportunity to support a public health primary prevention approach to address parent stress and mental health. There are, however, few low-literacy, broad, scalable interventions to improve parents’ knowledge, attitudes, and behaviors around these topics. The Health Care Institute (HCI), housed at the UCLA Anderson School of Management, in collaboration with the National Center for Early Childhood Health and Wellness, used a train-the-trainer (TTT) approach to train over 1,500 front line staff from Early Head Start (EHS) and Head Start (HS) programs across 29 agencies, as well as parent participants in trainings conducted at their sites, on parent stress and depression behavioral prevention and management.
Purpose
This paper describes the TTT training and its impact on parent knowledge, attitudes, and self-reported self-care behaviors related to stress and depression.
Methods
Program Description
The Health Care Institute (HCI) has used a strategic and systematic approach to deliver health promotion training programs for EHS/HS agencies across the United States (Dudovitz et al., 2020; Herman et al., 2012, 2013). Their approach focuses on leadership skills, enhancing management and workforce capacity, and implementation strategies for EHS/HS agencies to work effectively with parents, staff, and community stakeholders on various health promoting topics. Trainings focus on core areas that address common childhood health conditions. Previous evaluations of oral health and nutrition and physical activity trainings demonstrated improvements in parental knowledge, attitudes, self-reported health behaviors, and health outcomes (Dudovitz et al., 2020; Herman et al., 2012). In 2019, the HCI developed and conducted trainings focused on stress management and depression.
Through a national application process, 28 EHS/HS agencies were selected to engage in a 4-year working relationship with the HCI that focused on supporting family engagement and health promotion at their respective sites. Each year, a team from each selected EHS/HS agency was invited to attend a 2-day train-the-trainer (TTT) event, supported by the HCI. The goals of event were to build specific knowledge and skills so that each agency could: (a) develop a coordinated and strategic plan to disseminate a health promotion topic; (b) learn and apply implementation strategies to support buy-in and engagement of staff, parents, children, and community stakeholders around a specific health topic; (c) learn and apply adult learning principles and delivery techniques to teach a specific health topic; and (d) deliver consistent content around a specific health topic to staff and parents.
Goals of Program
During these trainings, a systematic approach was used to build leadership and workforce capacity using a TTT model to support health promotion around four highly relevant child health topics. Sessions during this two-day training included the following: (a) strategies to increase motivation and buy-in of staff and parents; (b) a roadmap to guide their goals and action steps; (c) a budget plan; and (d) modeling a mock session using power point slides, handouts, and examples of hands-on-activities demonstrating firsthand how the HCI strategies and materials could be used to effectively implement parent training programs at their respective agencies. In the third year, all agencies completed a virtual on-line TTT event to build workforce capacity around four mental health topics including the following: (a) “Early Childhood Trauma and Adversity,” (b) “Understanding Stress,” (c) “Positive Discipline,” and (d) “Understanding Depression.” Each agency selected two topics for their parent training programs.
As seen in Figure 1, in early March of 2019, five virtual webinars of 90-minutes duration were held following the same approach used in the in-person two-day TTT events in prior years. The first webinar training focused on trauma with staff and parents as the intended audience, and the subsequent three webinars focused on stress, positive discipline, and depression with only parents as the intended audience.
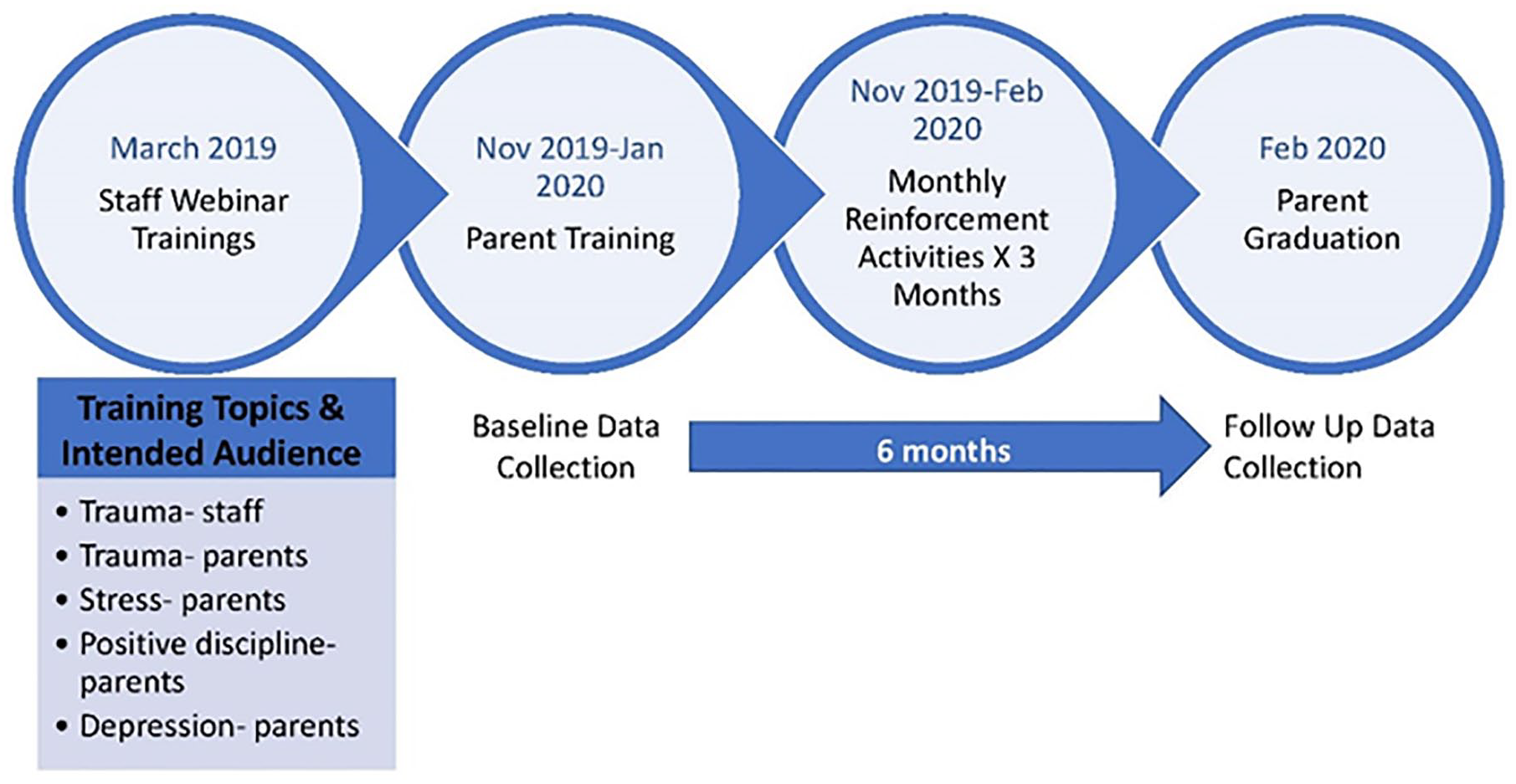
Timeline for Implementation and Data Collection
Train-the-Trainer Approach and Strategies
The EHS/HS agencies were provided with strategies and resources to train with consistency and high fidelity to content and messages. This was accomplished by: (a) using low literacy, “ready-to-use” annotated slides; (b) providing a four-page brochure; and (c) providing tip sheets that covered core topics related to stress and depression. Example brochures related to stress and depression can be found in the Supplemental Content. Low-literacy content and materials were developed by Georgetown University’s Center for Child and Human Development (GUCCHD) in partnership with the HCI and the National Center on Early Childhood Health and Wellness (NCECHW). The tip sheets that were provided during the training focused on (a) sources of stress and depression, (b) identifying the signs and symptoms of stress and depression, and (c) learning practical strategies to reduce stress.
Trainer Dissemination
Using the provided slides, brochures, and handouts, each EHS/HS team was then expected to conduct a 90-minute training for at least 50 parents from their respective site. Each agency had the flexibility to determine when the trainings would be delivered and what reinforcement activities would be used for parents. EHS/HS teams, however, were asked to conduct at least three home visits to reinforce the training content, using the tip sheets. Flexibility on the implementation strategies was intentional in order for each agency to best meet their local needs and cultures while aligning the training activities with required federal performance standards.
Each team trained their parents during the months of November 2019—January 2020. Activities to reinforce the training content spanned an average of 3 months from November 2019-February 2020. This study was determined to be exempt by the UCLA Institutional Review Board.
Data Collection
Baseline assessment of knowledge, attitudes, and self-reported self-care behaviors was completed immediately before the parent training and repeated 3-months after the training via a paper survey. Parent surveys were developed to measure knowledge, attitudes, and self-care practices. The content of the parent surveys was co-developed by GUCCHD and the HCI with attempts to keep all items no higher than a 6th-grade reading level. Participant names were used to link baseline to follow-up surveys.
Measures
EHS/HS Parent Knowledge, Attitudes, and Self-Care Practices Related to Stress
Three items assessed knowledge about stress. Parents were asked to select answers regarding the definition of, possible causes of, and symptoms of stress. To assess the definition of stress, parents were asked, “What is stress?” and asked to mark “All That Apply” from a list of four possible responses which included, “Bad things that happen in your life,” “Exciting things that have happened in your life” “Challenges in life” and “Physical or emotional responses to demands or pressures.” The number of listed items marked off was summed to determine a knowledge score related to defining stress and ranged from 0 to 4. Parents were then asked to identify common causes of stress and could mark “All That Apply” from a list of nine answers such as life demands, pressures, or events like illness, parenting, and financial stress. Knowledge scores related to causes of stress ranged from 0 to 9. Finally, parents were asked to mark “All That Apply” from a list of eight symptoms of stress, such as memory problems, difficulty sleeping, anger, and overuse of drugs and alcohol. A knowledge score related to symptoms of stress ranged from 0 to 8.
Assessment of parental attitudes about stress was measured using a Likert-type response option to four statements. Parents were asked, “What can you do to reduce stress in your life” with four response categories: “nothing,” “a little,” “a fair amount,” and “a lot.” This item was given a score of 1 to 4 with higher scores indicating a greater perceived ability to reduce life stress. Parents were also asked to indicate the degree to which they agreed or disagreed with three statements: “I know that taking care of myself and reducing my stress can help my children,” “I am able to recognize when I am experiencing stress,” and “I am aware of the symptoms of stress.” Parents were presented with three response categories: “Agree,” “Somewhat Agree,” and “Disagree,” and each item was given a score of 1 to 3 with higher scores indicating stronger agreement.
Parental self-care habits were measured using three Likert-type-scale response options to eight statements. Parents indicated whether they never, sometimes, or always engaged in self-care practices such as exercising, eating a healthy diet, noticing their thoughts and feelings, and focusing on breathing. Response range for each statement was 1 to 3 with higher scores indicating more frequent self-care practices. Finally, parents were asked, “How often do you feel stressed out?” Response options were “Most of the time,” “Sometimes,” and “Not very often.” This item was scored 1 to 3 with higher scores indicating greater frequency of feeling stressed.
EHS/HS Parent Knowledge, Attitudes, and Self-Care Practices Related to Depression
Items to assess knowledge about depression included three items. Parents were asked, “What is depression?” and asked to mark “All That Apply” from a list of three responses which included, “A medical illness that causes a constant feeling of sadness or lack of interest,” “Depression affects how a person feels; behaves and thinks” and “Depression is an illness.” Parents were also asked to identify common causes of depression and asked to mark “All That Apply” from a list of seven life events such as, family history, stressful events, and losing a loved one. Finally, to assess knowledge regarding symptoms of depression, parents were asked to mark “All That Apply” from a list of seven symptoms such as decreased interest or pleasure, difficulty sleeping, difficulty concentrating, and feeling tired or low-energy.
Assessment of parental attitudes regarding depression was assessed by asking parents to respond to five statements regarding depression in general (e.g., “I understand the causes of depression.”) and four statements about how to respond to depressive symptoms (e.g., “If I felt depressed I would ask a friend for help.”) Participants selected from three response categories: agree, somewhat agree, and disagree. Each item was scored 1 to 3 with higher scores indicating stronger agreement. In addition, parents were asked “What can you do to reduce depression in your life?” with four response categories: “Nothing” “A little,” “A fair amount” and “A lot.” This item was given a score of 1 to 4 with higher scores indicating stronger self-efficacy for reducing depression. Finally, parents were asked to self-report how often they felt depressed with the response options of “most of the time,” “sometimes,” and “not very often.” Response range for this statement was 1 to 3 with higher scores indicating more frequent feelings of depression. Parents also indicated whether they never, sometimes, or always lose their temper, drink, smoke, or use drugs excessively, worry too much, give up on plans or goals, and feel defeated or overwhelmed. Responses for each statement ranged 1 to 3 with higher scores indicating greater frequency.
Data Analysis
Descriptive statistics were generated for all variables. Follow up data were missing from 4 of the 28 agencies either because a participating agency had shut down, moved locations, or had staff turnover. Differences in baseline values were examined for those with and without follow up data. Among those with both baseline and follow up surveys, paired t-tests for variables with continuous outcomes and Chi2 tests for variables with categorical responses were completed to compare differences in baseline and post-training assessments. All analyses were conducted in STATA (version 15, StataCorp).
Results
Staff Satisfaction With the Training
At the conclusion of the training, a satisfaction survey was administered to the EHS/HS staff which showed favorable feedback (89% indicated high satisfaction with the webinars, 86% reported an improvement in knowledge on the subjects, and 91% were satisfied with the content expertise of the presenters).
Parent Stress
Eighteen of the 28 agencies (64%) chose to deliver the stress training to parents. In total, 1,089 parents completed the baseline survey across these 18 agencies, with 854 parents completing both baseline and follow up assessments (78% follow up rate). A comparison of all stress items at baseline between those with and without follow-up data did not show significant differences in knowledge, attitudes, or self-care practices (Table 1).
Stress Training Baseline Statistics for Those With and Without Follow Up-Data
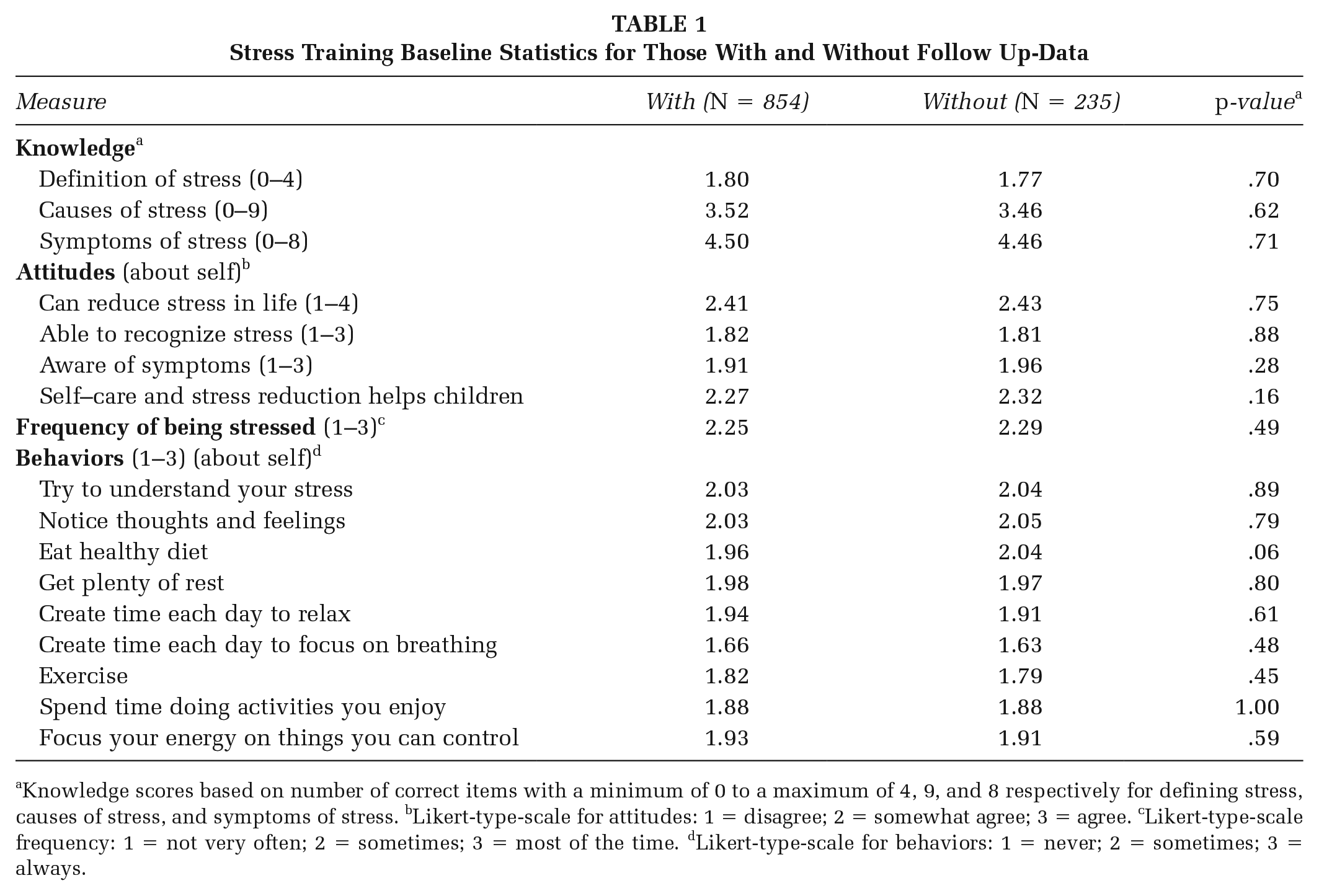
Knowledge scores based on number of correct items with a minimum of 0 to a maximum of 4, 9, and 8 respectively for defining stress, causes of stress, and symptoms of stress. bLikert-type-scale for attitudes: 1 = disagree; 2 = somewhat agree; 3 = agree. cLikert-type-scale frequency: 1 = not very often; 2 = sometimes; 3 = most of the time. dLikert-type-scale for behaviors: 1 = never; 2 = sometimes; 3 = always.
Among parents with both baseline and follow up data (Table 2), at baseline, the vast majority could not correctly define stress, or identify potential causes of stress. Parents scored slightly higher in identifying symptoms of stress at baseline, with an average of five of the eight symptoms of stress correctly identified. In regards to attitudes, parents scored the lowest when asked whether they could recognize when they experience stress. Finally, in regards to self-care habits, parents scored the lowest in creating time each day to focus on breathing, exercising regularly, and spending time doing joyful activities.
Change in Knowledge, Attitudes and Behaviors Regarding Stress From Baseline to Follow Up
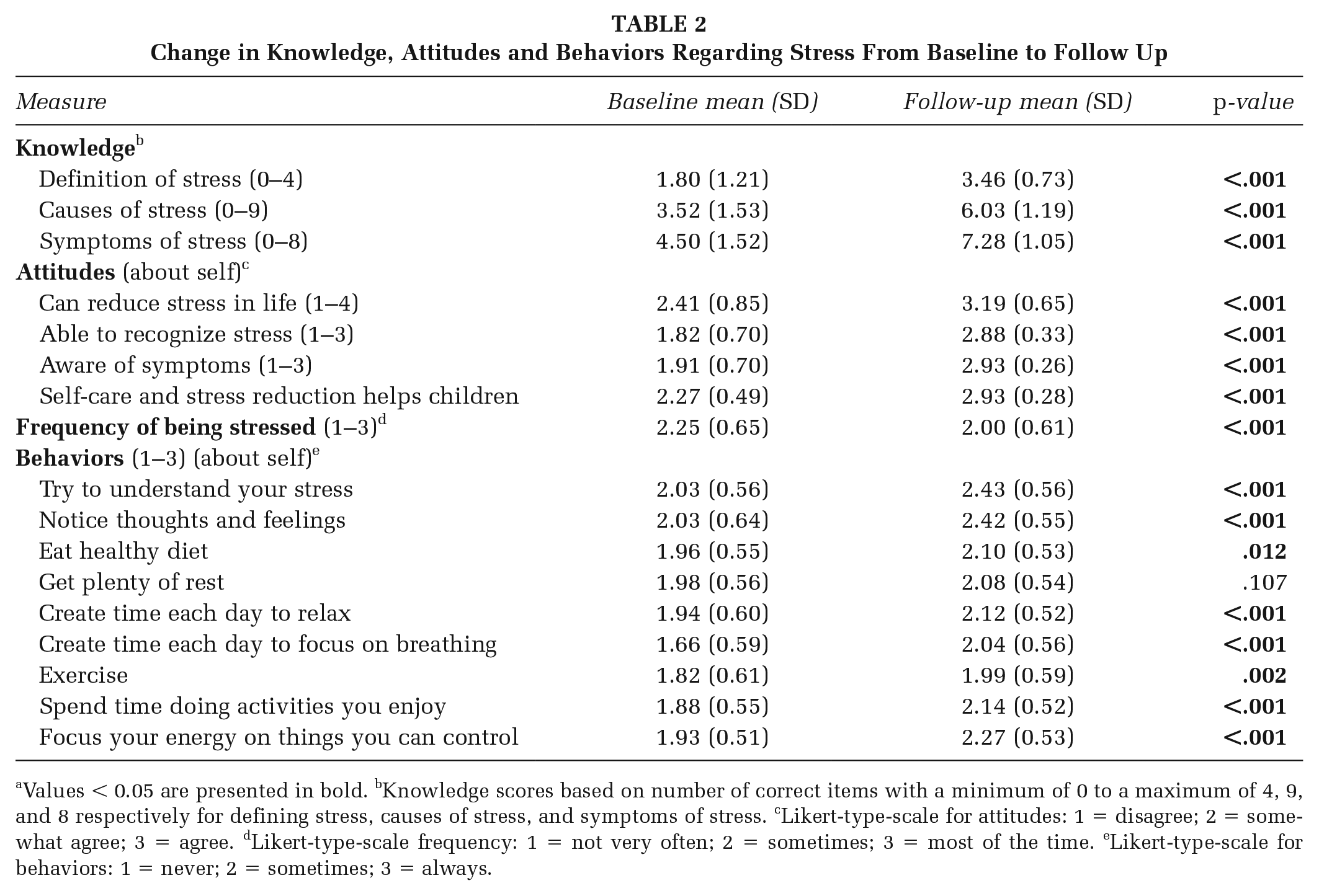
Knowledge scores based on number of correct items with a minimum of 0 to a maximum of 4, 9, and 8 respectively for defining stress, causes of stress, and symptoms of stress. cLikert-type-scale for attitudes: 1 = disagree; 2 = somewhat agree; 3 = agree. dLikert-type-scale frequency: 1 = not very often; 2 = sometimes; 3 = most of the time. eLikert-type-scale for behaviors: 1 = never; 2 = sometimes; 3 = always.
There was a statistically significant improvement in measures at follow up with the exception of getting plenty of rest. Knowledge regarding the definition of stress (M = 1.80, SD = 1.21 at baseline; M = 3.46, SD = 0.73 at follow up, p<.001) and symptoms of stress improved the most (M = 4.50, SD = 1.52 at baseline; M = 7.28, SD = 1.05 at follow up), with smaller but gains noted in parents’ knowledge of causes (M = 3.52, SD = 1.53 vs. M = 6.03, SD = 1.19). Parents had higher attitude scores related to overall self-care habits, with the largest gains among mindfulness habits (M = 2.03, SD = 0.64 vs. M = 2.42, SD = 0.55). Overall, parents reported a decrease in feeling stressed at follow-up compared to baseline (M = 2.0, SD = 0.65, compared to M = 2.25, SD = 0.61, p-value <.001).
Parent Depression
Five of the 28 agencies (18%) chose to deliver the depression training to parents. In total, 670 parents completed the baseline survey across the 5 agencies, with 324 parents completing both baseline and follow up assessments (48% follow-up rate). A comparison of all depression items at baseline between those with and without follow-up data did not show significant differences in knowledge, attitudes, or depressive symptoms (Table 3).
Depression Baseline for Those With Compared to Those Without Follow-Up Data
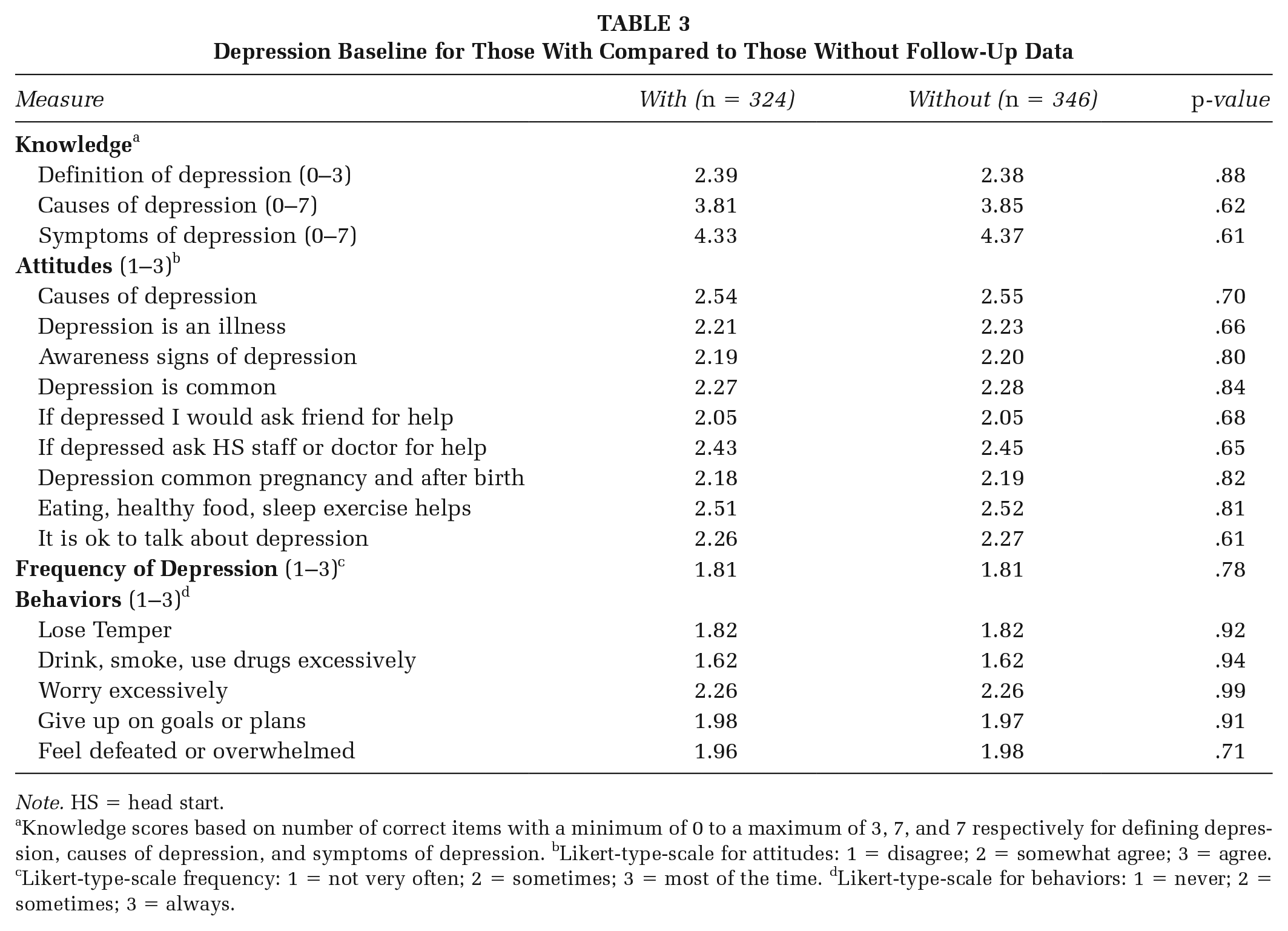
Note. HS = head start.
Knowledge scores based on number of correct items with a minimum of 0 to a maximum of 3, 7, and 7 respectively for defining depression, causes of depression, and symptoms of depression. bLikert-type-scale for attitudes: 1 = disagree; 2 = somewhat agree; 3 = agree. cLikert-type-scale frequency: 1 = not very often; 2 = sometimes; 3 = most of the time. dLikert-type-scale for behaviors: 1 = never; 2 = sometimes; 3 = always.
Among parents with both baseline and follow up data (Table 4), at baseline, most parents could define depression, and parents were able to identify approximately four of the seven potential symptoms of depression. In regards to attitudes, parents reported the strongest agreement when asked whether they understood the causes of depression, and the lowest agreement when asked if depression is common during pregnancy and after birth. Ratings on the frequency of depressive symptoms indicated that 13.4% felt depressed most of the time. In terms of related behaviors, excessive drinking, smoking and using drugs scored the lowest, while worrying too much was the highest rated symptom. When asked about how to respond to depressive symptoms, parents agreed less about whether they would ask a friend for help if they were feeling depressed, and agreed the strongest with eating healthy food, getting enough sleep, and moving around more as a way to feel less depressed.
Change in Knowledge, Attitudes and Behaviors Regarding Depression From Baseline to Follow Up (n = 324)
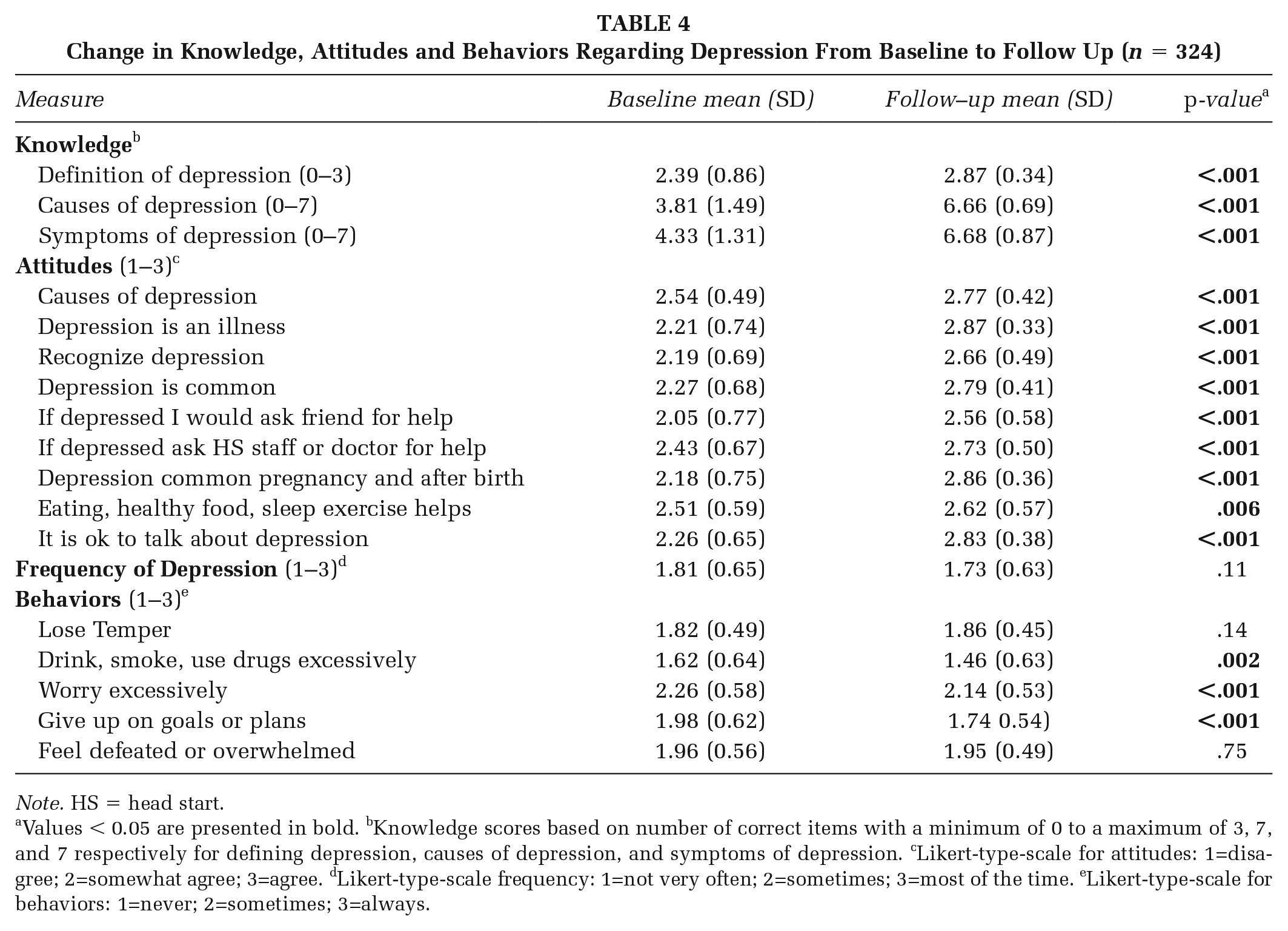
Note. HS = head start.
Knowledge scores based on number of correct items with a minimum of 0 to a maximum of 3, 7, and 7 respectively for defining depression, causes of depression, and symptoms of depression. cLikert-type-scale for attitudes: 1=disagree; 2=somewhat agree; 3=agree. dLikert-type-scale frequency: 1=not very often; 2=sometimes; 3=most of the time. eLikert-type-scale for behaviors: 1=never; 2=sometimes; 3=always.
At follow-up, the definition of depression and knowledge of symptoms and causes of depression all improved significantly. Parents reported lower ratings of drinking, smoking, and using drugs excessively, worrying excessively, and giving up on goals or plans at follow-up compared to baseline. The biggest gain in attitudes about how to respond to depressive symptoms from baseline to follow-up was the degree of parental agreement in asking a friend for help if they felt depressed. Parents did not report a significant decrease in how often they felt depressed at follow-up compared to baseline, with 11% reporting feeling depressed most of the time.
Discussion
We found improved knowledge, attitudes, and self-reported behaviors related to chronic stress and depression among EHS/HS parents from agencies across the United States following this parent training. Knowledge regarding the definitions, causes, and symptoms of stress and depression improved, which may indicate improved health literacy. Notably, in regards to stress, the largest gains were in the reported frequency of using self-care mindfulness strategies, such as noticing thoughts and feelings and creating time each day to focus on breathing. These are low-cost evidence-based coping strategies that may be particularly accessible for low-income families. In regards to depression, the biggest changes were in attitudes related to viewing depression as an illness, understanding depression as a common occurrence during pregnancy and the post-partum period, and reaching out for help if depression was experienced. Given that stigma is a key barrier to accessing depression-related care, these attitudes may serve to support depression care (Henderson et al., 2013). Collectively, these results indicate a promising intervention to impact knowledge and attitudes about stress, a common precursor to depression, and depression itself, which is a critical step in improving help-seeking and accessing mental health services. Furthermore, the use of a TTT approach to deliver the intervention to a wide range of parents from diverse EHS/HS agencies suggests that this approach is scalable.
Improved awareness and attitudes related to depression and reported increase of self-care mindfulness strategies indicate the intervention shows promise as an important component of a depression primary prevention strategy, by potentially reducing risk factors for depression and preventing the onset of disease (Compton & Shim, 2020). Preventing parental depression may also potentially prevent the wide-range effects parental depression can have on children’s physical health (i.e., underweight), attachment, and child development, including the cognitive and socio-emotional domains that may predispose children to poor behavioral and mental health outcomes (Stein et al., 2018).
Limitations
This study is limited by the use of self-report data, which could lead to recall and social-desirability bias. For example, parents may have been reluctant to report behaviors, such as excessive drug use, drinking, and smoking, given that surveys were collected by agency staff and were not anonymous. Parents may also have been motivated to report answers that they perceived as “correct” regardless of whether they accurately reflected their attitudes and behaviors. However, the substantial increase in parents’ ability to, at the very least, identify and select the “correct” answers suggests that stress and depression health literacy improved. We did not collect participant demographic data, such as race/ethnicity, and hence, it is unknown whether participating EHS/HS teams and parents are representative of the larger EHS/HS programs in the US or whether results varied across demographic groups. Participating Head Start agencies applied to participate in the family engagement and health promotion training and may therefore be a group of EHS/HS programs that were more motivated to engage with parents on these topics. We are also unable to assess whether changes were sustained long-term, beyond the 3-month follow up period assessed here.
Of note, follow-up survey response rates were low and fell during the COVID 19 pandemic, when many agencies were closed to in-person services, which may have affected the ability of agencies to conduct follow-up reinforcement and assessments. The parents lost to follow up, however, did not differ in baseline assessment of knowledge or attitudes when compared to parents who had both baseline and follow-up assessments completed. The low survey completion rates, particularly for the depression parent training, limited the power to detect significant changes and may have resulted in underestimating the impact of the training on self-reported behaviors and the frequency of depression. In addition, the fact that self-reported symptoms of stress and depression did not increase during this time is encouraging, given the added psychosocial and economic burdens families were likely coping with at the time of follow up data collection.
Implications for Practice
Despite these limitations, our findings have important implications for health promotion. First, our findings suggest that EHS/HS agencies are a promising site for delivering a selective primary preventive intervention for stress and depression to families coping with threats to mental wellness. Using a trusted agency approach for community-level health interventions has been shown to be effective for improving various health outcomes and decreasing health care costs (Wesson & Kitzman, 2018). The trust EHS/HS programs have among communities and families is a critical strength that can facilitate the delivery of interventions to promote mental wellness to diverse parents and communities. EHS/HS agencies serve many parents from groups that have been marginalized and may not have access to low literacy health promotion interventions. Hence, this strategy might help reduce disparities in parent mental health. Given associations between parent stress, depression, and child health, this strategy may also have important spillover effects on reducing disparities in child health and education outcomes (Stein et al., 2018).
Second, using a train-the-trainer approach in partnership with EHS/HS for disseminating health promotion interventions can reach the large number of children and parents in the Head Start programs across the nation. Although several parenting interventions have shown effectiveness in preventing maternal depression by reducing stress and depressive symptoms, they are often lengthy (i.e., 8–12 weeks), have associated costs (i.e., per-child costs greater than one thousand dollars), and rely on professional instructors rather than Head Start staff (i.e., certified and trained parent instructors) (Baydar et al., 2003; Reid et al., 2004; Silverstein et al., 2017). These features can create significant barriers for both parents and agencies to access many existing parenting interventions. Using a train-the-trainer approach can build capacity among EHS/HS staff and teams and have a higher likelihood of both disseminating and sustaining the intervention over time as EHS/HS programs work with “new” children and families as other children age out of the program. Further, the ability to conduct the training virtually, as indicated by the model presented here, enhanced both sustainability and scalability.
In conclusion, using a train-the-trainer model for delivering stress and depression health promotion interventions using a trusted agency approach, such as via EHS/HS programs, has the potential to improve population health for children and families experiencing poverty. Continuing to build upon this work is critical to addressing the high risk of chronic parental stress and depression among EHS/HS families.
Supplemental Material
sj-docx-1-hpp-10.1177_15248399211061132 – Supplemental material for Evaluation of a Health Education Intervention to Improve Parental Knowledge and Attitudes About Chronic Stress and Depression Among Head Start Families
Supplemental material, sj-docx-1-hpp-10.1177_15248399211061132 for Evaluation of a Health Education Intervention to Improve Parental Knowledge and Attitudes About Chronic Stress and Depression Among Head Start Families by Alma D. Guerrero, Ariella Herman, Carol Teutsch and Rebecca Dudovitz in Health Promotion Practice
Supplemental Material
sj-docx-2-hpp-10.1177_15248399211061132 – Supplemental material for Evaluation of a Health Education Intervention to Improve Parental Knowledge and Attitudes About Chronic Stress and Depression Among Head Start Families
Supplemental material, sj-docx-2-hpp-10.1177_15248399211061132 for Evaluation of a Health Education Intervention to Improve Parental Knowledge and Attitudes About Chronic Stress and Depression Among Head Start Families by Alma D. Guerrero, Ariella Herman, Carol Teutsch and Rebecca Dudovitz in Health Promotion Practice
Footnotes
Authors’ Note:
We would like to acknowledge Amy Hunter, Center for Child and Human Development Georgetown University for her help with development of the survey, training materials and handouts. This work was funded by a grant #90HC0005 for the U.S. Department of Health and Human Services, Administration for Children and Families, Office of Head Start, by the National Center on Early Childhood Health and Wellness.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.