
Abstract
In an arts in public health research team, artists may be undervalued as key research collaborators because of the difficulties in skillful integration of experts who possess not only different bodies of knowledge but also different ways of examining and valuing the world. Under the stewardship of two Rhode Island state agencies, an innovative research-driven enterprise, comprising researchers, clinicians, and community artists, was brought together to integrate arts-based interventions into statewide public health policy and practice. Here, we examine our work with the Rhode Island Arts and Health Advisory Group as a case study to illuminate our experiences in collaborating with artists on public health policy and practice research. Using existing frameworks from the literature, we define the attributes of, and challenges to, successful research collaborations and identify from our work how these apply to interdisciplinary collaborations between artists and public health practitioners. To support others working at the nexus of arts in public health, we include key experiences that were specific to the engagement of artists in research teams.
Keywords
Research is formalized curiosity. It is poking and prying with a purpose.
Public health has begun to shift to a “fifth wave,” which recognizes that “the public health community is dealing not with simple systems that can be predicted and controlled, but complex adaptive systems with multiple points of equilibrium that are unpredictably sensitive to small changes within the system” (Hanlon et al., 2011, p. 34). The co-occurring public health crises of 2020 (e.g., coronavirus disease 2019 [COVID-19] pandemic, health inequities) brought these concerns into stark relief.
To generate meaningful evidence to guide practice in these complex systems, research must reorient itself to not solely focus on measuring efficacy and effectiveness of interventions but also consider whether (and how) interventions interact with and affect the system (Rutter et al., 2017). In fact, the lessons of 2020 call on us to consider interventions, such as arts-based practices, as adaptive systems. Answering these complex questions requires interdisciplinary approaches, pushing individual researchers outside of their own discipline and collaborating with others through team science (Lakhani et al., 2012).
This shift calls for a change in mind-set from privileging specialist knowledge and expertise (i.e., “dominion and independence”) to valuing different ways of knowing and learning from and with others (i.e., “greater interdependence and cooperation”; Hanlon et al., 2011). Informing evidence-based arts in public health practice in this new paradigm calls for an increased role for artists on research teams. To ensure that research on arts in public health is patient centered, community responsive, and interdisciplinary requires new modes of engagement and integration of knowledge and methods across disciplines, including community-based research models (e.g., community-based participatory research, community-engaged research) and team science approaches.
Some work has been done to explore attributes of interdisciplinary teams (Lakhani et al., 2012) and team science as collaborative research practice (Little et al., 2017). However, there is a paucity of literature describing interdisciplinary research that includes artists as coequal research partners. Reflecting on our experience of engaging artists as part of a research team challenged what we thought we knew from our clinical and research training about interdisciplinary collaboration and products of those collaborations. Here, we explore our experiences in collaborating with artists on public health policy and practice research and elaborate on the attributes of, and challenges to, successful research collaborations between artists and public health practitioners using existing frameworks from the literature.
Case Study: The Rhode Island Arts and Health Advisory Group
The Rhode Island Arts and Health Advisory Group was convened in 2016 by the Rhode Island Department of Health and the Rhode Island State Council on the Arts to develop evidence-based recommendations for the integration of arts in health interventions and programming for the state of Rhode Island. The advisory group included artists, arts educators, musicians, dancers, storytellers, writers, health providers, administrators, and clinicians—many wearing multiple identities simultaneously.
To develop recommendations, the advisory group undertook a systematic review of the published research on arts in health by codesigning and executing the protocol, culminating in a review of the existing literature on relevant arts-based interventions, reported as an evidence map (Springs et al., 2019). The map was created by the advisory group to inform understanding of the evidence for the purpose of supporting responsible policy development.
Roles of Artists on the Research Team
In our advisory group, the majority of members served as coequal research partners who brought their artistic talents and training to the project and worked alongside public health researchers, clinicians, and statisticians. Thus, we describe this work as interdisciplinary research, in that we integrated “information, data, techniques, tools, perspectives, concepts, and/or theories from two or more disciplines . . . to advance fundamental understanding or to solve problems” (National Academies of Sciences, Engineering, & Medicine, 2005, p. 26). We also consider this work team science, as it was “a scientific collaboration conducted by more than one individual in an interdependent fashion, including research conducted by small teams and larger groups” (National Research Council, 2015, p. 22). These descriptors more accurately reflect the contributions made by the members who lent disciplinary, theoretical, and practical knowledge to all the critical stages of the project.
This case study provides a retrospective review of our experience through the lens of existing models to identify how these models fit and can be adapted to benefit future arts in public health research collaboration.
Attributes to Successful Interdisciplinary Research
An analysis of the interdisciplinary research literature identified seven attributes (team purpose, goals, leadership, communication, cohesion, mutual respect, and reflection) that contribute to successful interdisciplinary research teams. Table 1 provides definitions for each of these terms and an approach to implementing each one of them based on our experiences.
Attributes of Successful Interdisciplinary Research Collaborations and Approaches to Implement Them in Arts and Public Health Research
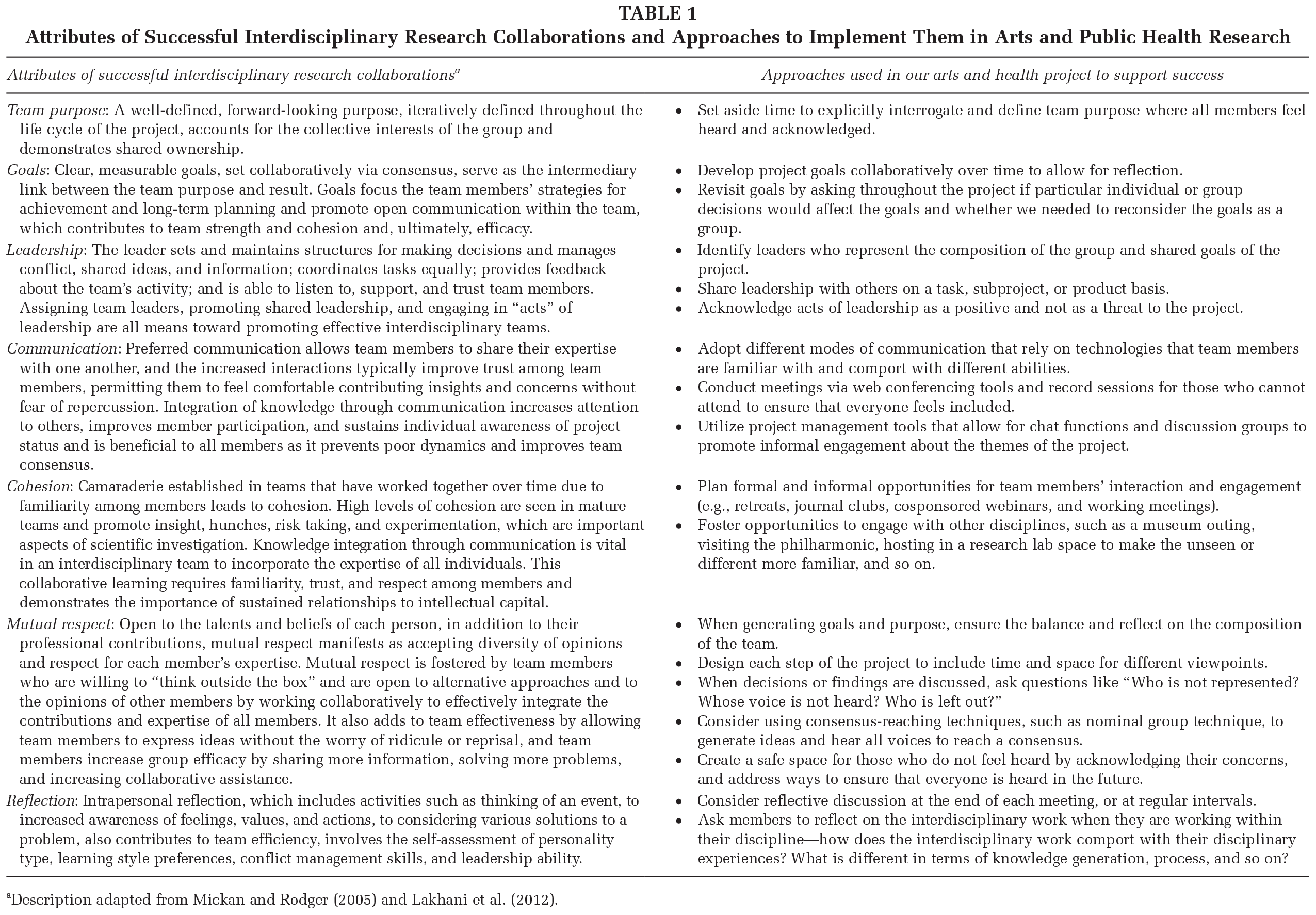
Description adapted from Mickan and Rodger (2005) and Lakhani et al. (2012).
We highlight team purpose, goals, cohesion, and mutual respect as key features to our success.
Team Purpose and Goals
Early in our project life cycle, it was collectively decided, and reaffirmed often, that the team purpose was to build explicit relationships between the disciplines of arts and health and to acknowledge that these disciplines coexist in our state—in some places seamlessly, in others more bifurcated and siloed. A goal of the project was not only to deliver evidence-based recommendations but, by doing so, to also demonstrate how artists, clinicians, and public health researchers could work effectively together to achieve the shared vision of improving community well-being.
Cohesion and Mutual Respect
The collaboration started from a place of curiosity, with all of us asking what is known about arts in health. Known—what counts as seen, heard, acknowledged, and valued in the public health space. For practical reasons, it was an initial step in the research process to develop a robust research question, and it started the process of codesigning the protocols. Asking the same question to a group who share the same goal but derive from different disciplines with distinct ways of knowing initiated powerful dialogue that illuminated the explicit role for not knowing in interdisciplinary collaboration, providing an investigative space that privileges asking questions, identifying problems, and valuing challenges.
We began from a place of humility, and this process fostered a shared acceptance that not knowing is not the same as not having expertise, and what we do not know was critical to the success of the project. For example, recognizing the limitations of research methods and research findings to provide solutions to all public health questions allowed space for arts-based practices to enter the conversation, as potential solutions not only to public health issues but also to the limitations of research practice.
Through our dialogues, we explored what we—collectively and individually—do not know. This exercise of interrogating what was known and unknown in the arts in public health space revealed that expertise is more than specialized knowledge but also the processes by which one makes sense of the world. For the purpose of this project, the necessary expertise required for success was not the type found in disciplinary silos but cocreated by the group and placed a value on curiosity as a foundational ethos for the team.
Through cocreation and co-implementation of the research plan, the team worked through each step of the project by discussing and making meaning of the process from their respective disciplines. Robust discussion, often with new ideas and different opinions raised, could potentially bog down project progress. Meeting facilitators worked to identify ways to continue conversations to ensure that team members did not feel marginalized or felt that they had to hold back opinions or ideas that will inform the project. Thus, we established a way through—not around—these issues by focusing the conversation on how these issues inform our thinking about the mutually agreed on products of collaboration (i.e., the final report, evidence map). By encouraging discussion while maintaining focus, we provided flexible space for discourse that was also project focused.
Hierarchy exists on research teams, and research often privileges those in academia with academic credentials. We acknowledged that this work would rely on honesty, psychological safety, and trust, which required us to examine hierarchy. In our case, that meant that hierarchy needed to be flattened. For example, a PhD researcher in the room acknowledged their dearth of knowledge about art and arts practice and asked that if they used a term, or characterized an arts practice improperly, to please interrupt and correct them so that shared meaning could be achieved. This allowed for open dialogue about terms, practices, theory, and meaning. It also modeled how to engage in dialogues across disciplines, identifying privilege and flattening hierarchy. Artists were encouraged to engage with nonartists or artists from other disciplines about their work and their methods. Clinicians shared content expertise on medical practices, but they were not the only experts on medical conditions—especially in the presence of those who represented patient communities. Everyone is also a patient—a caregiver with “expert” knowledge of these experiences—but in the research framework, we are often discouraged from embodying these parts of ourselves out of concern for biasing the trajectory of the work. In our work, we noted that research cannot afford to view research partners as unidimensional actors who identify only by their degrees attained or current job title. Successful recognition of these attributes requires a degree of humility, serving a higher purpose, and, ultimately, mutual respect that is fostered on strong interdisciplinary teams.
Challenges to Interdisciplinary Collaboration in Team Science
The Institute of Medicine (2001) acknowledged that their aim of more clinical/community partnerships could be hampered by disciplinary silos, egos, and rigid institutional norms. We identified additional complexity when approaching collaboration with artists through this lens. Though our research partners identified themselves as “artists,” the term artist represents a broad heterogeneity, for which a single, rigid silo would not suffice. Given this context, we encountered challenges to our work. In 2015, the National Research Council elaborated on seven features of team science that may present challenges to success: (1) high diversity of membership, (2) deep knowledge integration, (3) large size, (4) goal misalignment with other teams, (5) permeable team and group boundaries, (6) geographic dispersion, and (7) high task interdependence. Table 2 describes these challenges and provides approaches from work.
Challenges to Interdisciplinary Research Collaborations and Approaches to Mitigate Them in Arts and Public Health Research
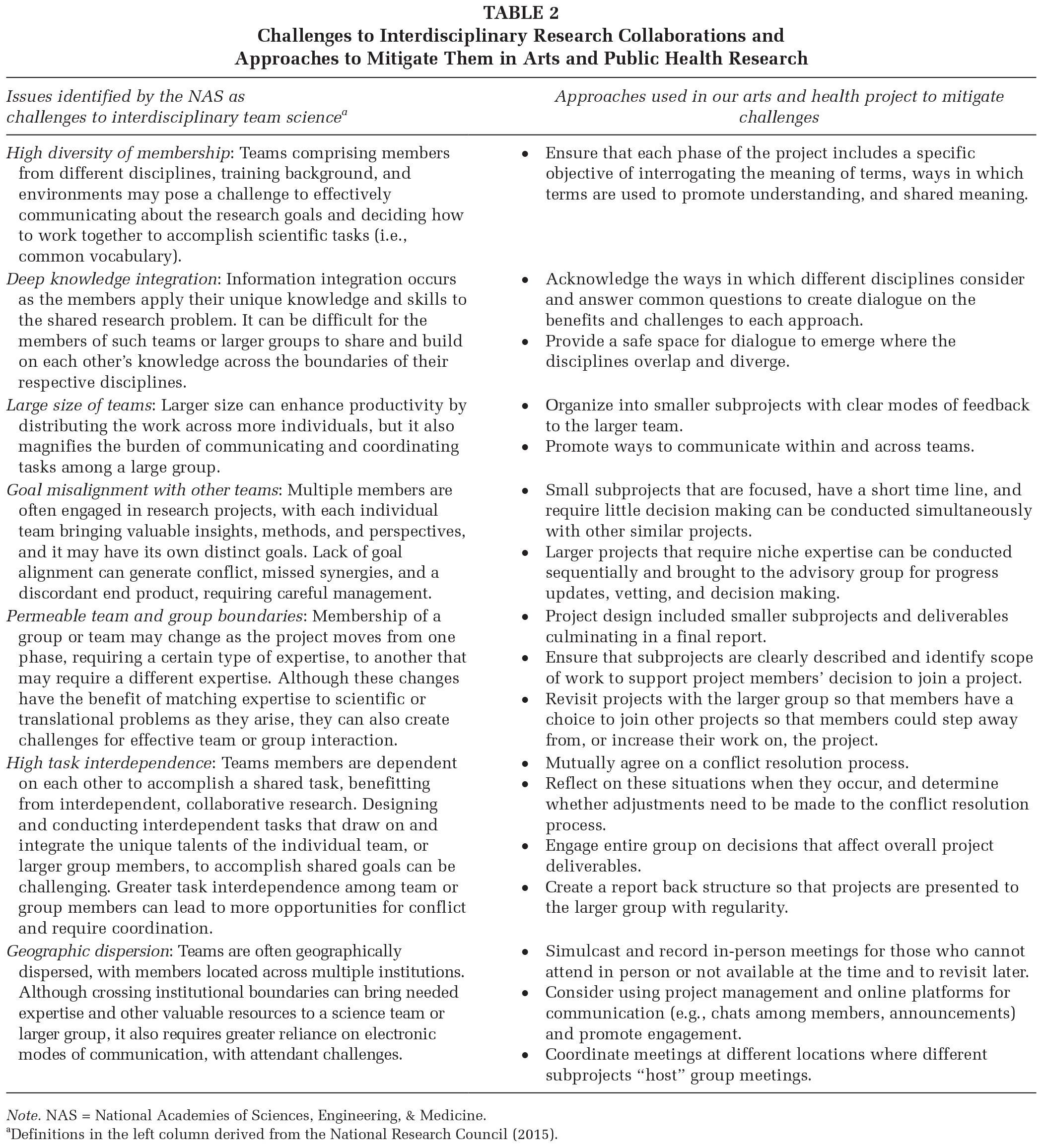
Note. NAS = National Academies of Sciences, Engineering, & Medicine.
Definitions in the left column derived from the National Research Council (2015).
We elaborate further on three challenges here.
High Diversity of Disciplines
This advisory group was selected based on each members’ expertise at the intersection of the arts and individual, community, and clinician well-being. We found that comprehensive representation does not necessarily promise a productive partnership, nor does it guarantee that a diversity of thought will be represented. We identified expertise obstacles, in that the advisory group had different disciplinary languages, processes, and practices. Acknowledging this early and revisiting this often required us to engage in the deliberate investigation of how our disciplines interact, overlap, and diverge as a necessary precondition for conducting the research. Empowering community voices that often go unheard in traditional health care spaces is a process in itself. The language of medical research is often dense and impenetrable. The group collectively worked hard to ensure that all the members were working from the same lexicon. True community engagement would not have been possible if, collectively, we did not use language that engaged the research team.
Deep Knowledge Integration
Our team came to this project with not only distinct disciplinary frames but also divergent views on accounting for different ways of knowing and what counts as evidence and why. To interpret research evidence, we had to bridge rigorous research methods by respecting critical outcomes that are difficult, if not impossible, to measure. We needed to foster a space for evidence and creativity to coexist. To overcome these empirical obstacles, each phase of the project included talking through the content, delving into emerging questions, concerns, and perspectives. For example, we found that the concept of assessing quality of research studies and peer review was very similar to the process of critique in artists practice and considered how these concepts might apply to the arts in public health research. The notion of assessing quality of research translated into the arts practice of critique, a place where our team found mutual ground and had robust conversation.
There are definitional and procedural variances even among similar arts-based interventions. Clarifying comparability was a collaborative investigation. We were actively translating these programs and interventions from one context to another, diligent in our efforts to not lose—or assign—deeper meaning to key study features. These considerations would have been lost otherwise on the nonartist clinicians and researchers, and we would have missed opportunities to compare interventions—or we might have compared incomparable interventions—because meaning was lost in translation between disciplines.
Permeable Team and Group Boundaries
On many interdisciplinary health care teams, members interact with others wearing their professional identity—physician, nurse, social worker, administrator, and so on—over their personal identity. In our group, many of the artists retained their personal identities and brought their experiences as patients and caregivers to the group dialogue. This provided an opportunity to hear patient and community voices early in the research process.
Empowerment also entailed letting go. Since the project was entirely novel to those participating, nobody could claim proprietary expertise. Group success depended on openness to different modes of thinking. For example, our researchers’ perspectives on evidence and outcome measures changed during the process. This dialogue changed the researchers thinking of the evidence map, giving them more comfort with uncertainty, risk taking, and the acceptance that the map might not support concrete recommendations.
Insights from Collaborating with Artists as Collaborators in Public Health Research
In retrospect, we can point to elements of work that were unique to our experiences working with artists on research teams and critical to the success of the project.
Working With Evidence as Materials
Evidence describing clinical interventions in academic journals and the lay media range from well-designed studies to anecdotal experiences. This holds especially true for reports on arts-based interventions and approaches. The group worked with experts in evidence-based medicine to understand how to navigate the information available on arts in health—whether derived from published studies or personal experience.
The artists on the team were essential to the literature review, as these discussions necessarily evolved to include reflections on how the research studies meshed with their practices. Many of the artists were actively working in clinics or with the community and were not indifferent stakeholders. Gaps in the evidence struck a tinny personal note for those artists whose careers were dedicated to those holes. Researchers were quick to point out that “gaps” in the map did not necessarily discredit specific arts-based categories but illustrated a lack of rigorous research published in the peer review literature and suggested ripe opportunities for future projects. As for areas with many studies, the saturation of research literature for a particular population or arts-based intervention did not necessarily mean it was better, or evidence based, as the quality of evidence may not be sufficient to translate into practice.
Using evidence synthesis methods as a tool of inquiry and knowledge generation, our interdisciplinary team worked to not just aggregate, but also interpret, existing evidence and allowed for a cocreated narrative to emerge. In this way, our team was able to assess how evidence fits, or fails, at the nexus of arts in public health.
Deciding on a Meaningful Product of Research Partnerships and Collaboration
Interdisciplinary work requires an a priori discussion about what constitutes a meaningful product of collaboration and may require compromise to reach agreement. Our group produced a publication quality evidence map that represents the medical literature in the field of arts in health. The group wanted this resource to be open access, accessible to community partners in Rhode Island and beyond. Thus, the first product of collaboration was not a typical academic research product—a peer-reviewed journal article—as this would benefit the small number of academics in the group. The open online evidence map was in line with the ethos and shared commitment of the group.
To a group of artists, the standard evidence synthesis method of reporting out using a static, tabular listing of studies would not do. Our artist collaborators learned to translate and explain research methodology to nonresearchers. It is a constant reevaluation of where to start and how to make yourself understood. The group coalesced around the idea of an interactive evidence map, an accessible interface that would not intimidate artist groups from accessing these studies while providing valid content for public health policy leaders who rely on evidence for decision making. We enlisted the expertise of data visualization experts to create a colorful matrix to identify populations and interventions studied across the field—a living, interactive online map of health care interventions.
Translating Research Evidence Into Public Health Practice
Through meetings, focus groups, and community presentations, we met with leaders from state agencies and clinical organizations to discuss our work, our findings, and understand the needs of the state’s health care ecosystem. The report’s recommendations centered on existing individual and community needs—medical and social problems—and how the arts could play a role. Chronic illness, priority populations (e.g., children and aging populations), and critical public health issues (e.g., opioid/substance use disorder) and other issues such as social isolation and resilience for patients, caregivers, and health care providers were areas that emerged from the dialogues with our stakeholders. We found out that the artists took a prominent role in disseminating our findings, adapting them into their current practice. As with many interdisciplinary research teams, the work served as fertile ground to seed future collaborations.
Designing Interdisciplinary Team Science Teams for Arts and Public Health
This project was initiated by two state agencies that wanted to collaborate—the Rhode Island Department of Health and the Rhode Island State Council for the Arts. Securing and maintaining “buy-in” from the agencies anchored this work and gave the work a sense of legitimacy, providing the artists with a sense of inclusion. While Rhode Island is small and agile, our work is replicable and scalable.
Future consideration should be paid to develop a well-rounded approach to true interdisciplinary collaboration among arts in public health practitioners to support meaningful knowledge translation. Our case study provides a provocation and space for introspection on the unique features of true interdisciplinary collaboration at the intersection of arts in public health:
Interdisciplinary partnerships at the nexus of arts in public health require a process that toggles between data-driven rigor and a rigorous examination of what each group values as data.
Team purpose and goals must amplify the shared purpose and a role for the arts and artists to meet existing health and community needs.
Leadership, cohesion, and mutual respect are necessary, but not sufficient, for successful interdisciplinary collaborations—choosing a complement of people with disciplinary expertise and soft skills to enable the team to function are equally important.
True interdisciplinary work requires establishing safe spaces because having your ideas challenged can be discomforting.
Artists are disciplinary experts and bring knowledge of theory and practice in arts and therefore should be compensated in commensurate fashion by other experts on the research team.
Discussion
Our advisory group took great care to investigate the role of arts in the context of local health needs and attempted to honor the intrinsic value of the arts while respecting the evidentiary standards medicine typically expects of health care interventions. To achieve our goal, we had to consider how to develop evidence-based recommendations for public health policy and practice when arts-based interventions do not fit the conventional medical model (Crawford, 2018). Signaling the value of the arts and artists in a data-driven culture is difficult when many arts interventions elude objective measurement using the standard tools in the researchers’ toolkit. These tools are inflexible and unyielding when faced with the dimensionality and complexity of arts interventions and their multipotent impacts on individuals and communities. The arts are not a molecule targeting a receptor but a human experience evoking passionate opinions about its value in health care with various levels of evidence existing to support such beliefs (Bickerdike et al., 2017). Complex interventions, such as arts-based practice, benefit from interdisciplinary and team science–based approaches, as these work to promote integration of practices and erode disciplinary obstacles. In turn, this work is suited to developing sensitive tools that not only identify the efficacy and effectiveness of arts interventions but also capture how arts and artists interact with public health systems.
Defining successful interdisciplinary teams requires more than contemplating the attributes and challenges we outlined here. Groups must be willing to do more than focus on designing the research; they must attend to the design of their team. While the technical skills of each member are important, team dynamics, interpersonal engagement, and a set of principles of practice, to include how conflict is resolved, and modes of efficient and effective communication are other key features that strengthen collaboration (Lakhani et al., 2012). Our work demonstrates that the translation of arts in public health research into policy and practice is improved when artists participate as stakeholders, community members, and disciplinary experts.
Footnotes
Authors’ Note:
The authors acknowledge the talented artists who participated in the Rhode Island Arts and Health Advisory Group; Valerie Rofeberg for her research expertise; and Spencer Phillips Hey for his work on the online evidence map. This work was funded in part by the Rhode Island Foundation (Springs), AHRQ R25HS23299 (Springs), and AHRQ K12HS022998 (Springs), and supported by the Rhode Island Department of Health, Rhode Island Council on the Arts.
Supplement Note:
This article is part of the Health Promotion Practice supplement, “Arts in Public Health.” The supplement includes exciting projects, strategies, frameworks, practices, and places that advance health through the arts. The Society for Public Health Education is grateful to the University of Florida Center for the Arts in Medicine and ArtPlace America for providing support for the issue. The entire supplement issue is available open access at ![]() .
.