
Abstract
Public health practice continues to expand beyond traditional partners to increase reach and impact in communities. This is particularly important in rural communities, who face inequities in the social determinants of health and increased chronic disease burden. However, the capacity for non-traditional community organizations to understand and implement public health work varies widely. Promoting policy, systems, and environmental change strategies (PSE’s) is a promising method to support public health in rural communities, due to their variety, flexibility, and potential impact.
Using a mixed methods approach to data analysis, we explore the barriers, challenges, and lessons learned from efforts in two rural Appalachian counties to stimulate use of PSE strategies through micro-funding. Several significant barriers were identified: challenges with evaluation and reporting, and lack of understanding and limited utilization of PSE strategies. Successful approaches to overcome these barriers included (1) changing reporting processes to reduce reliance on technology and shift reporting burden from community partners to researchers, (2) adapting data collection to capitalize on strengths of project partners, and (3) abandoning scientific language to embrace more common terminology used in communities. Policy changes were the least utilized strategy. This strategy may be less relevant in rural grassroots organizations with a small staff. Additional research into barriers to policy change is recommended. Enhanced training and support for grassroots, local-level PSE interventions could expand public health promotion in rural areas, reducing rural health disparities.
Keywords
A critical element in the evolution of public health practice is the movement to engage non-traditional public health partners at the grassroots level. These partnerships can facilitate efforts to implement evidence-based strategies known to improve population health (Buys & Rennekamp, 2020; DeSalvo et al., 2017). This is vital in rural communities, which face high burdens of disease and disadvantages such as lower socioeconomic status and less access to health promoting resources (Ziller & Milkowski, 2020). Rural health departments are providing more direct care and less population-level health promotion (Harris et al., 2016). Rural areas suffer from lack of access to medical care, aging water systems, crumbling roads, outdated schools, and lack of access to broadband internet. These disparities in the social determinants of health threaten to widen the existing gap between urban and rural health (Ziller & Milkowski, 2020).
Background
Engaging Non-Traditional Partners
Given the limited capacity and resources in rural communities, non-health-related grassroots organizations are being encouraged to develop, implement, evaluate, and sustain evidence-based public health promotion projects. However, the capacity for organizations to conceptualize and implement this work varies widely (Leeman et al., 2015). Program infrastructure and organizational capacity to implement and sustain interventions have also been identified as barriers to improving public health (Lavinghouze et al., 2014). Many of these barriers arise from the nature of grassroots organizations: few staff, reliance on volunteer labor, lack of access to reporting mechanisms such as computers and broadband internet, and lack of educational background or training to do the types of evaluation and reporting required by researchers.
Policy, Systems, and Environmental Change Strategies
Training community organizations to implement policy, systems, and environmental change (PSE) strategies holds promise as an effective means to build capacity in non-traditional public health partners. PSE strategies have the potential to create broad-reaching sustainable health impacts (Bunnell et al., 2012; Kelly et al., 2021; Rohan et al., 2019). PSE strategies have been used in efforts to improve obesity rates (Betancourt et al., 2017), prevent chronic disease (Bunnell et al., 2012), and reduce cancer rates (Townsend et al., 2019). Examples of successfully implemented health promotion policies include instituting a healthy food donation policy in food pantries and creating shared-use policies at school playgrounds. Successful systems changes include creating systems for schools to purchase locally grown produce to serve at school meals and creating a referral system for food pantry clients to receive produce boxes. Successful environmental change examples include installing signs to promote community trails, adding painted crosswalks and bike paths to streets, and installing community gardens at a church. Because PSE strategies are varied and flexible, they are relevant for health promotion in under-resourced areas. However, sparse research exists about the feasibility, adoption, and sustainability of this approach by rural communities.
Community-Based Participatory Research in Rural Communities
Supporting rural community organizations to conduct PSE work builds on prior public health work. Community organizations and laypeople have long been identified as critical partners in public health promotion. Community-based participatory research (CBPR) can reduce health disparities by engaging these groups to build equitable, reciprocal relationships between communities, researchers, and practitioners (Wallerstein & Duran, 2010). Local-level capacity issues have been documented in CBPR research, describing the challenges of partnering with organizations that have fewer research skills and are uncomfortable with scientific language employed by university-based partners (May & Law, 2008). Appropriate, relevant training is not available for community partners (Coombe et al., 2020). Utilization of a CBPR-based approach can strengthen connections between public health researchers and community organizations and build capacity for local organizations to engage in public health promotion (May & Law, 2008). This approach can lead to increased community capacity, increased sustainability of programs, and improved health equity.
Micro-Funding as a CBPR Component
Efforts to engage communities in balanced, reciprocal relationships inspired the use of micro-funding as a component of the CBPR approach utilized by West Virginia University’s (WVU) Be Wild, Be Wonderful, Be Healthy (Be Healthy) project. Micro-funding (frequently called mini-grants) has gained traction as an effective means to authentically engage community members in public health interventions (Bobbitt-Cooke, 2005; Hartwig et al., 2006). Using CBPR and mini-grants enables researchers to support community-centered projects, address underlying capacity issues, and improve sustainability. Researchers have used micro-funding to create arts-based cancer screening initiatives (Friedman et al., 2019), offer monetary incentives to use farmers markets (Abildso et al., 2019), and create a wheelchair-accessible playground (Tompkins et al., 2022). Although existing studies point to the potential of mini-grants to stimulate local action, the lack of expertise among those responsible for local level implementation and evaluation presents a challenge to fully understanding the impact of mini-grants (Abildso et al., 2019; Tompkins et al., 2022). A micro-funding cancer prevention project identified the disconnect between the need for researchers to document progress and outcomes to funders and the conflicting community focus on meeting needs or providing services and disregard for reporting (Thompson et al., 2010). Incomplete implementation and evaluation data precludes thorough understanding of the impact of micro-finding; however, grassroots organizations are often focused on “doing the work” and not completing reports. Further, research in rural Appalachian communities in Tennessee identified a disconnect between rural communities’ definitions of success versus traditional public health outcome metrics (Kidwell et al., 2019).
Purpose and Aims
The overarching goal of the High Obesity Program (HOP, cooperative agreement CDC DP18-1809) is to support PSE changes to improve access to physical activity and healthy foods. In the most recent iteration of HOP, WVU’s Be Healthy project received funding for two counties selected by the CDC: Clay and McDowell. Both counties are rural, with mountainous terrain, rivers and creeks, and geographic barriers that result in small communities scattered across a large distance. Clay County is home to 8500 residents; McDowell County has 18,000 residents. Be Healthy utilized CBPR and micro-funding to stimulate implementation of PSE’s related to healthy food access and physical activity access. This article describes challenges faced and lessons learned while using a CBPR-based, micro-funding approach to stimulate PSE strategies in two rural counties as part of HOP. The lessons learned may provide other public health practitioners with guidance to build rural communities’ capacity to design, implement, and evaluate PSE strategies for health promotion. This article contributes to small but growing body of research identifying the challenges with implementation and evaluation of PSE strategies in rural communities.
Methods
PSE Definition
Written definitions of PSE’s were provided to community organizations and collaborators:
These definitions were used throughout all phases of the project.
PSE Support and Training Methods
PSE’s were described and emphasized in all project materials and communications. The project team created documents describing PSE’s and providing relevant examples. Mandatory training webinars were conducted after community collaborators were approved for funding. Technical assistance for PSE’s was provided by phone, email and in-person site visits. County-based Extension agents provided support and assistance for all aspects of community partner projects, including project design, application for funding, implementation, and data collection.
Process Evaluation Methods
A mixed-methods process evaluation was conducted using existing program data and reports. The outcome of interest, PSE strategy implementation, was assessed using these sources. Data were collected from funded projects’ grant applications, mid-term reports, end of year reports, phone interviews, and site visits. Table 1 describes data collection methods and sources.
Description of Data Sources, Including Changes Across Years
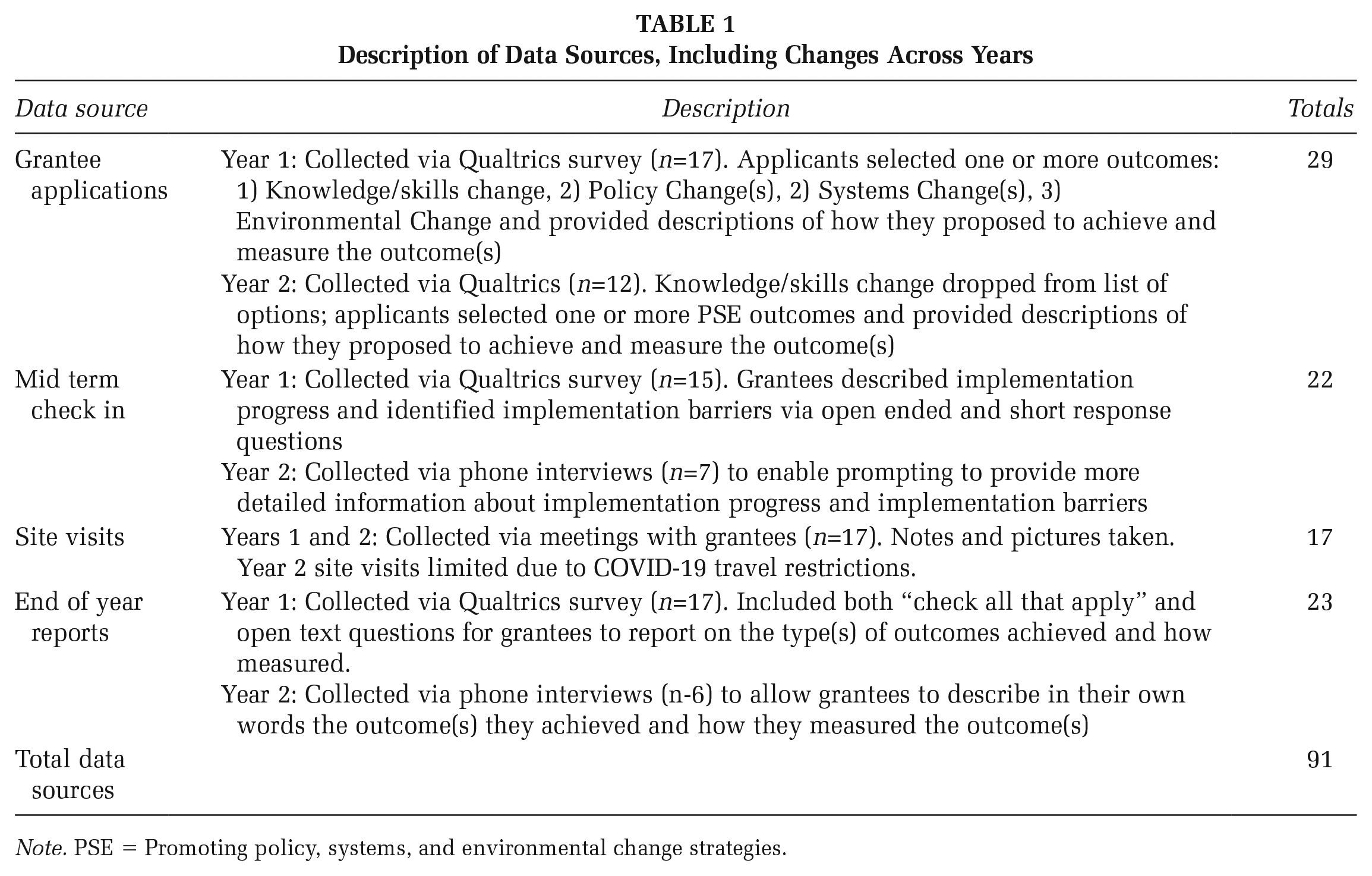
Note. PSE = Promoting policy, systems, and environmental change strategies.
Data Coding and Analyses
Authors of this article reviewed each data source independently, multiple times. Discrepancies were discussed and resolved among authors to ensure that the outcomes and themes accurately represent the data, challenges, and lessons learned.
Some reported PSE outcomes were re-coded by the evaluation team, due to misattribution. For example, when a respondent selected policy change as an outcome, but the description was for an environmental change, we recoded this to be an environment change. Consultation with project team members who had conducted site visits or county-based extension agents confirmed the accuracy of the revisions.
Funded partners’ reported PSE strategies were deductively coded independently by two team members using the PSE definitions described above. Non-PSE strategies (e.g., programs) more focused at the individual level were coded as I. Coding discrepancies were resolved by consensus. Frequencies of PSE strategies were calculated and grouped by organizational type using the typologies provided by the Internal Revenue Service (IRS) Activity Codes. These mixed methods data collection and analysis process led to the authors identifying challenges and lessons learned for implementing PSE strategies in these rural communities and settings. Identified themes include expanded reach, reporting and evaluation challenges, and the role of Extension agents.
Results
In year one, 17 projects were approved for funds amounting to $81,000. In year two, 12 projects were approved for $80,061 in funding. Mid-way through year two, the Covid-19 pandemic occurred. This resulted in implementation delays in four of the year two projects; their results are not included. Results were reported for a total of 25 projects: 17 year one projects and 8 year two projects. Details about funded projects can be found in Table 2.
Characteristics a of Funded Organizations by Year

Primarily derived from IRS Activity Codes https://nccs.urban.org/publication/irs-activity-codes
Table 3 displays information about the organizations that were funded, project outcomes, and examples of reported outcomes.
Cumulative (Years 1 and 2) Reported Outcomes by Organizational Type (n=25 Organizations).
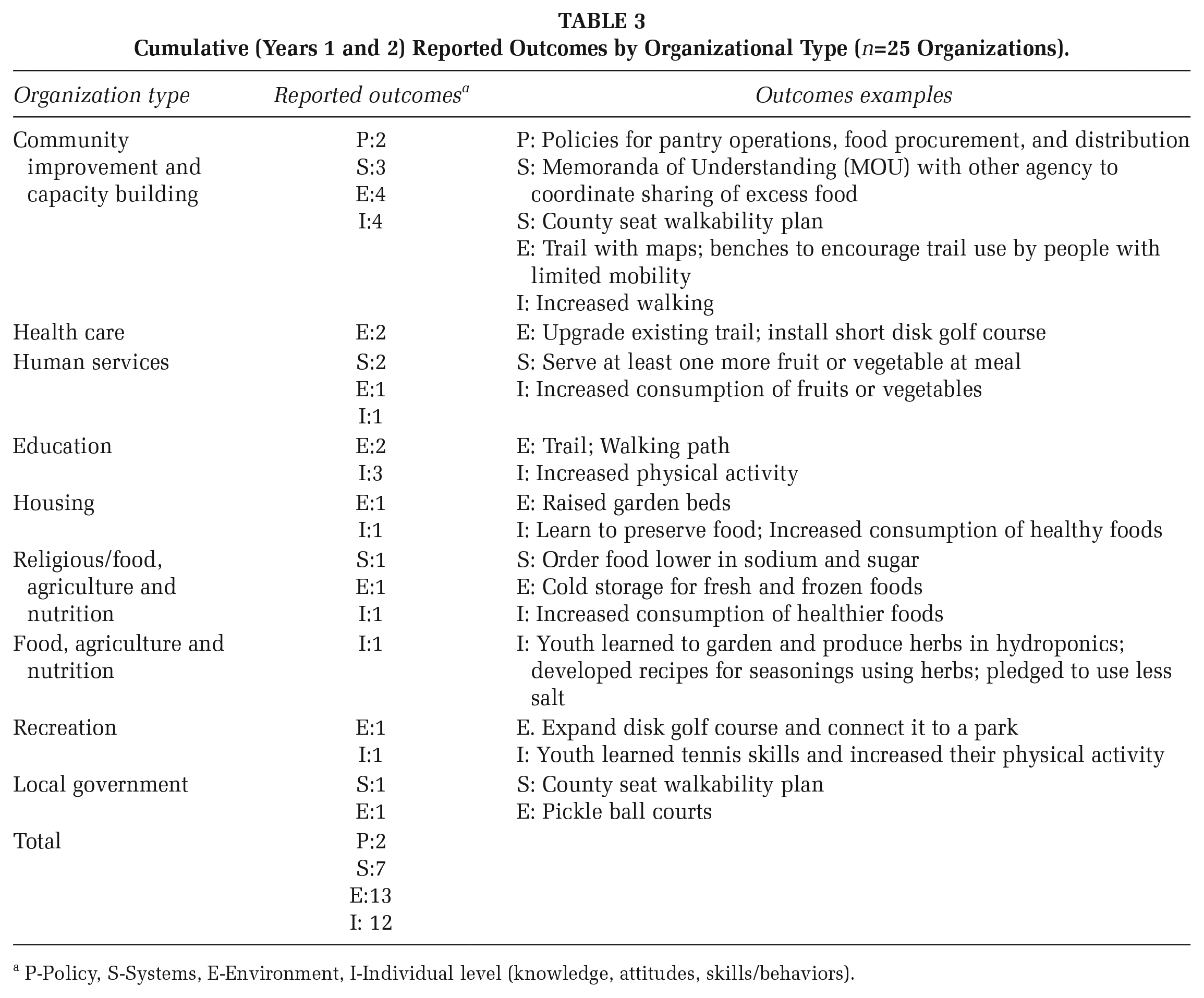
P-Policy, S-Systems, E-Environment, I-Individual level (knowledge, attitudes, skills/behaviors).
PSE Outcomes
Collectively, reporting organizations achieved a variety of PSE outcomes as well as those more focused on the individual level (knowledge, skills and behaviors). Changes to the environment were the most frequently reported outcome (n=13), followed by individual level (n=12), systems (n=7), and policy outcomes (n=2). Some outcomes reported by grantees had to be recoded to better represent the actual scope of outcomes achieved. For example, one grantee reported increased physical activity by children (behavior), but neglected to report the environmental change (e.g., walking path around playground) primarily responsible for the increased activity. Relatedly, reported individual level outcomes were problematic. Some were hypothesized as expected or projected to occur, rather than as having occurred. An example of this is a grantee reporting that because they distributed fruits and vegetables, people consumed more fruits and vegetables. On the other hand, some grantees provided very detailed examples of individual level changes via pre and post surveys.
It is notable that only two of the total reported outcomes were policies. This is consistent with existing research. A recent study of healthy eating and physical activity PSEs in Community Health Improvement Plans revealed a focus on individual level strategies rather than PSEs (Sreedhara et al., 2020). A church-based intervention to implement PSE changes to promote healthy eating and physical activity environments noted lack of policy changes and resistance to the use of the word “policy” and the need for alternative phrases like “guidelines” (Bernhart et al., 2022).
Expanded Reach
Community partners funded in the first year were able to expand impact and reach and layer additional PSE’s by applying for funding in year 2. One such partner, a community improvement organization, requested funding in year one to facilitate completion of a walking path at a community park. In end-of-year interviews, organizers reported receiving feedback that many individuals were unable to complete an entire lap due to disability issues (i.e., difficulty walking, chronic disease that impaired breathing) and would sit on the ground to rest. The next year, the organization applied for funding for benches along the path, enabling a wider range of ages and abilities to utilize the path.
Another community partner, a religious-based food, agriculture, and nutrition organization, expressed their desire to provide healthier food through their food pantry. In year one, the organization applied for funding for cold storage, to facilitate distribution of produce and frozen foods including fruits, vegetables and meat. Site visits led to discussions between project team members and organization staff, resulting in the implementation of a policy limiting sodium and sugar in items purchased for distribution in year 2.
Challenges in Reporting and Evaluation
Data collection and conversations occurring in the context of site visits and phone interviews led to the identification of challenges with the reporting and evaluation process. Most community partners in the two project counties had little experience with online reporting. Many grassroots level partner organizations rely solely on volunteers, others had very few (<5) staff (n=8), and some had both characteristics. On site visits, two partners reported that they did not have access to computers or smart phones to complete required documentation. Several partners mentioned struggles with broadband internet access which negatively impacted their ability to utilize the online survey portal. In mid-term phone interviews, one project partner stated that the reporting was too complicated and difficult to understand. On another site visit, a funded partner identified their lack of educational attainment and literacy as a barrier to adequately answering questions on the mid-term and end of year survey.
Inaccurate reporting by funded organizations was identified as an issue by the project team in year one. Inexperience with the type of reporting required by the HOP project led to mis-reported outcomes. Project partners vastly overestimated or underestimated the reach of their projects. One project described the reach (# with increased access) of an outdoor physical activity site based on the number of people who used an online check-in mechanism, rather than the number of community members with improved access. Another community measured reach of a walking path through the number of individuals who signed up for a walking program based at the path, rather than the number of residents with increased access due to development of the site. One respondent indicated that every person in the county (>8000) had increased access to physical activity due to a trail that was developed, regardless of their distance to the trail, because the trail was open to the public. In year 2, the evaluation team took over the designation of “reach” for funded projects, based on geographic identifiers (GEOID’s), census tract reporting, and CDC recommendations. This change provided greater consistency and accuracy in measurement of reach.
Academic Terminology and PSE Nomenclature
PSE nomenclature was also identified as a barrier to reporting and evaluation. Documents and online webinars were created to provide information and support for evaluation and reporting and PSE change strategies. These resources were underutilized and often did not meet the needs of funded partner organizations. Documents created for support were challenging to access, embedded within an online survey. While well-intentioned, these approaches were academic, research-based approaches and did not meet the needs and desires of the community.
Describing PSE strategies using research-based and academic terminology is confusing and off-putting to many community partners. However, the CBPR approach and ongoing development of collaborative, respectful partnerships resulted in the project team identifying several PSE changes that were not initially reported by partners. Using phone interviews and site visits, rather than online surveys, gave the project team a more realistic and nuanced understanding of the work being done by community partners, resulting in more accurate reporting. As trust between the project team and community partners increased, the flow of communication improved. Community members were more open about the challenges that were faced, allowing the project team to provide more meaningful support.
Role of Extension Agents
Discussion
In the first two years of Be Healthy, partner organizations implemented a total of 22 PSE changes in the two project counties. A variety of organization types were funded and completed projects. Incomplete and inaccurate reporting precludes an accurate estimation of reach; however, partners that collaborated for 2 years were able to expand the reach and depth of their specific projects. Environmental changes were the most implemented PSE strategy (n = 13). Environmental changes may be the easiest PSE strategy to understand and implement, while meeting a specific need in the community. This may be due in part to the need for external funding resources in rural counties. The number of environmental changes supports findings that providing resources and funding can drive environmental changes in communities (Kelly et al., 2021).
Systems changes (n = 7) included county seat walkability plans and MOU’s with agencies to coordinate sharing of excess foods. Interestingly, many of the systems changes required deeper collaboration and intensive technical assistance from project team members. External experts were recruited by the project team to assist with county seat walkability plans, resulting in a comprehensive written plan for each county. Both plans were developed in the second year of Be Healthy, when collaboration and trust had increased. This result is congruent with other research showing the development of deeper, more engaged relationships with partners and stakeholders leads to increased support for PSE’s (Rohan et al., 2019).
Policy changes (n=2) were the least implemented strategy. This could be due to dislike of the word “policy” and its connotation with rules, as seen in other PSE implementation studies (Bernhart et al., 2022). The staff size and lack of organizational structure in many local grassroots organizations may also explain the lack of policy changes. Organizations with a small number of staff do not feel the need to create policies. More than a third (n = 8) of funded partner organizations had fewer than 5 staff members. Thus, policy changes may have been deemed irrelevant or unimportant. This is an important consideration for future PSE work that involves rural grassroots organizations.
Strengths and Limitations
Several limitations to the study exist. Although a CBPR-informed approach was implemented by Be Healthy, HOP requirements preclude the project from being a full iteration of the CBPR approach. Challenges associated with data collection suggests the information presented in this article may provide an incomplete picture. Finally, the worldwide Covid-19 pandemic resulted in disruptions to the project that caused changes to project timelines, provision of technical assistance, and planned data collection methods.
The strengths of the study include the flexibility of the data collection methods. When initial data collection resulted in incomplete or inaccurate data, the project team collaborated with community partners to devise more appropriate, accurate methods to collect necessary data. This required additional time and effort from the project team but strengthened communication and trust between the project team and community partners. The ongoing cycle of engaging with community partners to improve processes led to improvements in the way the project team provided support to grassroots organizations in the two project counties.
Implications for Research and Practice
Strengthening the ability of grassroots community organizations to engage in public health promotion is a necessary step in the evolution of public health practice. Supporting community-based organizations in the design, implementation, and evaluation of PSE change strategies in rural communities has potential to reach underserved and excluded audiences. Lack of organizational capacity can hamper these efforts. Existing resources for PSE work are often geared toward higher capacity organizations or provided in methods that do not meet the needs of small grassroots organizations.
One implication for practice is the need for user-friendly PSE training that can serve the needs of grassroots community organizations and Extension agents. Training county-based Extension agents would enable local trusted partners to provide PSE strategy and evaluation support. Employing the same model that Cooperative Extension has used to bring agricultural research and expertise to communities for over a century is a promising model to build public health capacity. This approach could facilitate the translation of research- and evidence-based strategies into practice in rural communities.
Capacity for reporting and evaluation by small grassroots organizations will most likely remain limited. It is the responsibility of public health practitioners to adapt technical assistance, trainings, and reporting and evaluation requirements to align with the strengths and skills of community organizations. This includes making reporting and evaluation requirements more streamlined and less burdensome, while honoring the knowledge and skills of the community. We suggest that building capacity to do academic and research-based evaluation and reporting is inconsistent with the needs and strengths of rural grassroots organizations. Therefore, building capacity for academic-based reporting and research does not meet the needs of rural grassroots organizations and should be eliminated from researchers’ goals. Ongoing communication, engagement, and trust building can facilitate more useful methods of data collection and reporting.
While most of the findings in this study align with previous research, it is worth noting the lack of policy change implementation. In small grassroots organizations, policy change may not feel relevant or necessary. This merits further consideration by both funders and researchers.
In the future, public health researchers and practitioners need to be aware of the constraints and needs of grassroots-level organizations and adjust technical assistance, support, data collection, and workload accordingly. Continued focus on barriers and solutions to PSE implementation will help strengthen relationships between community partners and public health practitioners. This may lead to improved outcomes and reduced health disparities in rural communities.
Footnotes
Authors’ Note:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was supported by funding from the Centers for Disease Control and Prevention DP18-1809 5 NU58DP006563-03-00.
Supplement Note:
This article is part of the Health Promotion Practice supplement, “Reducing Chronic Disease through Physical Activity and Nutrition: More Public Health Practice in the Field.” The purpose of the supplement is to showcase innovative, community-centered, public health actions of SPAN, REACH, and HOP programs to advance nutrition and physical activity among priority populations in various settings. The Society for Public Health Education is grateful to the Centers for Disease Control and Prevention, Division of Nutrition, Physical Activity, and Obesity for providing support for the issue. The entire supplement issue is available open access at ![]() .
.