
Abstract
This article examines patterns in civic engagement and health among U.S. adolescents currently enrolled in school. Adolescents engage in multiple forms of civic action (e.g., civic discussions, volunteering, and political activities) and form varied civic attitudes and skills, which, in turn, may shape their health and well-being. Further, such associations between civic engagement and health may be differentially influenced by students’ social locations (e.g., socioeconomic position, race and ethnicity, and gender). The authors examined associations between civic engagement (behaviors, attitudes, and skills) and health (physical, mental, and well-being) and how these associations varied among four race-gender subgroups in the United States. Survey data from 1,286 adolescent students in grades 6–12 (average age = 14.56) were collected between fall 2021 and spring 2025. Analyses revealed that main effects for the full sample obscure distinct patterns of associations between civic engagement and health among subgroups. For example, there were more positive associations between components of civic engagement and health outcomes for both girl/transgender and gender-diverse subgroups (White and students of color) compared to boy subgroups, and political participation and civic discussions showed more negative associations with health outcomes for the boy and girl/TGD students of color subgroups compared to White subgroups. Sense of community was positively associated with health outcomes for all subgroups. Practitioners promoting civic health equity should consider different aspects of civic engagement, and programs are needed that are responsive to variations in the associations between civic engagement and health at different intersections of race/ethnicity and gender.
Adolescents increasingly interact with their sociopolitical contexts, become more aware of the world around them, discuss civic issues, participate in civic activities, and form civic beliefs and values (Malorni et al., 2024; Pinedo et al., 2024). Adolescents engage in multiple forms of civic action (e.g., civic discussions, volunteering, and political activities) and form varied civic attitudes and skills (Wray-Lake & Ballard, 2023), which can, in turn, shape their health (Ballard & Syme, 2016; Maker Castro et al., 2022; Mužík et al., 2025). Associations between civic engagement and health vary depending on students’ many social locations (e.g., socioeconomic position, race/ethnicity, and gender) (French et al., 2020; Karras et al., 2022).
Conceptual Framework
This study is grounded in developmental and ecological perspectives and is informed by a multitheoretical approach (see Wegemer et al., 2025, for a summary). Specifically, we draw on the conceptual framework of sociopolitical development (Watts et al., 2003), which emphasizes how civic engagement may serve a unique function for the development of adolescents from historically marginalized backgrounds. Thus, we advance this field of research and practice by investigating the associations of specific dimensions of civic engagement for health and whether they vary by the social locations of adolescents.
Civic Engagement and Health
Civic engagement includes prosocial and political commitments and contributions to society that are behavioral and psychological (Wray-Lake & Ballard, 2023), encompassing behaviors, attitudes, and skills (Wray-Lake et al., 2017). While conceptually broad, dimensions of civic engagement (e.g., behaviors vs. attitudes) and different behaviors (e.g., volunteering vs. activism) have unique predictors, experiences, and consequences for adolescent health (Mužík et al., 2025). Civic engagement has historically been viewed through a lens of positive youth development and considered to be a constructive activity with benefits to individuals and communities (Ballard & Syme, 2016). However, youth experience both costs and benefits of civic engagement, especially when it involves navigating and acting on unjust, inequitable, or highly polarized policies and practices, which can be exacerbated in the current media/social media environment to which youth are near-constantly exposed (Dunn et al., 2022; González-Bailón et al., 2023). Consequently, both the costs and benefits of civic engagement may vary depending on adolescents’ social identities and their contexts (Pinedo et al., 2024; Wegemer et al., 2025).
Civic Behaviors and Health
Among high school students, prosocial civic behaviors such as volunteering are positively associated with psychological well-being and negatively associated with depressive symptoms (Kim & Morgül, 2017; Wray-Lake et al., 2019). In contrast, more political civic behaviors (e.g., activism) are often negatively associated with adolescents’ health (Conner, Crawford, et al., 2023; Pavlova & Lühr, 2023), although activism is sometimes beneficial for youth, depending on context (Heberle et al., 2022; Testa & Cavallini, 2021).
Civic Attitudes and Health
Civic attitudes describe the ways that people think and feel about their community or society, including how connected people feel to those around them and how empowered they feel to make a difference in their communities. Adolescents’ civic attitudes of community connectedness (Lardier, 2018) and civic self-efficacy (Maker Castro et al., 2022) are associated with better health.
Civic Skills and Health
Civic skills are closely related to civic attitudes but might function differently for health, as skills indicate having practice with civic life, whereas attitudes encompass cognitive and emotional views and beliefs about civic life. Some evidence suggests that civic skills are associated with higher health and well-being (Christens & Peterson, 2012).
Patterns of Associations Between Civic Engagement and Health Across Groups of Adolescents From Different Sociodemographic Backgrounds
Ecological conditions (e.g., systems of oppression, current events, and school and community contexts) may explain variations in civic engagement among youth (Hope et al., 2023; Pinedo et al., 2024). Adolescents’ opportunities to engage civically, and possibly the net effects of such involvement on health, are structured by interlocking social hierarchies (Hall et al., 2022; Saavedra et al., 2024). Individuals who hold identities (e.g., race/ethnicity, gender, sexual orientation, and socioeconomic position) that are marginalized due to structural forces such as racism, sexism, heterocentrism, and classism (Williams & Medlock, 2017) might experience health challenges associated with civic engagement (Baskin-Sommers et al., 2021; Manalo-Pedro et al., 2024). Although sociodemographic characteristics are imperfect proxies of ecological conditions and social experiences (Adkins-Jackson et al., 2022), they are accessible in self-reported data and often used to study civic engagement and associated outcomes across groups. Heterogeneity within groups adds complexity. For example, people may share some experiences as racialized minorities but differ on others, such as experiences with sexism (Saavedra et al., 2024). Studies examining civic engagement and adolescent health by race and gender extend current literature (Heberle et al., 2022; Saavedra et al., 2024; Zong et al., 2024).
Study Aims and Hypotheses
Our study (1) examines associations between civic engagement (behavior, attitudes, and skills) and health (physical, mental, and well-being) and (2) explores variations in patterns of associations for adolescent middle and high school students by self-reported sociodemographic backgrounds (gender and race/ethnicity). We hypothesize that civic attitudes will be positively associated with health, and some civic behaviors (volunteering) will be associated with better health, while others (political behaviors) will be associated with worse health. However, we expect that patterns will differ for subgroups, whereby White girls and transgender and gender-diverse (TGD) youth and youth of color (both boys and girls/TGD) will show more negative associations between civic predictors and health outcomes.
Method
Data Collection
Data come from baseline surveys (preintervention) of a randomized controlled trial studying the impact of a civics education intervention on adolescent well-being (Cohen et al., 2025). Teachers from across the United States were recruited to participate via multiple recruitment strategies. Teachers invited their students to complete surveys (via RedCap) during one class period, and students completed surveys (or opted out) after completing electronic assent/content forms. The study was approved by the Institutional Review Board at the Wake Forest University School of Medicine.
Participants
Our analytic sample included 1,286 students (mean age = 14.56) from grades 6 to 12 (see Table 1 for demographic data) who participated in the study between fall 2021 and spring 2025. Participants self-reported their race/ethnicity as one or more of the following options: White; Black or African American; Hispanic, Latinx, or Spanish origin; Native American, American Indian, and/or Alaskan Native; Asian or Asian American and/or Pacific Islander and/or Native Hawaiian; Middle Eastern and/or North African; and Other. They also self-reported their gender as one of the following: man or boy, woman or girl, trans male/trans man, trans female/trans woman, genderqueer/gender nonconforming, nonbinary, or a different identity. For the purpose of analysis, given statistical power constraints, we reduced participants’ self-reported race/ethnicity responses into two categories (White or non-White) and did the same for participants’ self-reported gender (cisgender boys or girls and TGD individuals). This resulted in the following groupings: White boys (n = 238), White girls/TGD (n = 300), boys of color (n = 328), and girls/TGD students of color (n = 420).
Participant Demographics (Average Age = 14.54)
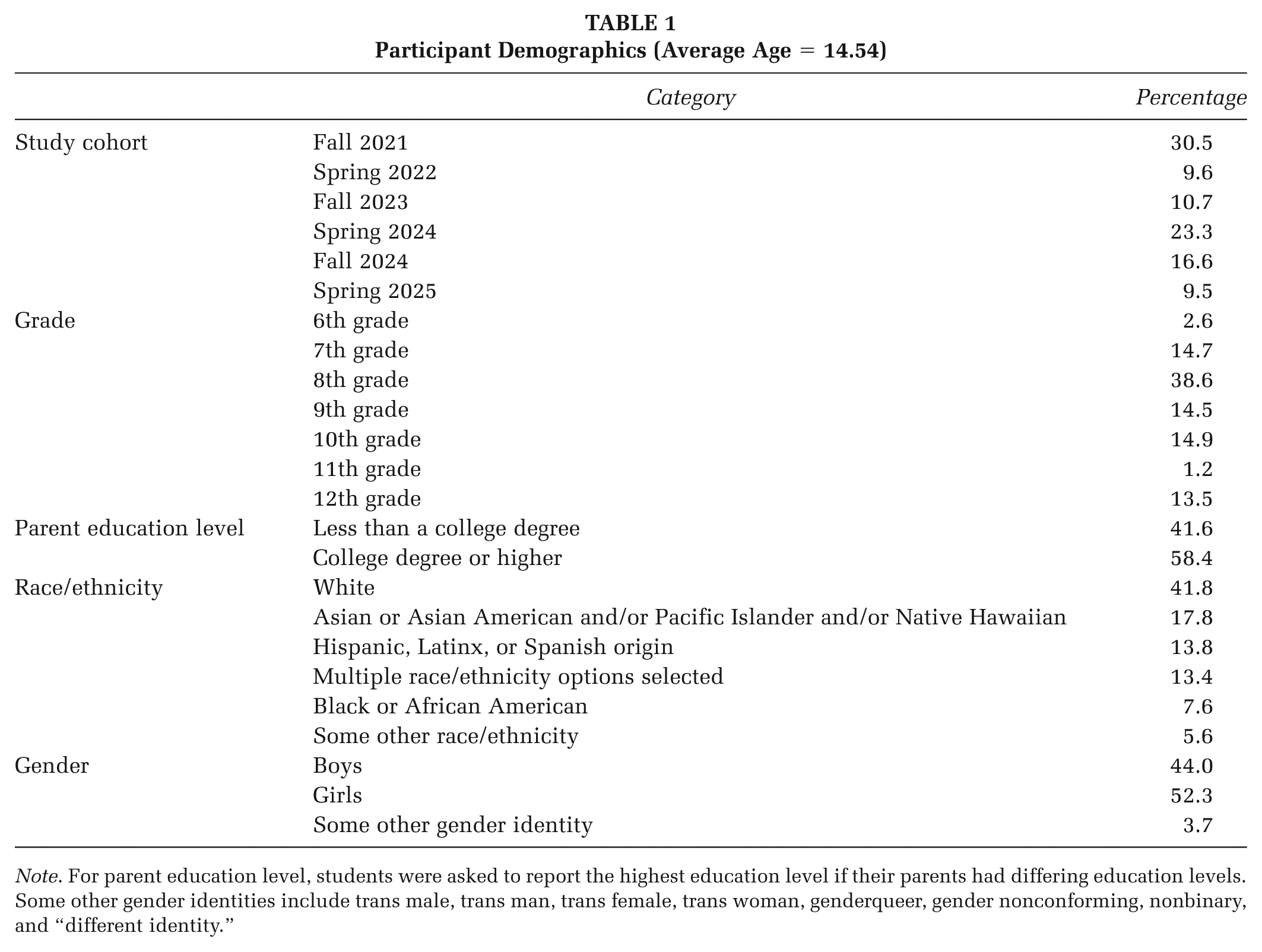
Note. For parent education level, students were asked to report the highest education level if their parents had differing education levels. Some other gender identities include trans male, trans man, trans female, trans woman, genderqueer, gender nonconforming, nonbinary, and “different identity.”
Measures
Additional information about Measures is available in Supplemental Materials Table 1.
Civic Behaviors
We measured three civic behaviors: volunteering, political participation, and discussion. Items for volunteering (three items, Cronbach’s alpha = 0.68) and political participation (six items, Cronbach’s alpha = 0.72) were adapted from the Youth Inventory of Involvement (Pancer et al., 2007); items for discussion (four items, Cronbach’s alpha = 0.88) were written by the study team. Students responded to all items on a 5-point Likert-type scale, ranging from 1 = Never to 5 = Very Often, after the question stem “Please rate how often you have participated in each activity in the past 3 months.”
Civic Attitudes
We assessed three civic attitudes. Sense of community (four items, Cronbach’s alpha = 0.82) was adapted from the California Healthy Kids Survey (Austin et al., 2010). Two items (Cronbach’s alpha = 0.65) captured participants’ motivation to influence (Ozer & Schotland, 2011). Civic self-efficacy was measured using three items (Syvertsen et al., 2015) (Cronbach’s alpha = 0.76). All items for civic attitudes were responded to on a 5-point Likert-type scale, ranging from 1 = Strongly Disagree to 5 = Strongly Agree.
Civic Skills
Civic skills were measured using three items adapted from Ozer and Schotland (2011) (Cronbach’s alpha = 0.67). Participants responded to these items on a 5-point Likert-type scale, ranging from 1 = Strongly Disagree to 5 = Strongly Agree.
Health Outcomes
Outcomes were each measured using a single item, adapted from the National Longitudinal Study of Adolescent to Adult Health self-rated health item (Codebooks, n.d.). The response scales for the health outcomes were a five-point scale from 1 = Poor to 5 = Excellent. The question for overall well-being was “In general, how is your overall wellness?” The other two questions were “In general, how is your physical health?” and “In general, how is your mental health?”
Analysis Plan
See Supplemental File for details about data cleaning, preparation, preliminary analysis, and model fit results (Supplemental Tables 2 and 3). For Aim 1, we fit a path model also using Mplus 8.10 to examine the associations between civic engagement (behavior, attitudes, and skills) and health (physical health, mental health, and overall well-being). We controlled for participant age, study cohort, and parent education level in the model. We planned to account for clustering by school using the TYPE = COMPLEX option in Mplus but could not due to model nonconvergence. All missing data were handled using Full Information Maximum Likelihood (FIML). Model fit was assessed using the same criteria as those proposed by Hu and Bentler (1999) for the multifactor Confirmatory Factor Analysis (CFA).
For Aim 2, we conducted the path model as a multiple-group mixture model, with the four demographic groups as a known grouping variable (KNOWNCLASS option in Mplus). We controlled for age, study cohort, and parental education level in the model and specified school as a clustering variable and used TYPE = COMPLEX to estimate adjusted standard errors. To assess the model fit of the multiple-group mixture model, we conducted a chi-square difference test to compare this new model with the model that includes only one group from Aim 1, which is nested within the Aim 2 model.
Results
Aim 1: Associations Between Civic Engagement and Health
Figure 1 presents the path model results examining the associations between civic engagement (behavior, attitudes, and skills) and health (physical health, mental health, and overall well-being).
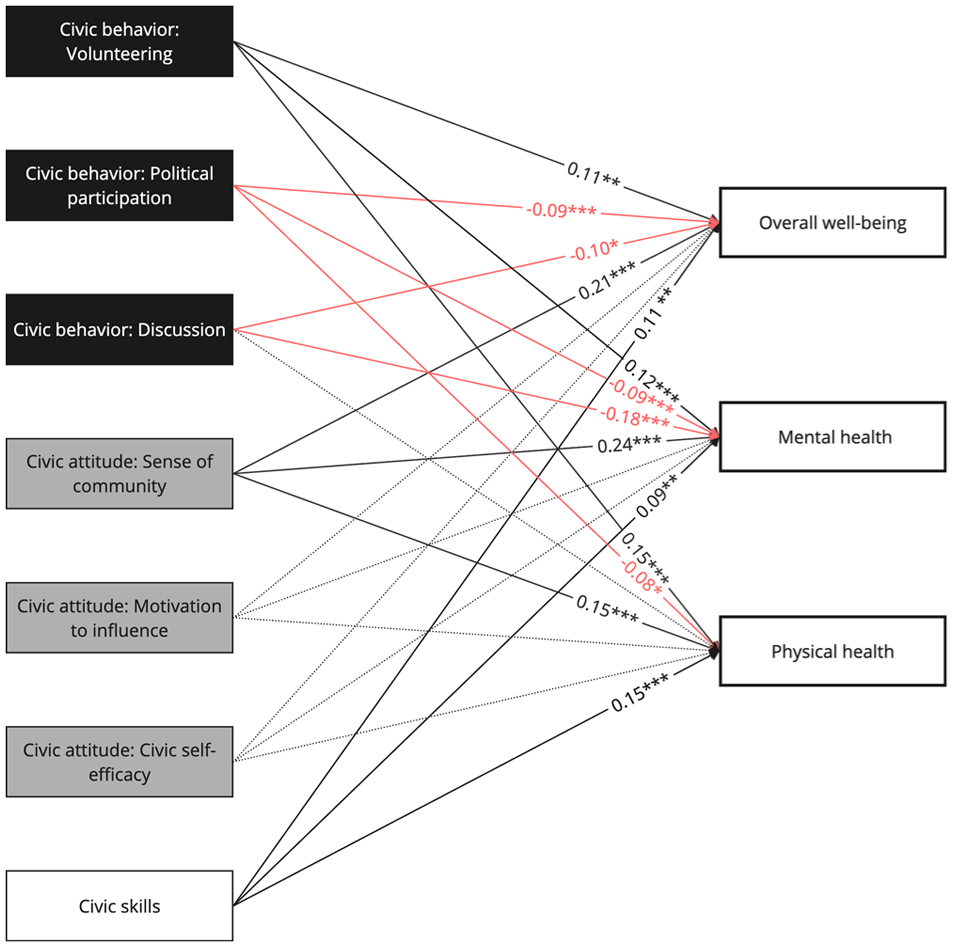
Results of Path Analysis Examining Aim 1
Civic Behaviors
Volunteering was positively associated with all three health outcomes (overall well-being [β = 0.11, p < .01], mental health [β = 0.12, p < .001], and physical health [β = 0.15, p < .001]). In contrast, we found negative links between political participation and health (overall well-being [β = −0.09, p < .001], mental health [β = −0.09, p < .001], and physical health [β = −0.08, p < .05]). Discussion-based civic behaviors were negatively related to two health outcomes (overall well-being [β = −0.10, p < .05] and mental health [β = −0.18, p < .001]).
Civic Attitudes
Sense of community was positively related to overall well-being (β = 0.21, p < .001), mental health (β = 0.24, p < .001), and physical health (β = 0.15, p < .001). Motivation to influence and civic self-efficacy were not associated with health.
Civic Skills
Civic skills consistently demonstrated positive associations with health (overall well-being [β = 0.11, p = .01], mental health [β = 0.09, p = .02], and physical health [β = 0.15, p < .001]).
Aim 2: Variations in Associations by Gender and Race/Ethnicity
We explored variations in Aim 1 associations for four demographic groups (White boys, White girls/TGD students, boys of color, and girls/TGD students of color) with a multiple-group mixture model (Figures 2 and 3, Table 2). The Aim 2 model provided a better fit to the data than the Aim 1 model (p < .001 for the chi-square test).
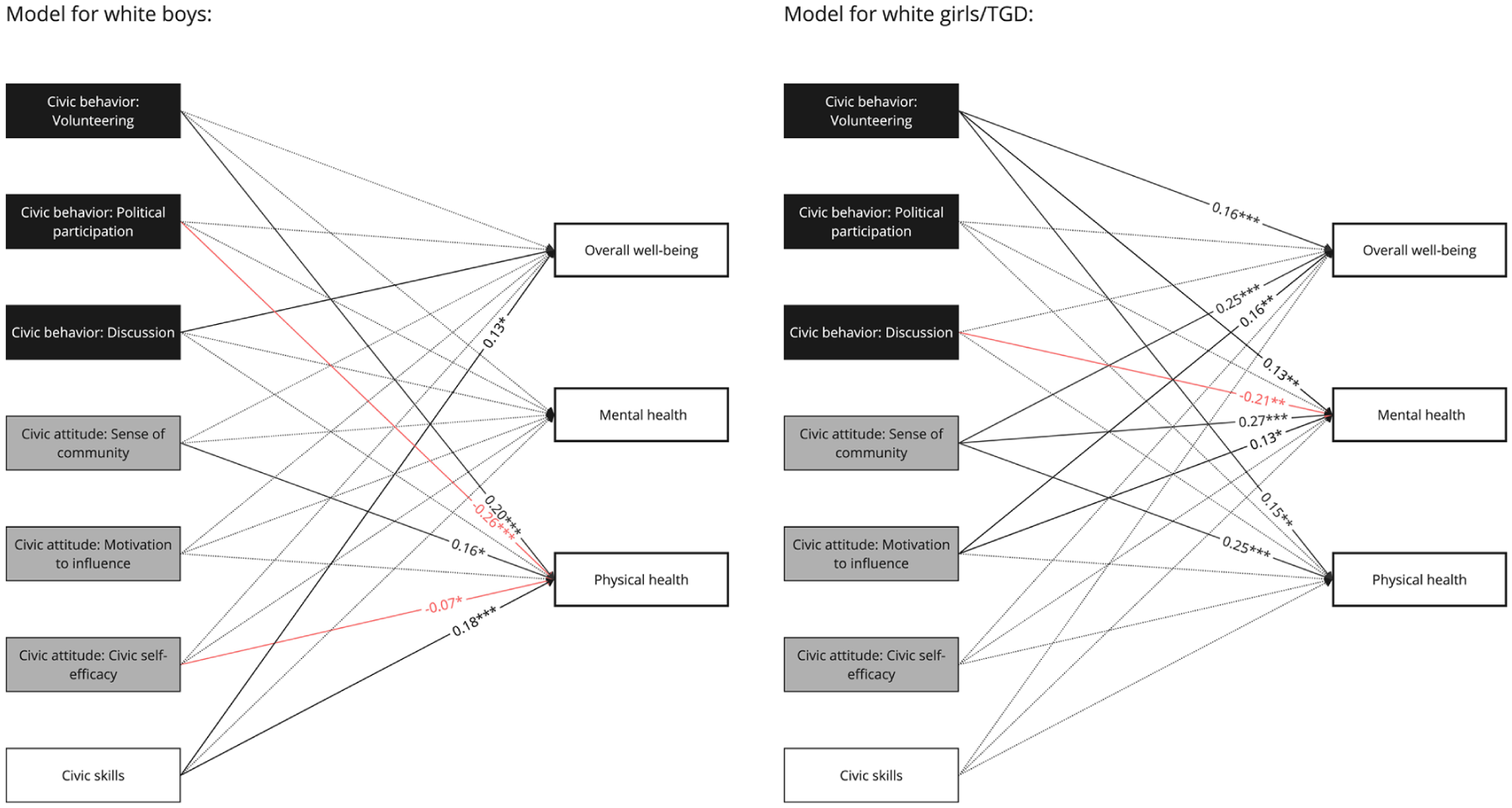
Results of a Multiple-Group Mixture Model Examining Aim 2 for White Boys and White Girls/TGD Participants
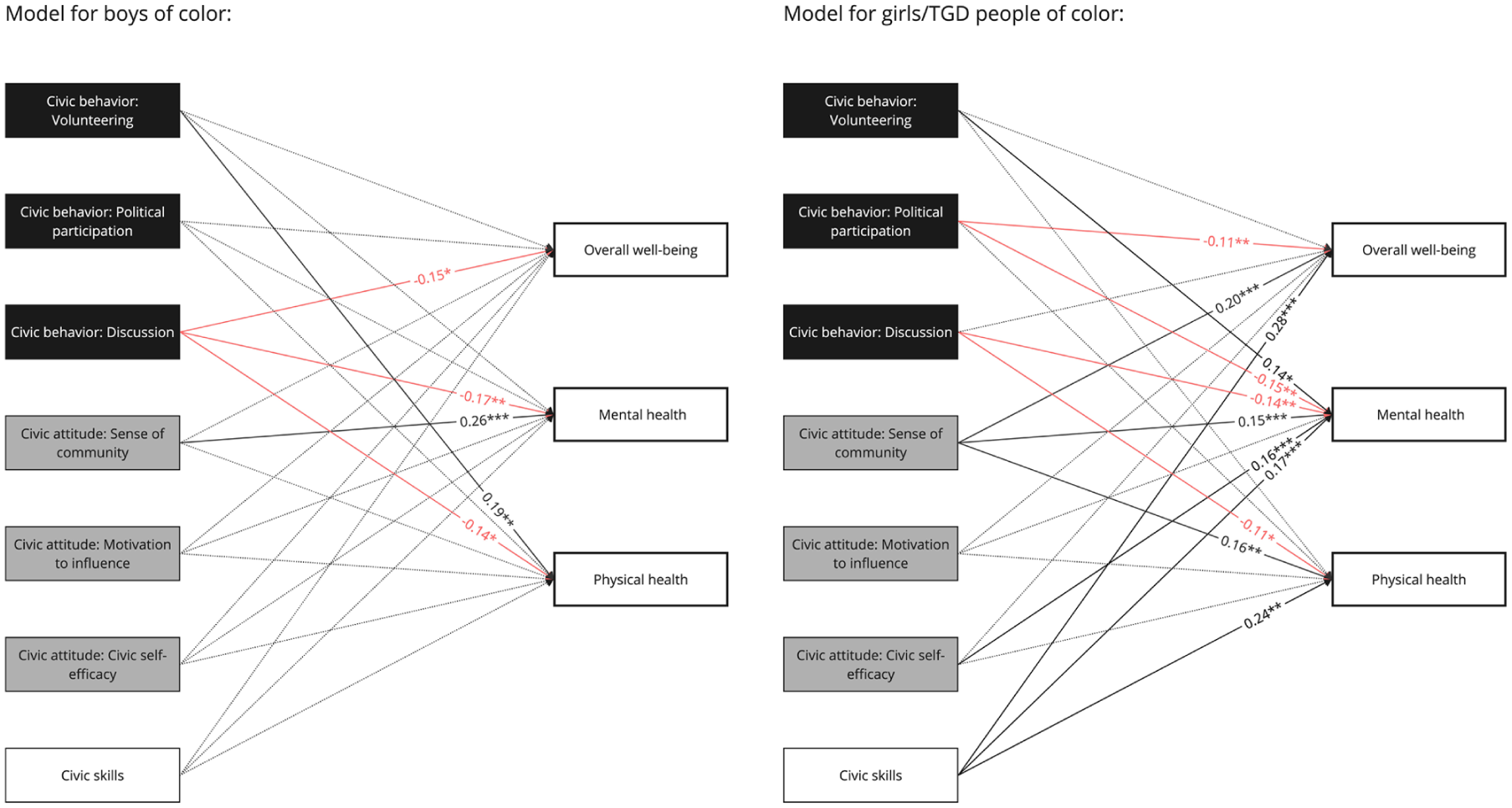
Results of Multiple-Group Mixture Model Examining Aim 2, for Boys of Color and Girls/TGD People of Color
Results of Multiple-Group Mixture Model Examining Aim 2
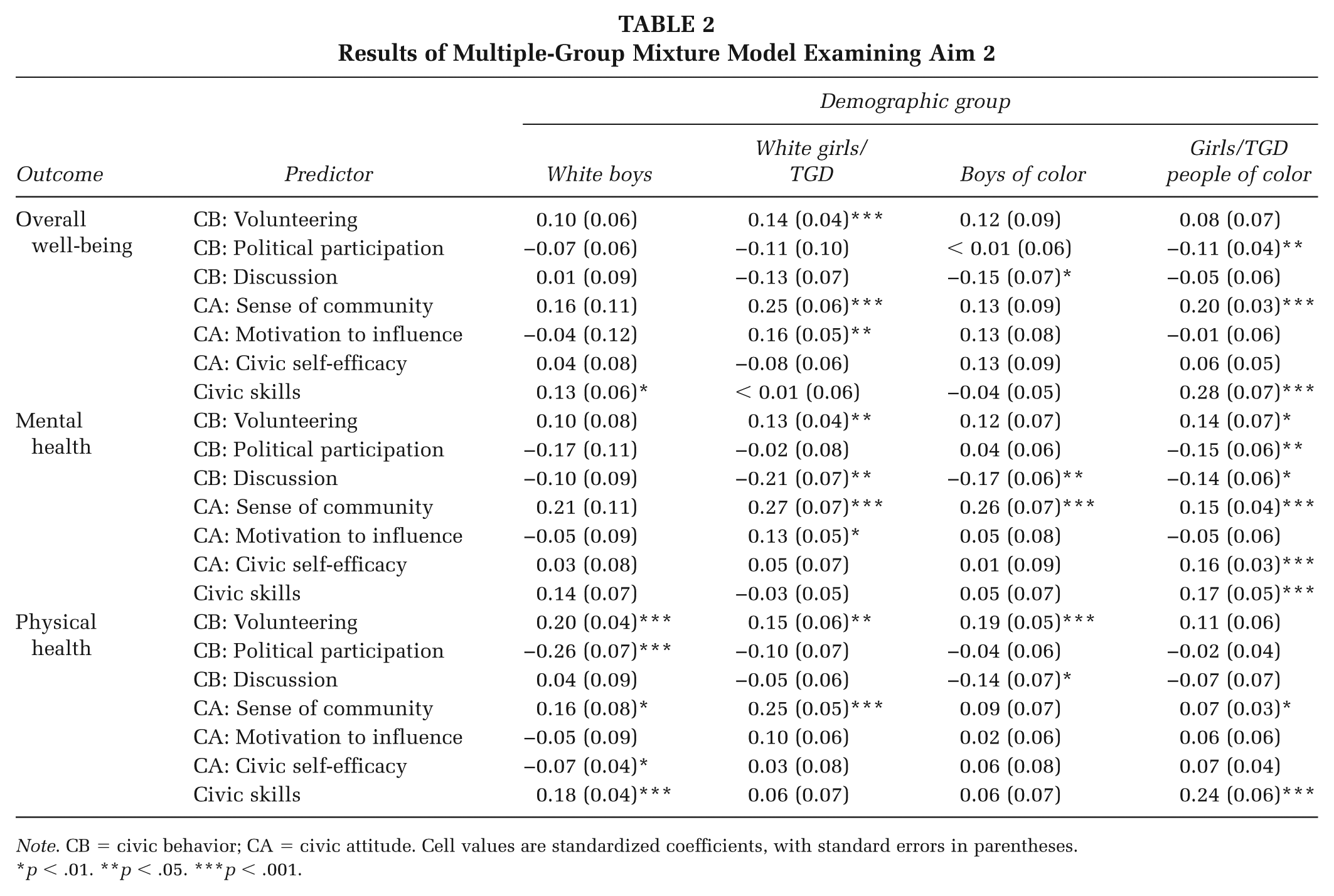
Note. CB = civic behavior; CA = civic attitude. Cell values are standardized coefficients, with standard errors in parentheses.
p < .01. **p < .05. ***p < .001.
Civic Behaviors
Volunteering was positively associated with all three health outcomes for White girls/TGD students (overall well-being [β = 0.16, p < .001], mental health [β = 0.13, p < .01], and physical health [β = 0.15, p < .01]). For both White boys (β = 0.20, p < .001) and boys of color (β = 0.19, p < .01), volunteering was only positively associated with physical health. For girls/TGD students of color, volunteering was positively associated only with mental health (β = 0.15, p < .05). Political participation was negatively related to physical health for White boys (β = −0.26, p < .001) and not associated with health outcomes for White girls/TGD students or boys of color. For girls/TGD people of color, political participation was negatively related to two health outcomes (overall well-being [β = −0.11, p < .001] and mental health [β = −0.15, p < .01]). Discussion was not associated with health for White boys. For all three other demographic groups, discussion was associated negatively with at least one health outcome: White girls/TGD students: mental health (β = −0.21, p < .01); boys of color: overall well-being (β = −0.15, p < .05), mental health (β = −0.17, p < .01), and physical health (β = −0.14, p < .05); and girls/TGD students of color: mental health (β = −0.14, p < .01) and physical health (β = −0.11, p < .05).
Civic Attitudes
Sense of community was associated positively with all three health outcomes for White girls/TGD students (overall well-being [β = 0.25, p < .001], mental health [β = 0.27, p < .001], and physical health [β = 0.25, p < .001]) and girls/TGD students of color (overall well-being [β = 020, p < .001], mental health [β = 0.15, p < .001], and physical health [β = 0.16, p < .05]). For White boys, it was only positively associated with physical health (β = 0.16, p = .031), and for boys of color, it was only positively associated with mental health (β = 0.26, p < .001). For White boys and both boys and girls/TGD students of color, motivation to influence was not associated with health. For White girls/TGD students, motivation to influence was positively associated with overall well-being (β = 0.16, p < .01) and physical health (β = 0.13, p < .05). Civic self-efficacy was negatively related to physical health (β = −0.07, p < .05) for White boys and positively linked to mental health (β = 0.16, p = .001) for White girls/TGD students. For boys of color and girls/TGD students of color, civic self-efficacy had no links to health.
Civic Skills
Civic skills were positively associated with overall well-being (β = 0.13, p < .05) and physical health (β = 0.18, p < .001) for White boys and with all three health measures for girls/TGD people of color (overall well-being [β = 0.28, p < .001], mental health [β = 0.17, p < .001], physical health [β = 0.24, p < .01]). Civic skills were not associated with health outcomes for White girls or boys of color.
Discussion
We examined how multiple aspects of civic engagement are related to health among a diverse sample of U.S. adolescent middle and high school students and found these associations varied by race-gender subgroup.
Civic Engagement and Health: Main Effects Across the Full Sample of Middle and High School Students
Overall, in the full sample, different civic behaviors had different weak associations with health. Specifically, volunteering was positively associated with all three health outcomes, while political behaviors and civic discussions were negatively associated with outcomes. This aligns with evidence that volunteering is positively associated with health (Lanza et al., 2023; Schreier et al., 2013) and departs somewhat from prior evidence with older samples that found positive associations for traditional political behaviors and negative associations between expressive and activist forms of civic behavior and health outcomes (e.g., Ballard et al., 2020). Our finding suggests that civic discussions are negatively related to all health outcomes, extending research that exposure to political issues can be distressing (Hoyt et al., 2018; Oosterhoff et al., 2022; Suzuki et al., 2023), perhaps especially if one is mostly engaged in discussion about potentially sensitive and complex issues without meaningful opportunities for civic action and connection with others.
The only civic attitude positively associated with all three health outcomes was the sense of community. These three associations were the strongest, suggesting that feeling a sense of community is robustly related to health; this aligns with evidence of positive associations between perceived social connectedness and health (Holt-Lunstad, 2021; Leigh-Hunt et al., 2017). Sense of community is a promising target for civic interventions to support healthy adolescent development. Interestingly, motivation to influence and civic self-efficacy were not related to health outcomes, while civic skills were positively but weakly associated.
Associations Across Sociodemographic Groups
The overall pattern of main effects, however, obscures more nuanced patterns of associations between civic engagement and health among sociodemographic subgroups.
Associations Between Civic Behaviors and Health Differ Across Subgroups
For volunteering, the White girls/TGD students subgroup had positive associations with all three health outcomes, with scattered positive associations for the other subgroups. A prior study found differences across race in the benefits of volunteering for hypertension; benefits were present for White but not for African American adults (Tavares et al., 2013). Future research can elucidate if and how gendered and racialized experiences may shape how volunteering relates to health, including whether there are differences in types of volunteering or volunteering experiences.
Political participation was negatively associated with health outcomes for White boys and girls/TGD students of color. Recent election-related studies have documented that civic events and participation were disproportionately experienced as stressful by racial/ethnic minoritized youth compared to White-identifying youth (Ballard et al., 2022; Hoyt et al., 2018; Suzuki et al., 2023). This topic merits further research to see whether our findings are replicable and, if so, elucidate potential explanations.
Political discussions were negatively associated with health outcomes for boys and girls/nonbinary students of color and White girls/TGD students; there were null associations for White boys. Political discussions may be experienced as less difficult for White boys, given that White men occupy a position of power in the United States (Liu, 2017). The context of civic discussions or the interaction of civic topics and contextual factors likely matter for explaining this finding (Graf et al., 2024); classroom civic discussions are not experienced in the same ways for young people across race and gender, with students of color often experiencing a less respectful and open climate than their White peers (Conrad et al., 2022). Teacher training interventions may be a promising approach to increase teachers’ skills and confidence in effectively facilitating civic discussions with students from varied demographic backgrounds (e.g., Bondy, 2025). During the study time period, civic and political topics dominating news coverage included racialized violence, reproductive health, and immigration policy; these are all topics with potentially heightened significance for people of color and women (Hahn, 2003) and which are often reported as stressful and difficult to discuss (Cornejo et al., 2022).
Associations Between Civic Attitudes and Health Differ Across Subgroups
Sense of community was strongly positively related to all three health outcomes for both girl/TGD student subgroups; scattered positive associations were also present for both boy subgroups. This finding is aligned with a body of evidence about social connectedness and health (Holt-Lunstad, 2021) and evidence that the sense of belonging is key to well-being when participating in civic programs (Conner, Greytak, et al., 2023).
Motivation to influence was positively associated with overall well-being and mental health for White girls but was null for all other subgroups. Future research is needed to replicate and understand this finding. While self-efficacy is generally thought to be an indicator of empowerment and found to be positively associated with health in prior research (Ballard et al., 2019; Maker Castro et al., 2022), this study found that perhaps this is not the case for White boys or any students of color but may be for White girls/TGD students. It is important to highlight that in this case, findings in opposite directions among subgroups explain the overall null associations in the full sample and underscore the importance of examining associations across meaningful subgroups.
Subgroup analyses also reveal an interesting story behind the full group positive associations between civic skills and health outcomes: this finding appears to be driven by White boys and girls and TGD students of color. For girls and TGD students of color, civic skills were moderately to strongly positively related to all three health outcomes, while they were unrelated for White girls and TGD students and boys of color. Two positive associations were present for White boys. Civic skills, in this study, measured as reporting a good understanding of political issues, feeling confident in communication skills with adults, and knowing where to gather information to solve problems, may be an especially important target for civic programs aiming to bolster the health and well-being of this group of adolescents (Maker Castro et al., 2024; Saavedra et al., 2024). This is a very important finding, especially in the context of other findings for the girls and TGD students of color subgroups, which revealed negative associations between civic behaviors (political behaviors and discussions) and health outcomes.
Limitations and Implications for Future Research
Several limitations should be noted. We had to significantly simplify racialized and gendered experiences. Given that subgroup analyses revealed a different picture compared to the full sample pattern of main effects, future research should employ subgroup analyses, ideally using robust measures of social experiences such as discrimination and marginalization to move beyond sociodemographics as proxies for complex experiences. In addition, research should apply an intersectional lens and analytic approach and examine heterogeneity within groups (e.g., different racialized experiences rather than the umbrella of all students of color and TGD adolescents separately from girls).
As with most studies examining civic engagement and health (Mužík et al., 2025), this study was cross-sectional and used self-reported health outcomes. Future studies should examine outcomes longitudinally, use health records or other objective data sources, and employ rigorous designs, such as randomized controlled trials, to clarify the causal nature of associations.
Implications for Practice
Acknowledging the complexity of school environments for civic development, we must monitor the changing political environment and identify tenable school-based civic interventions and additional promising contexts for civic interventions. While sense of community seems to be a powerful positive experience for all, civic interventions may yield stronger results when they target different mechanisms depending on student experiences. In a context of heightened partisanship and increased pressure on teachers and school districts, many teachers report feeling uneasy facilitating civic discussions (Stoddard & Hess, 2024). This is understandable; however, it is also problematic, as students must learn to discuss civic issues across differences. Practices, policies, and supports are needed for middle and high school students to engage in high-quality, critical, and respectful civic discussions.
Supplemental Material
sj-docx-1-hpp-10.1177_15248399261443235 – Supplemental material for Patterns in Civic Engagement and Health Among Diverse Adolescent Students
Supplemental material, sj-docx-1-hpp-10.1177_15248399261443235 for Patterns in Civic Engagement and Health Among Diverse Adolescent Students by Parissa J. Ballard, Sara Suzuki, Erin Manalo-Pedro and Alison K. Cohen in Health Promotion Practice
Footnotes
Authors’ Note:
The authors thank Grisel Trejo, Paul Wesson, Jason Fitzgerald, Wendy Morales, and Mark Wolfson for their contributions to the overall study. We are grateful to the participating teachers for the work they do in their classrooms, and we thank them and the students for participating in this study. The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by a grant from the Robert Wood Johnson Foundation under the Evidence for Action program (76972; 83343) to PI Parissa Ballard, Ph.D., and Co-PI Alison Cohen, Ph.D.
Materials and Code Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.