
Abstract
This study grew from a need identified by professionals working in the same community to explore interagency support for augmentative and alternative communication device implementation with students, families, and professionals involving the local school system and university. A case study was used to document intervention with a second-grade student who had developmental and severe expressive language delays. Based on the collaboration that was initiated between university and school corporation during the device acquisition process, it was determined that an interagency support system for this student would provide the best long-term solution for training, implementation, and maintenance related to her device. The participant’s intervention progress before and after intervention was described using tests and video interactions. Interviews with the principal collaborators (two speech and language pathologists) and the parent were conducted post intervention. Findings revealed positive changes in performance on the receptive and expressive vocabulary testing and scores on communication functions used based on video analyses before and after intervention. Spontaneous device use at home and school was, however, limited. As the study represented one case, no further statistical analysis was conducted. Finally, some reflections on the process were provided by the two main interagency collaborators as well as the mother of the participant, and implications for future intervention were discussed.
The amount and type of support for augmentative and alternative communication (AAC) device implementation are pivotal to successful AAC intervention (Soto, Müller, Hunt, & Goetz, 2001). However, even with support services from speech and language pathologists (SLPs), occupational therapists, and other education professionals within the schools, there are significant challenges ranging from uneven levels of expertise and experience in AAC intervention to limitations in time and lack of communication between team members (Dowden et al., 2006; Parette, Huer, & Brotherson, 2001; Stoner, Angell, & Bailey, 2010). The difficulties include high therapy caseloads, complex cases, long wait periods in acquiring devices, limited knowledge and experience in working with sophisticated communication devices, and limited opportunities for therapists to train teachers and paraeducators to ensure sufficient support for use within the classroom. The high level of skill required and intensity of AAC device implementation have also led to ongoing concern relating to the cost of AAC intervention (Parette & Marr, 1997). School districts are therefore faced with multiple challenges in considering personnel needs, workload requirements of SLPs and educators to address effectively the needs of students with AAC needs. The importance of a collaborative approach toward AAC intervention in schools is widely supported by administrators, team members, and families as they acknowledge the complexity of an integrated approach to intervention (Beukelman & Mirenda, 2005; Calculator & Black, 2009; Friend & Cook, 1992; Lave & Wenger, 1991). In spite of this realization, however, American Speech-Language-Hearing Association (ASHA; 2005) in the description of the roles and responsibilities of SLPs with respect to AAC pointed out that little information is available about the applicability of collaborative models of service delivery for individuals who use AAC.
Interagency Collaboration
Warmington et al. (2004) described interagency collaboration as more than one agency working together in a planned and formal way, rather than simply working together through informal networking. The purpose of collaboration is to develop an adaptive service between multiprofessional settings described as co-configuration, that is, a process in which agencies otherwise loosely connected are required to collaborate with young people and their families to develop forms of support over extended periods of time (Lloyd, Stead, & Kendrick, 2001). This process is described by distributed professional expertise (thus a shift away from compact teams) as well as the inclusion of more than just professional networks to include families and assistants who do not share the same common professional background or values. Co-configuration thus refers to the way in which teams realign themselves to partner with other agencies to ensure optimal service delivery. For example, teams do not need to share or meet at a common physical location as long as they are able to develop sufficient opportunities and strategies to exchange ideas and experiences. These interactions also do not need to include all team members each time but need to be structured (configured) to meet the needs of the clients. This type of association has encouraged a shift away from the concept of teamwork to knotworking. The term knotworking refers to “a rapid changing, partially improvised collaboration of performance between otherwise loosely connected professionals” (Warmington et al., 2004, p. 2). It is therefore a more dynamic association between agencies based on current service needs and skill requirements. Team members are able to reconfigure (i.e., creating knots) with different team members to more effectively address the changing needs of the clients and their families. Traditional Individualized Education Program (IEP) teams in schools tend to be less flexible. In the current study, the agencies involved were a university speech and hearing clinic, a school district (primary intervention contexts), as well as a researcher from special education who was involved to facilitate data collection and report outcomes.
Activity theory (Vygotsky, 1986) was used as a basic model for collaboration in the current study as it focused on the object of the activity system, that is, the case study as a means to learn in practice. Activity was aimed at promoting expansive learning, that is, to strengthen the ability to reinterpret and expand understanding of the object (case in context) among professionals and service users (parents and child). Figure 1 describes the nature of the activity model as applied in this study.
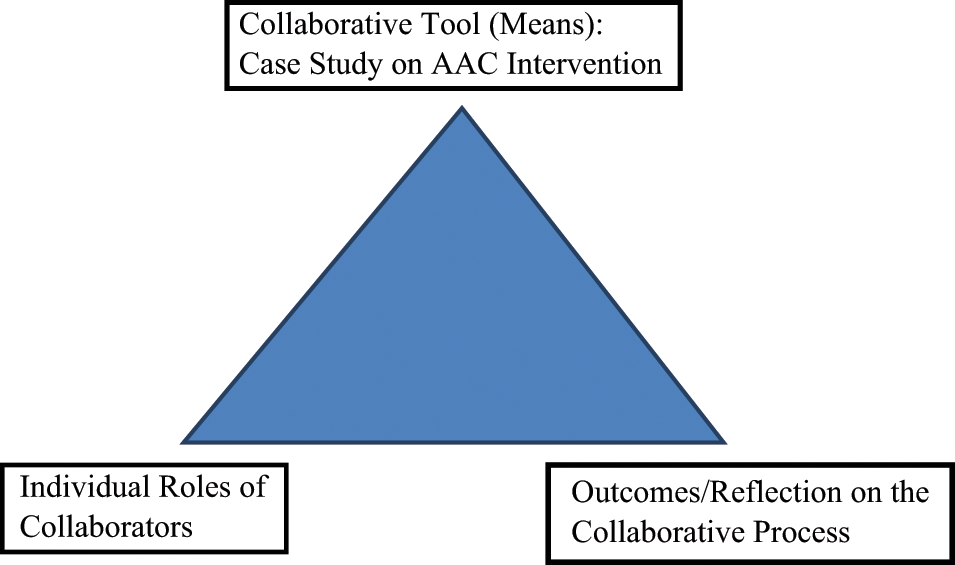
First generation activity model (Vygotsky, 1986).
The collaborative model used in the study presented with three components of an activity system. The first component refers to the individual roles of the collaborators, that is, the SLP at the university, the SLP and intervention team in the school district, and the researcher at the special education program at the university. The SLP at the university was primarily responsible for the acquisition of the device through Medicaid, for the provision of direct therapy services to the child, and to provide parent consultation and training. The SLP working in the school district provided direct individual therapy services to the child, small/large group therapy services in the classroom, and training to classroom personnel. Both therapeutic settings thus worked in a complementary way to provide therapeutic exposure to the student and family to intensify the AAC intervention process. The researcher was responsible for the data analysis of tests and interviews as well as reporting on the collaboration process. The second component related to the collaborative tools, the means through which interaction occurred, for example, frequent meetings between collaborators to plan intervention and reflect on the process and data recording of the process. The third component referred to the outcomes of the process that can be described in terms of the outcomes of the intervention for the child and family as well as the reflections of the intervention team in relation to the feasibility of the collaborative process.
This case study described the process and outcomes of an interagency collaboration between a university and a public school district. The aim was achieved through two sub-aims: first, by using intervention with a specific child to demonstrate the effectiveness of the collaborative intervention focused on extending the child’s use of different communication functions using a newly acquired communication device and second, by describing the process of collaboration as well as collaborators’ evaluation of the outcomes and challenges of the process.
Method
A case study design was used to document the participant’s intervention progress across home and school settings. Two SLPs (the main intervention collaborators) coordinated training, implementation, and maintenance of the device across both settings. In accordance with the aims of the study, data were collected on two levels: First, pre- and postintervention measures were taken to describe progress related to changes in the participant’s communication skills after a 3-month treatment period. Second, the reflections of the primary collaborators as well as those of the mother were described. This strategy for data collection was selected in accordance with the nature of the interagency collaboration that was based on the university clinic setting interacting with the child and parent in supporting operational competence versus routine intervention at school focused on linguistic, social, and pragmatic competence. Minimal additional demands were made on school personnel’s time except for the interaction between primary collaborators (two SLPs and researcher).
Participant
The participant (D) was a second-grade girl who initially used low tech. She was in a self-contained classroom for multiage students with significant disabilities, and had developmental and severe expressive language delay with chronic lung and vision problems. Other descriptive data and pretesting included the Peabody Picture Vocabulary Test–Third Edition (PPVT-III; Dunn & Dunn, 1997) standard score of 40 (preintervention) and an Expressive Vocabulary Test (EVT; Williams, 1997) standard score of 40 (preintervention). As neither test was standardized for children with little or no functional speech, only standard scores were reported. A subjective rating of her speech intelligibility before intervention was rated on a 1- to 4-point scale: 1 (not at all intelligible), 2 (emerging intelligibility), 3 (intelligible most of the time), and 4 (always intelligible) by the school SLP and teacher. In spite of poor intelligibility, her primary mode of communication was verbal. She was willing to engage in interaction and was able to use two- and three-word utterances, which were frequently supplemented by the use of pointing. She also used manual signs sporadically that were reminiscent of previous learning experiences. The decision to provide D with a DynaVox V-Max device was made by the two primary collaborators in interaction with the parents after an initial evaluation conducted in the university setting. This evaluation included a test to evaluate D’s abilities to locate symbols on a 40 location overlay and practice using available university devices, that is, Mighty Mo (DynaVox) and Springboard Lite Prentke Römich Company (PRC). The decision to acquire the DynaVox V-Max was based on D’s unintelligibility and motivation to interact with others prior to the decision to document the intervention process. Intervention goals were aligned with the child’s IEP goals, that is, to facilitate the development of her communication skills by expanding her ability to use different communication functions (see the appendix). IEP goals were written to reflect expressive and receptive language skills that were not device specific per the regulations of the school district, for example, D would use multimodal communication (e.g., voice output device, pictures, signs, vocalizations) to answer 10 different wh- questions correctly 5/5 times across 2 data days. In addition, mode of communication was left out of the school goal to allow for all of her communication modalities to be honored because the educational team had noted an increase in verbal communication.
Collaboration Team
Mother: D’s family included a mother, a father, and four siblings ages 15, 12, and 9 years. The mother did not work outside the home and was a collaborator in the project.
Primary collaborators: Both SLPs were licensed with the ASHA. The school-based SLP had 8 years experience and the university-based SLP had 13 years experience. These therapists had been collaborating with several clients and therefore had a relationship prior to the study.
The special education researcher, an AAC specialist at the same university, was new to the university and school district but had spent time observing, meeting, and consulting in the school district with both SLPs for 6 months before the start of the intervention study.
Coders: Two SLPs were involved in the coding process. They were aware that the purpose of the study was to describe the communication interaction of the child but were blinded to the pre- and post phases of the study. Agreement between coders is reported in Table 1.
Means of Preintervention and Postintervention Results on the Modified INCH and Interrater Agreement.
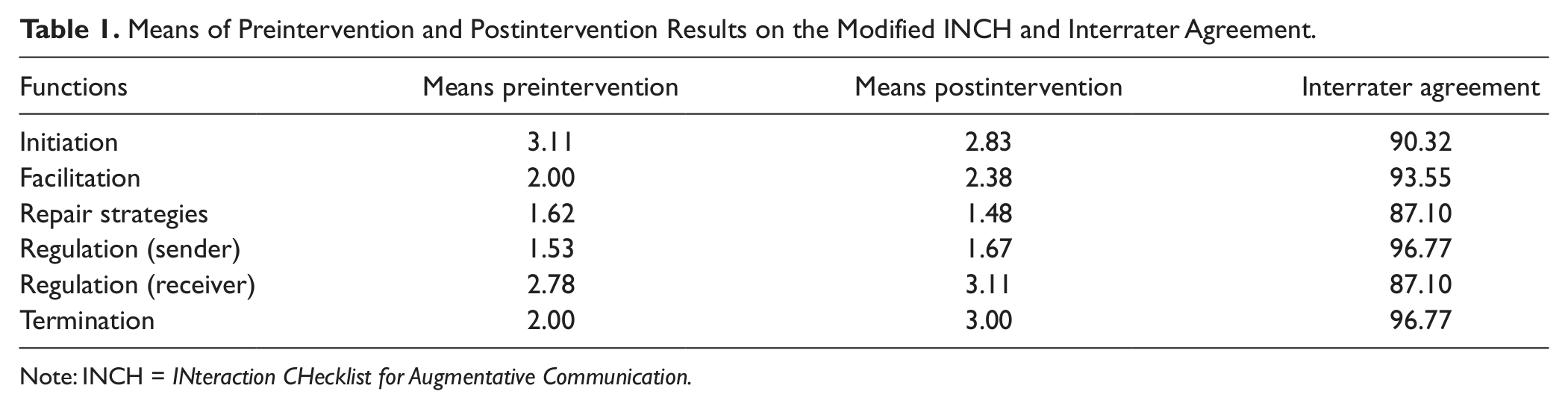
Note: INCH = INteraction CHecklist for Augmentative Communication.
Equipment and Material Used for Analysis of Data
The participant in the study used a DynaVox V-Max using Gateway 40. Gateway 40 addresses the needs of children chronologically between 3 and 12 years, whose receptive skills fall somewhere in the 30- to 60-month range. The expressive performance of these users could range from the use of two- to three-word telegraphic sentences to the use of syntactically correct sentences. The main page was arranged in a modified Fitzgerald key format, with links to words from a variety of grammatically organized categories. This gave the child consistent access to the core vocabulary without needing to navigate from the main page.
Recording equipment included a flip video camera (Insignia 3" liquid crystal display), which was used to record interactions with the client in the home and school settings. An audio recorder (Sony ICD-PX720) was used to conduct a postintervention interview with the mother. Transcription of the interview was done using a downloadable software package, Express Scribe. Tests used included the PPVT (Dunn & Dunn, 1997) and the EVT (Williams, 1997). Only standard test scores were used due to lack of standardization on children with little or no functional speech. The analysis of the video recordings was conducted using a rating scale based on frequency of use (1 = never, 2 = seldom, 3 = frequently, 4 = most of the times/always) and items identified in the INteraction CHecklist for Augmentative Communication (INCH; Bolton & Dashiell, 1984). INCH was used as a basis for the development of the coding of communication functions. Please see the Data Recording Sheet used by the coders in the appendix.
Intervention and Collaboration Process
Research activities commenced after approval was obtained from the Institutional Review Board (IRB) of the university. The director of special education provided approval for the project and was supportive in exploring an interagency collaborative process. Parent approval was obtained as part of the IRB process. Meetings between all three collaborators (two SLPs and researcher) were held approximately every 2 weeks during the initial acquisition and intervention periods with at least one face-to-face contact during subsequent months to monitor intervention progress. Frequent Internet contact was maintained throughout the process. Meetings focused on sharing information on the progress of intervention goals in the school and university contexts as well as identifying challenges that needed to be addressed.
Intervention: University context
The participant received treatment twice a week at the University Speech and Hearing Clinic for 45 min each. Target objectives were to familiarize the participant with the navigation of the device by using verbal direction during structured practice sessions. These sessions included use of the device during conversation (i.e., talking with the therapist about her family and friends), making requests (i.e., “I want . . .,” “I need . . .”), and making comments (i.e., “I see . . .,” “I have . . .”). The SLP used different activities based on D’s interest, for example, dressing paper dolls by requesting different pieces of clothing, teaching food-related locations by using miniature toys pulled out of a bag, and telling what she had in her hand. When D produced an utterance on the device, the SLP responded by way of conversation, for example, by stating her own likes and dislikes of the specific food to encourage further device use. Parent training was supported through observation of the treatment sessions by the participant’s mother and nurse (who accompanied the child during the day), and through specific time allotted before and after every 45-min treatment session (typically 10 min in duration in both cases). Meetings before sessions focused on whether and how the device had been used at home between sessions and problem solving any specific issues the family encountered with functional use, programming, and so on. Meetings after sessions were used to provide the parent with homework assignments, with verbal directions provided in conjunction with printed directions. These homework activities were aimed at facilitating use of the device at home (e.g., using “I want” and “clothing” to allow the participant to pick out what she wanted to wear or using “I go” and “places” to allow the participant to ask to go somewhere). The participant demonstrated the ability to navigate the V-Max early on in therapy and was creating novel utterances by the third session (e.g., “I like shopping”).
Intervention: School context
The participant additionally received intervention once a week at her elementary school. Individual therapy sessions with the child were conducted in her special education classroom. These sessions were aimed at improving D’s use of the device in answering questions, and providing comments and expansions based on the content of a storybook, a structured activity (e.g., art project), play situation (e.g., Legos), or engaging in communication exchanges with the educational team. In addition, the SLP visited the classroom of the student once a week to assist the teacher and paraeducators in using the device. This intervention focused on the use of the device during calendar time in the class and a structured art activity. As the SLP had limited time (30 min, once a week), time was distributed among direct intervention with the student, observation of the student working with teaching staff in a one-on-one work session, small group work, and in the general education classroom collaborating with the special education and general education teacher to create opportunities to use the device in both settings. The SLP provided feedback and ongoing training to the paraprofessional, collaborating with the research team, and provided some guidelines for the programming of the device.
Device programming
Conversation was targeted during initial sessions using the About Me, Family, and Quickfire locations on the main page. Requests and comments were targeted using the Gateway 40 location, which gave the participant access to pronouns (e.g., “I”) and a variety of verbs (e.g., “want,” “need,” “like,” “feel,” etc.) that she could use to build phrases. Specific category locations were trained using specific games/activities that would require category-specific vocabulary (e.g., combining “I want” with the category “clothing” to request clothing items to dress paper dolls). It should be noted that during initial sessions, training was also focused on general navigation of the device using the functions of clear and go back by using verbal direction and visual cueing.
Some initial programming was done by the university SLP to ensure easy access to highly motivating content, for example, the names of the participant, family members, and her pet cat. For the main part, however, intervention within the university and school setting was focused on assisting the student to access existing vocabulary in the device. The parents were encouraged to familiarize themselves with the Gateway 40 framework before adding their own vocabulary to avoid duplicating already existing vocabulary. They, however, preferred to program in their own information by typing monologues per button to provide the school with news content that D could share during relevant school interactions.
Collaboration process
Phase 1—The decision making and acquisition of the device began with an initial assessment through the university clinic. When the participant demonstrated the ability to use a high tech AAC device during assessment trials using a variety of devices, the parents were provided with printed information and website locations to investigate a variety of AAC devices by the SLP. They were requested to investigate and compare the devices in terms of their affordability, ease of use, portability, and flexibility in accommodating their daughter’s changing academic and communication needs. The school SLP provided additional information to the parents and researcher about what had previously been used in the school setting (primarily low tech picture communication symbols on a communication board, and the “Go Talk” using 9 and 20 location overlays to answer “wh” questions and to facilitate making comments in class). She additionally noted that she was most familiar with DynaVox AAC devices. Feedback from the parents (based on their personal research) supported the decision by the school and university SLPs that the DynaVox V-Max was the preferred device. The university then completed and submitted a speech generating device acquisition report/request through Medicaid.
Phase 2—the 3-month intervention phase—included structured meetings between the collaborators approximately every 2 weeks after school for 1 to 1.5 hr. During these meetings, information was shared on two topics: first, D’s progress in using the device during therapy sessions as well as in the class context and second, D’s difficulties in keeping focus during sessions. Specific content discussed during meetings included how to better guide the parents and paraeducators to use the device with the participant during interactions, how to better support the classroom teacher, and how to address programming challenges that arose during the course of intervention.
Data Collection Strategies
Pre- and post measurements included testing as well as analysis of video footage of interactions. Measures of receptive (PPVT-III) and expressive (EVT) vocabulary were administered pre- and post intervention. Video footage was taken of the participant interacting with a variety of individuals at home and school pre- and post intervention to assess the participant’s interactive behavior. Eight preintervention and six postintervention interactions were recorded at home, and four preintervention and four postintervention interactions at school. Each of these lasted between 5 and 12 min. No specific request was made for individuals to include the device post intervention to allow participants to use communication strategies of their choice. Three preintervention and three postintervention interactions were randomly selected for purposes of analysis. Preintervention interactions analyzed included an interaction with the mother during dress fitting, an interaction with her father while in the car, and a book reading interaction with the school therapist. Postintervention interactions included a coloring interaction with the school therapist (device was used), a computer interaction with her older brother at home (no device), and a conversation with her mother (with device). Video clips of before and after intervention were randomly presented for coders to reduce bias in analysis of preinteraction and postinteraction data. These interactions were analyzed using a rating scale based on the items of the INCH (Bolton & Dashiell, 1984) developed for this purpose (see the appendix).
Primary collaborators were asked to submit written individual reflections of their perceptions of the collaboration process to the researcher at the end of the intervention process. In addition, an interview was conducted with the mother of the participant to obtain her reflections on the intervention process. Questions posed included the following: How would you describe the intervention provided by the university and the school? What were the advantages of this collaboration for your child? What advantages can you see from this type of collaboration for parents of children with severe communication problems? What do you think could be the disadvantages of this type of process? These reflections were analyzed by the researcher and the themes checked for reliability by the SLPs involved. Final categories were based on consensus.
Analysis and Conformability of Data
Descriptive data of central tendency (means and median) were used to describe the intervention outcomes before and after treatment. The video analyses of the interactions with D were conducted by using categories included in the INCH (appendix), which were rated on a 4-point scale (1 = seldom to 4 = always). A subjective rating of intelligibility (Dowden, 1997) was done on a 4-point rating scale (1 = poor, 4 = always intelligible). Interrater agreement (three raters) for the observation of communication skills on the video ranged between 87% and 97% (Table 1.). As this study represents one case, no further statistical analysis was conducted.
Findings and Discussion
Findings are presented in two tiers. First, the effectiveness of the intervention is described by presenting pre- and postintervention data of the child’s communication behavior. Second, a critical evaluation of the interagency collaboration is presented as reflected in feedback received by the two main interagency agency collaborators and an interview with the mother.
Preintervention and Postintervention Results
Increased test scores were evident on the PPVT (pre = 40, post = 66) as well as EVT (pre = 40, post = 47), respectively. These raw scores were used to monitor progress in the absence of any standardized assessments available and suitable for this population. Table 1 describes the communication ability of the participant before and after intervention as well as the interrater agreement on the rating of the specific categories. There was also an increase in the mean number of interactions before and after the introduction of the device (before: 2.07, SD = 0.95; after: 2.17, SD = 0.97). As this study only represents one case, no further statistical analysis was conducted on these measures as well as the data obtained by the INCH in Table 1.
Although less initiation was observed after intervention, the client tended to make more effort to facilitate interaction and needed to use fewer repair strategies. The decrease in repair strategies could suggest that communication partners had less difficulty understanding her post intervention. As the rating of the participant’s intelligibility remained unchanged (mostly 1 = poor or 2 = emerging according to the appendix) before and after intervention, this slight change could likely be attributed to the use of the AAC device. Regulation activities in the sender as described in the appendix (e.g., alerts receiver when more time is needed for composing, shifts topics smoothly, uses pauses, maintains interest, and gives feedback when not understood) as well as receiver role (e.g., the use of eye contact to indicate attention to sender, indicate understanding of message and stays on topic consistent with place, role, and social situation) also indicated a higher frequency of use. Termination activities (e.g., uses farewells and indicates when finished with message) also increased, which might reflect heightened awareness of the interaction context.
Although the possibility that these changes could be attributed to the nature of the interaction or messages practiced on the device cannot be ruled out, it seemed highly unlikely. No repetitive responses that could be a result of device practice or training were evident in these interactions. The parent and school SLP were also asked to submit naturalistic interactions with the participant for potential preintervention and postintervention analyses.
Data from the observations and testing do indicate some increase, albeit small in the communication skill of the student. The class teacher and SLP in the school also observed that there was an increase in spontaneous speech. Her length of utterance was most frequently one word, although two- and three-word combinations were observed. Her production at the single word and two- and three-word combination levels was often unintelligible (especially to unfamiliar listeners) and broke grammatical rules. When using her device, D was observed to combine up to four words (e.g., I want red marker) during structured teacher-directed activities. Often an initial verbal prompt was needed, which could be faded quickly once D understood the expectation of the activity. During unstructured activities, D attempted to communicate verbally first. When visually cued to use her device, she most frequently used one-word utterances.
There was little evidence of spontaneous device use. The mother as well as the school SLP reported inconsistent use of the device in home and school contexts. The mother confirmed that D mostly used the device for clarification purposes at home. The school SLP and the teacher also reported a lack of use of the device in general classroom interactions. Two main issues could have contributed to the limited device use:
The appropriateness of device selection for D can be questioned. The ASHA (2005) technical report on AAC roles and responsibilities of SLPs highlights the principles of valid assessments and the importance of ecological sensitivity in the selection of AAC strategies. In addition, the need for capability assessments as well as feature matching is described. These AAC assessment processes require well-trained SLPs and special educators who are able to integrate different components of the assessment to guide device selection. A shortage of professionals (SLPs and special educators) with skills in AAC implementation is, however, well reported in schools (see, for example, Ratcliff, Koul, & Lloyd, 2008, and more recently, Anderson, 2012). As this client was ambulatory, the choice of a V-Max might not have been the best match. However, at the time of the intervention with D, iPads were not commonly used in schools and software applications were very limited in scope.
Underestimating the time investment and skills required to reach some level of proficiency in using the device also contributed to hesitancy in using the device within daily settings by parents and school personnel.
Reflections on the Collaboration
As a final stage in the collaborative process between the university and school district teams, the reflections of the two SLPs were provided, followed by comments from the interview with the mother after the initial intervention period. As far as the process and the outcomes of collaboration were concerned, both SLPs experienced them as mostly positive that is evident from the following comments:
I see real potential and benefit for having an active collaborative relationship between [the university] and [school district]. Although this study specifically targeted one student in the [school district], it illuminated the areas where an interdisciplinary model could strongly benefit both students and professionals in the local community.
I think we all learned that we work well as a team. Though we may have felt that our specific agencies could have done more, we still accomplished a lot in a short span of time, and certainly proved that interagency collaboration can accomplish more than work as an individual provider. . . I think this was a good start, and look forward to where this takes us in the future!
Although both SLPs felt that there had been a positive outcome, the school SLP also acknowledged the need for better support in the natural environment of the student:
Collaboration is critical, so is treating in the natural environment. I believe that proceeding forward, it may be helpful for this interdisciplinary team to think about more creative ways of training/treating students with newly acquired devices. Although the one-on-one clinical setting is very important for skill acquisition and practice, practice and learning must also take place in the environments where the student will be using the device the most. The other huge piece is a better training of the school staff and parents.
Both SLPs acknowledged gains made in intervention as the student has shown some increased skills. Although the student did not use the device as frequently as collaborators had hoped, the additional intervention within both settings contributed considerably toward the student’s confidence in engaging with other students in interaction. Teacher and paraeducators commented on the participant’s increased willingness to engage with other students and a notable increase in her verbal communication. Shortcomings identified in the implementation revolved around too few and too fragmented training opportunities in working with school personnel and the parent. Although considerable time was spent with the participant in assisting her to gain access to the vocabulary on the device, carryover of the use of the device for communication purposes was limited. This could reflect on the need for more extensive partner training to facilitate the use of the device in interactions. The school therapist acknowledged this by stating,
Finally, as our school district moves forward with an ever decreasing budget, we need to think creatively about how we can still provide the same level of service with less money for materials, less staff, larger caseload sizes, more responsibilities, and less time. Many of these factors contribute to the lack of success that is often seen with AAC device users in our district. Because of this study, the team has identified how we, as a team, can work together to support not only the students, but the parents and professionals involved.
A separate interview was also conducted to obtain information about how the mother viewed the process and outcomes of the collaboration, and her recommendations for future collaboration. The mother was particularly positive about the process of collaboration between the university and the school system in obtaining the device.
Well, I got to tell you, for me it was a wonderful thing because they handled it all. It was going through X [clinical faculty at the university]. I believe she also had a hard time getting it—approval for it . . . They were extremely helpful.
Because Y [therapist at school] was associated with the university, it was fabulous because she had ties with the university . . . and everything at the school went as well as it can, given what they have to work with.
She stated that she took D to the university where she received therapy for one semester twice a week. “I think it was exactly what I expected . . . it was good.” However, the mother continued by identifying the difficulties involved in the use of the device in therapy.
Did they also guide you [as a parent] in the use of the device at this point?
Yes they did, but it is tough on everyone. They only use the device for the 1 hr that they had D and that was it. So, they would get it, and it takes time, and I think that is what they are experiencing at school too.
I felt bad for everyone involved because it . . . the students [speech and language] didn’t have time with the device and . . . you know, every kid turns up with a different device and every device is programmed different and that’s just crazy.
She continued to elaborate on the difficulties experienced in using the device within the school context:
I think they have tried to incorporate it to the best of their ability and time constraints. We all went in thinking this will be great, we can do this, we can make it work. And as time progresses what I see as a parent is that it is just not that easy.
The mother largely attributed the difficulty in device implementation at home and school to the lack of sufficient liaison between school and home in relation to device programming and use.
Because like E [her husband] pointed out to me: On any computer, if you don’t know where someone is storing a file, it is like looking for the word Physics in the F section of the dictionary. You are not going to find it unless someone is going to tell you: “You go here and here.”
When asked to reflect on how this aspect can be better addressed through an interagency, collaborative approach, the mother stated,
If there are student teachers or therapists and they have to complete those types of internships, is there some way where they will spend an entire day with a child with an AAC device and be in charge of making sure the parent knows what is done, the child knows and the teacher knows? Because Mr. R [teacher] does not have the time and he doesn’t have access to the computer [device].
So what you are saying is that the university can have a stronger hand in helping with the programming and use of the device?
Programming and helping a child use it within the classroom on a day to day basis.
The interview with the mother largely confirmed the comments made by the two primary collaborators:
I cannot help but think of how we, as the school team, fell short. From the school perspective, I think that I would have front loaded the majority of my time in staff training and creating a more solid plan for implementation. Our subject was not able to retain and generalize the skills from the IU Clinic. For this reason, I believe that I could have focused my energies in a way that would have better ensured device use at school when I was not present in the classroom instead of spending those initial weeks exclusively working with her in a 1:1 work format.
In my setting, I see the need for more parent training—perhaps a home component and additionally having the parent sit in on some sessions to learn and interact with their child, and involvement in the school setting if possible [potentially providing extra support/training to the teacher and paraeducators in collaboration with the school SLP]. Skills demonstrated in the university setting [e.g., conversation] were not always seen in other settings, and these aforementioned improvements could serve to bridge that gap.
The main challenge remained the transmission of knowledge about the programming and use of the device across different contexts. More instruction of parents, teachers, and paraeducators need to be provided to facilitate the use of the device in general interactions. The collaborators reiterated that the building of relationships between them was valuable in allowing them the opportunity to work together to address a variety of challenges in AAC intervention at home and at school. The specific roles for each agency have to be revisited to address changing needs for the participant, classroom personnel, and family. For example, the location of therapy should be within the school context to facilitate carryover. Training of the teacher, paraeducators, and parent also needs to be readdressed to facilitate common understanding of the role of communication within everyday activities and education of the participant.
Concluding Comments
This case study described gains and challenges experienced in providing AAC intervention with a young client using a sophisticated AAC device within a school district. It highlights the need for critical reflection on the assessment and intervention processes used by collaborators to address shortcomings in service delivery. The reflections on the processes and outcomes also confirm the need for more AAC-trained professionals. The case study used activity theory as a basic model for collaboration that centers around three different components (Figure 1), that is, the collaboration tool or means of collaboration (case study), the roles of the collaborators, and finally the outcomes and reflection on the outcomes and process. The model focused on the outcomes of a targeted activity, in this instance, intervention with a specific child rather than primarily focusing on the nature of the collaboration per se. It is well documented that collaborative efforts can be very time-consuming with few documented outcomes unless well focused (Calculator & Black, 2009; Prelock, Miller, & Reed, 1995).
Communication tool or means
The outcomes of the intervention indicated a positive trend in outcomes of the child’s interaction pattern after 3 months (Table 1). This trend reflected an increase in communication skills of the child although use of the device was limited. As intervention was provided twice a week by the university and once a week by the school, this more intense focus on the child’s communication behavior most likely contributed to the general increase in speech and willingness to want to engage with peers in the classroom as reported by the teacher and paraeducators. However, D’s speech remained mostly unintelligible, which necessitates a critical relook at strategies that can facilitate more extensive use of the device in different contexts.
Role of collaborators
The contribution of this project lies in deepening our understanding of the need for flexible interagency service models, thus the need for “tying and untying of collaborative knots” to allow teams to reposition themselves in relation to their respective roles, relationships, and goals in working toward successful intervention. The two agencies, the school and the university, started off with a clear delineation of their roles as located within the two separate localities although similar therapy outcomes were targeted. Outcomes focused on improving the participant’s operational (university based), linguistic, and social skills (school based). At the end of the initial 3-month intervention period, both agencies realized that a redefinition of roles and goals was needed, that is, the knot needed to be tied differently. Although it was clear that the location of intervention within the school context was important for the second phase of the intervention process, the “new knot” needed to go beyond a mere change in location to include a redefinition of the scope and processes for intervention to provide more support in the classroom and home context.
Collaborative outcomes and reflection on the process
The collaborative approach used was based on minimal intrusion to limit additional demands on school personnel’s time. The teacher and paraeducators were asked to identify time slots for collaboration within their school schedule. The first stage of the collaboration, that is, the process of acquisition of the device (which was primarily conducted by the university) was greatly appreciated by the mother and the school personnel. However, it is clear that the subsequent stages that were focused on intervention with the child and training of classroom staff and parents required further attention. These stages, however, would need to include opportunities for the main collaborators to increase their own skills in AAC assessment and implementation. Only by improving their own competencies in AAC intervention could they work toward quality service in the school district. Partner training (teachers, paraeducators, and parents) needs to be addressed and could require a reconfiguration of intervention goals and collaborative roles. First, a more systematic approach focused on language development and expansion is important. All partners need to share common goals and objectives to ensure realistic outcomes in relation to language development and use. A focus on “language use” rather than on exploring “new vocabulary” together with an incremental approach to the introduction of core and fringe vocabulary is critical in working toward a joint vision for intervention outcomes. Second, specific partner skills needed to be targeted for training, for example, by showing partners how to ask questions or use comments while enabling the child to respond by using vocabulary easily available to her. Third, the team needed to assign new roles in relation to “who will do what” to ensure that all communication partners as well as the child were supported.
Critical Evaluation and Recommendations for Future Research
This study documented an initiative by two SLPs working in the university and school contexts, and describes a bottom–up collaboration process to build more capacity in AAC implementation in the schools. The collaborative process was a natural outflow of professional interactions between two SLPs who chose to follow the strategy of “least intrusion” in the school context as a strategy to obtain buy-in and support from school personnel. In line with this approach, IEP goals were written to reflect expressive and receptive language skills that were not device specific per the regulations of the school district. The lack of data related to device implementation, however, represents a limitation in this study. Although the attitudes of school personnel and parents toward the collaboration process were positive, the current study did not differentiate between outcomes related to the process of collaboration and those related to strategies used, and outcomes of device selection and training of parents and professionals. A clearer differentiation between these processes would be of benefit in future studies.
In view of this, the following recommendations can be made for further intervention and research:
Training opportunities for main collaborators in AAC intervention need to be prioritized to ensure that professionals have the necessary skills and expertise to guide the process of AAC assessment and intervention. Over the past few years, AAC technology has undergone profound changes as mobile technology and AAC Apps have become more available. We need to ensure that school personnel have up-to-date knowledge and skills to guide AAC intervention teams in schools.
A clearer differentiation needs to be made between processes and outcomes related to device selection and training and those describing the intervention outcomes. The use of Light’s (1989) description of communication competencies, that of operational, linguistic, social, and strategic, could be a useful analytical framework to consider.
Collaborative agencies sharing the same location (both working in the school) will facilitate dynamic goal formulation relevant to the changing needs of the participant and the family. This will facilitate planning (Prelock et al., 1995) to allow for refined role differentiation for intervention. Refined role differentiation could be an important strategy in reducing the teacher’s, paraeducator’s, and parents’ anxiety in using the device as they are exposed to more incremental and systematic long-term training.
The exploration of “optimal time” necessary for successful collaborative efforts is important to ensure sufficient planning for intervention and collaboration. For example, collaborations focused on the introduction of sophisticated communication devices within the school context could be more time intensive than the introduction of a Picture Exchange Communication System (PECS) system for individual children. School districts need to have more explicit guidelines to include device trials and to budget for time required for successful device implementation.
As the collaboration process develops, the roles of the interagency collaborators could change. The impact of changing roles in interagency collaboration and its impact on each of the agencies would be critical to enhance understanding of issues surrounding sustainability of collaboration efforts. For example, the mother suggested that students in speech and hearing or special education could be used to facilitate device use in the classroom. It would be important to explore how this idea could be applied within the university and school policy contexts.
Finally, although having different agencies conduct intervention in the same location has advantages, it can be expensive and impractical. The use of tele-rehabilitation strategies such as the use of Skype, for example, could be explored to supplement training sessions with parents, teachers, and paraeducators to facilitate implementation in the natural environment. The use of these strategies by the different agents would necessitate careful consideration of the needs of classroom personnel and parents to ensure a collaborative rather than a unidirectional supplementation of face-to-face contact with tele-rehabilitation sessions.
Footnotes
Appendix
Acknowledgements
The authors would like to acknowledge the support of the director of special education, Kathleen Hugo; school personnel and parents from Monroe County Community School Corporation; and the Indiana University speech and hearing student who participated in this study. Their commitment to the improvement of service delivery within the school system is inspirational.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.