
Abstract
This preliminary qualitative description study explored knowledge from urban Ghanaians about the nature and impact of their self-reported voice problem. Ten Ghanaians were screened for a self-reported voice disorder using the Voice Handicap Index–10 (VHI-10), and they also completed a structured interview with a speech-language therapist. Content analysis was completed from interview responses using quantification of data. Four out of 10 adult Ghanaians demonstrated high VHI-10 scores that indicated a self-reported voice disorder. Themes that emerged included a recurring problem with voice, multiple vocal impairments, limitations with participating in vocal activities, and other health problems. Lack of financial resources and little knowledge about voice disorders were barriers to accessing care. In summary, four adult Ghanaians with a self-reported voice disorder described multiple problems with their voice, limiting their participation in vocal activities. Implications of these preliminary findings include early identification and improving voice care access to avoid handicapping voice problems.
Introduction
Voice is central to daily life for millions of Ghanaians who rely on it for societal and occupational participation (Ghana Statistical Service, 2013; Kitcher et al., 2006; Osei-Bagyina, 2000). Only two studies currently exist that provide initial data on the burden of voice problems in Ghana. Osei-Bagyina (2000) conducted a retrospective chart review of 623 clients presenting to Komfo Anokye Teaching Hospital’s Speech and Language Unit in Kumasi. Identified by “specialists in the field” over a 4-year period, 2.7% of clients from 9 months to 86 years of age were diagnosed with a voice problem. In another retrospective chart review, Kitcher and colleagues (2006) reported on cases of laryngeal cancer (N = 115, 17–85 years, M = 55.5 years) presenting from 1998 to 2003 to Korle-Bu Teaching Hospital in Accra. Squamous cell carcinoma of the vocal fold was the most common malignancy and abnormal voice (dysphonia) was the most common symptom. Only 13% of cases presented within 6 months of symptom onset (median: 12–18 months), with 37% showing locally advanced laryngeal disease. Although these studies provide initial prevalence data and describe voice problems caused by laryngeal cancer, they lack relevant information on the nature of vocal impairments and their impact on participation in vocal activities.
The first step in addressing a public health issue, such as voice disorders, is by describing the nature of the condition. A voice can be considered disordered any time it does not work, perform, or sound as it typically should, so that it interferes with communication (Roy et al., 2005). Voice disorders can occur in the absence of organic laryngeal pathology or other neurological and psychological conditions known to affect voice; in such cases, laryngeal endoscopy would reveal an otherwise normal larynx aside from muscular hyperfunction (Verdolini et al., 2006). Accordingly, one’s perception of their voice is highly relevant to determining the presence of a voice disorder. Knowledge gained from the individual provides personal insight into the nature and impact of their voice disorder. This study was directed at raising awareness of this potential public health concern by providing an early description of self-reported voice disorders on an almost entirely unstudied urban Ghana population. Two research questions were addressed in this study:
Materials and Methods
Qualitative Description Study Design
We used a qualitative description design as an efficient, inexpensive method for gathering knowledge from adults with a self-reported voice disorder living within metropolitan Accra—the capital of Ghana (Sandelowski, 2000). Qualitative description research is a naturalistic approach that uses an inductive process to develop a relativistic, context-specific understanding of a phenomenon from an individual’s subjective knowledge (Bradshaw et al., 2017). Qualitative description studies stay close to individuals’ meaning by providing less interpretation of data than in other qualitative designs (Sandelowski, 2000).
Researcher/Interviewer Characteristics
Structured interviews were administered by male speech-language therapists (SLTs) with more than 5 years of clinical experience (A.Z. and C.A.). One interviewer (A.Z.) from the United States had extensive training and work experience in international settings, was of European descent, and spoke American English. He held a Certificate of Clinical Competence from the American Speech-Language Hearing Association and was licensed to practice as an SLT in the United States. His clinical and research interests were in voice disorders. The other interviewer (C.A.) was from Ghana, of Ga ethnic origin, and spoke English and Ga. He trained as an SLT in the United Kingdom and practiced in the Ear, Nose, and Throat Department at Korle-Bu Teaching Hospital. He had a clinical interest in voice disorders. University of Ghana graduate students in SLT translated for three participants whose languages were not spoken by the primary interviewers (Twi [n = 2] and Ewe [n = 1], both of which are widely spoken in metropolitan Accra). Interviewers transcribed participants’ responses contemporaneously on paper.
Study Context
This study followed the Declaration of Helsinki principles (World Medical Association, 2013). Verbal consent to participate was obtained before administering study procedures. The study was conducted on a single day at Korle-Bu Teaching Hospital’s Speech and Hearing Center in Accra. The interview tool was prepared by the first and last authors (C.A. and A.Z., respectively) and peer reviewed by two University of Ghana SLT faculty.
Sampling Strategy and Recruitment
This qualitative description study used purposive sampling to identify individuals above 17 years of age with a self-reported voice disorder who resided in metropolitan Accra. The research occurred during a free screening at the Speech and Hearing Center that was offered to the public to increase awareness about voice disorders. Radio announcements, paper flyers, and electronic postings occurred the week prior to the event and presented the screening’s purpose, date and time, location, and organizing bodies. Participants enrolled in the study consecutively upon arrival to the site.
Participants were administered the Voice Handicap Index–10 (VHI-10) as a screening tool to identify individuals at risk for a voice disorder (Rosen et al., 2004). The VHI-10 is a valid and reliable patient-reported outcome measure (PROM) that asks about physical, emotional, and functional aspects of a voice disorder. Scoring of the VHI-10 is based on a 5-point Likert-type scale with rating options from 0 = never to 4 = always. The 10 ratings of the VHI-10 items are summed to derive a self-reported vocal handicap score. For this study, a VHI-10 score ≥7.5 was selected as a specificity cut-off score due to its excellent classification abilities in a large endoscopically diagnosed patient sample (Behlau et al., 2016).
Units of Study
Qualitative description studies tend toward smaller sample sizes (Bradshaw et al., 2017; Sandelowski, 2000). This study enrolled a small sample of 10 adult Ghanaians who presented to a screening for voice. Table 1 provides participant characteristics. Reported medical history revealed a relatively healthy set of ambulatory, community-dwelling urban Ghanaians. Four of the 10 individuals who were screened were identified as having a self-reported voice disorder (VHI-10 ≥ 7.5; Behlau et al., 2016). The average age of participants with a self-reported voice disorder was 39.0 ± 12.1 years. All participants with a self-reported voice disorder completed tertiary education and spoke English.
Participant Characteristics by VHI-10 Group.
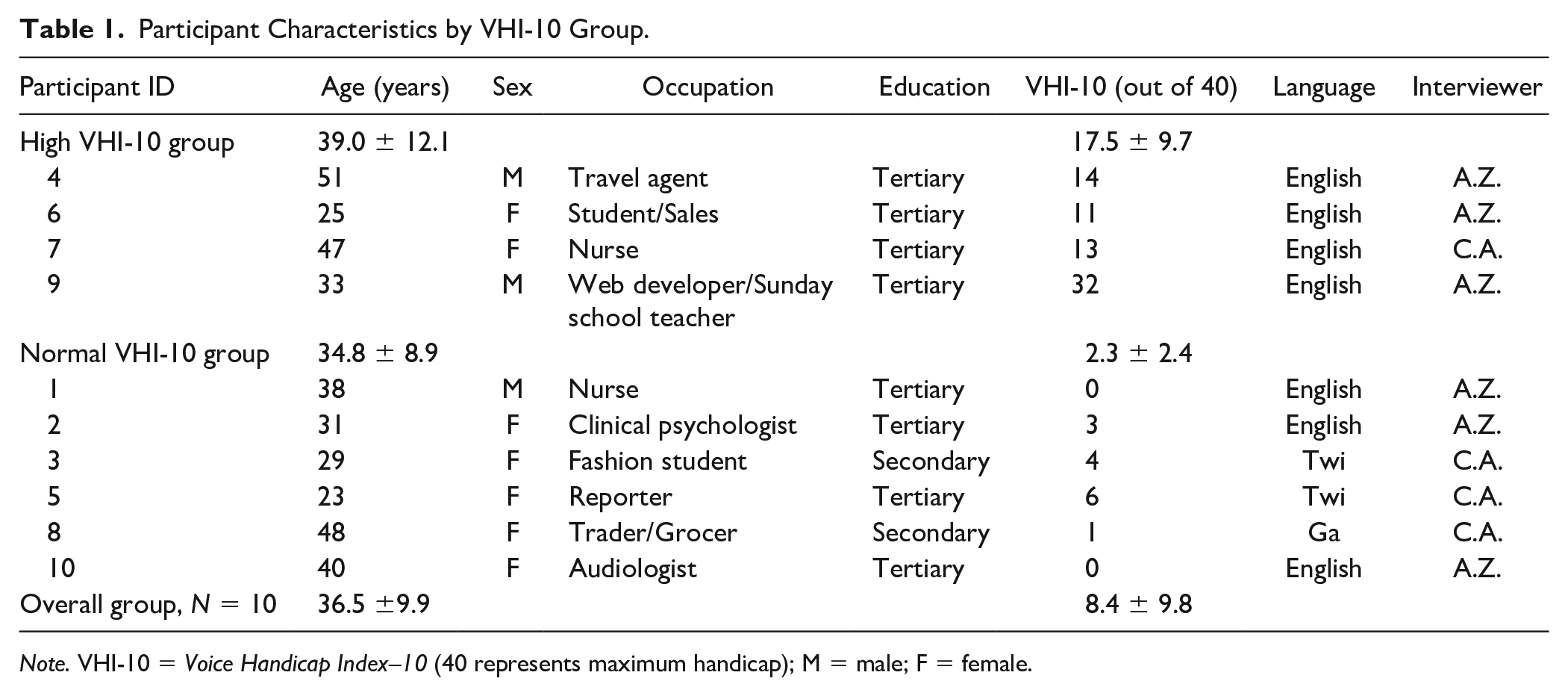
Note. VHI-10 = Voice Handicap Index–10 (40 represents maximum handicap); M = male; F = female.
Interview Corpora
During structured interviews, broad information on voice disorders was probed for based on a biopsychosocial classification framework of health and health-related domains, the International Classification of Functioning, Disability and Health (ICF; World Health Organization, 2013, 2017). The ICF considers impairments in physiological body functions and anatomical structures, limitations in carrying out activities, and restrictions in participating in life situations in addition to environmental and personal context factors. The ICF framework offers an opportunity to gain insight into the way people think about a disability by analyzing textual information elicited from interviews on health and health-related domains.
Drawing on the ICF framework, the breadth and depth of questions in this study allowed for rich exploration of an array of topics related to voice disorders (see Figure 1; World Health Organization, 2013, 2017). Information on symptoms (impairments) included voice problem onset and duration; issues with pitch, loudness, and voice quality; as well as any other self-reported symptoms related to voice. Voice use information (activity limitations) included voice habits at work, vocal loudness during typical use, duration of speaking time, and vocal demands. Participation restrictions included in ability to engage in activities requiring voice as well as absences at work, losses of income, and career changes as a result of voice problems.
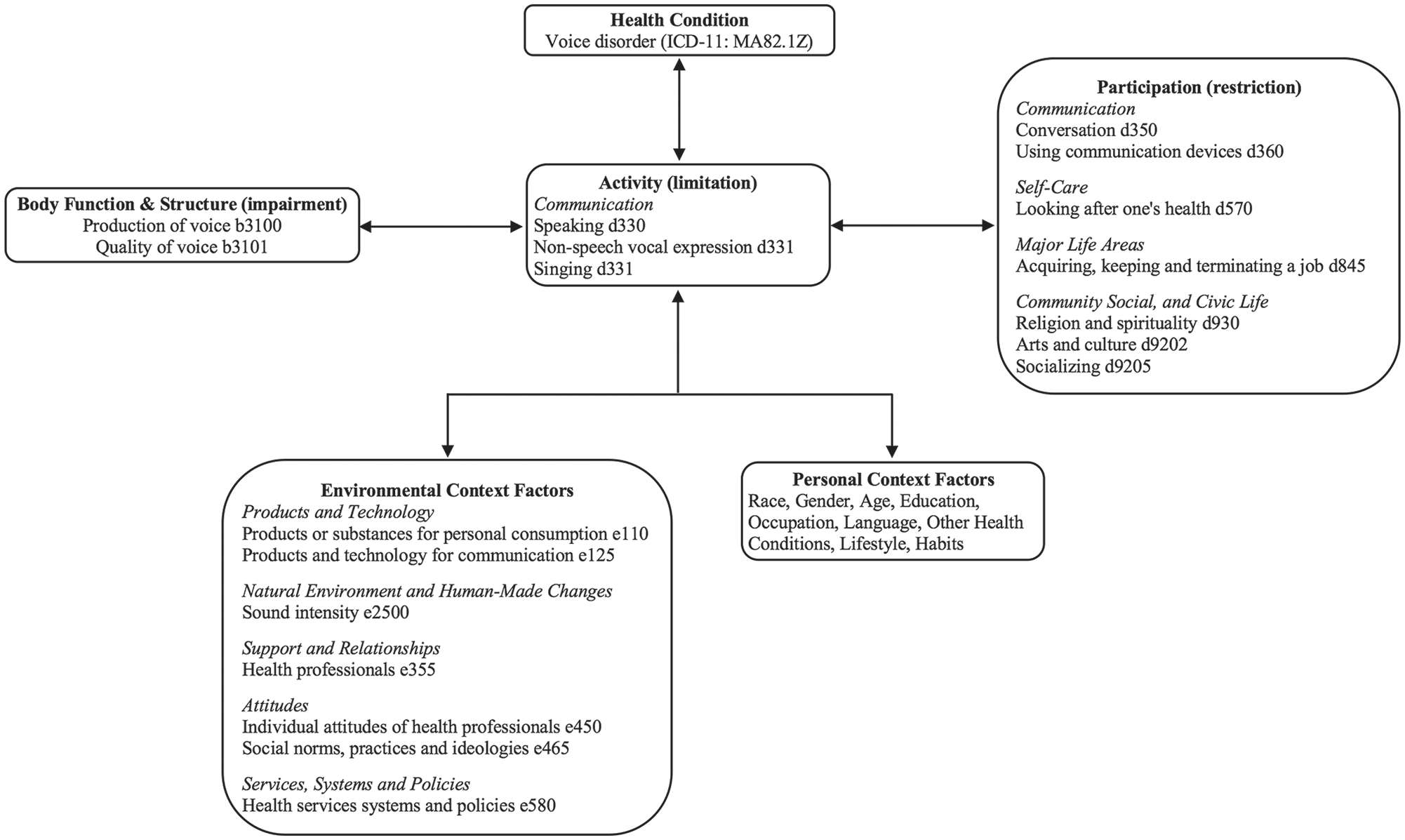
Framework for understanding self-reported voice disorders in Ghana.
Lifestyle topics (environmental and personal factors) included tobacco and alcohol use, hydration, eating habits, employment, home and work noise levels, and church worship patterns. Other environmental and personal factors that were queried included medical information (current medications, reflux-related symptoms [heartburn, globus sensation, chronic throat clearing, effort with swallowing], respiratory or stomach problems, head, neck, or chest injury and surgery, prolonged intubation, laryngitis, sinus infections, and post-nasal drainage), information on management (treatments sought and received as well as associated barriers to health care), and demographics (age, gender, educational level, and employment status).
Study Procedures
After establishing rapport and credibility, participants completed the VHI-10 in English (Rosen et al., 2004). English is the official language of Ghana and widely spoken in metropolitan Accra; however, those unable to read or understand English were provided with verbal translations of the 10 items to rate in their native language with the typed English scale presented as a visual aid. All participants rated VHI-10 items related to physical, emotional, and functional aspects of a voice disorder using the 0 to 4 Likert-type scale. Then, an SLT completed a 30-min structured interview in a quiet room with the participant seated across a small table. Interviews were not audio- or video-recorded to improve the participants’ candidness in their responses (Jones et al., 2013; Wylie et al., 2017). The structured interview was preferred over semi- or unstructured interviews for the ease of documenting responses on paper contemporaneously.
The SLT followed an interview tool adapted from published research that consisted of the same series of mostly closed-ended questions (Roy et al., 2005). The initial portion of the interview sought information on symptoms and impact before moving onto treatment-seeking behaviors in a natural progression. Key questions about voice were queried earlier in the interview to reduce the likelihood of respondent fatigue. Demographics were accessed at the end. Appropriate response categories were provided based on current understanding of voice disorders; other was also a response option. Based on a participant’s response, the SLT was guided to the next appropriate question. Interviewers verbally confirmed participant responses at the time of data collection.
Bias and Trustworthiness
To reduce cross-cultural biases, cultural background research on Ghana was conducted when designing the questionnaire followed by editing from University of Ghana faculty in Accra. Trustworthiness was improved by assigning three-digit participant codes to maintain anonymity. Researchers used de-identified data when conducting analyses to remain blinded to participants. Finally, transparency was increased by following recommendations outlined in the document Standards for Reporting Qualitative Research (O’Brien et al., 2014).
Data Processing
Anonymized and transcribed responses were coded and entered into a data management spreadsheet for content analysis by a research assistant who was a US SLT graduate student (A.H.). The last author (A.Z.) blindly verified responses were coded and entered correctly. Codes included 0/1 for dichotomous variables and a series of numeric values for categorical variables with more than two response options. Summary values were generated (frequencies, f; percentages, %) and used in content analysis to identify themes and subthemes. Quantitative data, such as age and VHI-10 scores, were limited to descriptive analyses with reporting of central tendency and variability to appreciate any differences in characteristics among this sample of adult urban Ghanaians.
Qualitative Data Analysis
Content analysis was completed by the last author (A.Z.) performing quantification of the coded interview data. The interview transcripts from the six individuals who scored within normal limits on the VHI-10 (<7.5) also underwent content analysis. The availability of their knowledge permitted an iterative analysis process that yielded a more precise interpretation of themes for adults with self-reported voice disorders (Bradshaw et al., 2017; Sandelowski, 2000).
The iterative process for establishing themes involved a two-step procedure in which thresholds were applied to variables. Variables that met an 80% threshold were identified in participants with high VHI-10 scores (high VHI-10 group) as well as those whose VHI-10 scores were within normal limits (normal VHI-10 group). This threshold was met when the same responses were provided by three out of four participants in the high VHI-10 group and five out of six participants in the normal VHI-10 group. Variables that met the 80% threshold in both groups were determined to be themes shared by the entire sample of adult Ghanaians. A variable that met the 80% threshold in the high VHI-10 group exclusively, that is, responses for that variable were below a 33% threshold for participants in the normal VHI-10 group, was determined to be unique themes for participants identified to have a self-reported voice disorder. Straight descriptions were generated of each high VHI-10 participant’s account, highlighting their distinct personal experience with their self-reported voice disorder (Bradshaw et al., 2017; Sandelowski, 2000).
Results
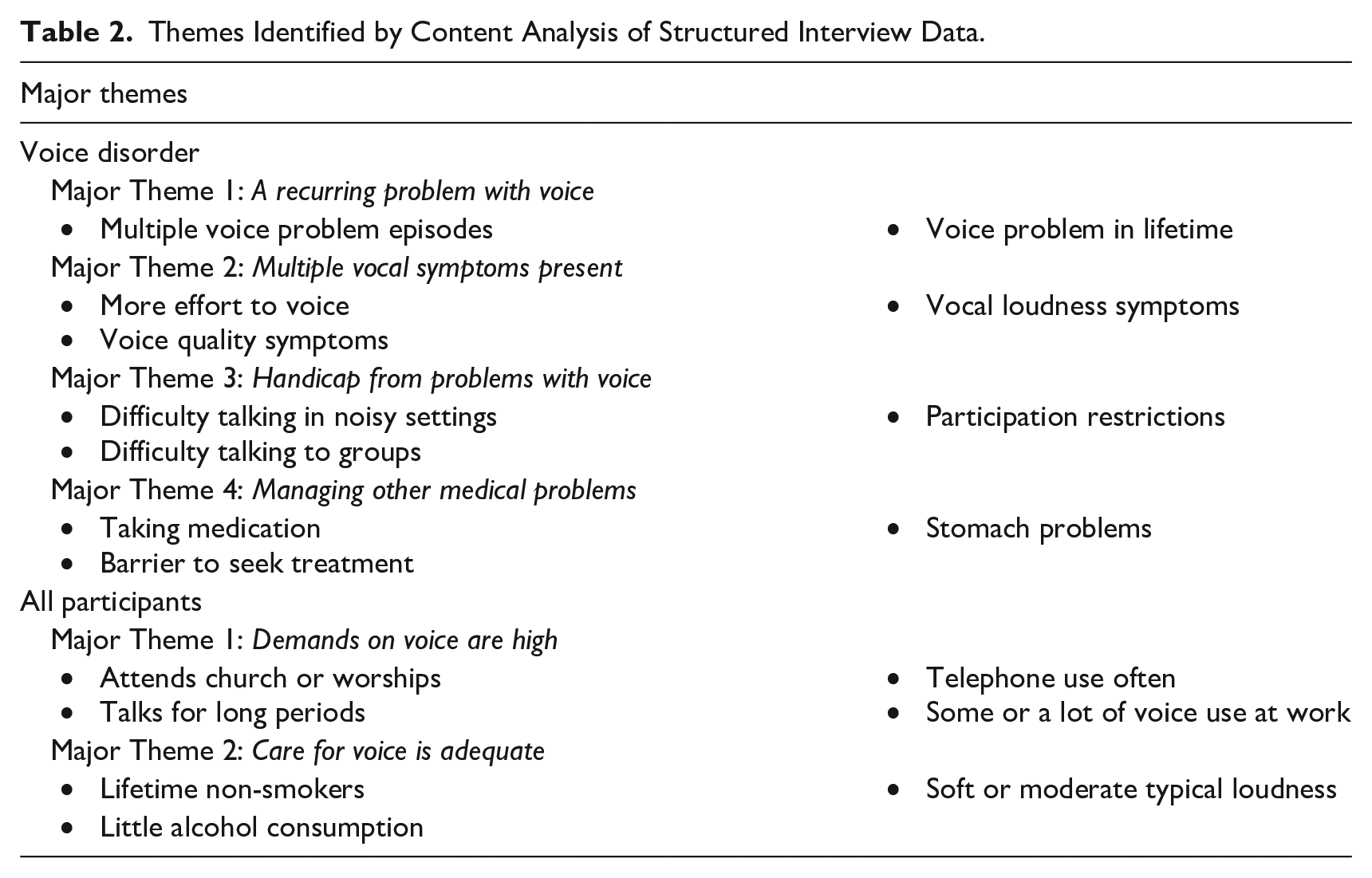
This qualitative description study collected knowledge from urban Ghanaians during structured interviews to explore the nature and impact of their self-reported voice disorder. Ten participants between the ages of 23 and 51 years, a majority of whom were female, attended a screening event for voice problems in Accra in March 2018. Using a VHI-10 cut-off score for specificity (VHI-10 ≥ 7.5; Behlau et al., 2016), four participants (two males) were identified as having a self-reported voice disorder. Four overarching themes emerged from the analysis of coded interview content of participants in the high VHI-10 group. Structured interviews also were conducted with participants in the normal VHI-10 group (see Table 2). Analysis of these interviews along with those of participants in the high VHI-10 group revealed two themes for the overall group of adult Ghanaians who resided within Accra.
Themes Identified by Content Analysis of Structured Interview Data.
Themes for Adult Ghanaians With a Voice Disorder
One theme that emerged was the experience of recurring problems with voice. Although multiple episodes of voice problems were common (3/4), their course tended to be short, lasting less than 4 weeks (3/4). Two participants in the high VHI-10 group reported their voice problem occurred off and on, whereas one participant in the high VHI-10 group indicated their voice problem had been continuous. All four participants in the high VHI-10 group endorsed a voice problem at some point over their lifetime.
Another theme that emerged was experiencing a constellation of voice symptoms. Three participants in the high VHI-10 group reported voice quality–related symptoms, of which vocal strain and breathy voice quality were exclusive to this group. Three participants in the high VHI-10 group reported more effort to voice, and two participants reported discomfort with voicing that was exclusive to the high VHI-10 group. All participants in the high VHI-10 group reported loudness-related complaints. Loudness-related symptoms included whisper voice (n = 2), difficulty being loud (n = 2), being too soft (n = 1), or being too loud (n = 1).
The third theme that emerged was the experience of vocal handicap. All participants in the high VHI-10 group reported difficulty with their voice in talking to groups or in noisy settings, and this finding was exclusive to this group. Three participants in the high VHI-10 group did not consider themselves to be talkative. Vocal activity restrictions were common, and only one participant in the high VHI-10 group described that their voice disorder affected their participation in life situations.
The final theme that emerged was the experience of other health-related issues. The entire high VHI-10 group reported a history of stomach problems. Three participants in the high VHI-10 group indicated problems with acid reflux/heartburn, whereas one participant indicated gastritis. Three participants in the high VHI-10 group reported they were prescribed one to two medications. Care for voice disorders was reported by one participant in the high VHI-10 group, which included prescription medication. Three participants in the high VHI-10 group reported barriers to voice care that included limited financial resources (n = 2) and lack of awareness about treating voice disorders using SLT (n = 2).
Straight Descriptions of Each Voice Disorder
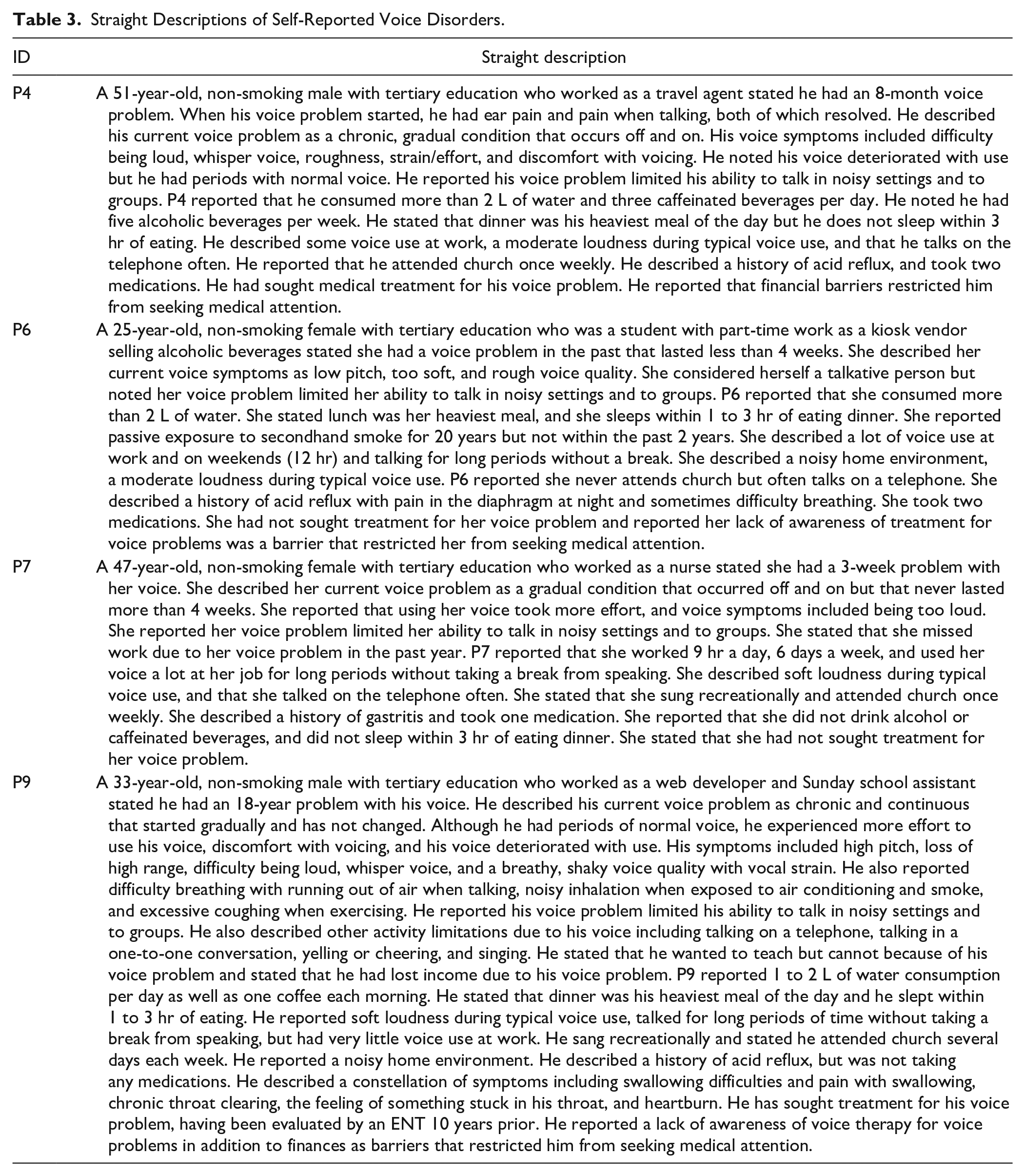
Rich descriptive summaries were generated from the interview responses of participants in the high VHI-10 group about their self-reported voice disorder (see Table 3). Although some parallels existed, each descriptive summary showed unique experiences with self-reported voice disorders among this sample of urban Ghanaians. These rich descriptive summaries highlight the importance of obtaining a person’s perception of their voice problem and provide preliminary evidence of the subjective nature of voice disorders.
Straight Descriptions of Self-Reported Voice Disorders.
Themes for Adult Ghanaians Regardless of Voice Status
Content analysis of interview responses from the entire sample of adult Ghanaians resulted in two themes related to voice. The first theme was high vocal demands. Most participants reported a lot or some voice use at work, whereas two participants reported little occupational voice use. Many participants reported that they used the telephone often (8/10) and talked for long periods without a break (7/9). Most participants (8/10) attended church or worshipped at least weekly.
The other theme was adequate voice care. Seven (78%) participants (five without a voice disorder) reported consumption of greater than 2 L of non-caffeinated fluids per day. Caffeine intake was limited in the seven participants that indicated consumption. All participants denied smoking tobacco (lifetime), and most participants (7/10) did not drink alcohol. Two participants in the normal VHI-10 group (33%) reported less than one drink per week, whereas one participant in the high VHI-10 group (25%) reported five alcoholic drinks per week. Nine participants considered their typical loudness to be soft or moderate, and only one participant who was in the normal VHI-10 group reported being loud or very loud.
Discussion
This qualitative description study aimed to raise awareness about self-reported voice disorders in Ghana. Two adult females and two adult males in the understudied setting of urban Ghana were identified by the VHI-10 as having a self-reported voice disorder (Behlau et al., 2016; Rosen et al., 2004). In drawing from the ICF biopsychosocial framework (World Health Organization, 2013, 2017), a variety of information about health-related dimensions that influence voice was gathered during structured interviews of urban Ghanaians. Several themes emerged from content analysis of coded interview responses, and straight descriptions of each participant’s self-reported voice disorder provided an initial picture of their unique experience. The vocal disability described by four participants encompassed a range of changes to vocal functioning and was affected by environmental and personal context factors. The preliminary findings from this qualitative description study together with published retrospective studies of voice problems hint at a potentially relevant public health concern in Ghana (Kitcher et al., 2006; Osei-Bagyina, 2000). The following discussion interprets study themes and provides suggestions for the public health SLT in Ghana on management and prevention of voice disorders.
Vocal Impairments and Their Restrictions on Vocal Activities and Life Situations
One theme was the experience of recurring problems with voice. Problems with voice were episodic for two participants in the high VHI-10 group, and one participant experienced a continuous issue with their voice. In terms of vocal functioning, the second theme was the experience of a large number of voice-related symptoms. Voice quality–related symptoms and complaints of vocal effort predominated, and loudness-related symptoms were commonly reported. In summary, problems with voice for this sample of urban Ghanaians involved multiple symptoms that occurred mostly episodically.
The third theme that emerged was limitations to vocal activities and restrictions in life situations. Specific activities affected by vocal disability were talking in groups (100% reporting difficulty) and talking in noisy environments (100% reporting difficulty). The finding that participants in the high VHI-10 group felt handicapped by their voice in groups or noisy environments is not surprising given the sound pressure requirements to be heard in those contexts. The consequences of one participant’s voice disorder were missed work, job changes, and a loss of income as a result of not being able to teach. This participant’s restriction with teaching highlights the occupational impact of voice disorders (Roy et al., 2005).
Three participants in the high VHI-10 group indicated they were not talkative. This finding may reflect a negative consequence of voice disorders (Roy et al., 2005). Another explanation is that different patterns of voice use are associated with different voice disorders. Roy and colleagues (2000) observed that extroversion was associated with vocal fold nodules, whereas introversion was associated with functional dysphonia characterized by muscle tension. Taken together, self-reported voice disorders in this sample of urban Ghanaians resulted in non-trivial personal and professional consequences and negatively affected voice-related quality of life.
Environmental and Personal Context Factors
The final theme that emerged was the experience of other health-related issues with barriers to management. The entire high VHI-10 group reported a history of stomach problems, of which acid reflux (n = 3) was common. Three participants in the high VHI-10 group reported pharmaceutical management including one participant who was prescribed medication for acid reflux. Management of voice and other communication disorders has been reported to consist mostly of medical interventions (Fagan & Jacobs, 2009; Wylie et al., 2017).
Financial barriers and lack of awareness of management for voice disorders by SLTs were described by participants in the high VHI-10 group. Few SLT services exist to manage voice and other communication disorders among Ghana’s 10 regions; all are concentrated in urban settings and accessed primarily by patients with sufficient financial resources (Crowley et al., 2013). Perhaps, due to such barriers, Ghanaians with voice and other communication disorders have been reported to seek treatment later in their disease process (Fagan & Jacobs, 2009). Kitcher and colleagues (2006) found in their laryngeal cancer cases the average duration of hoarseness before presentation ranged from 11 to 17 months and was as high as 60 months. These issues emphasize a need for further research on the obstacles faced by Ghanaians in accessing SLT services for voice disorders.
Shared Experiences With Voice in Urban Ghana
Two themes emerged for the entire sample of urban Ghanaian adults. The first theme related to high vocal demands. The group described a large number of daily activities that required voice. Many participants reported frequent telephone use (8/10), worshipped at least weekly (8/10), and talked for long periods without a break (7/9). Most participants reported a lot or some voice use at work, whereas only two participants reported little occupational voice use. Given the increased risk for voice disorders with heavy vocal demands (Roy et al., 2005), potential risk factors for voice disorders in Ghana need to be examined further.
The second theme for this sample of adult urban Ghanaians related to adequate voice care. Aside from the heavy vocal demands, the group generally described behaviors that were associated with maintaining vocal health. Participants mostly reported a soft to moderate level of vocal loudness when speaking (90%). They indicated a high level of hydration, and alcohol consumption was reported to be minimal. None of the participants in this sample reported any prior or current tobacco use, a finding that is in line with data showing only 3.8% of Ghanaians are reportedly current smokers (8.9% male, 0.3% female) and less than 10% reported having ever smoked (22.0% male, 1.2% female; Owusu-Dabo et al., 2009). These preliminary findings suggest that protective factors helped to maintain the vocal health and wellness of many from this sample of adult Ghanaians.
Implications for Voice Disorder Management in Ghana
Management of voice disorders in Ghana is limited by few university-trained SLTs, and SLT training programs in Ghana are only commencing (Crowley et al., 2013; Wylie et al., 2014, 2016). Increasing the rehabilitation workforce in Ghana to provide individualized services for voice disorders that meets population needs will take considerable time. Efforts in Ghana likely require a broader, public health approach of community-level SLT services for those at risk for a voice disorder (McAllister et al., 2013).
Community-level SLTs can have a major impact in a public health role. The public health SLT can perform outreach to develop positive attitudinal responses to voice disorders, provide education on voice disorders that includes early detection, and offer vocal injury prevention to at-risk groups of Ghanaians such as teachers and preachers (Wylie et al., 2018; Ziegler, 2020). The findings of this study indicate the need for a multi-dimensional voice evaluation in individuals who access care for voice problems (i.e., tertiary prevention/treatment). Finally, study findings suggest PROMs (e.g., VHI-10) can yield information about the symptoms and impact of voice problems that complements clinical signs of voice disorders obtained from auditory-perceptual evaluation of the voice and visual inspection of the larynx. PROMs can be re-administered post-intervention to appraise the patient’s perception of the response to treatment.
Limitations
Several limitations deserve mention. Structured interviews involved closed-ended questions that may have limited information sharing. Participants were not contacted to confirm interpretation of study findings and interviews were not recorded, both of which have the potential to affect the accuracy of reporting on participants’ experiences. Using the VHI-10, which has never been validated for administration in Ghana, may have introduced cross-cultural bias. Finally, this sample of participants primarily consisted of educated, young, and middle-aged adult females who resided in or near Accra, which does not fully reflect the diversity of Ghanaian society in terms of educational level, age, gender, and geographical region.
Future Directions
Large-scale epidemiological research is needed to examine the risk factors for voice disorders in Ghana and their burden, including in occupational voice users such as teachers and preachers. Such research will provide targets for cost-effective prevention programs for voice that can be implemented by public health SLTs and tested for effectiveness on a national scale.
Conclusion
This qualitative description study in Accra, Ghana, identified four adult participants with a self-reported voice disorder. Preliminary findings indicated that voice disorders were associated with limitations in vocal activities that required loud voice. Barriers to care were also highlighted. A public health SLT approach is indicated for voice disorders in Ghana. Future, large-scale epidemiological research on voice disorders in Ghana is necessary to expand current understanding of this potential public health issue.
Footnotes
Acknowledgements
The authors are grateful for Victoria Akua Nana Owusu, Josephine Ohenewa Bampoe, and the 2018 master’s students from the University of Ghana’s Speech and Language Therapy program for their assistance with screenings. The last author (A.Z.) thanks the individuals and organizations who donated to the Ghana Voice Campaign. This research was presented as a poster at the Fall Voice Conference on October 26–27, 2018, in Seattle, USA.
Authors’ Note
This research was conducted while Dr. Ziegler was Assistant Professor in the Department of Otolaryngology—Head & Neck Surgery, Oregon Health & Science University.
Author Contributions
C.A., A.H., and A.Z. contributed to study concept and design, and analysis and interpretation of data; C.A., G.T., L.G., and A.Z. contributed to acquisition of data; and C.A. and A.Z. performed critical revision for important intellectual content. All authors drafted the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded, in part, by the Australian Government’s Direct Aid Program and the University of Ghana.