
Abstract
Cross-cultural studies of mental health and illness generally adhere to one of two agendas: the comparison of mental health between sites using standard measurement tools, or the identification of locally specific ways of discussing mental illness. Here, we illustrate a methodological approach to measuring mental health that unites these two agendas. Using examples from our work in India and Haiti, we show how researchers can use mixed methods to identify idioms of distress, develop locally derived tools to measure them, evaluate the psychometric properties of these tools, and contextualize the results with relevant ethnographic information. Such an approach is beneficial because it generates results that attend to important cross-cultural differences in expressions of distress while still maintaining comparability of mental health and illness across research sites.
Introduction
Among social scientists interested in mental health, identifying idioms of distress and developing culturally specific mental health assessments have been key research priorities (Bolton 2001; Kohrt and Harper 2008; Patel et al. 2001; van Ommeren et al. 1999). Understanding psychological distress from diverse cultural perspectives is important both theoretically and clinically because, as Kirmayer (1989:327) notes, “Cultural variations in the diagnosis and handling of behavior and experience influence the natural history of psychiatric disorders and emotional distress.”
This culturally particularistic agenda contrasts with another dominant trend in cross-cultural mental health research: efforts to generate standardized instruments usable across settings (see Kohrt et al. 2011; Weller et al. 2008). This approach facilitates cross-cultural comparison of quantified degrees of distress but has been accused of promoting “efforts to persuade others to accept our definitions of disease and our medicine, and widespread disregard for culturally defined illnesses and the socio-cultural contexts of all disease” (Hahn and Gaines 1985:13).
We suggest that a mixed methods approach, including both standardized and culturally specific instruments enriched by ethnographic work, is the most effective way to understand distress cross-culturally. Such an approach acknowledges the “cultural variations” and “socio-cultural contexts of all diseases” to which Kirmayer (1989) and Hahn and Gaines (1985) draw attention, while at the same time preserving our ability to make cross-cultural comparisons. Aside from this ideological value, a mixed methods approach is pragmatically useful because qualitative and quantitative methods can provide a more robust reflection of reality by compensating for one another’s shortcomings (Greene 2008; Tashakkori and Teddlie 2010). A survey, for instance, provides a large-scale view of trends that would be missing from case studies, while case studies provide context and meaning in which to interpret survey results.
The methods presented here were parts of larger studies on chronic physical and mental illness comorbidities in India, and on mental ill health in Haiti. The goal was to develop locally relevant ways to assess mental health alongside standard mental health measurement tools. The resultant scales were ultimately used to assess prevalence and severity of depression, anxiety, and locally relevant distress syndromes in the study groups.
Our studies focus on the idiom of “tension” in North India and various idioms, including “thinking too much,” in Haiti. The English word tension is common in Hindi-speaking and other linguistic groups (Halliburton 2005; Kielmann and Bentley 2003; Pereira et al. 2007), and it might have important consequences for physical and mental well-being (Weaver and Hadley 2011). “Thinking too much” has been widely reported cross-culturally, including in Haiti (Bolton 2012; Kaiser et al. 2014; Patel 1995). This idiom, which describes prolonged rumination, social isolation, and sadness, has been compared to depression and anxiety, which have no meaningful translations in Kreyòl (Keys et al. 2012).
The methods presented here are particularly useful for establishing prevalence of common mental disorders in places where psychiatric terms have limited meaning because they account for forms of distress that may not be captured by depression and anxiety screeners or that people may underreport because of stigma attached to psychiatric problems. In both India and Haiti, mental illness has been historically diagnosed only when a person experiences severe symptoms such as florid psychosis or dementia (Farmer 1992; Raguram et al. 1996; World Health Organization/Pan American Health Organization [WHO/PAHO] 2010). Therefore, people with common mental disorders are unlikely to visit mental health care providers. Assessment methods that use locally acceptable terms are thus crucial for capturing people’s experiences of distress cross-culturally. This process could be applied in other cultural contexts, both rural and urban, to identify and measure the severity of distress in locally and internationally relevant terms.
The methods described here build on previous mixed methods work in scale development and testing (see Bolton 2001; Borgatti 1999; DeVellis 2012; Tashakkori and Teddlie 2010) but contribute a new emphasis on the retention of ethnographic data alongside scales. This ethnographic focus is important for preserving the variation in distress experiences, for making apparent to readers what specific aspects of distress are (or are not) measured by the scales being developed, and for increasing transparency.
Study Contexts
Objectives
The India study explored how women with and without type 2 diabetes negotiate social roles and family life. We used two methods to assess mental health: a Hindi version of the Hopkins Symptoms Checklist-25 (HSCL) for depression and anxiety and a locally derived scale measuring “tension.”
The Haiti study explored perceptions and resources for mental illness. This included the first large epidemiologic study of mental illness in rural Haiti. We measured mental illness using culturally adapted versions of the Beck Depression Inventory (BDI) and Beck Anxiety Inventory (BAI) and a locally developed scale based on common idioms of distress.
Research Methods: Sampling, Data Collection, and Ethical Considerations
The first phase of each study involved using ethnographic methods to collect baseline information about idioms of distress. We used this ethnography to identify important idioms of distress and develop tools for measuring their severity, pilot tested them, and applied them in larger epidemiologic surveys. We subsequently conducted a second round of ethnography to develop case studies.
Verbal informed consent was obtained prior to participation in each study. All study procedures were preapproved by the Institutional Review Board of Emory University and locally by the Haitian Ministry of Health, the University College of Medical Sciences, New Delhi, and the Indian Council of Medical Research.
India Study
In a 2009 pilot phase, we recruited 62 diabetic and nondiabetic women from 14 private health clinics throughout Delhi for freelist interviews (Borgatti 1999). Freelists asked women to name as many symptoms or characteristics of tension as they could. We retained items mentioned by three or more individuals into a 20-item scale with the prompt, “In the past two weeks, to what extent have you felt the following mood-related items?” with three response categories ranging from “not at all” to “a lot.” We piloted the tension scale and the culturally adapted Hindi HSCL with an additional sample of 30 diabetic women to establish baseline internal consistency and face validity of each instrument (Weaver and Hadley 2011).
In a larger research phase in 2010–2011, we reduced the tension scale to 14 items. Items were eliminated after review with three laypeople and two mental health professionals if they were deemed nearly universal (e.g., “disappointment due to unmet expectations”) or were combined into one item if they were deemed nearly identical (e.g., combining “general anxiety” with “general stress/lack of relaxation”). Two hundred and eighty women (n = 184 diabetic) were recruited from seven private clinics, a public hospital, and two charitable clinics to capture various socioeconomic strata.
We purposively selected 30 diabetic women from the group of 184 for case study interviews, maximizing variation in socioeconomic status (SES), caste, and religion. We visited each participant at least once at home to conduct semistructured interviews, which followed a modified version of Kleinman’s illness narrative interview (Liburd et al. 2004). All interviews, each of which took about an hour, were conducted privately in Hindi by the first author and a female Indian research assistant and were audio recorded.
Haiti Study
In a 2010 pilot phase, we collected ethnographic data through 31 semistructured interviews, 11 focus groups, and participant observation with four individuals suffering from mental distress (Keys et al. 2012). Interviews lasted between 45 minutes and 1.5 hours and were audio recorded. Each case study was visited four or five times and engaged with in casual conversation and observation of daily activities and interactions, as well as semistructured interviews with case study participants, family, and friends. Observation notes were taken throughout, and semistructured interviews were audio recorded.
To adapt the BDI and BAI into Kreyòl, we employed van Ommeren et al.’s (1999) approach for transcultural translation of mental health instruments. This approach involves collecting initial translations from both lay and professional individuals. We then held lay focus groups addressing comprehensibility, acceptability, and item relevance.
Through qualitative data collection, including the individual interviews, focus groups, and participant observation described previously, we identified 43 potential idioms. Following discussions with two Haitian clinicians and an additional focus group with community members, we reduced the list to 17 items, removing idioms that were thought to be nearly universal, were not well understood, or were redundant. We piloted the remaining 17 items among 97 participants, with participants indicating their experience of each item during the previous two weeks on a five-item Likert-type scale ranging from “never” to “all the time.” We then removed four more items because they were infrequently endorsed and seemed to reference stigmatizing concepts (Kaiser et al. 2013).
We applied the final 13-item idioms of distress screener, along with the culturally adapted BDI and BAI, as part of a 408-person epidemiologic survey in 2011 (Wagenaar et al. 2012). Participants were randomly selected through a modified version of the World Health Organization’s “random walk” protocol (World Health Organization [WHO] 1991). Trained Haitian research assistants conducted the surveys in Kreyòl, which took approximately one hour.
Analytic Methods: Evaluating Locally Derived Mental Health Scales Overview of Data Analyses
Our analyses aimed to test the statistical reliability and ethnographic validity of our locally derived mental health scales using mixed data sources. Our main strategy was to quantitatively compare response patterns between the locally derived and standard mental health instruments, then to situate these comparisons in ethnographic context using the qualitative results obtained from case studies, semistructured interviews, and focus groups.
We performed quantitative analyses using SAS 9.2 and SPSS 18.0.2. Qualitative data were transcribed, translated, and entered into MaxQDA10. Details of the analysis processes are described subsequently.
Quantitative Analyses
We calculated univariate and bivariate statistics (means, proportions, correlations, and cross-tabulations) to explore the range, variation, and basic relationships of our study variables. They demonstrated strong positive relationships between participants’ scores on locally derived and standard mental health scales (.52 ≤ r ≤ .75).
Next, we tested internal consistency of each mental health instrument using Cronbach’s α, which indicates the strength of intercorrelations among items. A value above .70 is conventionally acceptable (Nunnally and Bernstein 1994). In both studies, the standard and locally derived mental health measurement tools had Cronbach’s α values exceeding .80, suggesting internal consistency—that is, the items in each scale measure the same underlying construct.
We subsequently used t-tests to examine differences in mean HSCL or BDI/BAI scores between individuals who endorsed or did not endorse experience of each item on the locally developed scale. These analyses indicated the degree to which each item in the locally derived scales corresponded with depression versus anxiety. For instance, those who did not endorse experience of a given item on the tension scale scored significantly lower on both the HSCL depression and anxiety sections than those who endorsed the item, suggesting that the tension items might be equally related to depression and anxiety. In the Haiti study, several items on the idioms of distress scale were more consistently related to anxiety than to depression.
A principal components analysis (PCA) further illustrated the constructs being measured by our locally derived scales. Components were identified for retention based on eigenvalue and scree analyses (Cattell 1966; Kaiser 1960) and proportion of variance accounted for by each component.
A PCA using direct oblimin rotation on the India data identified one dominant component in the tension scale, explaining 40.5% of the variance. The HSCL had two dominant components, explaining 34.0% and 13.9% of the variance. For the Haiti data, the idioms of distress scale included four primary components explaining between 7.4% and 38.1% of the variance. The BAI and BDI each had one dominant component explaining 29.9% and 28.7% of the variance, respectively. Based on these results, we concluded that each scale seemed to be functioning as expected: the tension scale, BDI, and BAI measured single constructs; the HSCL measured two constructs; and the Haitian idioms of distress screener contained multiple components.
Finally, we used multivariable linear regression with a stepwise elimination process, beginning with all possible predictor variables, to identify significant predictors of our local distress measures (see Appendix for variables considered for inclusion). Relationships observed in both statistical models are supported in published literature, suggesting convergent validity of scales (see Table 1).
Multivariable Linear Regression Model for “Tension” Total Score among Urban Indian Women (n = 280; Top) and Idioms of Distress Total Score among Rural Haitians (n = 402; Bottom).
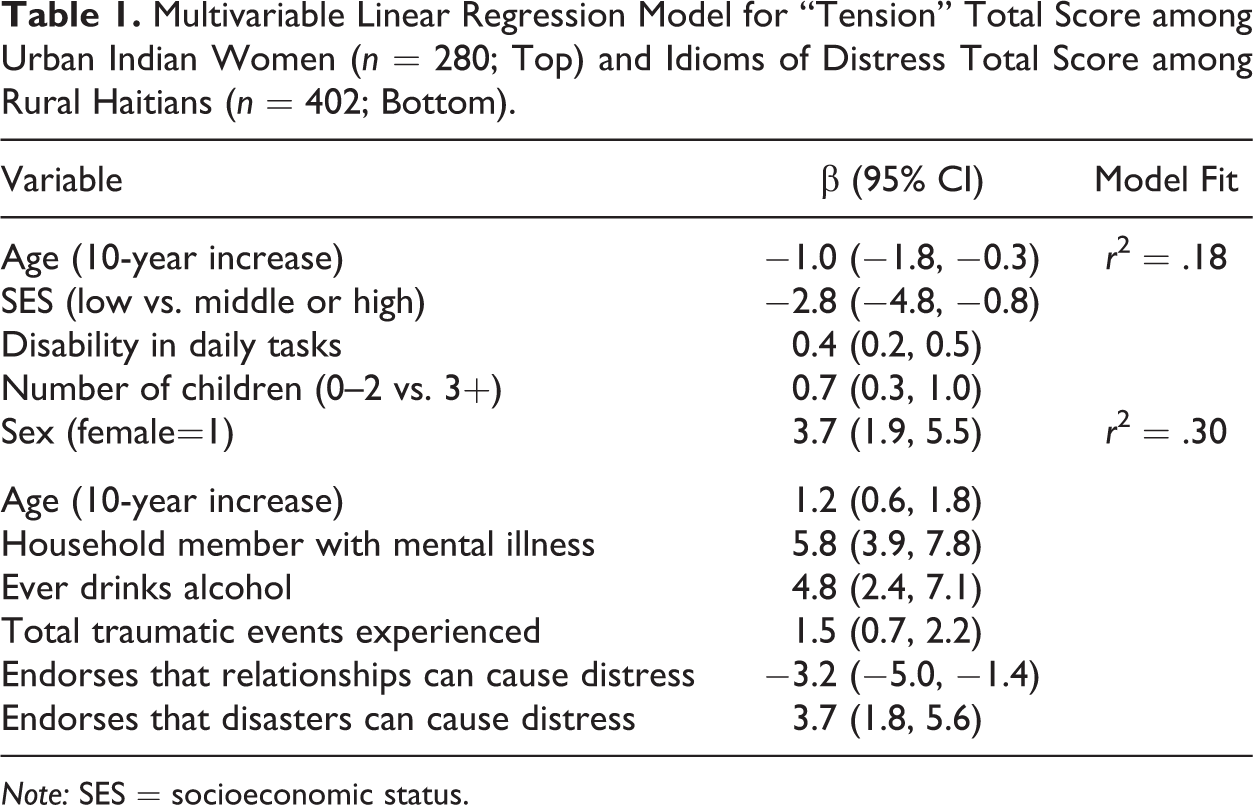
Note: SES = socioeconomic status.
Qualitative Analyses
In addition to the statistical analyses presented previously, a key criterion for evaluating locally developed psychometric scales is their comprehensibility to the populations among which they have been developed, sometimes referred to as face validity or ethnographic validity (Wutich and Ragsdale 2008). Although we present the qualitative analyses second, they were, in fact, conducted in two phases before and after the quantitative data collection and used iteratively in scale development (see Figure 1).
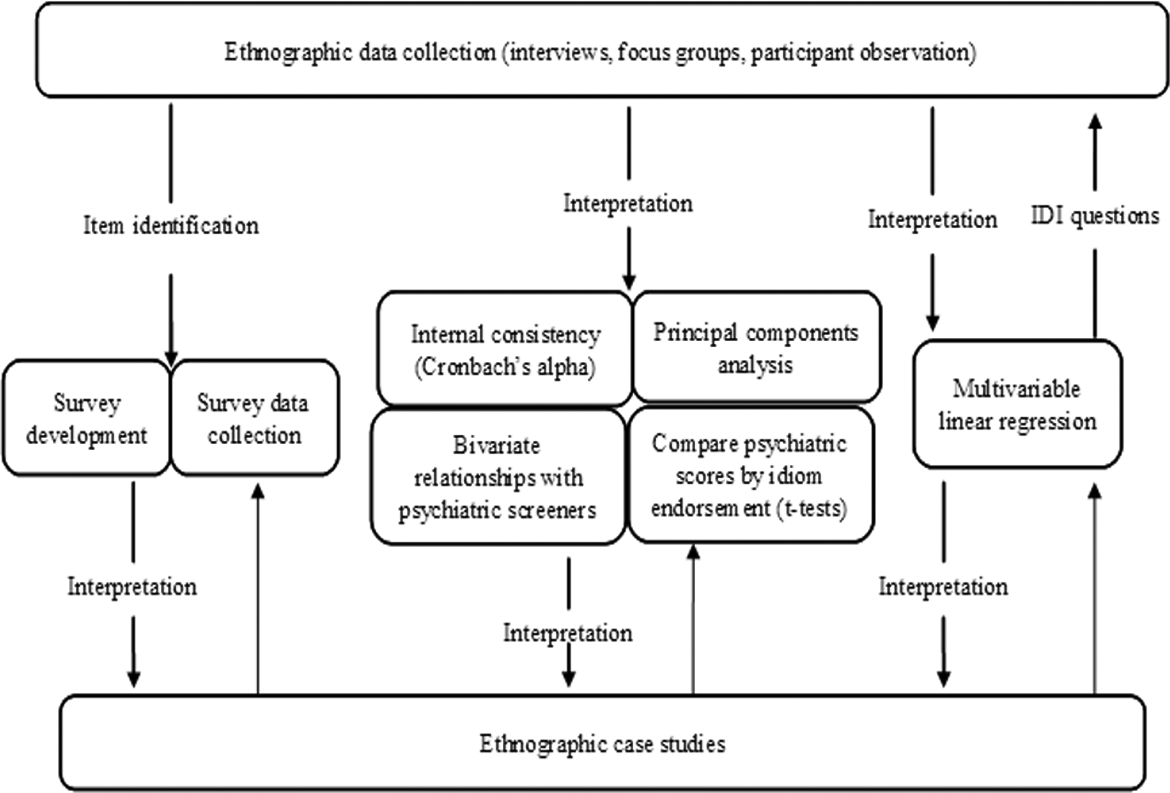
The mixed methods process used to develop and evaluate locally derived mental health measurement tools.
Transcripts and field notes from each pilot phase were analyzed using keyword-in-context searches for “tension,” “depression,” and “anxiety” for the India data and “thinking too much” for the Haiti data to identify passages where distress was discussed (Ryan and Bernard 2003). These potentially relevant passages were then coded for emergent themes using open coding based on repetition of themes, followed by selective coding (Corbin and Strauss 2007). Finally, coded segments were classified as relating to characterization, recognition, causation, or consequences of the idiom in question and examined for similarities and differences. Transcripts of case studies were examined individually for frequency of the idiom in question, richness of description, and comparisons between psychiatric terms and local idioms.
Characterization and recognition of tension
Tension is used to describe variable levels of distress in North India. A common response among women when asked about tension was “Tension happens; what good does it do us to think all the time?” The contrast between this and other cases, where tension was used to discuss serious personal and family crises, drew our attention to the versatility of the expression. When women used tension to talk about significant troubles, they described symptoms resembling the hopelessness and suicidal ideation of clinical depression. Case studies were especially useful for illuminating the range of uses of tension and led us to expect that tension would not correspond neatly to either depression or anxiety but might include elements of both. The quantitative analyses confirmed that tension is closely related to both depression and anxiety but does not function in precisely the same manner as either one.
Some wealthy, English-speaking women directly associated tension with clinical depression, such as this woman who took antidepressants: “I get tension very quickly, because I take depression medicines, right? So I take tension quickly over small issues.” No one, however, linked tension with clinical anxiety, despite the strong positive correlations between women’s tension and anxiety scores. The ethnographic linkage between tension and depression supported the idea that tension is a relevant category in women’s lives that can overlap with conventional common mental illnesses, but contextual data are needed to assess its severity. Statements like the one mentioned previously suggest that the term “depression” is gaining some currency among high-SES groups in New Delhi. Clinical anxiety appears not to have entered the public consciousness to the same degree, however, and thus might be met with resistance or misunderstanding.
Causation and consequences of tension
The most common etiologies of tension were specific events or circumstances, especially strained relationships. This contrasts with biomedical etiologies of depression and anxiety, in which no precipitating event need occur, but it is consonant with recent proposals about new ways of classifying mental disorders in the upcoming International Classification of Disease-11 (Maercker et al. 2013). It also has important implications for prevention and treatment of tension.
The ethnographic work helped us qualify the consequences of tension for both physical and mental health, an important aspect of any investigation that deals with a previously unmeasured idiom of distress. Women agreed that tension had physical, emotional, interpersonal, and behavioral consequences not easily captured by quantitative data.
The causes and consequences of tension in women’s lives are diverse; as such, it is a challenge to isolate a single operational definition of tension. The retention of ethnographic work alongside a quantitative tension scale helps underscore the complexities of distress experiences. This ethnographic work also provides important directions for future study of tension by suggesting potential causes and outcomes associated with it, such as social strain, and potential points of disjuncture between local and psychiatric understandings of mental ill health.
Characterization and recognition of thinking too much
The Haiti idioms of distress screener involved multiple idioms; here we present ethnographic results pertaining to the most common idiom, thinking too much, as an example of value added through ethnographic data.
As the term suggests, the essential feature of thinking too much (reflechi twòp) is persistent rumination. The classification of thinking too much depends not only on the quantity of thought but on the subject of one’s thoughts. For example, respondents explained that reflection is normal following the loss of a family member, but thinking too much occurs when someone persistently focuses on one issue, becomes overwhelmed by it, and thinks without searching for a solution. This distinction is clinically important because it highlights a fine-grained difference between socially acceptable and unacceptable forms of preoccupation, which if ignored might lead to overdiagnosis of depression or anxiety or, in the opposite direction, overlooking legitimate distress.
Participants indicated that someone thinking too much can be easily recognized when they sit in solitude, lose weight, or become unusually quiet. One community member explained, “It’s easy to see when someone is in a situation like this, because they will just stay by themselves. They won’t take company with anyone. He is thinking, pondering.” Thinking too much, like tension, can describe varying levels of distress, often recognizable by length of time and extent of concomitant social isolation and physical consequences. In fact, three-fourths of our sample endorsed any experience of thinking too much. It is thus essential to couple endorsement of thinking too much with contextual information that indicates when this idiom represents significant psychoemotional distress.
Causation and consequences of thinking too much
Concerns over money and food were commonly named causes of thinking too much. As was the case for tension, these situations were often driven by specific events and external factors, such as job loss or failed crops. Following precipitating events, general lack of activities was described as exacerbating thinking too much. The family of a man suspected of being fou (crazy) explained that he used to have a job and participate in activities, but now he only thinks and cannot do what he wants. His inability to contribute to the family as he once did is compounded by having ample time to “sit and think,” or ruminate.
While the focus on rumination may resemble anxiety, thinking too much also resembles depression due to its close links to social isolation and serious sadness; many references to thinking too much arose when participants were asked to talk about sadness. The consequences of thinking too much are similar to those of depression and anxiety as well. People who are thinking too much are described as remaining deep in thought instead of eating, resulting in weight loss. One who is thinking too much continues ruminating at night, thus having trouble sleeping. Other sicknesses follow from thinking too much, including physical sicknesses, as well as more significant mental problems, such as memory loss and, on rare occasions, fou, a term for psychosis that is often linked to schizophrenia (Desrosiers and Fleurose 2002). Since depression and anxiety have no conceptual equivalents in Kreyòl, thinking too much perhaps provides a locally meaningful way to communicate these experiences. At the same time, these idioms cannot be reduced to psychiatric categories and should be incorporated into clinical communication, rather than displaced or disregarded.
Discussion and Conclusion
Establishing locally relevant ways to measure mental health is crucial if cross-cultural psychiatry and psychological anthropology intend to respect non-biomedical ways of understanding distress. It is, however, useful to establish how non-biomedical expressions compare with common mental disorders to test claims of cross-cultural comparison. In this article, we have presented a process that could be applied in any context to (1) identify locally salient ways of expressing distress; (2) develop tools for quantitatively measuring this distress; and (3) compare, statistically and ethnographically, how local expressions of distress; map onto international, biomedical characterizations of anxiety and depression. Our studies took place in India and Haiti, developing countries with limited psychiatric infrastructure, where stigma surrounding psychiatric disorders is strong. Although the approach outlined in this article could be applied anywhere, it would be especially useful when discussion of distress in biomedical terms is socially unacceptable or unfamiliar.
We used a process of epidemiologic surveys bracketed by phases of ethnography to establish locally derived scales to measure distress. Particularly important were the ethnographic phases that started and ended our research. Our emphasis on the presentation of ethnographic results along with quantitative results departs somewhat from previous scholars’ work on mixed methods scale development and testing. While most such works rely on ethnography to develop scales, they often unintentionally undermine its importance by emphasizing only the quantifiability of the resulting scales (see Bolton 2012; DeVellis 2012).
We maintain an emphasis on ethnography for both practical and ideological reasons. It creates transparency by giving readers access to primary data about local use and experience of idioms. Presenting ethnography alongside quantitative scales helps correct for the usual emphasis on solely quantifiable results. Ethnography illuminates potential problems with standard depression and anxiety screeners, such as the danger of overdiagnosis or points of potential incomprehensibility. Finally, sensitivity to ethnographic data could affect the way the scales are used in the future. For example, it might encourage mental health professionals working in Haiti to adopt local terms for discussing distress, such as thinking too much, instead of clinical terms like depression for mental health screening. Although additional research would be needed before thinking too much could replace depression, privileging local forms of communication might ultimately furnish more accurate results, enhance acceptability, and improve outcomes.
The mixed methods approach to mental health assessment presented in this article is valuable because it facilitates cross-cultural comparisons by linking local idioms of distress to depression and anxiety. At the same time, we maintain sensitivity to the plurality of distress expressions and experiences by developing and testing locally derived tools for measuring mental health. This research agenda respects culturally defined illnesses and acknowledges the contextuality of all illness experiences, while still maintaining the comparative enterprise of cross-cultural psychiatry. In doing so, it preserves the best of both worlds from cross-cultural psychiatry and psychological anthropology.
Footnotes
Appendix
Acknowledgments
We thank Michael Kramer for reviewing an earlier version of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author's research was supported by the National Science Foundation, the Fulbright-Hays Foundation, and the Lemelson/Society for Psychological Anthropology fellowship. The second author was supported by the National Science Foundation and Emory University's Global Health Institute.