
Abstract
Purpose:
To present the successful resolution of a type Ia endoleak in a patient previously treated with a fenestrated Anaconda endograft using a custom-made branched endograft.
Technique:
The limited working length and the retrograde orientation of the renal arteries due to caudal migration of the previous fenestrated endograft required a unique custom-made 5-branched graft configuration designed by COOK Medical (Bloomington, Indiana). This design featured 2 short (10-mm) retrograde branches for the renal arteries, along with an additional branch extending from the main body of the graft to accommodate the contralateral limb of the previous endograft. A .014″ wire was used as a stabilizing “pull-through wire” for the Fustar sheath, providing adequate stability for the challenging catheterization of the target vessels.
Conclusion:
Custom-made branched endovascular aneurysm repair after failed fenestrated Anaconda device is a feasible solution. Thorough planning and complex endovascular techniques may be necessary.
Clinical Impact
This technical report highlights the significant challenges associated with endovascular reintervention following failure of fenestrated endografts. Such reoperations often require customized grafts and advanced endovascular skills. Our experience demonstrates that with appropriate planning, branched endovascular repair (bEVAR) can be a feasible and effective solution for managing failed fenestrated endovascular aneurysm repair (fEVAR) apart from open conversion.
Keywords
Introduction
Fenestrated (fEVAR) and branched (bEVAR) endovascular aneurysm repair have become the first-line treatment option for complex abdominal aortic pathologies in most centers, especially in high surgical risk patients.1,2 New devices and techniques have allowed to overcome significant anatomical challenges, with several companies now offering a range of specific custom-made devices.2–4
Although short-term outcomes in terms of morbidity and mortality are better compared to open repair, the increased rate of reinterventions over time highlight the importance of close follow-up and timely management to ensure long-term treatment success.2–6 In cases of failed previous f/bEVAR, there is no established standard of care regarding the most appropriate technique. 1 The choice of approach is a case-specific decision, influenced by the surgeon’s experience, technical expertise, and the available facilities. Open conversion remains a viable option but is usually associated with prohibitive surgical risk in most patients along with high technical difficulty. Performing a new fenestrated/branched endovascular aneurysm repair (f/bEVAR) within a previous f/bEVAR has been shown to be effective but presents significant technical challenges. 5
The fenestrated Anaconda Endograft (Vascutek, Inchinnan, UK) was introduced in 2011 and offers several features, such as the ability to reposition the body and to position the superior mesenteric (SMA) or celiac trunk (CT) in an anterior augmented scallop, as well as the lack of stent material compromising the position of the fenestrations. 7 Many single- and multi-center studies report favorable outcomes; however, there is a notable incidence of type Ia endoleaks. 3
We present the case of a late presenting type Ia endoleak after fEVAR with an Anaconda graft, which was treated with a branched custom-made device.
Technique
Patient History and Procedure Planning
A 66-year-old male patient was referred to our hospital for management of an enlarging abdominal aortic aneurysm (AAA) secondary to a type Ia endoleak following previous treatment with a 3-fenestrated graft. He had been diagnosed 5 years ago with a juxtarenal AAA with a maximum diameter of 8 cm and had been treated with a 3-fenestrated Anaconda graft (Vascutek, Inchinnan, UK) in another hospital. During follow-up, the patient developed a late type Ia endoleak and subsequently presented with an enlarging 11 cm aneurysm (Figure 1).
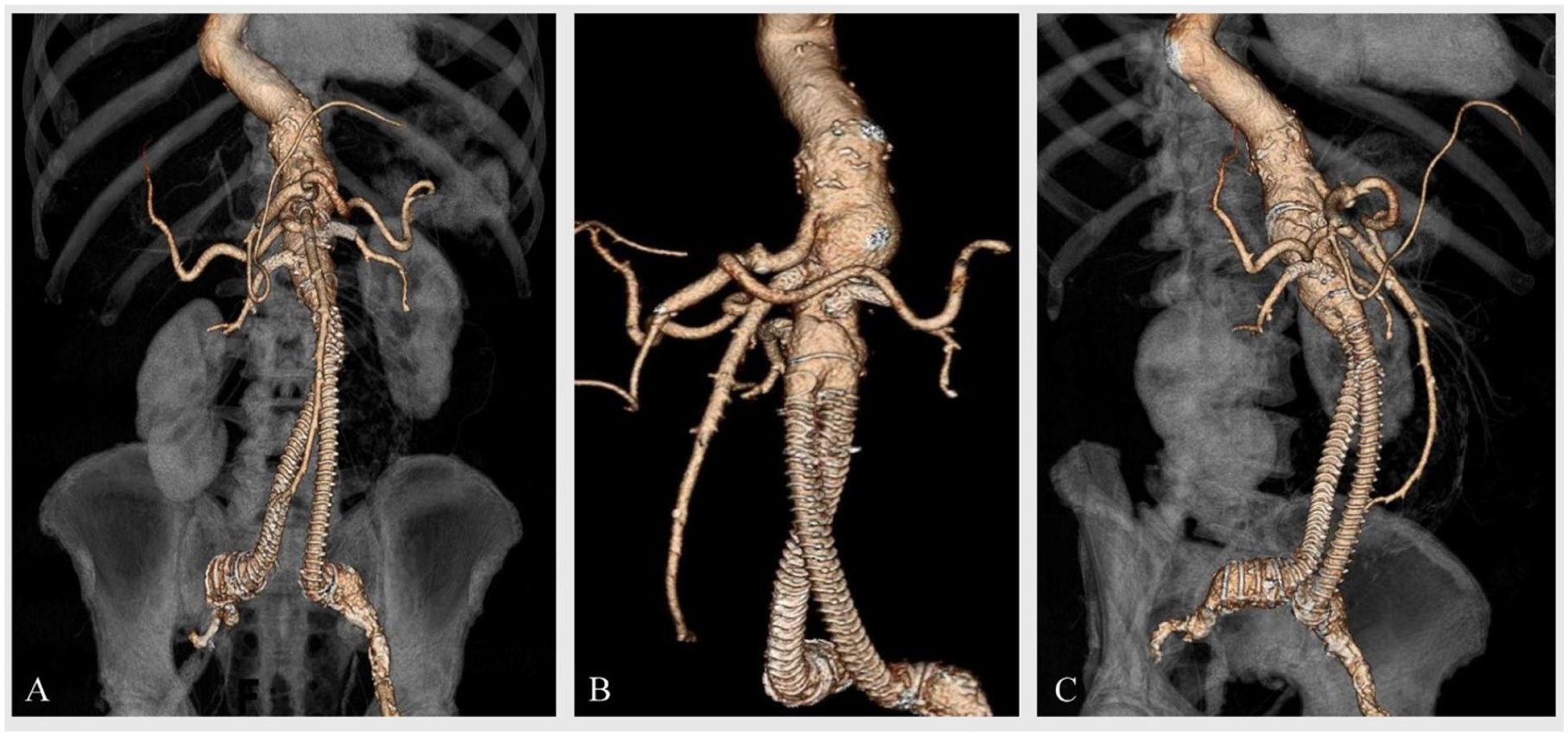
Preoperative CT angiography of an 11 cm aneurysm due to type Ia endoleak after treatment with a fenestrated Anaconda endograft: (A) 3D reconstruction, (B) LAO projection, and (C) RAO projection.
The patient’s medical history is notable for multiple comorbidities. These include 2-vessel coronary artery disease, treated with percutaneous transluminal coronary angioplasty (PTCA), ischemic mitral valve insufficiency, and peripheral artery disease (PAD) classified as stage IIb according to the Fontaine Classification in the left leg. In addition, the patient presents with bilateral popliteal artery aneurysms. Surgical history includes a femoro-popliteal bypass on the right leg and endarterectomy of the right internal carotid artery. Moreover, the patient has type II diabetes mellitus, hypertension, obesity, chronic kidney disease (stage III), and history of heavy smoking (46 pack-years), with cessation reported 6 years ago.
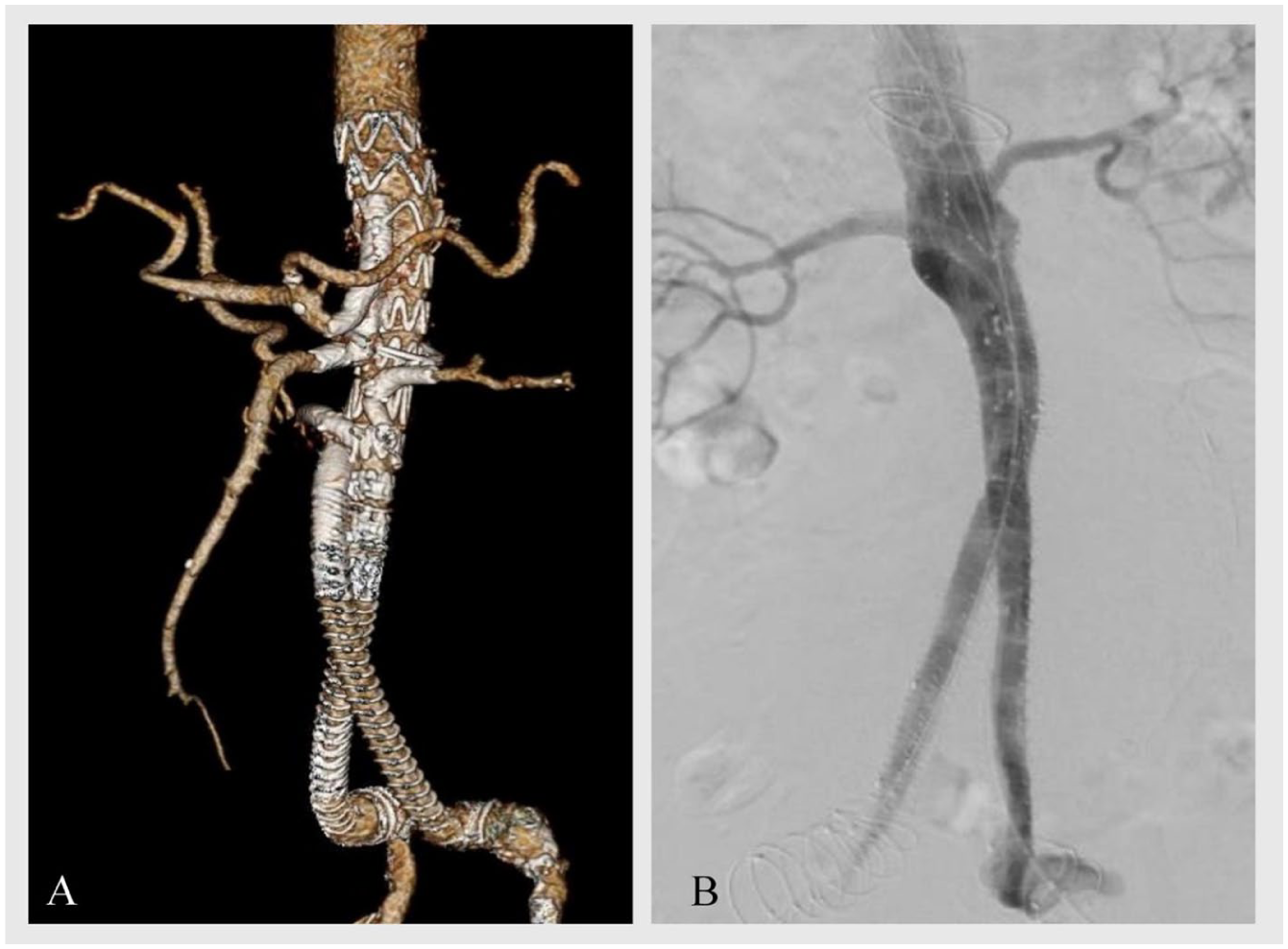
Therefore, the multidisciplinary aortic board deemed the patient unfit for open surgery, and an endovascular approach was consequently selected. The previously implanted Anaconda endograft had a main body proximal diameter of 30 mm with an inner lumen diameter approximately 27 to 28 mm. The proximal landing zone was in the level of visceral aorta incorporating the SMA and the renal arteries. The iliac limbs had an outer diameter of 14 mm, and an inner lumen diameter of 10 to 11 mm, with bilateral distal landing above common iliac artery bifurcation. The distance between the lowest renal artery to endograft bifurcation was measured to be 25 mm. Apart from the CT, the SMA, and the right and left renal arteries (RRA, LRA) had been previously stented with bridging stent-grafts measuring 8.5 mm, 6.5 mm, and 6 mm in internal diameter, respectively. The exact bridging stent used for each target vessel could not be determined. The fenestrated graft appeared to be caudally migrated leading to the subsequent retrograde orientation of the renal bridging stent-grafts (Figure 2), adding an additional significant challenge. The clock position of the renal arteries was located at 11:30 and 1:30 o’ clock position, respectively, while SMA was located at 12:00 o’clock and the contralateral limb at approximately 11:45 o’ clock. Taking into account all the technical challenges, a COOK Medical (Bloomington, Indiana) Custom-made (CMD) 5-branched device was ordered (Figure 3). The complex anatomy of the aneurysm and the visceral vessels due to the previous fenestrated graft demanded a unique CMD graft configuration. Specifically, the low-profile graft consisted of 2 antegrade 8 mm branches for the CT and the SMA and 2 retrograde and short, 10-mm-length, branches for the renal arteries. Moreover, an extra fifth branch was incorporated to perfuse the contralateral limb, as the neo-bifurcation of the previous graft was too high to accommodate a bifurcated device, even with an inverted aortic limb, without significantly increasing the aortic coverage. An incorporated bifurcated graft configuration was not feasible due to short length of lowest renal to previous endograft bifurcation. In addition, an alternative option would have been to land in the ipsilateral limb and perform a femoro-femoral crossover bypass. However, due to the patient’s comorbidities, including PAD, obesity, and diabetes, this approach would be associated with a higher risk of graft occlusion and infection.

Caudal migration of a 3-fenestrated Anaconda endograft and retrograde orientation of the renal bridging stent-grafts.
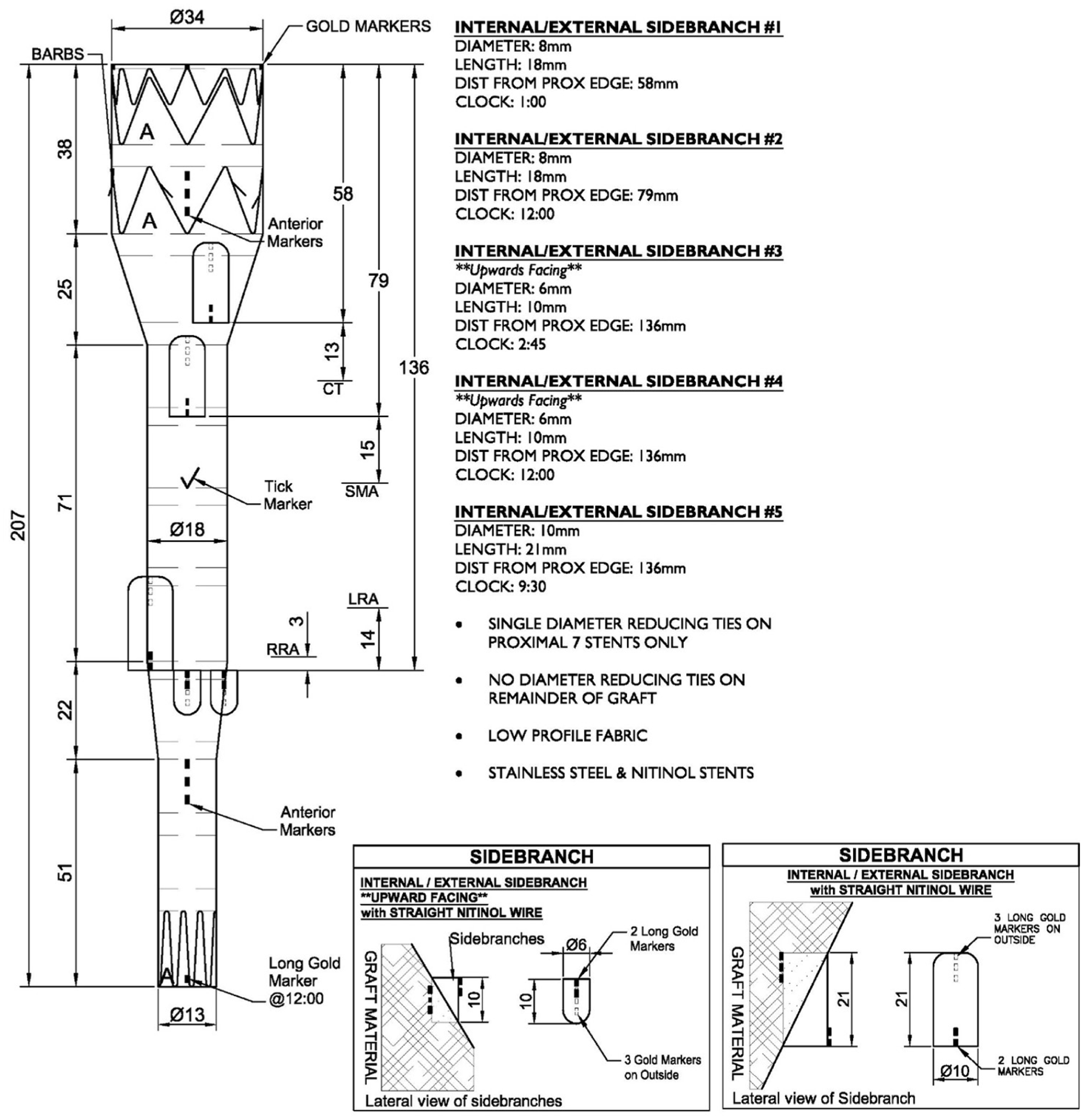
Custom-made 5-branched endograft plan with a 34 mm proximal and a 13 mm distal diameter, incorporating two 10 mm retrograde branches for the renal arteries and 1 extra branch for the contralateral limb.
Procedure
The procedure was performed under general anesthesia, with bilateral percutaneous femoral access using ProGlide devices (Abbott Vascular, Santa Clara, California) in a pre-close technique. Activated Clotting Time (ACT)-guided heparinization was carried out with a target of 250 to 300 seconds and computed tomography fusion guidance was used. Following predilatation with 16Fr and 18Fr dilators, the custom-made device was advanced through the right access. Simultaneously, an angiographic catheter was advanced via the left access. Then, the COOK Medical Custom-Made 5-branched device was introduced and positioned. An angiography was performed and the device was fully deployed under fluoroscopy. The device sheath was then replaced by an 18Fr introducer sheath (Oscor Inc., Palm Harbor, Florida). The retrograde renal branches and the respective arteries were catheterized via the right femoral access under fusion guidance using a soft Terumo 0.035″ hydrophilic guidewire and a 5F Bernstein II diagnostic catheter (IMPRESS, Merit Medical Systems, South Jordan, Utah) (Figure 4A). Following renal artery catheterization, the soft wire was exchanged for a Rosen wire, followed by the introduction of 7Fr COOK flexor sheath into the renal artery. The bridging stent-grafts were advanced over the sheaths, which were subsequently retracted, allowing for stent deployment. A Viabahn 6 x 50 mm stent-graft (W.L. Gore & Associates, Flagstaff, Arizona) was deployed in the LRA and a BeGraft Plus 6 x 38 mm stent-graft (Bentley Innomed GmbH, Hechingen, Germany) in the RRA. The visceral antegrade branches and respective arteries were then catheterized via the right femoral access using a 10Fr × 55 cm Fustar steerable sheath (Lifetech Scientific, Shenzhen, China). To increase stability during the “up and over” access, before inserting the steerable sheath, a .014″ wire was inserted through the sheath bended in the middle and rerouted back outside the steerable sheath. Both the sheath and bended wire were inserted through the 18Fr femoral access sheath, and both ends of the wires were secured with clamps in order to have a stabilizing “pull through-and-through wire” (Figure 5). In addition, a 7Fr x 70 cm COOK flexor sheath was introduced inside the steerable sheath. Catheterization was first performed for the SMA using a soft Terumo wire and a Bernstein II catheter (Figure 4B). After successful catheterization and exchange of the soft wire with a Rosen wire, the SMA bridging stents (BeGraft Plus 8 x 57-mm and iCover 8 x 17-mm [iVascular, Barcelona, Spain]) were advanced and deployed. The CT was then catheterized using the same “up and over” access and catheterization techniques and 2 BeGraft plus stents (8 x 57 mm + 8 x 27 mm) were deployed (Figure 4C).
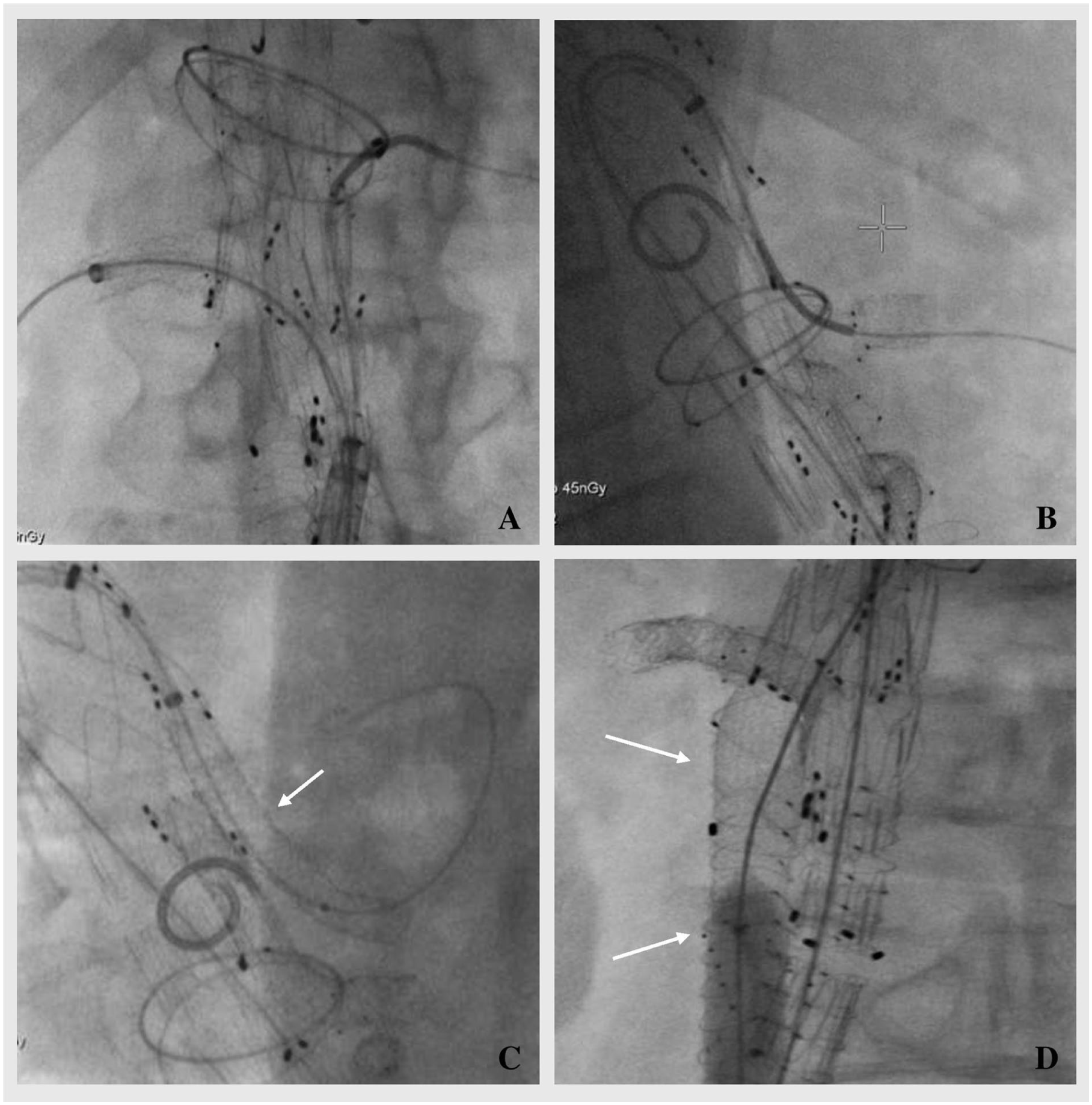
Procedure of a custom-made 5-branched EVAR to treat a type Ia endoleak after prior treatment with a 3-fenestrated Anaconda endograft. (A) Catheterization of the renal arteries. (B) Catheterization of the superior mesenteric artery using the “up and over” access. (C) Deployment of 2 BeGraft plus stents in the celiac trunk. (D) Extension of the branch for the contralateral limb with a Viabahn 11 x 100 mm stent and molding with a 10 mm PowerFlex Pro balloon catheter.
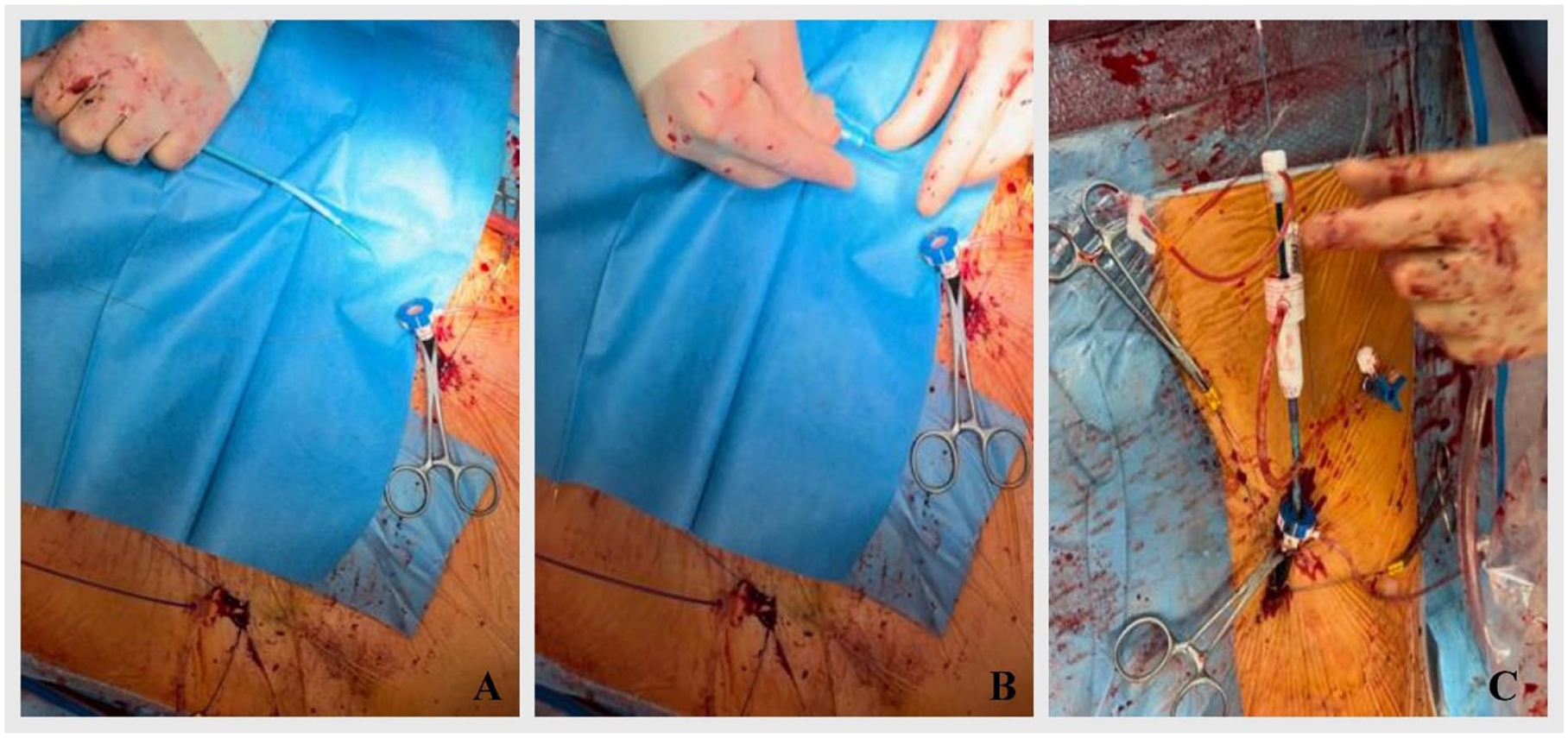
“Pull through-and-through” wire technique to increase stability during the “up and over” access: (A, B) Prior to the insertion of the Fustar steerable sheath, introduction of a .014″ wire through the sheath which was bended in the middle and rerouted back outside the steerable sheath. Then, insertion of both the sheath and the bended wire through the 18Fr femoral access sheath and securing of both ends of the wires with clamps. (C) Final sheath configuration.
The final branch for the contralateral limb (left iliac) was catheterized from the left femoral access and extended using a Viabahn 11 x 100 mm stent, which was molded using a 10 mm PowerFlex Pro balloon catheter (Cordis, Hialeah, Florida) (Figure 4D). The final angiographic assessment revealed proper endograft positioning and no evidence of endoleak (Figure 6).
(A) Postoperative CT angiography and (B) final angiography of a custom-made 5-branched EVAR performed to treat an 11 cm aneurysm due to type Ia endoleak after 3-fenestrated Anaconda endograft.
Postoperative
Postoperatively, the patient developed spinal cord ischemia manifesting as paraplegia, which was managed with spinal drainage and physiotherapy, leading to progressively improved neurological function and near-complete recovery by discharge. The renal function remained normal (serum creatinine: 1.1 mg/dL; eGFR: 70 mL/min/1.73 m2). The patient was discharged on postoperative day 10 with continued anticoagulation therapy (rivaroxaban 20 mg), which he had been receiving preoperatively, and antiplatelet therapy (aspirin 100 mg). At 30-day follow-up, computed tomography angiography (CTA) revealed no evidence of endoleak and no signs of device or bridging stent-grafts failure.
One year postoperatively, the patient presented with elevated inflammatory markers, and graft infection was subsequently confirmed by PET-CT scan, localized to the region of the iliac limbs. Given the high operative risk associated with complete graft explantation, a more conservative approach was undertaken. This involved sac debridement with evacuation of inflammatory material, explantation of the iliac stents, and reconstruction using a bovine pericardium graft. In the last follow-up, the patient remained clinically stable, and the CTA revealed no presence of endoleaks or target vessel occlusion.
Discussion
The fenestrated Anaconda graft is a viable option for the treatment of complex AAA3,8,9; however, increased incidence of type Ia endoleak after fenestrated Anaconda has been described in the literature, directly or shortly postoperatively. 10 In many cases, it resolves spontaneously, or it requires minimal reintervention. 3 In this case, the endoleak presented 6 years after the initial surgery. In our case, we believe that the limited proximal fixation of the Anaconda graft was the cause of graft failure. The Anaconda endograft relies solely on proximal rings for sealing and lacks a metallic scaffold at the proximal neck, which may provide insufficient radial force and fixation strength, leading to gradual graft migration and the development of a type Ia endoleak.
The use of fenestrated or branched endovascular devices in cases of previously failed EVAR has been documented in the literature, yielding favorable outcomes, despite the technical challenges.11–13
However, only few cases of f/bEVAR performed after a prior f/bEVAR have been documented. Spanos et al 14 reported the first case of fEVAR after failed fEVAR with favorable outcomes. The authors describe challenges related to the alignment of the new device and the cannulation of the fenestrations, for which advanced endovascular bailout techniques were used. Fernandez-Alonso et al 15 described a case of type Ia endoleak 10 years after fenestrated Anaconda endograft and treated the patient with a CMD 4-branched device. In this case, increased aortic coverage was necessary since the endograft extended approximately 86 mm above the CT, while the authors reported long distances between the branches and the respective ostium of the TVs (21 mm and 24 mm) in order to be able to accommodate a bifurcated device with an inverted limb. In the reported case, due to the unique configuration of the endograft, the aortic coverage was limited to 68 mm while the distances between the branches and the TVs ostium were approximately 10 mm, in line with standard practice.
The “pull through-and-through wire” technique has previously been described by Panuccio et al. 16 The authors stress that this technique provides great stability and reduces the procedure time compared with transaxillary approach. To the best of our knowledge, this technique has not been described with the use of a steerable sheath. Based on our experience, the combination of this technique with the use of a steerable sheath provided enhanced flexibility and stability. This approach enabled successful catheterization of severely angulated TVs without the need for upper extremity access, while also facilitating precise intravascular maneuvers.
Graft infection in patients with prior complex endovascular repair remains a challenging clinical problem. 17 In our case, the etiology is uncertain, but prior repair at the same site and implantation of 2 different devices over several years may have contributed. Given the localized nature of the infection, the iliac segment was surgically removed and replaced with a bovine pericardial graft. Considering the high complexity and prior interventions, complete graft explantation would have entailed significant operative risk; thus, a targeted conservative approach was considered appropriate. In such complex cases, careful risk-benefit assessment is crucial to optimize patient outcomes. 18
The reported case presented multiple technical challenges, and complex endovascular techniques were employed, including steerable sheaths and through-and-through wires, which provided enhanced stability, minimized manipulation, and allowed for more precise catheterization.19,20 First, the catheterization of the renal arteries with retrograde configuration due to the caudal migration of the previous fenestrated endograft was achieved via retrograde 10-mm branches. The 10-mm short retrograde branches were required due to the limited space between the 2 grafts, which restricted major manipulations, as well as the high and angulated position of the renal arteries. In addition, the neo-bifurcation of the Anaconda graft was positioned too high to accommodate even a bifurcated device with an inverted limb, necessitating a unique configuration and the use of an additional fifth branch for the contralateral limb.
This rare graft design underlines the importance of thorough planning in such complex cases and highlights that, in experienced centers, CMD devices can be utilized to treat a wide range of aortic pathologies.
Conclusion
Endovascular conversion with CMD bEVAR in case of a failed fEVAR is a viable technique, but it presents with technical challenges and demands rigorous planning and expertise on complex endovascular techniques.
Footnotes
Ethical Considerations
Informed consent was obtained from the patient for the use of clinical data related to aortic pathology for research and publication purposes, as part of a broader study approved by the Ethics Committee of Ludwig-Maximilians-Universität (LMU), Munich (Project Number: 22-0961/2020).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: N.T. and J.S. are consultants for COOK Medical and receive speaking fees from Bentley Innomed. All other authors declare no conflicts of interest.