
Abstract
Introduction:
Rise in anticoagulant use increases the likelihood that patients undergoing carotid artery stenting (CAS) are on anticoagulants. This complicates postprocedural antithrombotic management, as dual antiplatelet therapy is standard to reduce stent-related complications. To mitigate bleeding risks, patients on anticoagulants often briefly receive a single antiplatelet agent instead. Based on clinical practice, we hypothesized this regimen may increase in-stent stenosis, potentially raising the risk of recurrent ipsilateral transient ischemic attack or ischemic stroke.
Design:
Single-center, retrospective cohort study at a tertiary referral center.
Methods:
Patients with significant carotid artery stenosis treated with CAS (May 2005 to September 2024) were categorized into the anticoagulant (with or without antiplatelet therapy) or antiplatelet group (mono therapy or dual therapy). Primary outcome was in-stent stenosis at short-term (30 days to 8 weeks) and mid-term (1 year) follow-ups. Secondary outcomes included 30-day composite of thromboembolic and bleeding complications, reintervention, and other procedure-related adverse events. For the sensitivity analysis, multiple imputation was performed to address missing data.
Results:
Among 327 patients, 274 (83.8%) received antiplatelets and 53 (16.2%) anticoagulants. In-stent stenosis rates did not differ at short term (2.1% vs 2.8%, P = 1.00) but were higher in the anticoagulant group at mid-term (21.6% vs 7.4%, P = .01; adjusted odds ratio [OR] 3.29, 95% confidence interval [CI] 1.16-9.39), with more symptomatic cases (10.5% vs 1.0%, P = .01). All occurred in direct oral anticoagulant (DOAC) users, 75% also on single antiplatelet therapy. However, sensitivity analysis yielded a non-significant association (OR 1.29, 95% CI 0.54-3.07, P = .56). Secondary outcomes showed no significant differences.
Conclusion:
Anticoagulant use, specifically DOACs, appears associated with increased mid-term (symptomatic) in-stent stenosis in the primary analysis. However, this association was attenuated in the sensitivity analysis. Prospective studies are warranted to guide post-CAS antithrombotic therapy in anticoagulated patients.
Clinical Impact
As the number of patients undergoing carotid artery stenting while receiving oral anticoagulation continues to rise, clinicians face uncertainty regarding optimal post-procedural antithrombotic therapy. This study identifies a potential association between anticoagulant use, particularly direct oral anticoagulants, and increased mid-term carotid in-stent stenosis. Confirmation in prospective studies is required. The innovation of this study lies in addressing an important evidence gap in carotid intervention practice, providing the first comparison of in-stent stenosis outcomes between anticoagulant- and antiplatelet-treated patients.
Introduction
In-stent stenosis or occlusion after carotid artery stenting (CAS) can cause new cerebral ischemic events, potentially negating the benefits of the initial treatment for carotid stenosis. The reported incidence of in-stent stenosis after CAS varies widely in the literature, partly due to the lack of standardized diagnostic criteria.1,2 A meta-analysis of 5 randomized controlled trials reported a 10.0% prevalence (95% confidence interval [CI] 6.0-16.3) of severe restenosis (≥70%) or occlusion over a mean 62-month follow-up. 3 In another study, evaluating in-stent stenosis progression and its clinical impact, 20.2% developed a ≥50% stenosis over a mean follow-up of 51.7 months. This progression was associated with ipsilateral transient ischemic attacks (TIAs) or ischemic strokes in 11.0% vs 2.5% without significant stenosis. 4 These findings highlight that strategies aimed at minimizing thromboembolic events and mitigating clinical impact of in-stent stenosis may be crucial.
Current guidelines from the Society for Vascular Surgery (SVS) and European Society for Vascular Surgery (ESVS) recommend dual antiplatelet therapy (DAPT) during the periprocedural period and for at least 4 weeks postoperatively to minimize the risk of acute stent thrombosis or embolization triggered by intimal injury. However, limited data exist regarding optimal platelet inhibition strategies following CAS.1,5 Most recommendations are extrapolated from cardiology. 1 Only 2 small randomized controlled trials have evaluated DAPT in patients with symptomatic and asymptomatic carotid stenosis. Both showed that DAPT reduces the 30-day risk of ipsilateral thromboembolic events compared with single antiplatelet therapy (SAPT), without significantly increasing bleeding risk.6,7
The introduction of direct oral anticoagulants (DOACs), such as rivaroxaban and apixaban, has further complicated antithrombotic decision-making in CAS. These agents are increasingly used to treat conditions including venous thromboembolism, ventricular thrombus, and atrial fibrillation (AF). Over the past 15 years, DOAC use among patients with AF has increased, with median rates increasing from 10% in 2013 to 49% in 2020 in the United States. 8 This growing prevalence increases the likelihood of encountering patients requiring CAS already on DOAC therapy, raising concerns about balancing thromboembolic and bleeding risks. However, data on DOACs for stroke prevention and CAS remain limited.1,5 The American Heart Association and American Stroke Association discourage the use of vitamin K antagonists (VKAs) for secondary stroke prevention in non-cardioembolic stroke due to bleeding risks, but emphasize the need for further research on the efficacy of DOACs, either alone or combined with a platelet inhibitor vs DAPT. 9
Based on clinical experience, patients undergoing CAS and treated with anticoagulants (DOACs or VKAs, with or without additional antiplatelet therapy) are hypothesized to have a higher incidence of in-stent stenosis or occlusion and an increased risk of recurrent TIA or stroke compared with those receiving antiplatelet therapy alone. To explore this, a single-center retrospective study was conducted comparing periprocedural efficacy (incidence of in-stent stenosis or occlusion) and safety (thromboembolic and bleeding risk) during short-term and mid-term follow-ups in patients who underwent CAS for carotid artery stenosis, receiving either antiplatelet therapy alone vs anticoagulation (with or without antiplatelet therapy).
Materials and Methods
Study Design
This single-center, retrospective cohort study was conducted at a tertiary referral center. All consecutive patients with primary or recurrent (a)symptomatic significant (≥50%) carotid artery stenosis who underwent CAS at our center between May 2005 and September 2024 were eligible. Before the implementation of the latest electronic patient record system in December 2017, medical record numbers were maintained separately. From December 2017 onward, eligible patients were identified using the Diagnosis Treatment Combination system, a 9-digit code that encompasses all hospital activities. Patients were excluded if they underwent combined procedures (eg, hybrid carotid interventions or CAS performed alongside coronary artery bypass grafting during the same admission), if the procedure resulted in technical failure (ie, no stent placement), if treatment was non-deferred, defined as CAS within 48 hours of symptom onset, or if they underwent balloon angioplasty without stenting, had a carotid aneurysm, or underwent angioplasty with stenting of a carotid artery bypass.
The institutional review board granted dispensation in accordance with Dutch law on requirements for retrospective patient-based medical research. As participants were not subjected to procedures nor required to follow behavioral rules, the study did not fall within the scope of the Dutch Medical Research Involving Human Subjects Act (WMO), and informed consent was therefore not required. All patient-related data were processed pseudonymously and stored electronically in compliance with the Declaration of Helsinki’s ethical principles for medical research involving human subjects.
CAS Eligibility Criteria, Procedure, and Monitoring
Patients’ eligibility for CAS was discussed by a multidisciplinary board that included a vascular surgeon, stroke neurologist, and interventional radiologist. Our hospital followed a carotid endarterectomy (CEA)-first strategy until March 2020, with CAS reserved for patients considered high risk for open surgery. However, due to logistical constraints during the COVID-19 pandemic, a CAS-first approach was adopted. Hereafter, a patient-tailored approach was implemented. Carotid artery stenting was performed under local anesthesia with monitoring by an anesthesiology team in the angio-suite. Complete eligibility criteria, technical details, and intraoperative and postoperative monitoring have been reported elsewhere. 10 In addition, until 2014, use of embolic protection devices was at the interventionalist’s discretion; afterward, it was not standard practice. 11
Antithrombotic Management
At our institution, standard practice is to initiate DAPT at least 3 days before CAS. Patients not already on DAPT received a loading dose of 300 mg clopidogrel and/or 300 mg acetylsalicylic acid, followed by daily maintenance therapy with clopidogrel 75 mg and acetylsalicylic acid 80 mg or carbasalate calcium 100 mg post-procedure. Patients on DOACs and VKAs temporarily discontinued anticoagulation 2 to 3 days before CAS and switched to DAPT, unless there was a strict indication to continue anticoagulant therapy (eg, recent percutaneous coronary intervention [PCI]). In such cases, a single platelet inhibitor was added to the DOAC or VKA regimen. After sheath placement, heparin was administered as a single bolus of 50 IU/kg to a maximum of 5000 IU. Since 2009, clopidogrel sensitivity has been assessed using the VerifyNow™ system (Werfen, Barcelona, Spain). For partial responders (platelet reaction unit between 180 and 230), clopidogrel dose was doubled; non-responders (platelet reaction unit >230) switched to prasugrel 10 mg daily or ticagrelor 90 mg twice a day. Dual antiplatelet therapy was continued for 6 months, after which the patient transitioned to SAPT, unless there was another indication to continue DAPT. If a platelet inhibitor was used with a DOAC or VKA, this regimen continued for at least 1 month, also depending on the indication. In recent years, patients on VKAs before CAS have been preferentially switched to DOACs after CAS.
Follow-up
Patients attended follow-up appointments at our outpatient clinic 30 days to 8 weeks and 1 year after the intervention, with additional visits scheduled as clinically indicated. Before each visit, trained staff from our vascular laboratory conducted duplex ultrasound (DUS) scans to assess peak systolic velocity (PSV), B-mode diameter reduction, end-diastolic velocity, and the internal carotid artery (ICA)/common carotid artery PSV ratio. Stenosis classification followed consensus criteria for diagnosing ICA stenosis using gray-scale and Doppler ultrasonography. 12 If a significant restenosis (≥50% stenosis) was identified via DUS, further evaluation with computed tomography angiography (CTA) or magnetic resonance angiography (MRA) or repeat DUS was performed. Decisions regarding reintervention were made by a multidisciplinary board.
Outcomes
Primary outcome was the rate of in-stent stenosis, defined as a stenosis degree of ≥50% on DUS and/or CTA or MRA, assessed in the short term (30 days to 8 weeks) and mid-term (1 year). The stenosis was considered symptomatic in the presence of carotid territory symptoms.
Secondary outcomes included the composite rate of any death, any stroke (ischemic or hemorrhagic) or TIA within 30 days of the index procedure. Cerebrovascular accident was defined as an acute neurological event with focal symptoms lasting <24 hours (TIA) or ≥24 hours (stroke), assessed by a stroke neurologist. Other outcomes were reintervention during follow-up and a composite of cerebral hyperperfusion syndrome (CHS), myocardial infarction or cardiac complications requiring intervention, unplanned intensive care unit admission, and pseudoaneurysm within 30 days. Cerebral hyperperfusion syndrome was defined as new neurological symptoms or radiological findings within 30 days, accompanied by hyperperfusion on imaging or systolic blood pressure >180 mm Hg, without evidence of new cerebral ischemia or other causes. 13 Safety outcomes included a composite of major and non-major bleeding, defined by the International Society on Thrombosis and Haemostasis, encompassing intracranial hemorrhage and surgical site bleeding.14,15
Data Collection
Data included demographics, baseline characteristics, treatment time parameters, type of stent used, antithrombotic therapy post-intervention, primary and secondary outcomes, and duration between treatment and follow-up. Impaired renal function was defined as serum creatinine ≥1.5 mg/dL prior to intervention or dialysis dependency.
Statistical Analysis
Demographic and clinical variables were summarized using percentages for categorical variables and means (±SD) for continuous variables. Follow-up data were updated as of December 2024. Normality of continuous variables was assessed using the Shapiro-Wilk test. Normally-distributed data were analyzed using independent samples t tests and for skewed continuous variables, the Mann-Whitney U test was used. Categorical variables were compared using Fisher’s exact test or chi-square test. For binary outcomes, unadjusted odds ratios (ORs) were calculated, and adjusted ORs (aORs) were determined with logistic regression, accounting for potential confounders including age, sex, hypertension, cardiac history, and impaired renal function. Initially, an available case analysis was performed. To assess the impact of missing data on the results, multiple imputation using chained equations (with 5 imputations) was performed. Variables were imputed appropriately (Supplemental Appendix 1). The imputed datasets were pooled using Rubin’s Rules to combine estimates and standard errors appropriately. Fraction missing information (FMI) and relative efficiency (RE) were assessed to evaluate the extent of missing data and the robustness of the imputation process. If a patient switched from antiplatelet regimen to anticoagulant therapy (with or without SAPT/DAPT) or vice versa between the 30-day and 1-year follow-ups, the patient was assigned to the therapy used for the longer duration. All statistical analyses were conducted using SPSS, version 30.0 (IBM Corp, Armonk, New York, 2024).
Results
A total of 382 patients were assessed for eligibility, of which 327 met the inclusion criteria (Figure 1). Among them, 274 patients (83.8%) were assigned to the antiplatelet group, and 53 patients (16.2%) were assigned to the anticoagulant group (37 [69.8%] receiving DOAC). Patients in the anticoagulant group were significantly older than those in the antiplatelet group and had higher prevalences of hypertension, cardiac disease, impaired renal function, and, inherent to the assigned group, AF. Second-generation (mesh) carotid stents were used in 87.2% of patients in the antiplatelet group and 81.1% of patients in the anticoagulant group, with no statistically significant difference between groups. Baseline characteristics of the study population are summarized in Table 1.
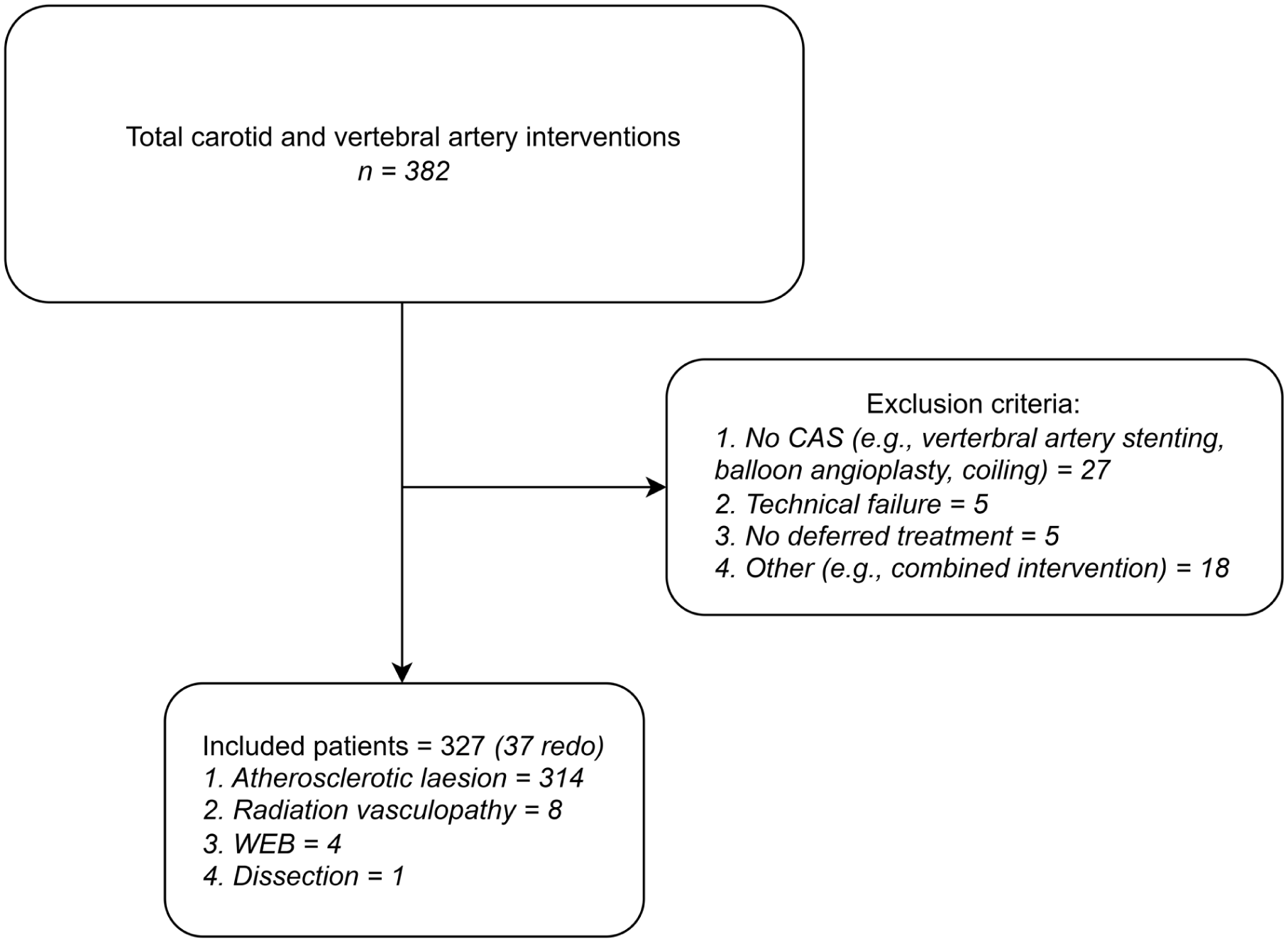
Flowchart of patient inclusion and exclusion. CAS, carotid artery stenting.
Patient Baseline Characteristics.
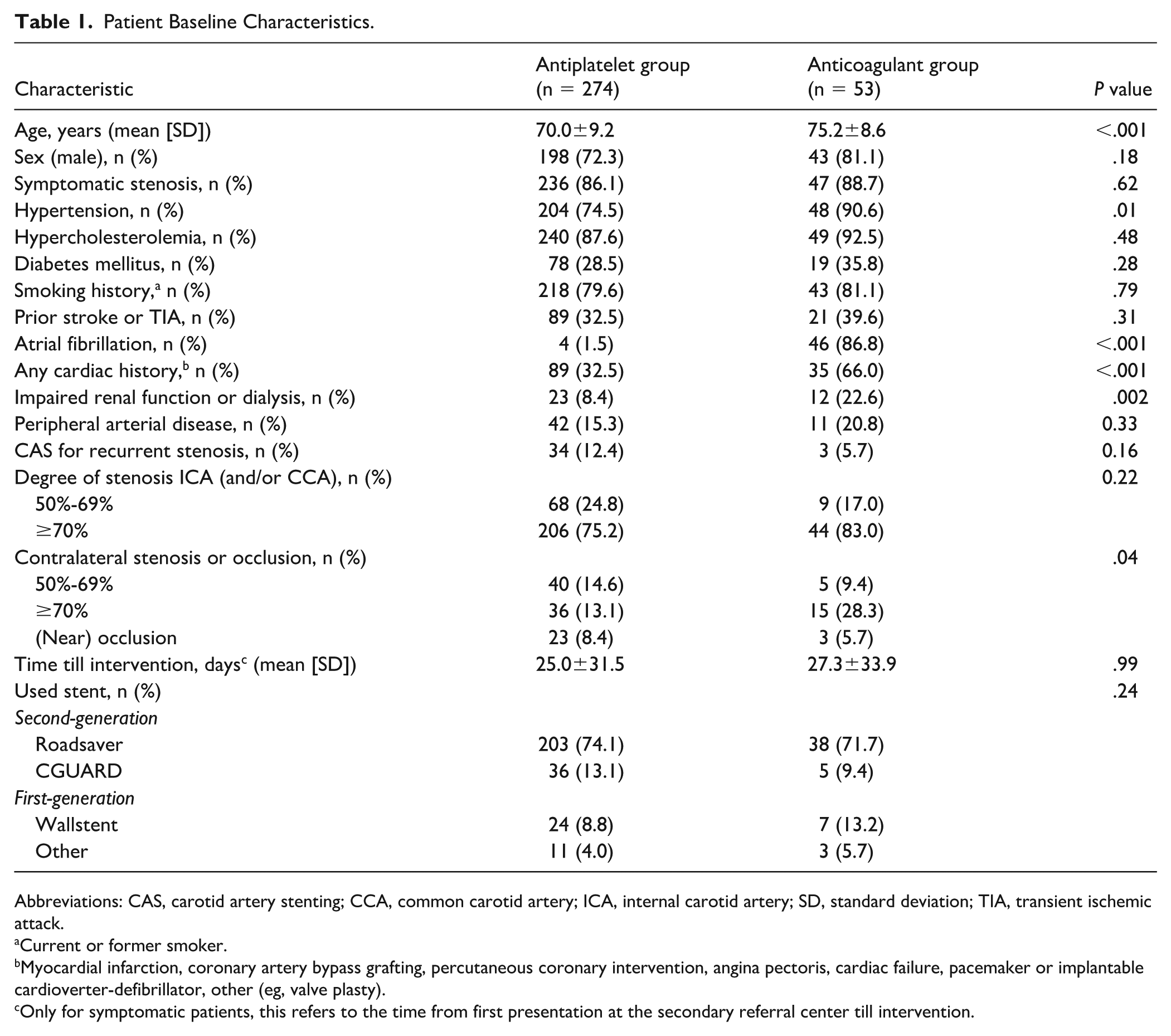
Abbreviations: CAS, carotid artery stenting; CCA, common carotid artery; ICA, internal carotid artery; SD, standard deviation; TIA, transient ischemic attack.
Current or former smoker.
Myocardial infarction, coronary artery bypass grafting, percutaneous coronary intervention, angina pectoris, cardiac failure, pacemaker or implantable cardioverter-defibrillator, other (eg, valve plasty).
Only for symptomatic patients, this refers to the time from first presentation at the secondary referral center till intervention.
During follow-up, comparable proportions of patients were lost to follow-up with imaging, as detailed in Table 2. During follow-up, 3 patients (1.1%) in the antiplatelet group crossed over to the anticoagulant group. Two patients developed AF, while 1 patient initiated a DOAC for peripheral arterial occlusive disease.
Follow-up After CAS Between Groups.
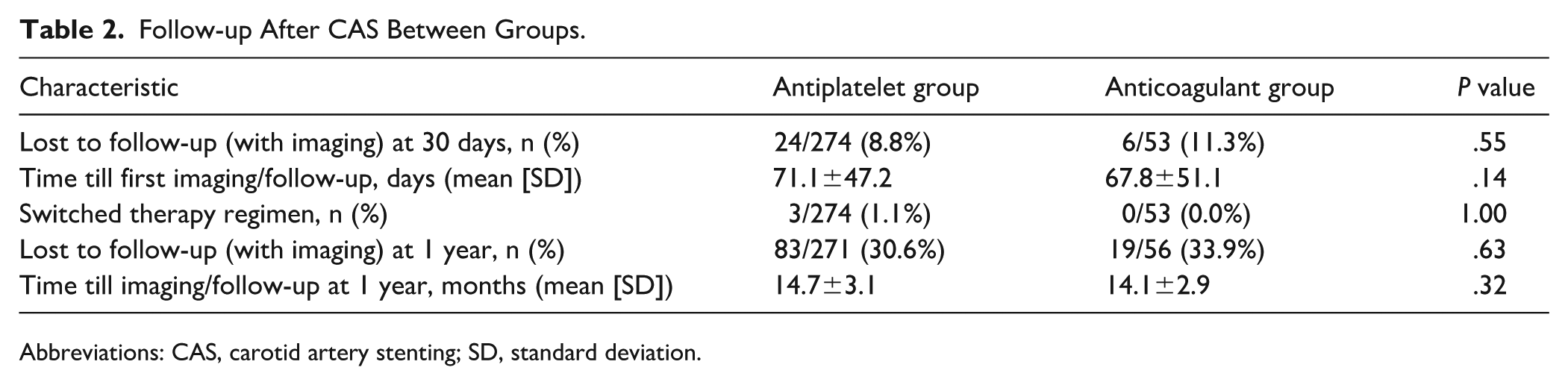
Abbreviations: CAS, carotid artery stenting; SD, standard deviation.
Primary Outcome
The incidence of in-stent stenosis at short-term follow-up was similar between the anticoagulant and antiplatelet groups (2.1% vs 2.8%, P = 1.00). During the 1-year follow-up, in-stent stenosis was significantly more frequent in the anticoagulant group (8 patients, 21.6%) than in the antiplatelet group (14 patients, 7.4%; P = .01). Among the patients with restenosis during the 1-year follow-up, 4 (10.5%) patients in the anticoagulant group and 2 (1.0%) in the antiplatelet group were symptomatic (P = .01), as detailed in Table 3. All patients with in-stent stenosis in the anticoagulant group were using a DOAC, including 2 of the 3 who switched therapy regimens, with 6 (75.0%) also on SAPT. In the antiplatelet group, all but 1 patient with in-stent stenosis at the 1-year follow-up had sufficient platelet inhibition using VerifyNow. The same was observed in the anticoagulant group. In each patient, treatment regimen was altered adequately. The antithrombotic regimen of patients with an in-stent stenosis is summarized in Supplemental Table 1.
Primary and Secondary Outcomes After CAS Between Groups.
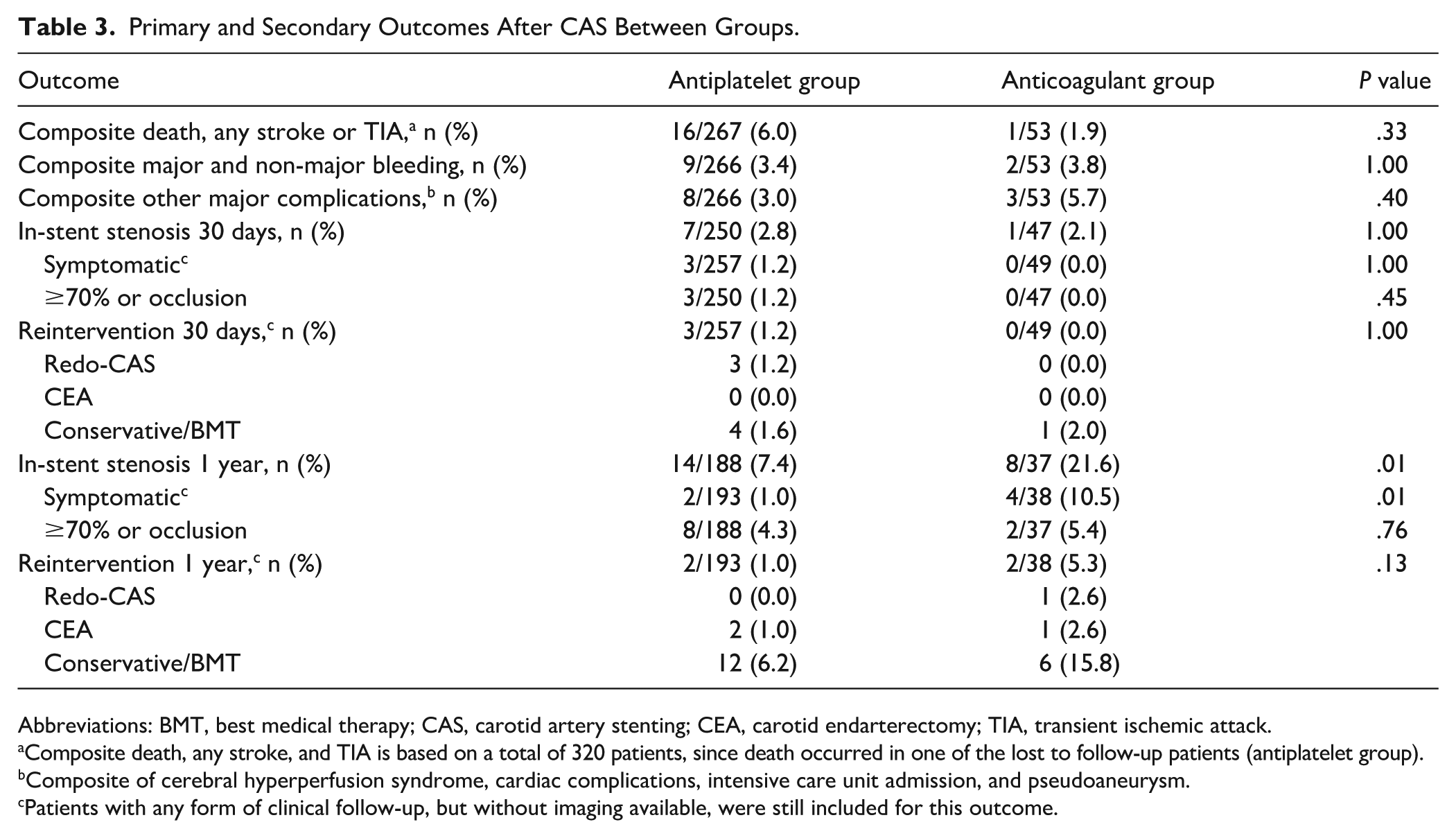
Abbreviations: BMT, best medical therapy; CAS, carotid artery stenting; CEA, carotid endarterectomy; TIA, transient ischemic attack.
Composite death, any stroke, and TIA is based on a total of 320 patients, since death occurred in one of the lost to follow-up patients (antiplatelet group).
Composite of cerebral hyperperfusion syndrome, cardiac complications, intensive care unit admission, and pseudoaneurysm.
Patients with any form of clinical follow-up, but without imaging available, were still included for this outcome.
Use of anticoagulants was associated with an increased risk of in-stent stenosis at 1 year, with an unadjusted OR of 3.43 (95% CI 1.32-8.90, P = .01). The risk remained significantly increased after adjusting for potential confounders (OR 3.29, 95% CI 1.16-9.39, P = .03). However, sensitivity analysis using multiple imputation for missing data yielded a non-significant association (OR 1.29, 95% CI 0.54-3.07, P = .56). The FMI of 0.30 indicates that 30% of the uncertainty in the adjusted OR was due to missing data. Despite an RE of 0.94, suggesting minimal loss of efficiency from the imputation, the attenuation of the OR and loss of statistical significance imply that the associations observed may have been influenced by missing data. No significant differences in short-term in-stent stenosis were observed, as presented in Table 4. For DOACs (27 of 41 with 1-year imaging follow-up) compared with antiplatelets, the aOR was 5.34 (95% CI 1.85-15.38, P = .002). However, this significance was also not sustained in the sensitivity analysis (aOR 1.79, 95% CI 0.70-4.56, P = .22, FMI 0.29, RE 0.95). All restenoses during mid-term follow-up occurred in second-generation stents. In the antiplatelet group, 13 restenoses (92.9%) occurred after Roadsaver stent placement and 1 (7.1%) after CGUARD stent placement; in the anticoagulant group, 7 (87.5%) and 1 (12.5%) restenoses occurred after Roadsaver and CGUARD stent placement, respectively. The difference between groups was not statistically significant (P = 1.00).
Odds Ratios for Treatment Outcomes After CAS: Anticoagulants vs Antiplatelet Therapy, Based on Available Data and Sensitivity Analysis Using Multiple Imputation.
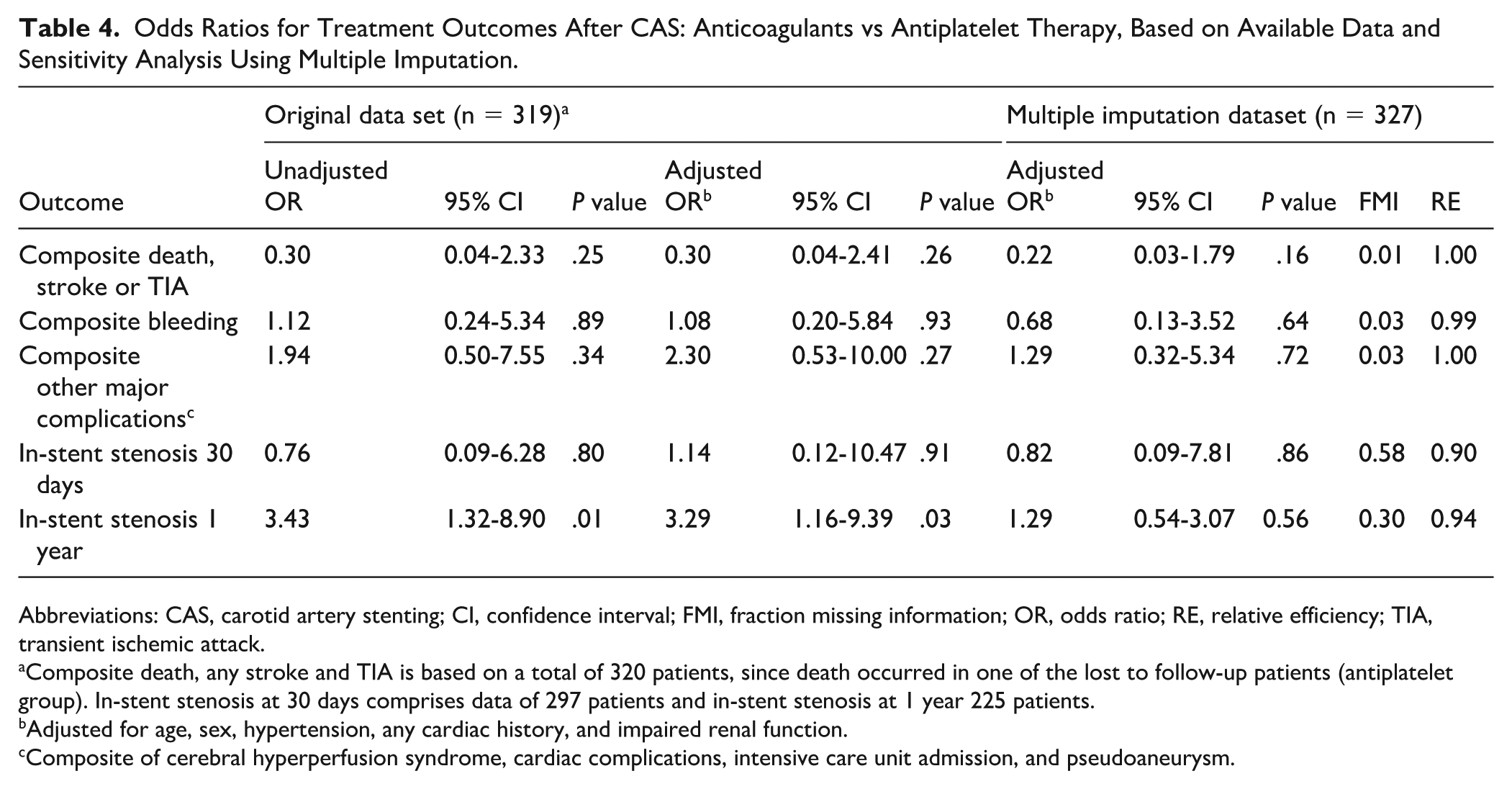
Abbreviations: CAS, carotid artery stenting; CI, confidence interval; FMI, fraction missing information; OR, odds ratio; RE, relative efficiency; TIA, transient ischemic attack.
Composite death, any stroke and TIA is based on a total of 320 patients, since death occurred in one of the lost to follow-up patients (antiplatelet group). In-stent stenosis at 30 days comprises data of 297 patients and in-stent stenosis at 1 year 225 patients.
Adjusted for age, sex, hypertension, any cardiac history, and impaired renal function.
Composite of cerebral hyperperfusion syndrome, cardiac complications, intensive care unit admission, and pseudoaneurysm.
Secondary and Safety Outcomes
The occurrence of all composite outcomes was comparable between groups. Composite outcome of death, any stroke, and TIA was lower in the anticoagulant group (1 patient, 1.9%) compared with the antiplatelet group (16 patients, 6.0%), but this difference was not statistically significant (P = .33). The bleeding risk (major and non-major), reintervention rates, and types were similar between groups, as detailed in Table 3. Unadjusted and adjusted ORs, along with sensitivity analyses, did not demonstrate an increased risk for these outcomes between groups, as shown in Table 4.
Discussion
In this study, comparing anticoagulant therapy (with or without the use of antiplatelets) with antiplatelet therapy after CAS, the use of oral anticoagulants (particularly DOACs) appears to be associated with an increased risk of developing in-stent stenosis in the mid-term, despite most patients being on dual therapy (DOAC combined with SAPT). However, after multiple imputation, this association was attenuated. The use of anticoagulants with or without antiplatelet therapy was not associated with an increased risk of death, any stroke or TIA, or major and non-major bleeding in the short term.
A retrospective single-center study of 91 patients evaluated bleeding risks associated with different antithrombotic regimens in patients with AF undergoing CAS. 16 The study compared DAPT (clopidogrel and aspirin; 25 patients), DOAC combined with clopidogrel (24 patients), and triple therapy (DOAC combined with DAPT; 42 patients). In the triple therapy group, significantly more patients experienced major and clinically relevant non-major bleeding within the first 30 days after CAS. The efficacy outcome, the occurrence of thromboembolic complications, remained comparable for all groups. Only 1 patient in the DOAC combined with clopidogrel group developed in-stent thrombosis with minor stroke symptoms. 16 In our patient population, anticoagulants combined with antiplatelet therapy did not increase bleeding risk, consistent with the aforementioned study. However, findings differ regarding thromboembolic risks, with in-stent stenosis occurring significantly more frequent in the anticoagulant (with or without antiplatelet therapy) group compared with the DAPT group.
In cardiology, several trials have investigated the benefits and risks of combining anticoagulant therapy with antiplatelet therapy compared with antiplatelet therapy alone in patients with acute coronary syndromes, including those undergoing PCI with stent placement.17 -19 In 1 trial, significantly more bleeding events occurred in the DOAC plus antiplatelet therapy group compared with antiplatelet therapy alone, without a reduction in ischemic events, including stent thrombosis. 17 In a post-hoc analysis, treatment strategies were categorized as DOAC with SAPT or DAPT vs placebo with SAPT or DAPT alone and stratified based on whether patients underwent PCI. No significant difference in in-stent thrombosis was observed between the groups. However, the combination of DOAC with antiplatelet therapy, whether SAPT or DAPT, significantly increased the risk of major or minor bleeding. After PCI, only apixaban with DAPT was associated with an increased risk of major or minor bleeding. 20 Another trial compared different doses of rivaroxaban combined with antiplatelet therapy to DAPT alone. This study also reported higher rates of major and minor bleeding with all rivaroxaban dosages, except for the low-dose regimen, where minor bleeding was not significantly increased. Risk of fatal bleeding was not statistically significantly different. Notably, stent thrombosis occurred significantly less frequently with the low-dose rivaroxaban regimen compared with DAPT alone (hazard ratio [HR] 0.65, 95% CI 0.45-0.94, P = .02). In addition, the low-dose rivaroxaban regimen was associated with reduced mortality from all causes and cardiovascular causes. Therefore, the authors suggest that low-dose rivaroxaban may represent a promising new treatment strategy for patients with acute coronary syndrome. 18 A third, more recent trial compared low-dose rivaroxaban with aspirin, both combined with a P2Y12 receptor inhibitor. No differences were found in bleeding risk or ischemic events, including stent thrombosis. However, the study was not sufficiently powered to assess the ischemic endpoint. 19 The results regarding stent thrombosis are inconsistent across trials. The present findings add to this complexity, suggesting a possible association between DOAC therapy and in-stent stenosis after CAS. The duration of combined antithrombotic therapy may be a critical factor influencing these outcomes. Current guidelines recommend that patients with AF undergoing PCI while on DOAC therapy transition from DAPT (ie, triple therapy) to SAPT within 1 to 4 weeks, depending on the risk of in-stent thrombosis, and continue this regimen for up to 12 months. 21 In our cohort of patients with in-stent stenosis, the majority were managed with a combination of DOAC and SAPT yet still developed in-stent stenosis. Further research is required to explore the potential correlation between DOAC therapy and in-stent stenosis in CAS, as findings from PCI studies are unlikely to be directly extrapolatable to the pathophysiology of carotid stenosis.
According to a systematic review and meta-analysis, the incidence of in-stent stenosis (≥70% or occlusion) following CAS was 10.0% (95% CI 6.0-16.3) over a mean follow-up of 62 months. 3 In our study population, the incidence of severe in-stent stenosis (≥70% or occlusion) was 3.6% (10 of 225) over a mean follow-up of 15 months, while the incidence of moderate and severe in-stent stenosis (≥50% or occlusion) was 9.8% (22 of 225). It is important to note the shorter follow-up period in our study. The same meta-analysis reported that the majority of symptomatic in-stent stenoses, though not statistically significant, occurred in the moderate restenosis group (<70%) compared with the severe restenosis group (2.0% vs 0.8%; OR 0.87, 95% CI 0.24-3.21, P = .83). Therefore, authors state that surveillance DUS after CAS and treatment of asymptomatic restenosis would not benefit the patient. 3 Similarly, in our study population, the majority of symptomatic in-stent stenoses were observed in the moderate restenosis group (33.3%, 4 of 12) compared with the high-grade group (20%, 2 of 10). However, the percentages in our cohort were notably higher than those reported in the literature, possibly due to the smaller sample size of our study. Future studies are needed to investigate the impact of in-stent stenosis, especially in patients using a DOAC, as they seem to have an increased risk of symptomatic in-stent stenosis.
Limitations
One of the major limitations of this study is its retrospective, non-blinded, and single-center design. This methodology is inherently more susceptible to bias compared with a prospective, multi-center and randomized approach. In addition, because baseline characteristics differed between groups and randomization was not possible, confounding (by indication) could have influenced study results. To address this issue, adjusted ORs were calculated to account for potential confounding effects. Adjustment for the clinical condition necessitating anticoagulant therapy (eg, AF) was statistically limited due to its strong correlation with treatment allocation. Therefore, residual confounding by indication must be considered when interpreting the results, as the underlying cardiovascular risk profile associated with such conditions may itself contribute to an increased risk of in-stent stenosis. Another limitation is the small sample size, particularly in the anticoagulant group, which restricts generalizability of the findings and limits the scope for extensive subgroup analysis. Consequently, composite outcomes were analyzed instead of comparisons for individual outcomes to mitigate this limitation. Furthermore, as a tertiary referral center, a significant number of patients were lost to follow-up, primarily because they opted to have their follow-up DUS and/or CTA performed at their local hospital. Another important reason for loss to follow-up was that patients treated in 2024 had not yet reached the 1-year follow-up mark at the time of analysis. Although multiple imputation was employed to mitigate bias due to missing follow-up data, some degree of uncertainty in the estimates remains. The follow-up duration in this study was relatively short, limiting the ability to investigate late in-stent stenosis between treatment groups. Finally, the modality used to assess in-stent stenosis (DUS) has the potential to overestimate the severity of stenosis. However, the same imaging modality and criteria were applied consistently across both patient groups, minimizing potential bias in comparative analyses.
Conclusion
To the best of our knowledge, this is the first study to evaluate the incidence of in-stent stenosis during short-term and mid-term follow-ups after CAS in patients treated with antiplatelet therapy vs anticoagulants. No definitive conclusions can be drawn from this study. The primary analysis suggested a possible association between anticoagulant use and an increased risk of developing in-stent stenosis in the mid-term, despite most patients receiving dual therapy (anticoagulant combined with SAPT); however, this association was attenuated in the sensitivity analysis. Therefore, the findings of this study should be interpreted with caution, also given the limited sample size, potential confounding, and possible bias. Notably, within the anticoagulant group, all cases of in-stent stenosis occurred in patients using a DOAC. While DOACs in cardiology are known to reduce or have no effect on the incidence of in-stent stenosis, our results do not allow firm conclusions in the setting of CAS. These findings highlight the need for further research to explore a potential correlation of DOAC use with carotid in-stent stenosis and to better understand the underlying mechanisms.
Supplemental Material
sj-docx-1-jet-10.1177_15266028261456460 – Supplemental material for In-Stent Stenosis or Occlusion After Carotid Artery Stenting in Patients Treated With Anticoagulants vs Antiplatelet Therapy
Supplemental material, sj-docx-1-jet-10.1177_15266028261456460 for In-Stent Stenosis or Occlusion After Carotid Artery Stenting in Patients Treated With Anticoagulants vs Antiplatelet Therapy by Mert Kök, Reinoud P. H. Bokkers, Aryan Mazuri, Saloua Akoudad, Maarten Uyttenboogaart and Clark J. Zeebregts in Journal of Endovascular Therapy
Footnotes
Ethical Considerations
The Ethics Committee of the University Medical Center Groningen waived the requirement for ethics approval for this retrospective study involving anonymized data.
Consent to Participate
The Ethics Committee of the University Medical Center Groningen also waived the requirement for informed consent because the study was based on retrospectively collected and anonymized data.
Author Contributions
All authors meet the criteria for authorship.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The research data are not publicly available.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.