
Abstract
Introduction:
Syndromic hereditary thoracic aortic disease (sHTAD), including Loeys-Dietz syndrome (LDS), often lead to aneurysmal disease with diffuse arterial involvement. Although open repair remains the gold standard in sHTAD, it carries significant morbidity. Herein, a hybrid approach for subclavian-axillary arterial aneurysm repair in patients with LDS is described.
Technique:
Two patients with prior aortic repair extending from the aortic root to the abdominal aorta were managed for extensive aneurysms involving the subclavian and proximal axillary artery. Via ipsilateral upper limb access, the prior proximal repair was extended with multiple self-expanding covered stents to the axillary artery, ensuring adequate overlap. The distal stent was exposed through a transverse arteriotomy, and an end-to-end anastomosis was created by incorporating the covered stent and arterial walls. In both cases, no salvage of the vertebral arteries was attempted; they were either covered or coiled. Mid-term follow-up showed no anastomotic pseudoaneurysms, kinking, or stenosis. One patient developed a persistent type II endoleak without sac enlargement and remains under surveillance.
Conclusion:
Hybrid repair with endovascular stent implantation, proximal non-native landing zone and open distal anastomosis may offer a safe and effective alternative for complex subclavian-axillary aneurysms in patients with LDS.
Clinical Impact
Syndromic hereditary thoracic aortic disease can result in aneurysms with extensive arterial involvement, and open repair remains the gold standard in these patients. A hybrid technique, involving endovascular extension of a previously replaced proximal landing zone to a distal native arterial segment, followed by open exposure and creation of an end-to-end anastomosis, is described. This approach was successfully applied in 2 cases, both with prior open and endovascular management of the proximal landing zone. Mid-term postoperative outcomes demonstrated acceptable efficacy and confirmed the feasibility of the technique. This hybrid approach may significantly reduce postoperative morbidity compared with conventional open repair.
Keywords
Introduction
Syndromic hereditary thoracic aortic diseases (sHTAD; also reported as genetic aortic syndromes) have been mainly related with the evolution of aneurysms and dissections of the thoracic and thoracoabdominal aorta.1,2 However, in patients with sHTAD, aneurysms in other vascular beds are not uncommon. 3 Among patients with sHTAD, the ones with Marfan and Loeys-Dietz syndromes (LDS) exhibit a higher risk for early-onset aortic pathology and involvement of multiple segments of the arterial tree.1-3 Surgical management in sHTAD is particularly challenging due to vessel wall fragility, complex anatomy, and need for multiple interventions over a patient’s lifetime. 3
Although open surgical repair remains the standard of care for sHTAD patients, the high morbidity associated with multiple extensive open procedures has prompted exploration of less invasive strategies.1-3 Endovascular and hybrid approaches seem to gain ground especially among high-risk patients with sHTAD, with hybrid strategies targeting to secure the landing zones with open repair before the application of endovascular techniques, to minimize the risk of retrograde dissection, rupture, and degeneration over time.4,5 These approaches allow for targeted exclusion of aneurysmal or dissected aortic or other arterial segments while minimizing the physiological burden of open surgery. 4 However, the evidence regarding their safety, efficacy, and long-term outcomes is scarce.
Herein, we describe a hybrid technique combining endovascular stent-graft implantation with open distal anastomosis for managing a subclavian-axillary artery aneurysm in 2 LDS cases.
Surgical Technique
Case 1 Presentation
A 42-year-old man with LDS and previous history of multiple open aortic procedures for type A dissection, including a Bentall procedure with mechanical aortic valve replacement, and a thoracoabdominal aortic replacement (Crawford procedure), was treated for an aortic arch (maximum diameter 57 mm) and right subclavian artery (RSA) aneurysmal degeneration. A 2-staged approach was selected, prioritizing the aortic arch repair via a Frozen Elephant Trunk (FET) repair. Notably, during the FET procedure, the first FET branch was directly anastomosed to the RSA, whereas an 8-mm interposition graft was anastomosed side to end between the proximal third of the first FET branch and the right common carotid artery (RCCA), allowing for an adequate graft length being available as a proximal landing zone for the next stage endovascular repair. The second FET branch was anastomosed to the left common carotid artery (LCCA), and the third branch was used for an extra-anatomic anastomosis to the left subclavian artery (LSA; zone 2 FET).
Regarding the peripheral aneurysm, an asymptomatic aneurysm extending from the proximal third of the RSA to the proximal third of the axillary artery, with a total length of 235 mm and a maximum diameter of 52 mm, set the indication for elective repair (Figure 1A). A hybrid approach was selected, consisting of proximal endovascular bridging to the existing FET branch and a distal open anastomosis incorporating the covered stent and the proximal brachial artery. This strategy was preferred over open repair due to the extensive aneurysm length and the presence of previously replaced proximal landing zones. The time interval between the FET and hybrid repair of the RSA aneurysm was 4 months. The slight increase of the subclavian aneurysm maximum diameter (from 52 mm in the pre-FET computed tomography angiography [CTA] to 55 mm in the post-FET CTA) did not affect the decision-making or operative planning.
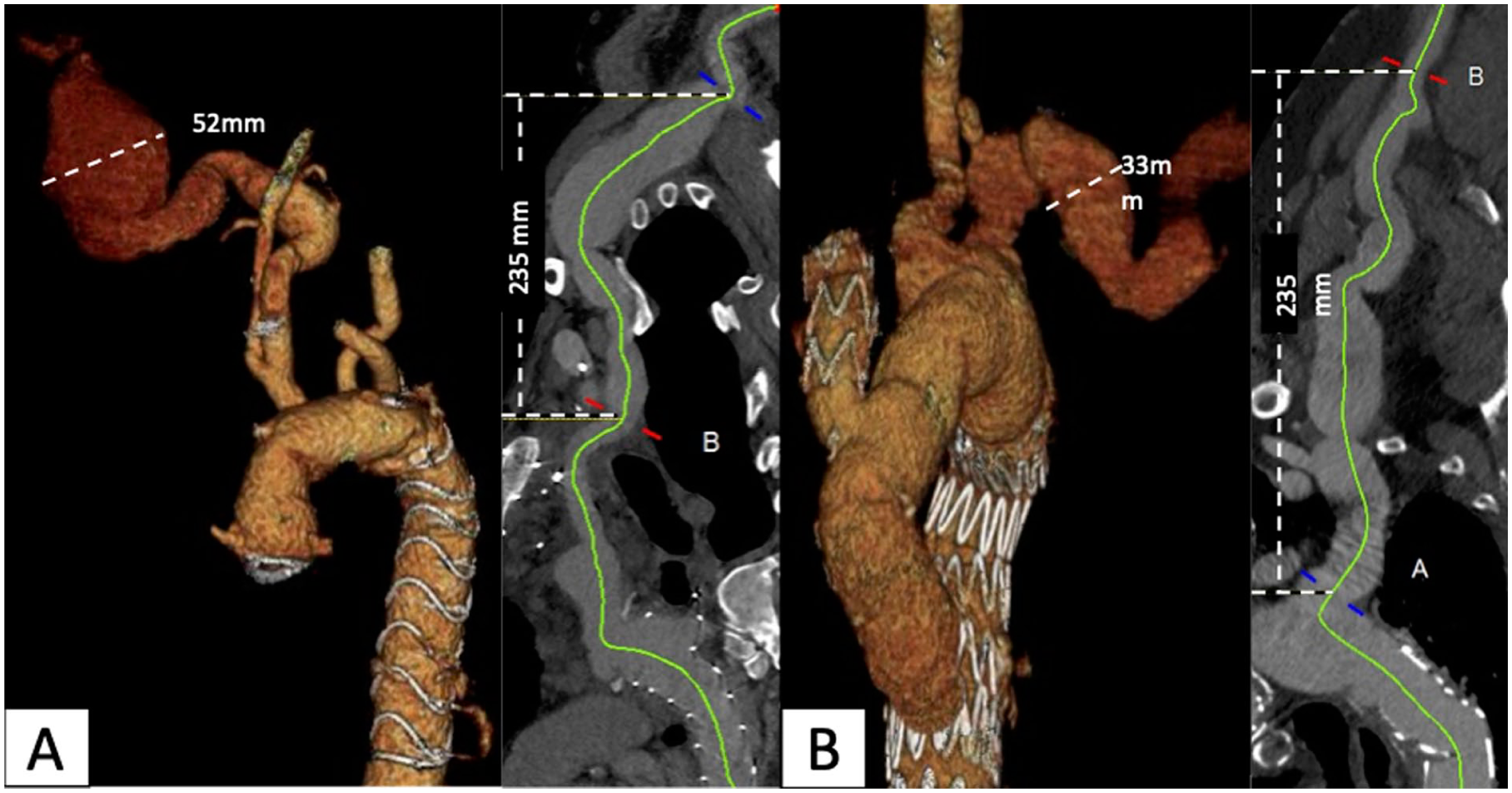
Three-dimensional and curved plane reconstruction based on the preoperative CTA. Panel (A) Case 1 with 52-mm right subclavian aneurysm; panel (B) Case 2 with 33-mm left subclavian aneurysm.
Case 2 Presentation
A 63-year-old woman with LDS and extensive aneurysmal disease, with history of a David procedure, hemiarch replacement up to zone 1 with innominate artery replacement, thoracoabdominal aortic replacement (Crawford procedure), and open abdominal aortic replacement with Y-prothesis, was treated for an aortic arch residual aneurysm (maximum diameter 55 mm) and an extensive (length 255 mm) aneurysm involving the LSA and left axillary artery, with a maximum diameter of 33 mm (the diameter in this arterial segment was consistently >20 mm; Figure 1B). In the past, an RSA aneurysm had been managed after multiple operations including plug occlusion of the RSA with nonselective coiling of the aneurysm, revascularization of the ipsilateral vertebral and axillary arteries via nonanatomical bypasses originating from the RCCA, and, ultimately, endovascular graft implantation in the innominate artery, covering the RSA due to persistent aneurysm perfusion.
An endovascular repair of the aortic arch aneurysm with a hybrid approach for the LSA aneurysm was chosen, due to multiple previous operations and replaced proximal landing zones. After creating a landing zone into the LCCA with an 8-mm Dacron interposition graft, a double antegrade branched endovascular aortic arch repair (bTEVAR; Cook Medical Inc., Brisbane, Australia) involving the LCCA and the LSA was performed, landing proximally distal to the innominate artery. Subsequent TEVAR implantation extending repair down to the level of the previously replaced thoracoabdominal aorta was performed. During this operation, the LSA aneurysm was repaired extending the bridging stents of the bTEVAR into the LSA and left axillary artery using multiple self-expanding covered stents (SECS) and reassuring the distal sealing with an open anastomosis.
Technique
Surgical exposure was achieved through a longitudinal axillary skin incision parallel to the brachial biceps muscle, followed by direct puncture of the respective distal axillary artery (right for case 1 and left for case 2). The subcapsular and circumflex humeral arteries, branches of the distal third of the axillary artery, were exposed and controlled via a vessel loop. Systemic heparinization was administered with a target activated clotting time >250 seconds. A 6F sheath was inserted into the axillary artery, followed by catheterization into the aorta and advancement of a Lunderquist wire (descending thoracic for case 1 and ascending thoracic for case 2 after the bTEVAR and TEVAR extension implantation).
After digital subtraction angiography of the proximal and distal landing zones for the planned endovascular repair, consecutive implantation of multiple SECS was performed with a minimum overlap of 30% of stent’s length, to achieve optimal sealing and decrease the risk of disconnection.
In case 1, the proximal landing zone constituted of the 12-mm Dacron FET branch (Thoraflex Hybrid; Terumo Aortic, Bolton Medical Inc., Sunrise, Florida), which was anastomosed to the proximal RSA. Three consecutive 16 mm × 80 mm Wrapsody SECS (Merit Medical, South Jordan, UT, USA) were implanted, followed by an ETLW-16-13-C-82-E Endurant limb (Medtronic, Minneapolis, Minnesota) to achieve appropriate tapering, and then 2 13 mm × 100 mm Viabahn (W. L. Gore & Associates, Newark, Delaware; Figure 2A).
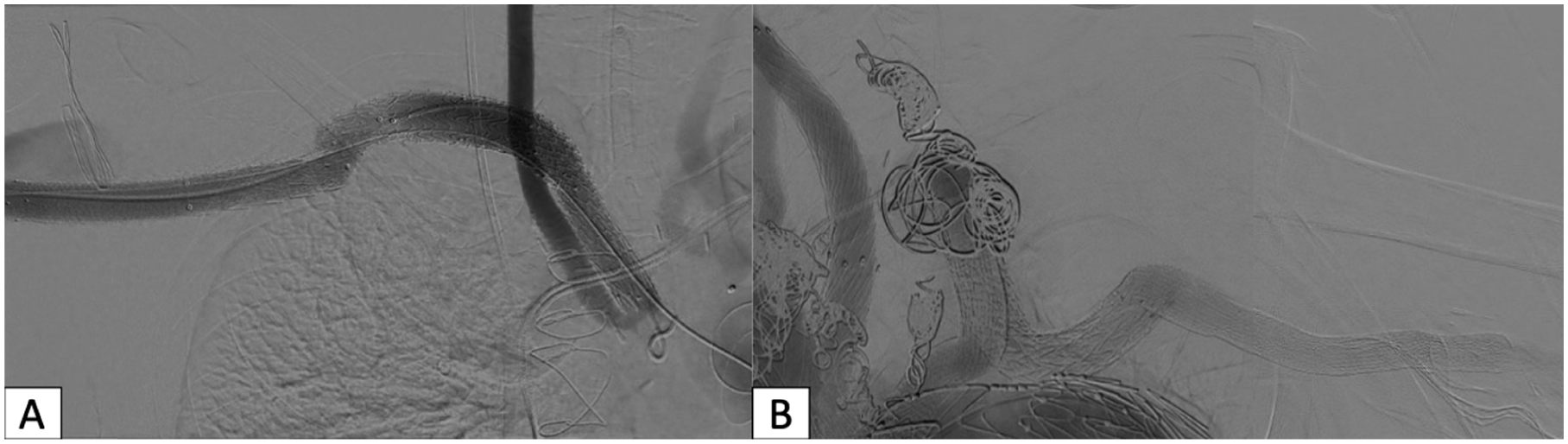
Final intraoperative angiography demonstrating successful aneurysm exclusion following SECS implantation in cases 1 and 2 (panels (A) and (B), respectively).
In case 2, the proximal landing zone consisted of the bTEVAR graft with an antegrade inner branch bridged to the LSA via an 11 mm × 100 mm Viabahn. Coverage extension to the distal landing zone in the axillary artery was achieved with consecutive implantation of 2 13 mm × 100 mm Viabahn, one 14 mm × 80 mm Wrapsody and one 10 mm × 100 mm Viabahn (Figure 2B). The mismatch between the last 2 stents was resolved using a VBX 10 mm × 79 mm as bridge (W. L. Gore & Associates; postdilated proximally to 14 mm).
In both cases, the distally positioned Viabahn was exposed via a transverse arteriotomy at its distal edge, after clamping the proximal and distal flow. The proximal clamp was positioned over a stented arterial segment (15 mm above the arteriotomy). An end-to-end continuous inlay anastomosis was performed using 5-0 Prolene suture and incorporating both the proximal SECS and vessel wall and the distal vessel wall.
In case 1, the right vertebral artery was intentionally covered, after prior imaging revealing a patent dominant left vertebral artery. No pre-emptive or intraoperative embolization was performed, given that no type II endoleak was evident in the completion angiography (Figure 2A). In case 2, a selective angiography at the end of the hybrid repair revealed a type II endoleak which was managed with coil embolization of the left vertebral and internal mammary artery (Figure 2B): via the right common femoral artery, which was used for the bTEVAR (and TEVAR extension) implantation, a catheter was advanced to catheterize the aneurysm sac, forwarded in parallel to the aortic devices to finally achieve catheterization of the subclavian aneurysm sac and type II endoleak-related branches. The final angiography revealed no endoleak or compromise in patency (Figure 2B).
Postoperative Course
Both patients had a short uneventful postoperative hospitalization. No stroke, upper limb ischemia, or bleeding was recorded. Radial arteries remained palpable after the procedure in both cases. The postoperative CTA revealed in case 1 a type II endoleak, originating from the covered vertebral and internal mammary arteries. No imaging features suggestive of a type III endoleak, such as inadequate overlap, component separation, or fabric disruption, were identified. Duplex ultrasound of the vertebral artery was not performed (Figure 3A), and in case 2, a small type Ia endoleak which was decided to be reassessed after 6 months (Figure 3B).
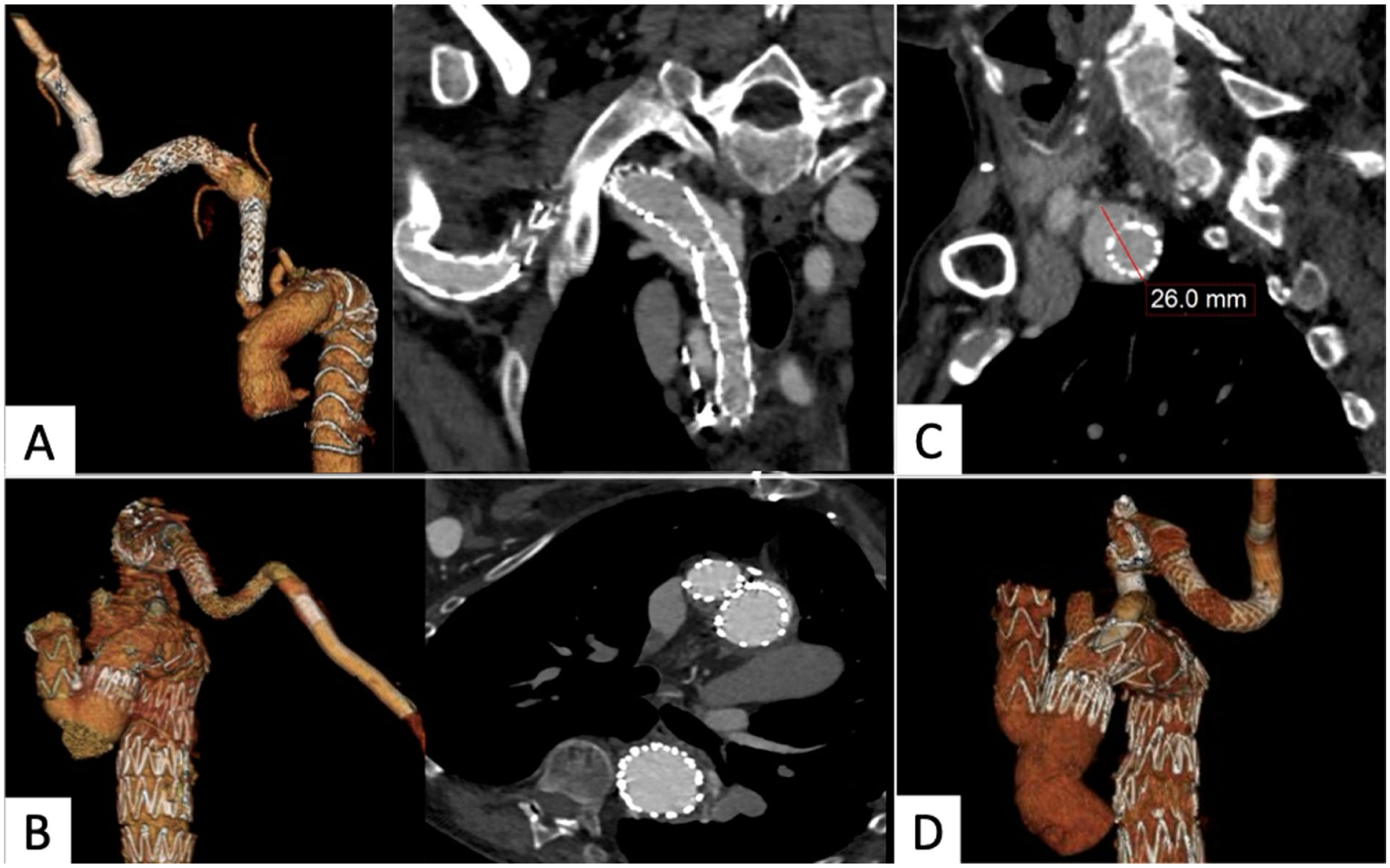
Three-dimensional reconstructions from postoperative CTA demonstrating vessel patency. Panel (A) case 1 with a type 2 endoleak from the vertebral and mammary artery; panel (B) case 2 with a residual type Ia endoleak; panel (C) follow-up CTA showing persistent endoleak but no diameter change; panel (D) follow-up CTA showing spontaneous resolution of the type Ia endoleak and successful aneurysm exclusion.
The mid-term follow-up was 17 months for case 1 and 20 months for case 2. For case 1, the type II endoleak persisted without sac increase compared with the predischarge CTA (Figure 3C), so a conservative management was decided. The postoperative type Ia endoleak of case 2 resolved at the 6-month follow-up CTA (Figure 3D). No anastomotic pseudoaneurysm, graft kink, or stenosis was detected in either patient.
Discussion
Current guidelines recommend individualized management of aortic aneurysms in patients with sHTAD, by setting lower diameter thresholds and growth rates for repair, suggesting open surgery as the standard of care and by intensifying the postoperative surveillance protocols.1,2 Although peripheral arterial involvement is not uncommon in this population, no specific recommendations on the anatomic criteria and diameter thresholds that may lead to an invasive management exist.1,2 Similarly, the available guidelines for the general population do not set a specific threshold for subclavian aneurysm repair, addressing only the case of aberrant subclavian artery, where a threshold for repair is set at 30 mm or even smaller diameters in case of symptoms.1,2 The described hybrid approach enabled a less invasive strategy while adhering to the key principles of aneurysm management in patients with sHTAD, including replacement of the proximal landing zone and securing the distal fixation through a direct anastomosis. 4 Compared with open reconstruction, a hybrid management of the subclavian artery aneurysms was performed using a simpler and less invasive axillary exposure. Furthermore, a controlled distal arteriotomy allows direct visualization and incorporation of both the covered stent and native vessel wall into an end-to-end anastomosis, closely replicating the stability of conventional open surgery and ensuring durable fixation and reliable sealing.
This technique proved applicable in 2 different clinical scenarios and demonstrated adequately durable mid-term results, despite differences in prior aortic arch repair. Both endovascular and open aortic arch repair permitted the use of the technique, as replaced proximal zones were established in both cases. 4 Cautious handling of specific aspects, like oversizing at the level of the covered stent into the Dacron FET branch, contributed to the technical success of the repair.6,7 Deployment of stent grafts into previously placed synthetic open grafts has been previously related to endoleak formation and an aggressive oversizing (30% [4 mm] in this case) may be rational in these cases, as in case 2. However, these endoleaks tend to follow a benign course, as illustrated by the self-limited Ia endoleak after bTEVAR landing into a prior open repair. 7
A relevant technical limitation is the lack of sufficiently long covered stent grafts to treat the entire diseased segment in a single device, particularly in the presence of severe tortuosity. Consequently, extensive overlapping zones are required. Endovascular repair was achieved with the use of multiple long SECS. The continuous and radially oriented expanding force of the SECS compared with the high radial force upon deployment and balloon inflation in balloon expandable covered stents (BECS) minimizes trauma to fragile vessel walls, whereas SECS better accommodate a joint-related motion. 8 Their superior adaptability to peripheral arterial tortuosity and greater available lengths allow extensive coverage with adequate overlap. 9 However, high-grade tortuosity and long coverage have been suggested to affect patency even for SECS. 10 In the current cases, a Lunderquist wire was used as an exchange wire to straighten the subclavian artery tortuosity in both cases. Alternative strategies, such as the use of a softer wire or a through-and-through configuration, were considered but not adopted as they may offer reduced support in highly tortuous anatomy and increase technical complexity, potentially requiring greater force at curvature points to maintain stability.
Extensive overlapping zones between stents were intentionally employed to accommodate both short-term recoil after Lunderquist wire removal and long-term vessel remodelling—either due to sufficient aneurysm exclusion and diameter reduction (leading to consequent lengthening of the vessel) or due to disease progression and subsequent movement of the stents within a progressively widened lumen. This approach parallels the rationale of multicomponent stent systems in complex aortic repair. 11 Large stent diameters minimize the thrombotic risk, whereas low-grade inter-stent oversizing allowed minor movement capacity. BECS usage has been widely avoided in patients with sHTAD, bearing a high risk for dissection and rupture; however, a single BECS was required in case 2 to achieve adequate sealing between 2 SECS. Its deployment was performed into an already covered section and overdilation was avoided. Although distal-to-proximal stent deployment might have facilitated tapering, it may jeopardize the integrity of the reconstruction, as repeated wire and catheter manipulations increase the risk of stent displacement, misalignment, and loss of overlap.
Viabahn covered stents provided a reliable interface for open anastomosis, allowing safe clamping and end-to-end reconstruction involving prosthetic and native segments while maintaining patency. Their flexibility enables the use of vascular clamps, without risk for fracture or residual stenosis while the heparin-bonded ePTFE surface enables smooth integration with both prosthetic and autologous materials and provides a suture-friendly surface that allows direct end-to-end anastomosis. 12 In addition, excess stent length can be safely trimmed due to the braided nitinol structure, allowing adaptation to anastomotic requirements. Previous reports have shown good short-term and long-term patency without increased risk of dehiscence, pseudoaneurysm, or infection rates, respecting that the anastomotic zones are free of calcification and sutures are place through both the graft and vessel wall layers, as in these cases. 13
A significant drawback of the described technique is the extensive coverage of the native artery, resulting to obstruction of antegrade flow into important subclavian side branches, including the vertebral artery. Cerebrovascular adverse events, such as transient ischemic attacks or ischemic strokes, may occur under the circumstance and this technique may be avoided or contraindicated in patients with perfusion compromise of the contralateral vertebral artery or a posterior inferior cerebellar artery-vertebral artery termination. 14 An individualized approach should be used depending on the anatomy of the patient and a reimplantation of the respective vertebral artery could be a viable operative option. However, vertebral artery debranching may lead to stroke while increasing the complexity of the repair due to the vessel wall fragility in patients with sHTAD. 14 Moreover, the need for coil embolization of subclavian side branches should be carefully determined, as coverage of them may lead to persistent type II endoleaks, as in case 1. In this case, the absence of a detectable endoleak in the completion angiography deferred embolization intraoperatively. Although no reintervention was required, due to a stable aneurysm sac, the imminent risk of endoleak type II leading to sac growth and setting an indication for reintervention could have been prevented by embolization of the respective vessels. 15 Importantly, in case 2, need for coil embolization was intentionally evaluated and, ultimately, performed after exclusion of the divisional branches, when flow inversion had already occurred, to minimize the risk of distal embolization. Catheter advancement parallel to the previously implanted endografts was considered safe, as distal sealing occurred within a surgically replaced aortic segment, thereby minimizing the risk of injury during wire and catheter manipulation.
Conclusion
This hybrid technique combining proximal endovascular repair into a replaced proximal landing zone with open distal anastomosis offered a safe and effective solution for complex subclavian-axillary artery aneurysms in patients with LDS. It allowed a prosthetic-to-prosthetic reconstruction while avoiding extensive manipulation of the fragile native vessels. Early results were excellent, though further standardization of the technique and long-term outcomes are needed.
Footnotes
Ethical Considerations
Due to the anonymized data, no Ethics Committee approval was needed according to the current state law.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Tilo Kölbel is a consultant and proctor for and has intellectual property with Cook Medical, receiving royalties, speaking fees, and research, travel, and educational grants. Petroula Nana is a consultant for Getinge receiving research and educational grants. All authors declare no support from any organization for the submitted work; no financial relationships with any organizations that might have an interest in the submitted work; no other relationships or activities that could appear to have influenced the submitted work.