
Abstract
Background:
Multisystem inflammatory syndrome in children (MIS-C) is a severe clinical entity emerging after severe acute respiratory syndrome coronavirus 2 infection, often characterized by cardiovascular involvement. This study aimed to evaluate the frequency and spectrum of cardiovascular involvement in children with MIS-C and to assess its association with clinical severity, biomarker profiles, and recovery outcomes.
Methods:
This study included 54 children diagnosed with MIS-C between June 2020 and December 2023. Clinical features, laboratory parameters, electrocardiographic and echocardiographic findings, treatments, and outcomes were analyzed. Clinical severity was classified as mild, moderate, or severe. Kaplan–Meier and Cox regression analyses were used to evaluate recovery trajectories and identify independent predictors.
Results:
Cardiovascular involvement was detected in 37% of patients. The most common findings were mitral regurgitation (50%), left ventricular dysfunction (20.4%), and pericardial effusion (18.5%). Patients with cardiovascular involvement were older and more likely to present with dyspnea, chest pain, tachycardia, tachypnea, and hypotension (all p < 0.01). They exhibited significantly higher C-reactive protein (CRP), interleukin-6 (IL-6), B-type natriuretic peptide (BNP), urea, and creatinine levels, and lower lymphocyte counts (p < 0.05). Moderate-to-severe cases showed markedly higher rates of left ventricular dysfunction (44%), mitral regurgitation (100%), pericardial effusion (36%), arrhythmias (16%), hypotension (44%), and inotropic requirement (44%) compared with mild cases (all p < 0.01). Recovery was significantly delayed in patients with cardiovascular involvement (median 12.5 vs. 8.0 days; p = 0.008) and in moderate-to-severe cases (14.0 vs. 7.5 days; p < 0.01). In Cox regression analysis, independent predictors of delayed recovery included cardiovascular involvement (HR: 0.48), CRP > 200 mg/L (HR: 0.52), lymphocyte count < 1000/µL (HR: 0.41), BNP > 10,000 ng/L (HR: 0.35), and IL-6 > 100 pg/mL (HR: 0.44).
Conclusion:
Cardiovascular involvement in MIS-C is a strong marker of severe disease, heightened systemic inflammation, and prolonged recovery. Echocardiographic abnormalities, combined with elevations in CRP, IL-6, and BNP provide valuable prognostic information.
Introduction
Multisystem inflammatory syndrome in children (MIS-C) is a rare but potentially life-threatening hyperinflammatory condition that typically develops 3–6 weeks after exposure to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (Feldstein et al., 2020). It is characterized by systemic inflammation leading to multisystem involvement, .most commonly affecting the cardiovascular, gastrointestinal, respiratory, neurological, and mucocutaneous systems (Gottlieb et al., 2021; Patel, 2022).
Among affected organ systems, cardiovascular involvement is particularly frequent and clinically consequential, reported in 34–82% of cases (Wu and Campbell, 2021). Cardiac manifestations range from transient myocardial dysfunction and myocarditis to coronary artery abnormalities, valvular insufficiency, pericardial effusion, arrhythmias, and hemodynamic instability. In severe cases, patients may develop distributive or cardiogenic shock requiring vasoactive support (Wu and Campbell, 2021). Given its prognostic implications, identifying cardiovascular involvement early in the disease course is crucial for risk stratification and management.
Despite increasing recognition of MIS-C, the relationship between cardiovascular involvement, inflammatory and cardiac biomarkers, clinical severity, and recovery trajectories remains incompletely defined. In particular, limited data exist integrating echocardiographic findings, biomarker profiles, and time-to-event outcomes. Therefore, this study aimed to characterize the frequency and pattern of cardiovascular involvement in children with MIS-C and to evaluate its association with clinical severity, laboratory biomarkers, and time to clinical recovery using multivariate and survival analyses.
Methods
This study included children diagnosed with MIS-C according to the Centers for Disease Control and Prevention criteria (Centers for Disease Control and Prevention, 2025), who were treated at the Necmettin Erbakan University Clinic of Pediatrics between June 2020 and December 2023. Patients’ medical records were retrospectively reviewed, and demographic characteristics, comorbidities, presenting symptoms, physical examination findings, laboratory parameters, treatment modalities, and hospitalization outcomes were systematically collected. Clinical features comprised fever duration; mucocutaneous, gastrointestinal, respiratory, and neurological manifestations; and signs of hemodynamic compromise. Hospitalization data included length of hospital stay, pediatric intensive care unit admission, requirement for mechanical ventilation, and clinical outcomes. Laboratory parameters encompassed complete blood count, inflammatory markers (C-reactive protein [CRP], ferritin, interleukin-6 [IL-6]), cardiac biomarkers (high-sensitivity troponin and N-terminal probrain natriuretic peptide), renal and hepatic function tests, and coagulation markers.
Clinical severity was stratified based on hemodynamic support (Vasoactive-Inotropic Score [VIS]), respiratory support intensity, and evidence of organ damage. Patients were categorized into three distinct severity groups: (1) mild cases, characterized by absence of vasoactive medication requirements, minimal or no supplemental oxygen needs, and either no evidence of organ damage or only minimal organ involvement; (2) moderate cases, defined by low-to-moderate hemodynamic support (VIS ≤ 10), significant oxygen support requirements, and/or isolated or mild organ dysfunction affecting single or limited organ systems; and (3) severe cases, distinguished by significant hemodynamic instability requiring intensive vasoactive support (VIS > 10), dependence on noninvasive or invasive mechanical ventilatory assistance, and/or moderate-to-severe organ damage, including ventricular dysfunction (Jonat et al., 2021).
All patients underwent cardiovascular evaluation, including electrocardiography and echocardiography. Cardiovascular involvement was defined as the presence of at least one of the following: heart failure, arterial hypotension, pericardial effusion, myocardial dysfunction, valvular dysfunction, myocarditis, coronary involvement, or cardiac arrhythmia. Myocardial dysfunction was defined as a left ventricular ejection fraction (LVEF) of 55% or lower (LVEF ≤ 55%), consistent with established pediatric cardiac dysfunction thresholds. An LVEF cutoff of ≤55% was used in accordance with commonly accepted pediatric echocardiographic standards (Kantor et al., 2013).
Statistical analysis
Statistical analyses were performed using SPSS version 23.0. Continuous variables were expressed as mean ± standard deviation, and categorical variables were expressed as frequencies and percentages. Group comparisons were conducted using Student’s t-test, one-way analysis of variance, or the chi-square test, as appropriate. Multivariate analysis of variance (MANOVA) was used to assess biomarker clusters associated with cardiovascular involvement and clinical severity. Time-to-event analyses were performed with the Kaplan–Meier estimator for univariate comparisons of survival curves across groups. The Cox proportional hazards regression model subsequently assessed the independent effects of covariates on time-to-event outcomes while adjusting for potential confounding variables. Clinical recovery was defined as sustained afebrile status for ≥48 h, normalization of vital signs, improvement in laboratory abnormalities, and recovery of organ function. A significance level of p < 0.05 was set for all inferential tests.
Results
The study cohort comprised 54 children (46.3% female) who met the diagnostic criteria for MIS-C. At the time of initial clinical presentation, fever was nearly universal, affecting 98.1% (n = 53) of patients, with a mean fever duration of 5.76 ± 2.11 days. Cardiovascular system involvement was documented in 37% (n = 20) of the cohort, while the remaining 63% (n = 34) demonstrated no evidence of cardiac compromise. The most frequently observed cardiac manifestations included mitral regurgitation, identified in 50% of cases (n = 27), followed by left ventricular systolic dysfunction in 20.4% (n = 11), and pericardial effusion in 18.5% (n = 10). Aortic regurgitation represented a less common finding, occurring in only 3.7% (n = 2) of patients.
The cohort’s initial severity assessment revealed the following distribution: 53.7% (n = 29) presented with mild disease, 22.2% (n = 12) with moderate disease, and 24.0% (n = 13) with severe disease. For stronger statistical power and clearer presentation of meaningful differences, patients were subsequently dichotomized into two analytical groups: mild disease (n = 29) and combined moderate-to-severe disease (n = 25).
Analysis of clinical outcomes revealed a more severe disease trajectory among patients with cardiovascular involvement. This subgroup experienced significantly higher incidences of multiple serious complications, including decreased urine output, clinical dehydration, acute kidney injury, heart failure, respiratory failure, pulmonary parenchymal involvement, distributive or cardiogenic shock, and requirement for endotracheal intubation with mechanical ventilation. The heightened disease severity in the cardiovascular involvement group was associated with more aggressive therapeutic interventions. Specifically, these patients required significantly greater utilization of inotropic cardiovascular support, targeted immunomodulatory therapy with anakinra, and therapeutic plasma exchange. Additionally, they received higher cumulative doses of corticosteroids and more frequent administration of low-molecular-weight heparin for thromboprophylaxis. Such intensive treatment requirements corresponded with prolonged health care use; the cardiovascular involvement group experienced significantly longer total hospital stays and extended ward-level care durations compared to patients without cardiac manifestations. Comparative data encompassing clinical and demographic variables for both stratification approaches are presented in Table 1.
Comparison of Patient Demographics, Clinical Symptoms, Treatments, and Hospitalization Metrics by Cardiovascular Involvement and Clinical Severity
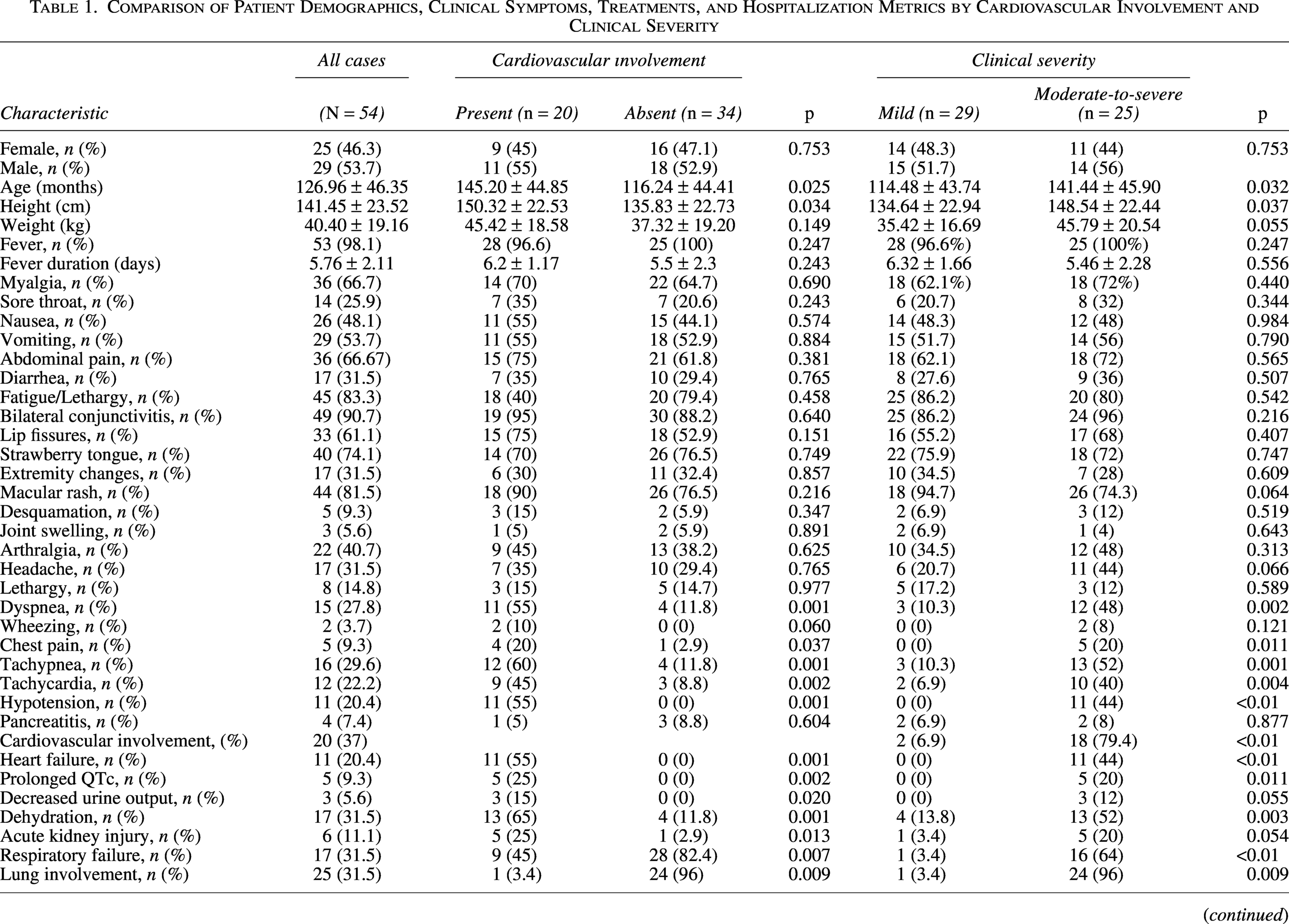
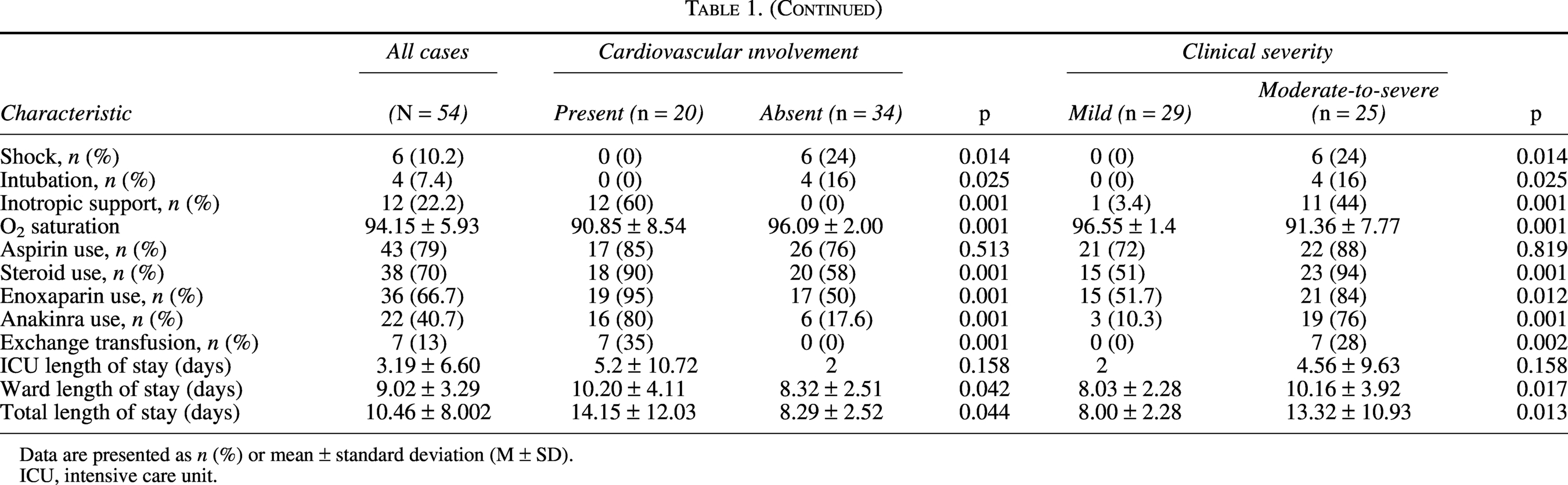
Data are presented as n (%) or mean ± standard deviation (M ± SD).
ICU, intensive care unit.
Laboratory analyses demonstrated distinct biomarker profiles associated with disease severity and cardiovascular involvement. Patients in the moderate-to-severe clinical severity group showed significantly elevated inflammatory markers (CRP and IL-6) and markers of organ dysfunction, including higher serum urea and creatinine levels, reflecting pronounced systemic inflammation. Patients with cardiovascular involvement exhibited significantly increased B-type natriuretic peptide (BNP) concentrations and reduced lymphocyte counts. Detailed laboratory parameters according to cardiovascular involvement and disease severity are presented in Table 2.
Comparison of Laboratory Findings by Cardiovascular Involvement and Clinical Severity
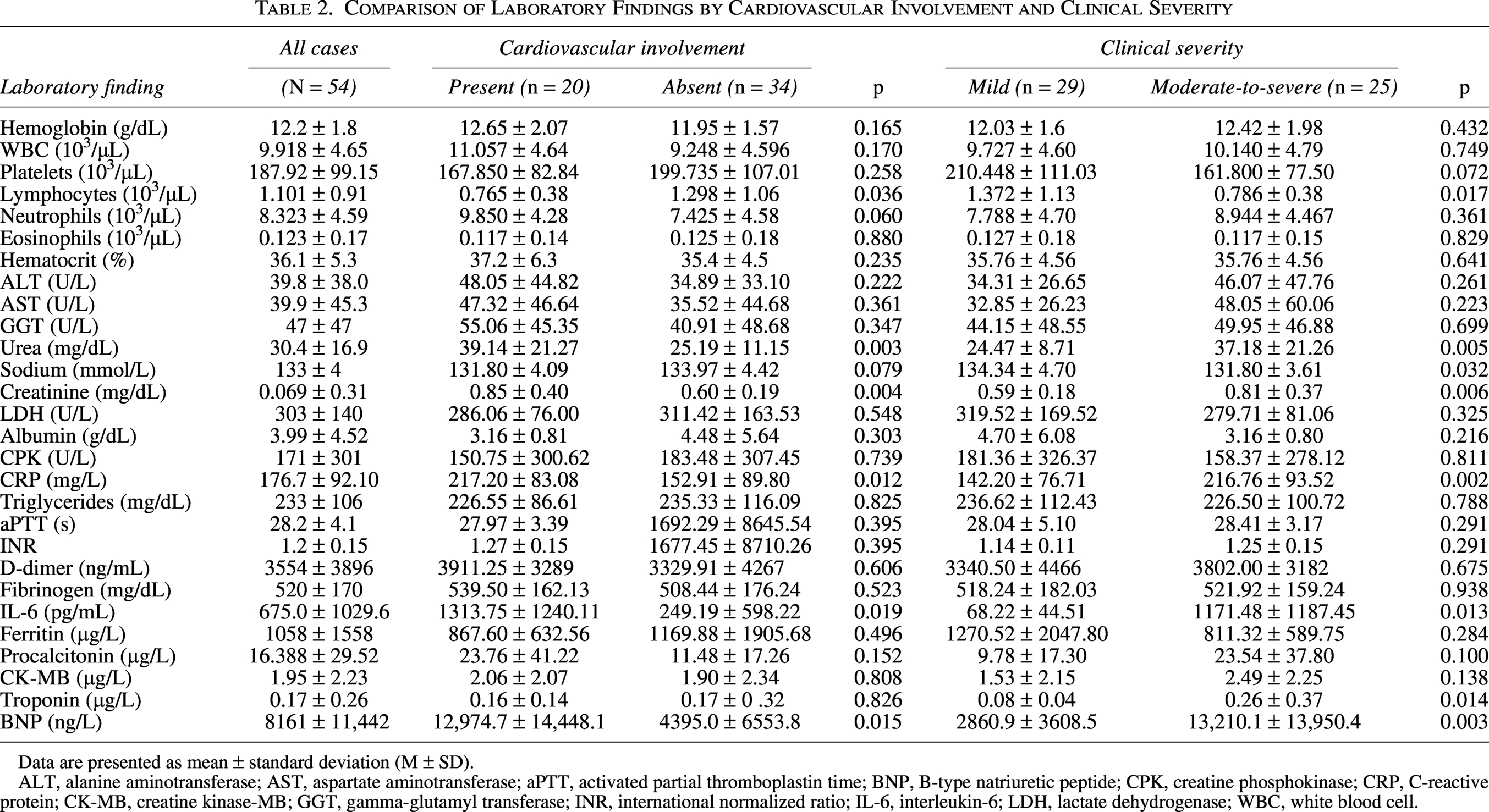
Data are presented as mean ± standard deviation (M ± SD).
ALT, alanine aminotransferase; AST, aspartate aminotransferase; aPTT, activated partial thromboplastin time; BNP, B-type natriuretic peptide; CPK, creatine phosphokinase; CRP, C-reactive protein; CK-MB, creatine kinase-MB; GGT, gamma-glutamyl transferase; INR, international normalized ratio; IL-6, interleukin-6; LDH, lactate dehydrogenase; WBC, white blood cell.
Evaluation of individual cardiac involvement criteria according to clinical severity revealed statistically significant differences for all parameters except coronary artery involvement, with severe cardiac manifestations being disproportionately more prevalent in the moderate-to-severe group. Cardiovascular parameters stratified by clinical severity are detailed in Table 3 and illustrated in Fig. 1.
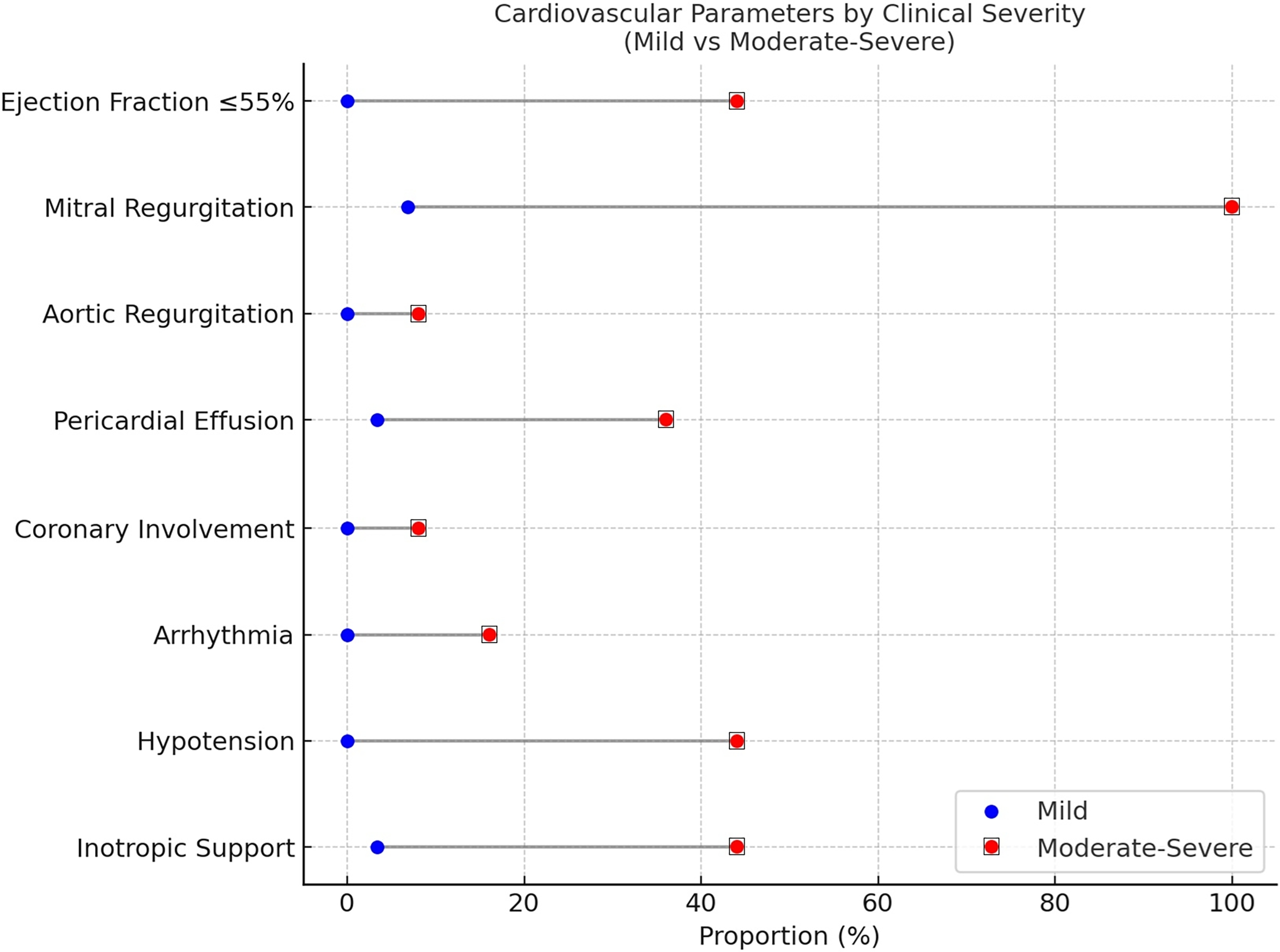
Proportional comparison of cardiovascular parameters by clinical severity group. The figure displays the proportion (%) of patients in the clinical severity groups who presented with each specified cardiovascular parameter.
Comparison of Cardiovascular Parameters by Clinical Severity
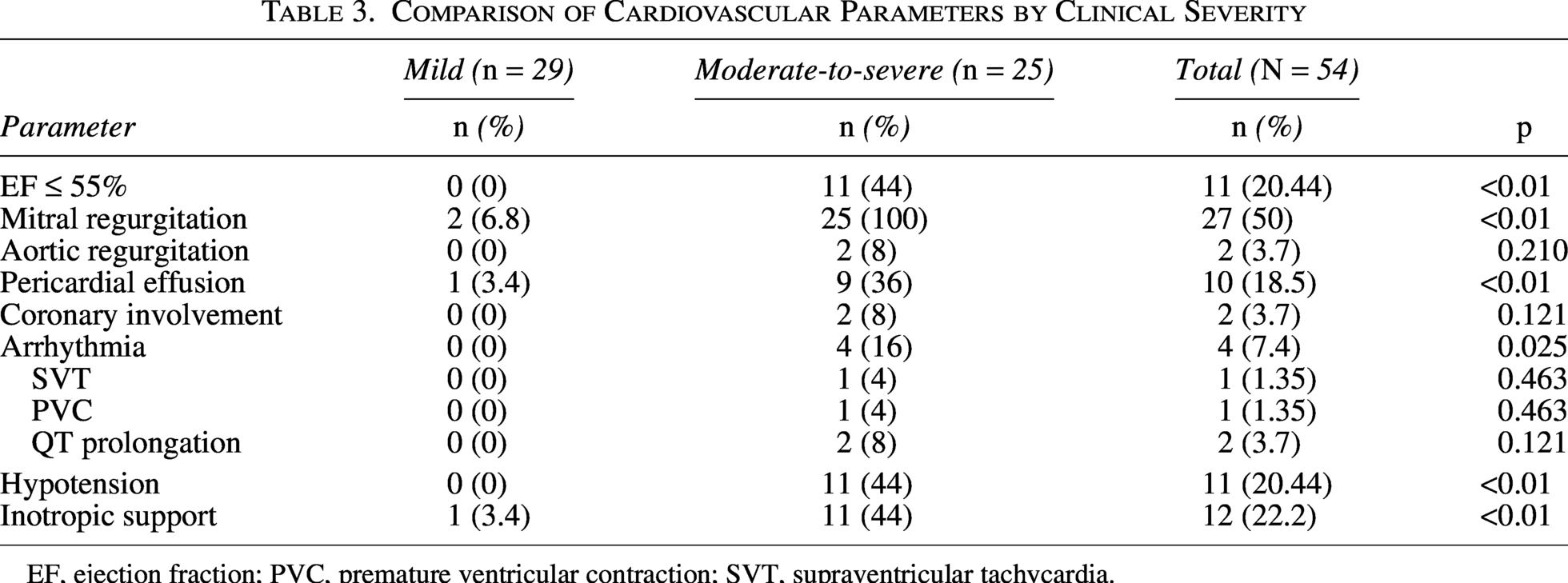
EF, ejection fraction; PVC, premature ventricular contraction; SVT, supraventricular tachycardia.
In the first MANOVA model, multivariate differences between patients with and without cardiovascular involvement were assessed using serum urea, creatinine, CRP, and lymphocyte count as dependent variables. Wilks’ Lambda demonstrated a statistically significant overall multivariate effect (p < 0.05), indicating a significant association between cardiovascular involvement and the combined variance of these biomarkers. A second MANOVA model comparing mild versus moderate-to-severe disease included CRP, IL-6, lymphocyte count, serum urea, sodium, creatinine, and cardiac troponin, again revealing a significant overall multivariate effect by Wilks’ Lambda (p < 0.05).
Kaplan–Meier analysis showed significantly prolonged time to clinical recovery in patients with cardiovascular involvement (median 12.5 days, 95% confidence interval [CI]: 10.2–14.8) compared to those without cardiac manifestations (median 8.0 days, 95% CI: 7.1–8.9; log-rank p = 0.008). Similarly, patients in the moderate-to-severe group exhibited longer recovery times (median 14.0 days, 95% CI: 11.5–16.5) than those with mild disease (median 7.5 days, 95% CI: 6.8–8.2; log-rank p < 0.01).
In Cox proportional hazards regression analysis, cardiovascular involvement emerged as an independent predictor of delayed recovery (HR: 0.48, 95% CI: 0.26–0.89; p = 0.021). Elevated inflammatory and cardiac biomarkers were also independently associated with prolonged recovery, including CRP > 200 mg/L (HR: 0.52, 95% CI: 0.28–0.95; p = 0.034), lymphocyte count < 1000 cells/μL (HR: 0.41, 95% CI: 0.21–0.79; p = 0.008), BNP > 10,000 ng/L (HR: 0.35, 95% CI: 0.16–0.76; p = 0.008), and IL-6 > 100 pg/mL (HR: 0.44, 95% CI: 0.23–0.84; p = 0.013). Full multivariable results are presented in Table 4.
Time-to-Event Analysis and Cox Regression for Risk Factors Delaying Recovery
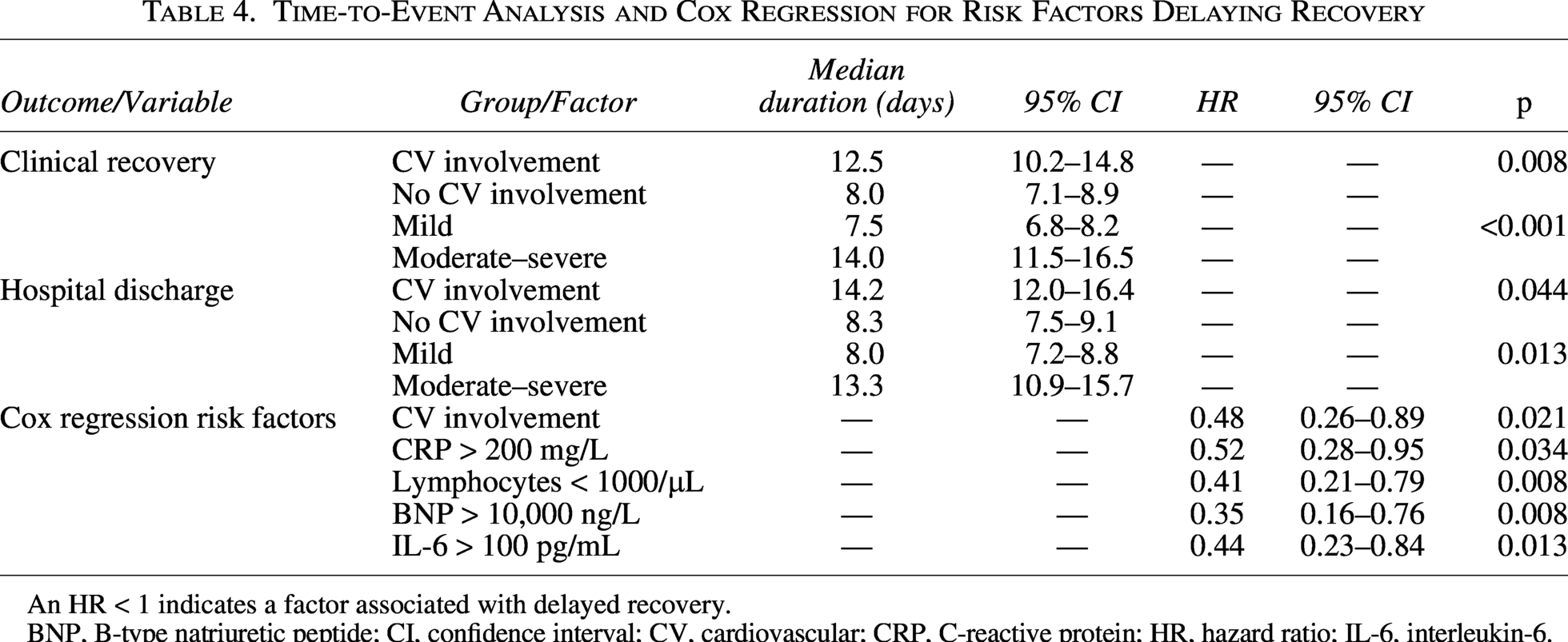
An HR < 1 indicates a factor associated with delayed recovery.
BNP, B-type natriuretic peptide; CI, confidence interval; CV, cardiovascular; CRP, C-reactive protein; HR, hazard ratio; IL-6, interleukin-6.
Discussion
This study demonstrates that cardiovascular involvement is a key determinant of disease severity, biomarker abnormalities, and clinical recovery in MIS-C. In our cohort, 37% of patients exhibited at least one form of cardiac involvement and consistently presented with more severe clinical features and significantly prolonged recovery times, underscoring the central role of cardiovascular dysfunction in MIS-C prognosis.
Previous studies have reported cardiovascular involvement rates ranging from 53% to 80% (Mileva et al., 2023), with myocardial dysfunction and valvular abnormalities being more frequent than coronary artery involvement. While some findings in our cohort were consistent with the literature, overall rates of cardiac involvement were lower, which may reflect earlier diagnosis and treatment as awareness of MIS-C has increased. Similar to prior reports, both cardiovascular involvement and clinical severity increased with age (Campanello et al., 2022; Mannarino et al., 2022).
Consistent with established case definitions, fever and gastrointestinal symptoms were the most common presenting complaints (Baradaran et al., 2020; Bichali et al., 2025). However, patients with cardiovascular involvement more frequently exhibited cardiac-specific symptoms such as dyspnea and chest pain, as well as clinical signs of circulatory compromise, including tachycardia, hypotension, and prolonged capillary refill time (Karagözlü et al., 2024). These findings support the utility of careful hemodynamic assessment for early identification of high-risk patients.
A major strength of this study is the integrated evaluation of laboratory biomarkers associated with cardiac involvement and disease severity. In line with previous reports (Kavurt et al., 2022; Mannarino et al., 2022), patients with cardiovascular involvement demonstrated markedly elevated inflammatory and cardiac biomarkers. Our multivariate analyses showed that elevated CRP, IL-6, BNP, urea, and creatinine levels, as well as lymphopenia, were strongly associated with both cardiovascular involvement and greater clinical severity. These findings indicate that increasing disease severity in MIS-C is reflected not only clinically but also biochemically, highlighting the prognostic value of systemic inflammatory, cardiac, and renal markers.
The mechanisms underlying cardiovascular complications in MIS-C are thought to involve immune-mediated myocardial injury, endothelial dysfunction, and microvascular inflammation (Alsaied et al., 2021). Two recent studies showed that hypotension, shock, and myocardial involvement are much more common in children with severe MIS-C (Belot et al., 2020; Avrusin et al., 2023). In our cohort, nearly all indicators of cardiac involvement—including reduced ejection fraction, hypotension, inotropic support, pericardial effusion, and arrhythmia—were significantly more frequent in patients with moderate-to-severe disease. Our Kaplan–Meier analysis results revealed that cardiovascular involvement is not only associated with increased disease severity in MIS-C but also with a significantly prolonged clinical recovery process. The median recovery time in patients with cardiovascular involvement was ∼56% longer than in those without (12.5 vs. 8.0 days), demonstrating that patients in this group require more intensive supportive care.
Importantly, Cox regression analysis identified BNP > 10,000 ng/L as the strongest independent predictor of delayed recovery, alongside elevated CRP and IL-6 levels and lymphopenia. These findings reinforce the role of cardiac stress and systemic inflammation in determining recovery kinetics and suggest that biomarker-based risk stratification may be useful in clinical practice.
Regarding cardiac outcomes, and in accordance with previous reports, most echocardiographic abnormalities in MIS-C tend to improve during early follow-up after hospital discharge. In our clinical follow-up practice, cardiac function and structural abnormalities generally demonstrated substantial improvement within the first month. However, systematic long-term echocardiographic outcome analysis was beyond the scope of the present study.
The study period encompassed multiple phases of the COVID-19 pandemic each characterized by different dominant SARS-CoV-2 variants. According to national epidemiological surveillance reports in Turkiye, a large proportion of patients in our cohort presented during the Delta-dominant period, while fewer cases occurred during the subsequent Omicron wave. In our descriptive evaluation, the overall pattern of cardiovascular involvement, disease severity, and recovery duration appeared broadly similar across these periods. However, because patient-level viral sequencing data were not available and the sample size was limited, variant-specific statistical analyses could not be performed.
Our findings have important implications for clinical practice and healthcare resource allocation in pediatric MIS-C. Identifying specific biomarker thresholds associated with prolonged recovery may help clinicians anticipate extended hospitalization requirements, particularly in patients presenting with the high-risk constellation of cardiovascular involvement, BNP > 10,000 ng/L, CRP > 200 mg/L, IL-6 > 100 pg/mL, and lymphocyte counts < 1000/μL. The median length of hospitalization exceeding 14 days in patients with cardiovascular involvement highlights the need for proactive intensive care resource planning. For patients identified as high risk for protracted recovery, serial cardiac biomarker monitoring may facilitate early detection of clinical deterioration or inadequate treatment response, potentially enabling timely therapeutic escalation.
Limitations
This study has several limitations. First, it represents a single-center retrospective cohort with a relatively small sample size. Second, SARS-CoV-2 variant identification was not available at the patient level because viral sequencing was not routinely performed. Finally, long-term echocardiographic follow-up outcomes were not systematically analyzed.
Conclusion
MIS-C cases with cardiovascular involvement exhibit a distinctly more severe clinical course, characterized by pronounced laboratory abnormalities, prolonged recovery, and increased need for intensive treatment. Although current diagnostic guidelines define MIS-C broadly, they do not explicitly stratify the extent of cardiovascular involvement or its prognostic significance. Our findings suggest that an integrated assessment incorporating clinical features, key inflammatory biomarkers, and cardiac findings may enhance risk stratification, improve prognostic accuracy, and support more tailored management strategies in MIS-C.
Authors’ Contributions
M.B.O., Ö.M.A., and U.S.: Conceptualization. M.B.O., U.S., and M.G.: Methodology. U.S. and F.S.: Software. M.B.O., T.B., and Ö.M.A.: Validation. M.B.O.: Formal analysis. U.S., M.G., A.S.E., and A.B.P.: Investigation. A.S.E., A.B.P., U.S., A.A., and M.G.: Resources. M.B.O., Ö.M.A., A.A., and U.S.: Data curation. M.B.O., U.S., and M.G.: Writing—original draft preparation. T.B.: Writing—review and editing. Ö.M.A.: Supervision. All authors have read and agreed to the published version of the article.
Ethics Statement
The study was approved by the Necmettin Erbakan University Ethics Committee (Protocol No.: ID26794) for compliance with the provisions of the Helsinki Declaration on the Rights of the Patient. All patients were appropriately anonymized. All patient representatives and patients aged 15 years or older gave consent in their case report form, allowing the use of their medical information anonymously in the research studies.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research received no external funding.