
Abstract
Objectives
: Crisis services are often a first point of contact for individuals needing mental health assessment and intervention. The rapid expansion of virtual care in recent years has enabled remote assessment and introduced novel ways to support crisis stabilization in the community. This scoping review aims to summarize the extent of the literature on virtual crisis assessment and intervention models.
Methods
: PubMed, PsycINFO, CINAHL, and ProQuest databases were searched for English- and French-language literature published between January 1, 2018, and June 30, 2024. Database search results were imported into the online Covidence review management program. A minimum of two reviewers screened titles and abstracts. Target information was extracted from included full texts and summarized thematically across study characteristics and outcomes.
Results
: A total of 5,345 titles were reviewed, with 45 publications included. Publications represented models from around the globe supporting youth and/or adult service users. Data synthesis highlighted the feasibility and potential for virtual care models supporting comprehensive crisis assessment (services that go beyond hotline de-escalation and triage), inpatient admission alternatives, and post-crisis follow-up.
Conclusion
: The available literature suggests that virtual crisis care options are growing, especially during and in the aftermath of the COVID-19 pandemic. Although few rigorous evaluations exist, there is strong evidence of feasibility with emerging and encouraging evidence for effectiveness. Further research focused on outcomes, comparisons of virtual and in-person models, and cost-effectiveness is warranted. Additional research could focus on virtual care models for the geriatric population, which is underrepresented in the available literature.
Introduction
In recent years, catalyzed by the COVID-19 pandemic, virtual care has rapidly expanded and evolved.1,2 During this period of rapid transformation, we experienced an unprecedented international rise in both telephone- and video-based virtual care across all health care settings. 3 The growth of virtual care has the potential to reduce barriers such as geographical distance, stigma, and even costs as it relates to both travel and fees, as virtual alternatives may be feasible with less overhead expense for the provider. 4 The field of mental health was an early leader in the use of virtual care and has continued to demonstrate wide applicability in terms of assessment and follow-up intervention. 5 Video assessment using telehealth based within health centers has accumulated substantial evidence for effectiveness and patient satisfaction in both routine outpatient and acute mental health care settings. 6 Further, empirical support for the ability to assess and manage mental health problems through video while people remain in their homes was gaining prior to the pandemic, with a number of papers summarizing the benefits and challenges of home-based telemental health for psychiatric assessment and the delivery of psychotherapy. 7
Overall demand for mental health care has been increasing, with crisis settings often being the first point of contact for individuals in acute psychological distress, albeit not always resulting in positive experiences. 8 Crisis and post-crisis mental health care is a setting where virtual access to assessment and follow-up care has the potential to reduce barriers to access, enable early intervention as a result of rapid access, and support development of self-management skills in the community. Particularly amid long emergency department (ED) wait times, difficulties and risks with overburdened acute care institutions and ED boarding, 9 and patient preference for person-centered options, 8 effective models that reduce use of, or length of time in, EDs and provide hospital alternatives are greatly needed. Emergency telemental health programs providing assessments for individuals presenting to both rural and urban EDs have effectively increased access to care and resulted in reduced length of stay in the ED and avoided hospitalizations. 10 On the other hand, home-based virtual assessment and intervention in the context of crisis, and even post-crisis, were not well studied prior to the pandemic, and guidance for care delivery in this setting was lacking.11–13
We undertook a scoping review of the literature to describe the current state of evidence regarding the use of crisis-based virtual care. In this review, we define crisis-based virtual care as remote assessment and intervention, in contrast to in-home and outreach models of crisis intervention, which focus on in-person support in the community as a core component of the service. 14 Our definition also goes beyond telephone- or text-based triage and de-escalation, which has long been offered through crisis hotlines. 15 These hotlines often serve as a gateway to other intervention that would typically be offered through an in-person contact with a community-based crisis response team, at an ED or crisis center, or through connection to another organization. 15 In this review, we focus on services providing exclusively or predominantly remote comprehensive crisis assessment and/or post-crisis care, defined as immediately following the crisis contact or within a short timeframe after, with the goals of crisis stabilization and reducing post-crisis negative outcomes.
Methods
This scoping review followed Arksey and O’Malley’s 16 methodological framework and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews checklist. 17 A protocol for the scoping review was registered on Open Science Framework (Registration DOI: https://doi.org/10.17605/OSF.IO/DHCZA) at the time of database searches.
SEARCH STRATEGY
We selected search terms and databases for the review based on the expertise of our team and in consultation with a librarian. Based on commonly used terms and terms found in the literature, search terms were generated for variations of the following concepts: (1) virtual care, (2) mental health, and (3) crisis or emergency. The search terms were tried in different combinations, and the results were compared for volume and relevancy. Given the variability in terminology used on the topic, the final search string was kept broad to ensure maximum inclusion: ((tele* OR video* OR virtual* OR hospital-at-home) AND (psych* OR mental health OR suicide) AND (crisis* OR acute care OR urgent OR emergen* OR hospital*)).
PubMed, PsycINFO, CINAHL, and ProQuest databases were queried using the search string above. Parameters were applied to each database search, including limiting searches by title and abstract, English- and French-language publications, and date range from January 1, 2018, to June 30, 2024. There were no limits on age criteria. Citations from each database were imported into the online Covidence review management software.
ELIGIBILITY CRITERIA AND LITERATURE SELECTION
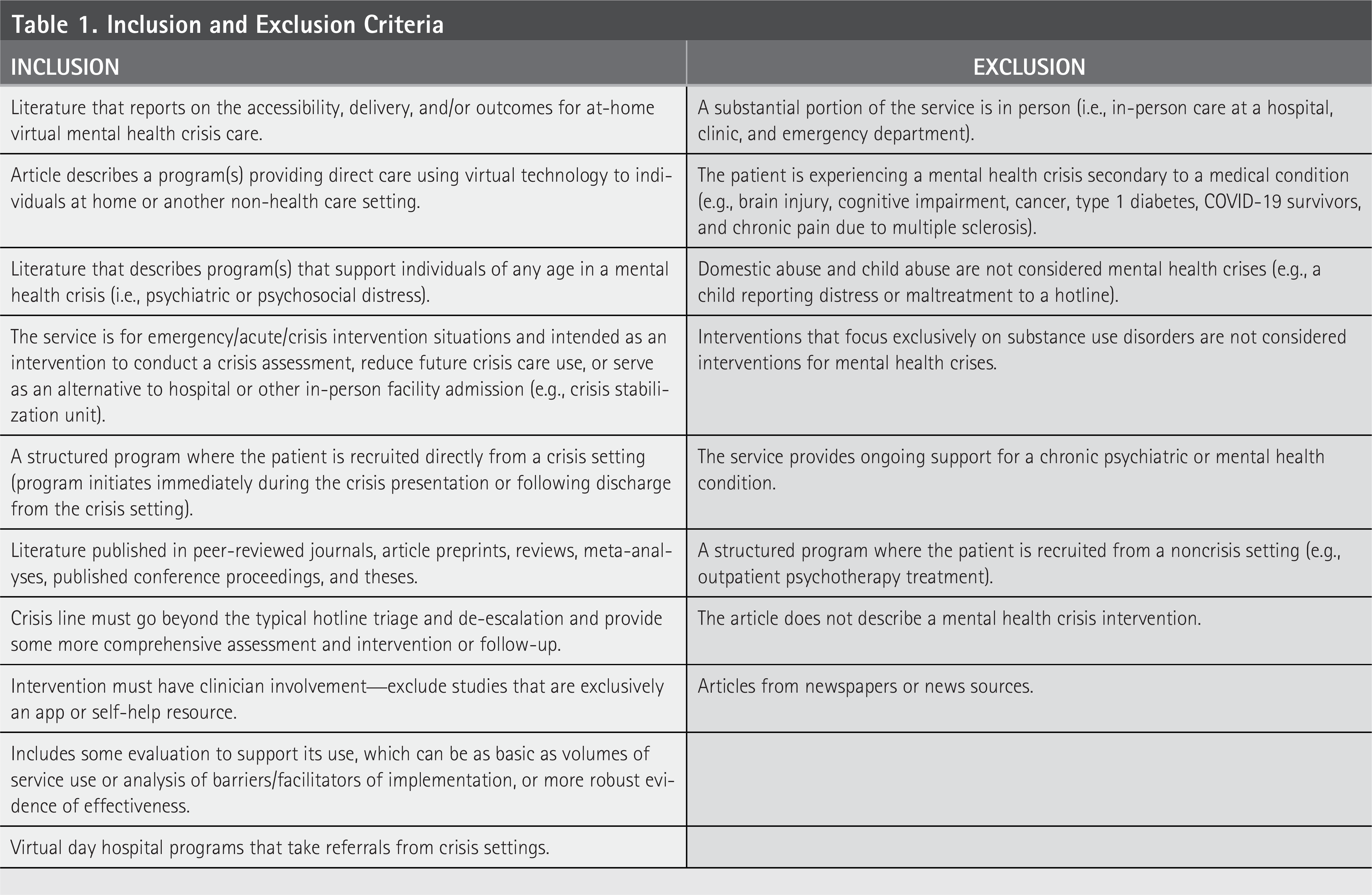
We established a set of eligibility criteria prior to screening citations (see Table 1). The task of screening citations was shared by all three authors. For each citation, at least two authors independently screened each citation by title and abstract. Overall agreement across raters was 96.3%, with interrater reliability between reviewer pairs ranging from a Cohen’s kappa of 1 (perfect agreement) to 0.38 (fair agreement) 18 ; however, articles were reviewed in a nonrandom fashion. Any disagreements were resolved by discussion with the entire study team, and eligibility criteria were revised or added as needed. Studies that potentially met the inclusion criteria were then screened by full text. Any uncertainty about article selection based on full-text review was discussed with the entire study team, while full-text articles that met criteria were included in the review.
Inclusion and Exclusion Criteria
DATA CHARTING
Two authors (S.S. and J.L.) extracted information from the full texts included in the review. The selection of variables for data extraction was based on recommendations from Arksey and O’Malley, 16 information related to the review’s objective, and study team discussion and included: “Authors/Year/Country,” “Objective(s),” “Data type,” “Design,” “Goal,” “Setting,” “Components,” “Frequency,” “Duration,” “Provider group,” “Total sample size,” “Population,” “Comparison,” “Recruited from,” “Relevant results.”
Results
A total of 7,765 references resulted from the database searches, with 5,345 remaining after duplicates were removed. Forty-five publications met the review’s inclusion criteria (see Fig. 1).

PRISMA diagram of study screening and selection process. Reasons for study exclusion: full text could not be obtained (n = 1); article does not describe a crisis intervention (n = 77); the service is not described in sufficient detail (n = 23); the intervention was initiated post-hospital discharge (n = 4); the article is written in a language other than English or French (n = 8); the service is exclusively in person (e.g., a hospital, clinic, emergency department; n = 23); the patient is recruited from a noncrisis setting (e.g., outpatient psychotherapy treatment; n = 4); the intervention does not have clinician involvement (e.g., exclusively an app or self-help resource; n = 5); the mental health crisis is secondary to a medical condition (e.g., brain injury, cognitive impairment, cancer; n = 3); the crisis line does not go beyond the typical hotline triage and de-escalation (no comprehensive assessment and intervention or follow-up; n = 5); the article does not include some evaluation to support the intervention’s use (e.g., volumes of service use, analysis of barriers/facilitators of implementation, or more robust evidence of effectiveness; n = 34). PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Table 2 summarizes the 45 included articles. All articles were written in English, except for three articles that were written in French.20,29,62 The highest number of studies originated from the United States (n = 17)19,27,34,41,42,44,45,47,51–55,57,59,61 with others originating in Canada (n = 6),23,36,38,40,46,48,50 the United Kingdom (n = 4),22,25,49,58 France (n = 3),20,29,62 Australia (n = 2),28,39 the Dominican Republic (n = 2),31,35 and Spain (n = 2).30,56 A single publication originated from each of China, 24 Greece, 30 India, 60 Italy, 26 Mexico, 33 Norway, 37 Turkey, 21 and Qatar. 63 In total, the publications consisted of 22,045 participants (including 18,973 patients/clients23,26,28,29,35,37,43–45,47,49,51,53–58,60,61,63 and 3,170 health care providers, emergency medical service (EMS), and law enforcement21,23,24,27,29,33,35–37,48,59) as well as 507,214 administrative data (calls, contacts, referrals, consultations, encounters, discharges, visits, admissions).19,20,22,24,27,30–32,34,38–41,48,50,52,62 The total number of administrative data were unclear for two publications,25,42 and sample size was not applicable for one publication. 46
Summary of Publications Included in the Review

ALGOS, Algorithm to reduce suicide attempt; BDI-II, Beck Depression Inventory-II; CBT, Cognitive Behavioral Therapy; CI, confidence interval; CRHTT, Crisis Resolution Home Treatment Team; CSU, crisis stabilization unit; CTB, Crisis Toolbox; DBT, Dialectical Behavior Therapy; EBP, evidence-based practices; ED, emergency department; EDVC, Emergency Department Virtual Care; EFU program, Extended Crisis Follow-Up program; EMS, emergency medical service(s); *EMS, Emergency Medical System; EMS-DC, Emergency Medical Services Dispatch Center; GP, general practitioner; HCWs, health care workers; IOP, intensive outpatient; LOS, length of stay; MDD, major depressive disorder; MHNs, mental health nurses; OP, outpatient; OR, odds ratio; PES, Psychiatry Emergency Service; PHP, partial hospitalization program or partial hospital program; PTSD, post-traumatic stress disorder; PSCBT, problem-solving cognitive behavior therapy; RCT, randomized controlled trial; RUD, Risk–Urgency–Danger; SD, standard deviation; SPC, Suicide Prevention Center; SPI, Safety Planning Intervention; TAU, treatment as usual; TBPI, telephone-based psychosocial intervention; TC, telephone contact; TFP, telephone follow-up program; UASD, Autonomous University of Santo Domingo; VCC program, virtual crisis care program; vCSU, virtual crisis stabilization unit; YNHPH, Yale New Haven Psychiatric Hospital.
The methods of data collection for these studies varied including quantitative (n = 28),20,21,24,28,29,31,34,35,38–46,50–57,60,61,63 mixed (n = 15),19,22,23,25–27,30,32,33,36,47–49,58,62 and qualitative (n = 2).37,59 Study designs included program evaluations (n = 18),19,24–27,30,31,33–36,39,41,42,46,48,49,59 retrospective cohort studies (n = 15),22,23,32,38,40,43,44,47,50–55,63 randomized controlled trials (n = 4),57,58,60,62 cross-sectional studies (n = 2),20,29 quality improvement studies (n = 2),21,45 prospective cohort studies (n = 2),28,56 a non-randomized experimental study (n = 1), 61 and a qualitative study (n = 1). 37
TYPES OF VIRTUAL ASSESSMENTS AND INTERVENTIONS
Virtual programs were categorized into three types based on their function and objective(s): those offering crisis assessment and/or intervention (going beyond the standard triage and de-escalation aim of crisis hotlines), those providing a home-based alternative to hospital or other inpatient facility with high-intensity intervention, and those providing post-crisis intervention following discharge after a visit to an ED or other crisis center.
CRISIS ASSESSMENT AND INTERVENTION
A total of 22 publications19–39,63 describe comprehensive virtual assessments of mental health needs and/or intervention that includes extensive therapeutic interaction. Evaluations focused on at least one of the following areas: feasibility/acceptability (n = 14),19,21–29,33–36 user characteristics (n = 8),19,20,23,30,32,38,39,63 outcomes (n = 6),19,21,28,31,34,38 cost-effectiveness/savings (n = 1), 28 and social interaction experiences between providers and patients (n = 1). 37 Of the studies that focused on outcomes, these included service use outcomes,28,34,38 call characteristics, 19 program satisfaction, 21 and mental health services access. 31 Most crisis assessment services were for adults only (n = 8),22,24,26,28,29,32,33,38 six services were for all ages (both youth and adults),21,31,39,61,63 and four services were for youth only.20,23,34,36 Five services described did not explicitly specify the age range of the recipient population.19,25,27,30,35 Target populations ranged from youth and adults experiencing acute distress, mental health complaints, psychosocial issues, or suicidal crises19,24,26,28–32,35,37–39,63 to individuals with diagnoses of moderate to severe mental health problems. 22 Two other services targeted health care workers experiencing mental health crises.21,33 Similarly, the youth assessment services targeted minors experiencing mental health crises23,36 as well as children with various psychological disorders. 20 Special populations targeted included individuals experiencing mental health crises who are in contact with the police 27 and high school students at risk of suicide. 34
Patients of the virtual crisis assessment services were mostly recruited from the community (i.e., the general public; n = 13) with no referral necessary.19,24,25,28–32,35,36,39,63 The remainder of virtual crisis assessment services received referrals from a variety of sources (n = 8).20–22,26,27,33,34,37 More specifically, patients of the virtual crisis care (VCC) program in rural South Dakota, USA, were recruited by law enforcement from the community or from prisons as the service is initiated by law enforcement. 27 Three more virtual crisis assessment services recruited patients from mixed settings (i.e., inpatient and outpatient).22,26,37 Patients (as well as caregivers, i.e., parents) for the virtual crisis consultation service at the child and adolescent psychiatry department of the Reims University Hospital 20 were recruited from referrals from health care professionals (doctors, psychologists, nurses). The Hospital–School–Community Telepartnership (HSCT) program recruited students from participating school districts. 34 The mobile app called Ruh Sagligi Destek Sistemi-Mental Health Support System for telepsychiatry service recruited health care workers registered with the Ministry of Health (and their children) in Turkey, 21 while a crisis helpline in Mexico recruited frontline health care workers who work with patients infected by COVID-19. 33
Of the 22 publications describing virtual assessment services, 17 used the telephone as a way of communicating with patients,19,20,22,24–26,28–33,35,37–39,63 9 described using video,21,24,27,28,31,35–38 and 4 described using text/email.21,31,35,39 Two services reported in-person clinic visits as part of the program in addition to the virtual contact.24,31 The duration of virtual assessments varied between services. Most studies did not specify the duration of assessment services.19–23,25,26,28–32,35,63 The duration of the remainder of assessment services was usually about 30 min24,28,36,37 or between 60 and 90 min.33,34,38 For the most part, frequency of clinical contact was not specified for the assessment and intervention services (n = 14).19,21,24–31,35,37,63 The frequency of clinical contact for the remaining assessment services varied between 1 and 12 contacts/sessions per caller, patient, or student.20,22,23,33,34,36,38
The virtual assessment services are situated in a variety of settings. Six services are crisis helplines organized by university students and professors, a suicide prevention crisis center, and a collaboration between private and public care (the Kids Helpline did not specify where the clinical team is based; n = 6)26,30,33,35,39,63; four services are involved with EMS (i.e., call center, dispatch center, and helpline)28,29,32 or ambulance services (i.e., clinical support desk) 25 ; two are teleconsultation services in a university hospital’s child psychiatry department 20 and a collaboration between the Dominican Republic government and regulatory bodies for psychology and psychiatry 31 ; two are EDs23,36; and one of each: a call-in center at a COVID-19 testing location at a medical center, 19 a mobile app with telehealth service, 21 a psychology department within a community mental health team, 22 a mental health center, 24 a hub team staffed by clinicians from Avera eCARE, 27 a decentralized on-call system established in regional psychiatry centers, 37 and a crisis clinic facility. 38 The HSCT program did not specify the setting where the intervention team is situated. 34
Most virtual assessment services were staffed with multidisciplinary teams. The majority of publications described services staffed with psychology (i.e., psychologists, trainees, students, psychotherapists, licensed counselors or social workers, crisis workers, child development professionals, OTs; n = 15),19,21,22,24,26,30–36,38,39,63 followed by psychiatry (psychiatrists, residents, child and adolescent psychiatrists; n = 11),19–21,24,30,31,33–35,37,38 nursing (i.e., nurses, psychiatric nurses, mental health nurses; n = 6),24,28,36–38,63 and physicians (i.e., ED physicians, emergency physicians, anesthesiologists, general practitioners [GPs]; n = 3).23,29,36
At the Yvelines Emergency Medical Services Dispatch Center (EMS-DC), in particular, anesthesiologists (and other physicians working there) are expected to have suicide risk assessment training based on the Risk–Urgency–Danger (RUD) approach. The RUD approach sets national guidelines and standards for suicide risk assessment and is adopted by EMS telephone dispatch centers in France. 29 Some publications used generic terms without specifying the exact type of practitioner (i.e., behavioral health practitioners, mental health professionals, secondary triage practitioners, health sciences professors, health department professors; n = 4).25,27,28,35 The goal of most virtual assessment services is to resolve crises19,20,22–24,26–35,37,39,63 (plus provide referral support31,34 and reduce mental health morbidity and mortality during the COVID-19 pandemic 35 ), followed by diverting ED visits20,25,28,38 and diverting hospitalization.20,27,28 The goal of the pediatric ED Virtual Care service at the Children’s Hospital of Eastern Ontario (CHEO) is to maintain access to care during the COVID-19 pandemic. 36
Outcomes studied generally fell into four categories: user characteristics (n = 14),19,20,23,24,28,30–35,38,39,63 service usage (n = 10),22–26,32,34,35,38,39 service outcomes (n = 9),19,22,25–28,34,38,63 and service evaluation (satisfaction, feedback, scores, feasibility/acceptability, benefits and/or challenges; n = 13).21–29,33,35–37 Results of publications reporting on user characteristics focused on patient demographics and main complaints/reasons for presentation. The majority of virtual crisis service users were women (n = 9)19,24,28,31–35,39 and reported accessing virtual services for reasons involving anxiety (n = 6),19,28,31,32,35,63 depression/low mood (n = 4),28,32,35,63 suicidal thoughts and behaviors (n = 3),31,35,63 sleep problems (n = 3),19,31,63 and interpersonal conflict (including conflict with family; n = 4).20,32,35,39 Four publications reported that users were accessing virtual services for complaints and symptoms attributed to the COVID-19 pandemic (n = 4).19,30,32,35 Three publications compared the demographics of virtual and in-person users accessing the same crisis services.23,28,38 Youth accessing the CHEO ED virtually tended to present for reasons related to anxiety rather than depression and suicidal/self-harm thoughts and behaviors, and tended to be younger in age. 23
Similarly, adults accessing an EMS call center in Australia managed by mental health nurses via video telehealth tended to be younger and female compared with those adults who access the service by voice-only triage. 28 Adults accessing the virtual assessments from the Crisis Response Center compared with those attending in person were more likely to be older and live farther away from the Center, and were less likely to be male, engage in suicidal behavior, abuse substances, or experience psychosis. 38 Results of publications reporting on service usage typically focused on quantifying the number of sessions/visits attended by patients (n = 5),22,26,32,34,38 whether medication was prescribed to patients(n = 2),24,34 and what patients’ preferences were for communicating with clinicians virtually (n = 2).35,53 In regard to communication preferences, teen users of the Kids Helpline (KHL) liked communicating with providers by webchat and email more than phone calls. 39 Similarly, adult users of the Autonomous University of Santo Domingo (UASD) COVID-19 Psychological Helpline preferred messaging on WhatsApp rather than taking phone calls. 35 Results of publications reporting on service outcomes typically focused on the end result of crisis calls, visits, or sessions,22,26,38 especially referrals (to hospitalization, mental health care, community providers such as therapists and psychiatrists; n = 3)19,25,34 and pharmacological intervention or medication management.34,63
Finally, results of publications reporting on service evaluation typically focused on user and provider satisfaction (or similar). Satisfaction ratings were generally high among both users and providers,21–24,26,28,33,35,36 and two of these studies concluded that the services were feasible and acceptable (i.e., crisis support call service organized by a Community Mental Health Team, helpline organized by the National Institute of Psychiatry and the National Autonomous University of Mexico).22,33 Some studies collected qualitative feedback from users and providers, which revealed the benefits and challenges of virtual crisis assessments.25,27,36,37 Benefits included efficient access to crisis support, improved documentation, mitigation of involuntary committal procedures, enhanced transparency for clinical assessments and decisions, and effective clinical gaze (provider–patient interactions during therapeutic encounters, i.e., emergency psychiatric consultations).27,37 Challenges included high staff turnover, lack of in-person triage options, technical issues, network availability issues, and barriers to the acceptability of VCC (i.e., time constraints, insufficient staff support, and competence levels of clinicians).25,27,36
HOME-BASED ALTERNATIVE TO INPATIENT CARE
A total of 16 publications40–55 describe crisis interventions that are home-based alternatives to hospital or similar facility-based admissions and provide high-intensity care. These virtual interventions include partial hospital(ization) programs (PHPs; n = 6),44,47,52–55 a crisis stabilization unit (n = 4),40,46,48,50 intensive outpatient programs41–43,45,51 (IOPs; n = 5 including a day program called the Adult Transitions Program [ATP] 51 ), and a crisis resolution home treatment team (CRHTT; n = 1; the Crisis Toolbox [CTB] 49 ).
Thirteen studies evaluated intervention outcomes.40–43,45,47,49–55 The following outcomes were investigated: depression (n = 7),44,45,47,51,53–55 patient satisfaction (n = 6),47,49,52–55 visits/attendance (n = 3),42,43,52 suicidality/self-harm (n = 2),45,51 anxiety (n = 2),47,51 safety (n = 2),53,54 effectiveness (n = 1),53,54 hospitalization (n = 1), 52 patient progress (n = 1), 52 post-discharge acute care use (n = 1), 40 and patient-infant bonding (n = 1). 44 Of the 13 studies, 7 also focused on feasibility/acceptability,42–44,50–52,54 3 on user characteristics,40,45,50 and 1 on cost-effectiveness/savings. 40 Three other studies aimed to describe the implementation (i.e., feasibility/acceptability) of virtual crisis services (i.e., Yale New Haven Psychiatric Hospital’s telehealth group-based IOP and OP services, and vCSU).41,46,48 Of these, one also focused on user characteristics. 48
The majority of virtual crisis interventions were for adult patients (n = 11).40,41,46–50,52–55 A minority of interventions were for both youth and adult patients (n = 4).42,43,45,51 One intervention did not explicitly specify the age of users. 44 Patients of the virtual crisis interventions were mostly recruited from mixed settings (i.e., inpatient/outpatient),43–45,47,50–55 followed by EDs/crisis clinics40,46,48,49 and outpatient settings.41,42 The interventions’ target populations were individuals experiencing mental health crises40,43,48,49 and who are at risk of hospitalization,50,51 or any patient requiring acute, intensive psychiatric treatment in a PHP setting. 53 Target populations were patients with a wide range of mental disorders (i.e., mood disorders, anxiety disorders, psychotic disorders)41,52 with high acuity42,45,46 and/or comorbid conditions.45,47 Some virtual interventions targeted specific populations including borderline personality disorder, 54 major depressive disorder, 55 and women with perinatal mood and anxiety disorders. 44
Of the 16 publications describing components of the virtual crisis interventions, 14 included individual therapy40,43–49,51,53–55 and 12 included group therapy.41–48,51,53–55 Of the 12 publications including group therapy, 2 described a virtual outpatient intervention that is exclusively group-based and conducted over telehealth (i.e., telephone, virtual televideo, MyChart messaging/video).41,42 Most virtual crisis intervention programs offered connection via video (n = 12),40,43,45–48,50–55 followed by telephone (n = 7),40,43,46,48–50,52 and/or text (n = 4).40,46,50,52 One intervention (i.e., The Motherhood Center PHP) describes providing group and individual therapy over telehealth but does not specify if this is video- or phone-based contact. 42 Frequency of treatment/clinical contact (i.e., check-ins, individual therapy sessions, and group therapy sessions) varied between virtual crisis interventions. Contact frequency ranged from several times per week (n = 3)43,45,51 to daily (n = 9).40,42,47,48,50,52–55 For two interventions,44,46 the contact frequency was not specified. Duration of treatment also varied between virtual crisis interventions. Treatment duration ranged from 3 days 40 up to 6 weeks.43,52 For four interventions, the treatment duration was not specified.42,44,47,49
The virtual intervention teams are situated in a variety of settings. These include a 24/7 walk-in crisis center with crisis stabilization unit,40,46,48,50 IOPs at hospitals,41–43 a company (i.e., Charlie Health, Inc.), 45 and a day program at an academic medical center, 51 PHPs in hospitals,47,52–55 a health care center (i.e., Motherhood Center of New York), 44 and a Crisis Resolution Home Treatment Team (CRHTT) with no specified setting/location. 49 The goal of most virtual crisis interventions is to divert hospitalizations (n = 13),40,43,45–55 resolve crises (n = 9),40–44,46,48–50 divert ED visits (n = 5),43,45,46,51,52 and/or avoid repeat ED visits (n = 4).43,45,46,51 Most virtual crisis interventions were staffed with multidisciplinary teams.
The majority of publications described virtual programs staffed with psychologists, psychotherapy clinicians, clinical therapists, clinical counselors, mental health clinicians, or psychology students or fellows (n = 11),40,41,44,46,47,49–51,53–55 psychiatrists (or psychiatric trainees; n = 10),40,41,44,46–48,50,51,54,55 nurses or nurse practitioners (n = 4),46,48,50,51 social workers (n = 3),48,54,55 physician assistants (n = 3),40,46,51 and an occupational therapist. 51 In some cases, publications used generic terms to describe clinical staff, crisis workers, or clinicians on multidisciplinary teams of virtual crisis interventions.42,45,50,52
Studies generally reported results related to program acceptability/feasibility (including patient and provider satisfaction; n = 10),46–55 symptom improvement (n = 8),44,45,47,51–55 patient attendance (n = 7),42,43,45,52–55 and patient characteristics (n = 3).40,48,50 In terms of acceptability/feasibility, the vCSU had high levels of acceptability from providers 48 and was deemed feasible for a variety of mental health crisis patients. 50 Additionally, the vCSU received positive feedback from service users, families, and providers. 46 vCSU providers thought the model worked well for more than half of the patients referred and identified several benefits for users (i.e., stabilization support, stay at home, more care options, better outcomes are possible). 48
Providers also identified challenges related to the vCSU model, which included staff and resource limitations, procedural issues, program limitations compared with routine care, and possible lack of program suitability for some patient demographics. 48 Similarly, the Rhode Island Hospital Adult Partial Hospitalization Program (RIH PHP) received positive feedback. Both virtual and in-person users of the PHP reported being highly satisfied with the service.53–55 Virtual users of the CTB program also reported high levels of satisfaction with the service, 49 and virtual users of the Zucker Hillside Hospital PHP were as satisfied as in-person users with the service. 52 Like the Zucker Hillside Hospital PHP, virtual users of the Behavioral Health Partial Hospital Program (BHP) also had equally positive perceptions about the service compared with in-person users. 47 Both user groups felt they were informed and treated respectfully and would recommend the program to others. 47 Like the vCSU providers, virtual users of the BHP also identified advantages and challenges related to the service. 15
One advantage is increased access to treatment, and challenges include difficulty connecting with other patients in the program, technology issues, and difficulty establishing a therapeutic environment at home. 47 In terms of symptom improvement, studies generally reported significant decreases in depressive symptoms, anxiety, suicidality, and self-harm.45,51 When compared with in-person services, virtual services showed significant decreases in depressive symptoms, anxiety, suicidality, and overall mental health (i.e., coping, well-being, and functioning) that were equal or greater.44,47,52–55 In terms of attendance, studies generally reported increased appointment or session attendance42,43,52 and fewer days missed 54 for virtual service compared with in-person service. As well, studies reported increased treatment completion rates 55 and lower hospitalization rates 52 for virtual programs compared with in-person programs.
The RIH PHP reported on length of stay (LOS) and noted a higher average LOS for virtual patients compared with in-person patients.53–55 The vCSU 50 also reported on LOS (4.9 days, range of 1–10) but did not compare it with the in-patient CSU. Other studies simply reported on completion rates of virtual programs. One virtual IOP reported a mean completion rate of 85.9% (standard deviation [SD] = 16.48), 45 and one virtual day program (ATP) reported that 92% of virtual patients 51 completed the program.
Lastly, studies reported on the characteristics of patients who use virtual crisis interventions.40,48,50 Studies of the vCSU, in particular, reported on patient demographics at admission 40 and patient symptoms at assessment. 50 Both studies reported the presence of depression, anxiety, suicidal/self-harm behavior, and psychosis/mania.40,50 Psychosis/mania, in particular, was noted to be a significant predictor of transfer to hospital. 40 Furthermore, the feedback of vCSU crisis clinicians led to the development of four patient profiles who are a good fit for the vCSU model 48 ,p.7: (1) “barriers to care and ‘predictable’ mental health needs,” (2) “system-aware and avoidant,” (3) “high needs, system-naïve,” and (4) “acute and transient crisis.”
POST-CRISIS INTERVENTION
A total of seven publications56–62 describe virtual follow-up programs offered following an ED or other crisis visit that are less intensive than in-patient alternatives. The post-discharge programs include the telephone follow-up (TFP) program, 56 the telephone-based psychosocial intervention (TBPI), 60 the virtual patient navigation program, 57 problem-solving cognitive behavior therapy (PSCBT), 58 the extended crisis follow-up (EFU) program, 59 the Safety Planning Intervention (SPI), 61 and VigilanS. 62 Each study56–62 aimed to evaluate the virtual follow-up care intervention. For most studies, the focus of evaluation was on outcomes,56,57,60–62 which included suicidal behaviors, self-harm, suicide attempts and reattempts, completed suicides, ED to hospital admission conversions, acute care utilization, and outpatient mental health visits. The focus of evaluation for the EFU 59 and TBPI 60 programs was acceptability/feasibility only, while the focus of evaluation for PSCBT 58 was both feasibility and outcomes (i.e., depression, personal health, hopelessness, anxiety, suicidality, work and social adjustment, and health utility).
The study populations for virtual follow-up interventions consisted of adult patients or providers in four studies,56,57,60,61 while the PSCBT intervention 58 consisted of both youth and adult (i.e., ages 16–30) patients. Two studies59,62 did not explicitly specify the age of patient populations. Most of the patient populations were recruited from EDs,56,57,59–62 while the patient population for PSCBT 58 came from mixed settings including child and adolescent mental health services in EDs and hospital wards, community mental health services, and a local nonprofit organization. The target populations for the interventions were typically individuals who had presented to the ED for suicide attempts or self-harm and were discharged with high ongoing risk for suicide.56,58–62 The target population for the virtual patient navigation program 57 was individuals who received psychiatric consultations for mental health crises after presenting to the ED.
All seven publications56–62 described virtual interventions that used the telephone to communicate with patients. In addition to the telephone, some of these virtual interventions also used video57,58 and text or email. 62 Post-crisis interventions varied widely in terms of duration, ranging from 24 h 59 to 12 months 56 post-discharge; however, post-crisis interventions were most commonly up to 6 months in duration.61,62 Virtual PSCBT, on the other hand, is 10–12 sessions in duration. 58 In terms of frequency, most post-crisis interventions made contact with discharged patients on a weekly basis,57,58,61 while some interventions left 1 or more months in between contacts with discharged patients.56,62 Virtual interventions were operating from hospitals,56,60 EDs,57,61 a regional suicide prevention center, 59 and regional EMS. 62 The PSCBT intervention was carried out by CBT therapists but did not specify from where the therapists were based. The remainder of the virtual follow-up interventions were performed by nurses,56,62 behavioral health clinicians or counselors,57,59 and/or psychologists or project staff with backgrounds in psychology or social work.60–62 With the exception of the virtual patient navigation program, 57 which aims to divert hospitalization, the goal of all other interventions is to reduce repeat suicide attempts or self-harm.56,58–62
Most studies reported results related to treatment outcomes,56–58,61,62 and two studies reported on the feasibility and acceptability.59,60 In terms of treatment outcomes (i.e., suicidal behaviors, depression scores), the results were mixed. For the TFP, 56 no benefit of the intervention was found, with 23.6% of the intervention group reattempting and 0.5% completing suicide during the follow-up period, compared with 20.3% of the control group reattempting and 1.9% completing suicide over the same period. The TBPI program 60 also showed no benefit of intervention, with no difference in suicide attempts within 30 days of baseline compared with the control group. PSCBT 58 similarly reported negative results in that the RCT was not feasible for youth and young adults recruited from crisis mental health services for depression and self-harm based on stop-go criteria, recruitment, retention, and safety concerns.
On the other hand, positive results were reported for the virtual patient navigation program, which demonstrated significantly fewer instances of self-harm for the virtual patient navigation program compared with the control group over the follow-up period (−8.7%). 57 Similarly, suicidal behaviors for the SPI 61 were significantly less likely to occur over the follow-up period for the intervention group compared with the control group (3.03 vs. 5.29%, odds ratio = 0.56; 95% CI: 0.33–0.95). VigilanS 62 also reported positive results in that the intervention group showed a greater downward trend in ED visits for suicide attempts after implementation of the intervention (−15.8%) compared with the period of time before implementation (−5.9%). Control groups showed either no change in suicide attempts or an increase in suicide attempts over the same period of time. In terms of feasibility and acceptability, the EFU program 59 was deemed valuable by the psychiatry residents at the ED and the crisis counselors at the suicide prevention center. The residents and counselors discussed improving certain areas of the referral process, wanting to know more about the operations of the ED and the community program, and difficulties in identifying patients who are well-suited for the EFU program. 59
Discussion
This scoping review utilized a broad search strategy to identify and synthesize the recent literature on VCC. Published articles represented a wide range of programs from around the globe, targeting a variety of patient profiles and clinical needs from youth to adults. In summary, we found that VCC has encompassed the initial crisis assessment, post-crisis follow-up, and high-intensity virtual options as alternatives to hospital and other facility-based intervention. The existing literature supports that these models are feasible when appropriately designed and implemented,22,33,50,51,60 and can function to supplement in-person services for the target patient populations.36,38,40,46,48,50 In comparison with a previous review on crisis telepsychiatry that identified no published examples of a program that provided urgent psychiatric services to individuals in their home prior to 2018, 13 we identified a range of programs that came into operation during the COVID-19 pandemic when a number of factors coalesced to promote the rapid virtualization of all health care.19,22,24,30–36,38,40–43,46,48–55 This was a time of relaxed regulations and increased willingness to adopt virtual modalities. While some services represented virtual care adaptations of pre-existing services (e.g., partial hospitalization program and virtual crisis stabilization unit),22,31,32,35,36,38,40–43,46,48–55 other programs represented completely new services in a virtual format.19,24,30,33,34
The identified studies were diverse in design, including a number of RCTs, observational studies, program evaluations, and qualitative study designs. Although infrequent, studies that compared virtual with in-person care showed that PHPs44,47,52–55 and IOPs 41 could be equally as good or better in terms of outcomes such as patient satisfaction, treatment effect size, depression and anxiety symptom trajectories, decreased symptoms (i.e., depression, suicidality), and increased parent-infant bonding, coping, functioning, positive mental health, and well-being. Virtual care was unequivocally superior to in-person care in terms of increased attendance (i.e., appointments, treatment completion) and decreased hospitalization rates.41,52,54,55 Virtual care did, however, frequently show longer average length of stay53–55 compared with in-person care. Virtual care and in-person care also differed in terms of user demographics. Virtual care patients are less likely to have psychosis, engage in suicidal behavior, be male, abuse substances, have cognitive impairment, and have recent contact with the referral source.38,50 Patients seen remotely when in crisis are more likely to reside further from the referral source and be older, while in-person care patients are more likely to require an urgent psychiatry assessment and be hospitalized, 38 highlighting the higher acuity of the in-person service recipients.
Most studies examined programs that operated out of call centers, EDs, or hospital clinics; however, there were a handful of studies looking at virtual mental health crisis intervention embedded within law enforcement and EMS,25,27–29,32 exemplifying novel ways of integrating teams in resource-effective ways. Interventions offering crisis assessment and in-person acute care alternatives discussed the necessity of strong integration with in-person services to allow step-up (and step-down) care when needed to ensure patient needs are met and safety concerns can quickly be addressed. Understanding how virtual services map onto a spectrum of care options should continue to be an area of investigation to optimize service planning. Additionally, many services discussed the potential for virtual assessment serving a lower acuity population and/or functioning in a triaging capacity to allow people to remain at home and reduce ED crowding20,36,38; however, the services also frequently feed into rapid access outpatient options such that an ED visit can be diverted and replaced with timely outpatient mental health care, which has been highlighted as an area requiring attention. 64 Only two studies included a cost-saving analysis,28,40 indicating that this is an area needing additional research.
Additionally, studies in this review generally focused on short-term outcomes (e.g., referrals, repeat ED visits, hospitalizations), and there was a lack of longer-term follow-up data. Comparatively, evaluation of virtual urgent care more broadly has supported cost-effectiveness, with emphasis on maximizing scope of practice for nonphysicians to meet the needs of lower acuity users, who are more frequent users of virtual services. 65
Conversely, there has been inconclusive evidence regarding the outcomes and cost-effectiveness of virtual wards for medical needs, highlighting this as an area needing more research with a focus on identifying what works for whom.66–69 There was also an absence of studies in this scoping review focused on providing virtual mental health crisis services to the geriatric population specifically, a population that would be important to study in the context of virtual care as this group is often lacking in technological literacy along with other barriers.70–73
Scoping reviews, like systematic reviews, are methodologically rigorous. 74 Both types create and follow protocols to produce replicable reviews.74,75 Compared with systematic reviews, one common weakness of scoping reviews is that they do not assess the methodological quality of research studies. 75 This means that the strength of the evidence is unknown, and conclusions drawn from the evidence could be biased and should be accepted with caution. That said, scoping reviews, unlike systematic reviews, typically aim to include studies with a variety of research designs.74,76,77 We adopted a very broad search strategy in an attempt to capture all available literature, but given the variability in terms used to describe virtual care, it is possible that some relevant studies were missed.
Conclusions
Virtual care has found its place in the mental health system, accelerated by the COVID-19 pandemic. The literature indicates that many virtual options for crisis care are feasible and show growing evidence of effectiveness, especially for treatment engagement rates and decreased hospitalization for patients with lower acuity care needs. Post-pandemic, many services have reverted to usual in-person models of care, and in many circumstances, this is likely superior for patients with higher acuity needs. 78 The available literature supports that we can continue to consider the role of VCC along the continuum of services, especially as a strategy to overcome barriers to care, offer person-centered options, and optimize human resources. Additional research is needed to compare virtual and in-person models, examine longer-term outcomes, and assess cost-effectiveness.
Authors’ Contributions
J.L.: Conceptualization, writing—original draft, investigation—data collection. J.H.: Conceptualization, writing—review and editing original draft, investigation—data collection. S.S.: Conceptualization, investigation—data collection, writing—review and editing. R.U.: Conceptualization, investigation—data collection; writing—review and editing.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.