
Abstract
Background:
Telemedicine has gained increasing relevance as an innovative approach to support continuity of care for individuals with cognitive impairment. However, evidence regarding usability and short-term clinical effectiveness in patients with amnestic mild cognitive impairment (aMCI) is still limited. The present study aimed to assess the usability, feasibility, and preliminary clinical efficacy of a dedicated telemedicine platform integrating cognitive telerehabilitation and teleconsultation services for individuals with aMCI and their caregivers.
Methods:
A multicenter prospective study was conducted across 10 Centers for Cognitive Disorders and Dementia in the Calabria region, Italy. Subjects with aMCI (aged 50–80 years) and their caregivers were enrolled and participated in a 4-week intervention. The program included asynchronous tablet-based cognitive telerehabilitation and scheduled teleconsultations providing educational and psychological support. Usability was evaluated using the System Usability Scale (SUS). Secondary outcomes included adherence, satisfaction, changes in neuropsychological measures, and caregiver burden, assessed before and after the intervention.
Results:
A total of 285 participants (144 patients, 141 caregivers) were enrolled, and 267 completed the study (retention rate: 93.6%). The overall mean SUS score was 79.03 ± 16.89, indicating good-to-excellent usability across patients, caregivers, and health care professionals. Significant improvements were observed in global cognition, episodic memory, disease insight, anxiety, depressive symptoms, neuropsychiatric manifestations, and caregiver burden (all p < 0.05).
Conclusions:
This telemedicine platform demonstrated high usability, strong adherence, and positive clinical effects after a short intervention period. These findings support the feasibility and potential value of digital telerehabilitation solutions for individuals with aMCI and their caregivers.
Keywords
Introduction
Telemedicine represents a rapidly expanding approach within health care systems, recently adopted as a means of delivering medical assistance and treatment remotely. The World Health Organization (WHO) defines telemedicine broadly as “the practice of medicine at a distance, where patient and health professional are separated by geographical distance, utilizing information and communication technologies for the exchange of valid information for diagnosis, treatment, and prevention of disease and injuries, research and evaluation, and for the continuing education of health care providers, all in the interests of advancing the health of individuals and their communities” (WHO Group Consultation on Health Telematics). 1
In recent years, particularly in the wake of the COVID-19 pandemic, telemedicine has garnered significant attention as health care services were often reduced to their bare minimum, 2 supported by emerging technologies. In this context, the development of innovative strategies to ensure continuity of care became imperative, with telemedicine proposed as a viable solution for the provision of remote services, including rehabilitation therapies. Telerehabilitation, defined as the delivery of rehabilitation services through information and communication technologies, 3 has been designed to reduce the length of hospital stays and to provide support for patients with motor disabilities and/or environmental barriers that limit their access to rehabilitation clinics postdischarge. This approach offers the advantage of delivering extended therapies tailored to individual patient needs while simultaneously optimizing health care delivery. 4
As an evolving field, telerehabilitation has outpaced the current level of research, encompassing a spectrum of therapeutic interventions and behavior therapies aimed at conditions such as stroke, movement disorders, dementia, and cognitive dysfunction, along with practices in physical therapy, occupational therapy, and special education. 5 Epidemiological data indicate that neurodegenerative diseases increasingly affect elderly patients and their families, posing a significant challenge for clinical medicine and necessitating the adoption of new care models.
In Italy, the prevalence of dementia is estimated at approximately 1.2 million elderly individuals, with a sharp upward trajectory correlated with age, alongside approximately 952,000 individuals with mild cognitive impairment (MCI). 6 Within this context, the future management of individuals with cognitive impairment is expected to increasingly leverage digital technology for diagnosis, monitoring, and treatment, particularly within elderly care systems.
Digital tools for patients with cognitive impairment may also yield time and resource efficiencies, facilitating the assessment of a wide range of cognitive functions and reducing geographical, economic, and social disparities in access to diagnostic and therapeutic options, thereby enhancing health care providers’ capacity to manage a larger number of patients remotely.7,8
The present study was aimed at assessing the usability and clinical efficacy of a telematic and telerehabilitation platform designed for individuals with MCI or early-stage dementia and their caregivers. To the best of our knowledge, this is the first multicenter study conducted in Calabria (a region in the South of Italy) evaluating both the usability and clinical efficacy of a telemedicine and telerehabilitation platform across multiple Centers for Cognitive Disorders and Dementia (CCDDs). This is particularly relevant given that in this region the access to specialized cognitive care services can be challenging, especially for residents of smaller towns and rural areas. By implementing a standardized yet personalized approach, this study provides valuable insights into the feasibility of digital interventions in settings with geographic and infrastructural barriers.
Methods
STUDY PROTOCOL
A total of 10 CCDDs, equally distributed throughout the region of Calabria, in Italy, were invited to participate in the study. The selected centers were chosen based on their expertise in the diagnosis and management of subjects with MCI and dementia. The flowchart of the study is shown in Fig. 1. The recruitment period lasted from April to December 2023. Each CCDD was committed to recruiting subjects affected by amnestic MCI (aMCI) and their caregivers, if available. The inclusion criteria were as follows: (1) diagnosis of aMCI9,10; (2) age between 50 and 80 years; (3) at least 5 years of education; (4) stable pharmacologic treatment for at least 3 months; and (5) willingness to participate, after being adequately informed about the aims and methods of the study. Exclusion criteria were as follows: (1) the presence of visual, acoustic, or sensitive deficits; (2) the presence of other neurological or psychiatric disorders able to compromise cognitive functions; and (3) living in areas without adequate internet connection. For each subject affected by aMCI, a related caregiver was recruited, if available, fulfilling the following criteria of inclusion: (1) living with the subject affected by aMCI and (2) willing to participate in the study. All recruited subjects with aMCI and their caregivers gave their written informed consent to participate in the study. The CCDD of the Neurology Unit of the University “Magna Graecia” of Catanzaro was the Hub-Coordinating Center of the study project, with a role of planning, development, and implementation of all interventions. In each CCDD, the study team included a physician (neurologist/geriatrician), a neuropsychologist, and a health care social worker. The activities of the physician included: (1) recruitment of subjects with aMCI and their caregivers; (2) explanation of the study aims and protocol; (3) assistance in signing the informed consent, if required; (4) clinical monitoring during the study period; (5) monthly reports of progress activities; and (6) final report.
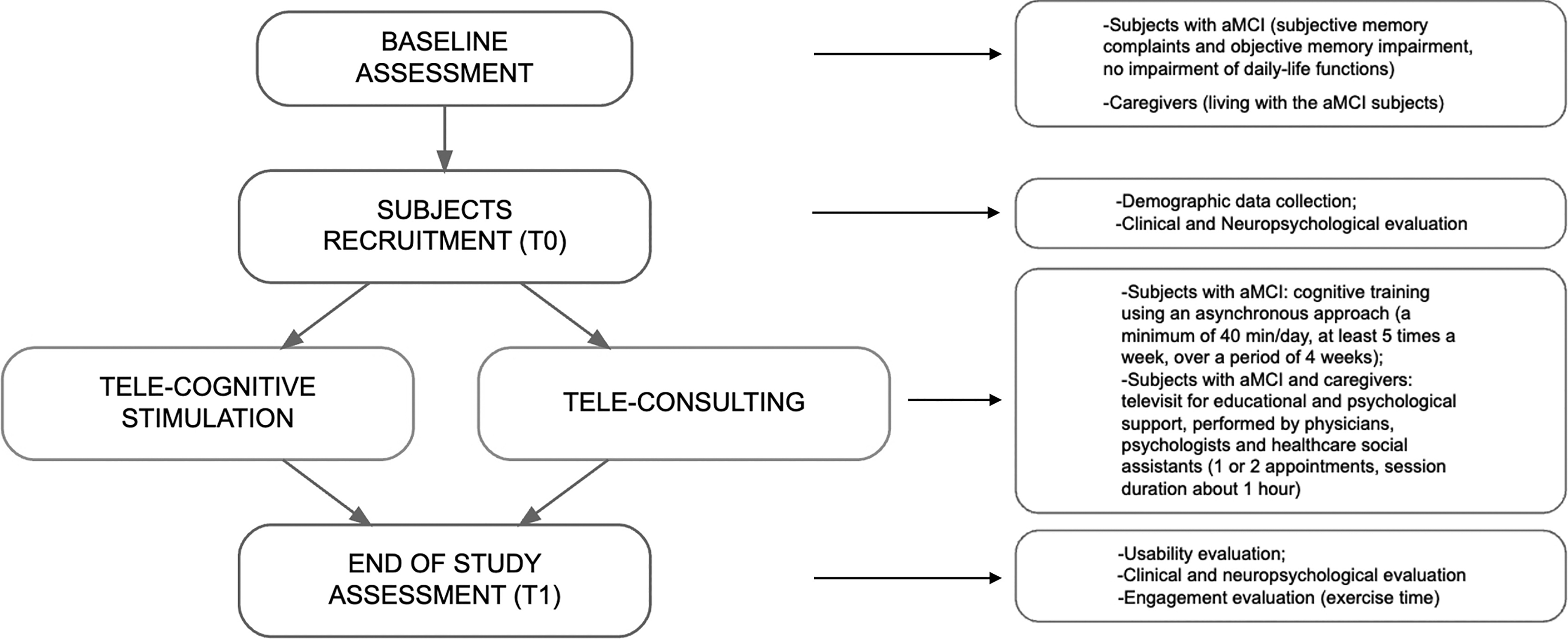
Flowchart of the project.
The neuropsychologist roles covered the following: (1) the extended neuropsychological evaluation of subjects with aMCI, performed at baseline (T0) and after a month of telerehabilitation (T1); (2) data entry on the platform; (3) definition of the personalized stimulation exercises programs; (4) training of the recruited subjects with aMCI to the use of the telerehabilitation application, downloaded on a dedicated tablet (at least one face-to-face meeting + telephone/online availability); (5) monitoring of subjects’ activity; (6) teleconsultations with caregivers; (7) monthly reports of progress activities; and (8) final report, usability assessment, and satisfaction questionnaire.
The health care social worker had the role of: (1) interviewing the caregivers; (2) entering data on the platform; (3) support of the link with the general practitioners of the subjects enrolled in the project; (4) participation to the teleconsultation; (5) providing information regarding assistance or services available in the area of provenience; (6) monthly reports of progress activities; and (7) final report, usability assessment, and satisfaction questionnaire.
The study protocol was approved and funded by the Italian Ministry of Health in August 2022 and then approved by the Local Ethics Committee (protocol code n. 341, November 17, 2022), in accordance with the Declaration of Helsinki.
Clinical and neuropsychological evaluation
All demographic and clinical data of the subjects affected by aMCI, recruited in the study, were collected in an electronic data collection sheet, provided by an anonymization procedure. Demographic and socio-sanitary data of related caregivers were also collected. At baseline (T0), all subjects with aMCI underwent an extended neuropsychological evaluation, including: Mini-Mental State Examination (MMSE), 11 Clinical Dementia Rating Scale (CDR), 12 Clinical Insight Rating Scale (CIRS), 13 Activities of Daily Living (ADL), 14 Instrumental Activities of Daily Living (IADL), 15 General Anxiety Disorder-7 (GAD-7), 16 Patient Health Questionnaire-9 (PHQ-9), 17 and Babcock Story Recall Test. 18 Caregiver’s Burden Inventory (CBI) 19 and Neuropsychiatric Inventory (NPI) 20 scores were collected from caregivers. The same extended evaluation was performed in subjects with aMCI, after the 4-week cognitive telerehabilitation program, and in caregivers, after the 4-week teleconsultation program (T1).
Telemedicine platform
A digital telemedicine platform (named “Pohema”), already in use at the University “Magna Graecia” of Catanzaro, was implemented, creating a study dedicated domain. The web platform, hosted in a secure cloud, was available for the entire duration of the study, allowing the team study to store sociodemographic and clinical data in the dedicated e-clinical records and manage the activities planned for subjects affected by aMCI/dementia and their caregivers. The platform had a responsive structure, so it was equally usable from PCs, tablets, and smartphones simply through an internet connection. The telemedicine platform domain was also designed to host and manage applications dedicated to the service of cognitive telerehabilitation and teleconsultations for educational and psychological support to subjects affected and caregivers (Fig. 2A).
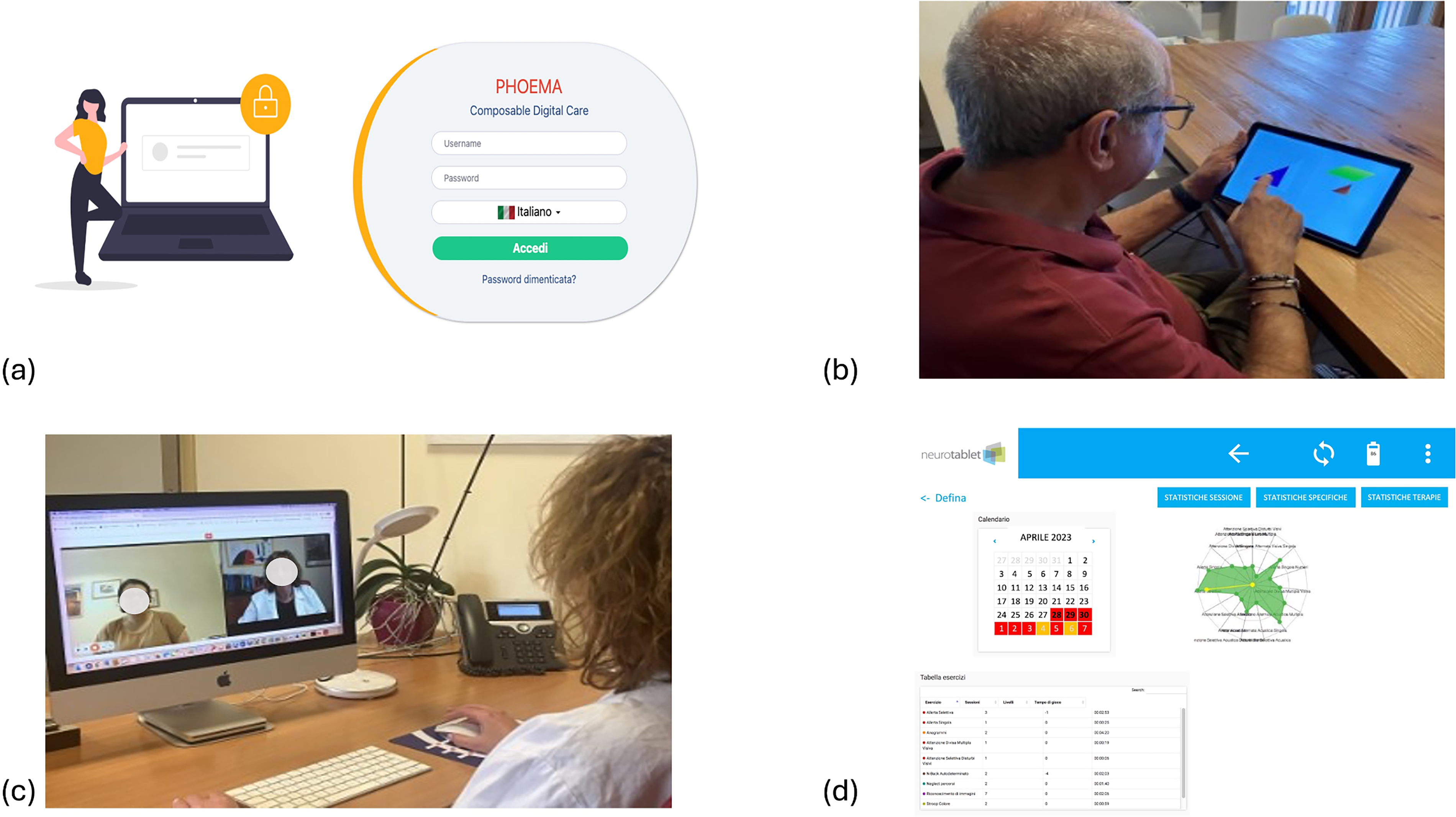
Representation of telemedicine platform, tele-visit, and telerehabilitation activities.
Cognitive telerehabilitation
An application for cognitive telerehabilitation (Neurotablet®) 21 was used to create personalized therapeutic programs, set by the psychologist, for each subject affected by aMCI included in the study. The application was connected with the telemedicine platform, allowing the therapists to design the cognitive rehabilitative program, monitor the activities of the subjects during the treatment period, and also to communicate with them, using the messaging function. The application was given free of charge to the participants for the treatment period, and all participants received a tablet with internet access provided to use it.
The application had two different interfaces: a therapist and a patient/caregiver interface. The former supported the therapist in setting specific objectives of the cognitive rehabilitation treatment for each recruited subject, selecting a series of exercises for the therapeutic path, and remotely following progress data. The patient interface was a simplified, user-friendly training modality, customized to carry out cognitive treatment at home, even without the help or constant assistance of a caregiver, while being monitored remotely (Fig. 2B). The tablet application contained 30 different exercises, with a total of 10,000 levels, divided into six cognitive areas: attention, executive functions, speech, memory, neglect, and perception. The telerehabilitation sessions were performed with an asynchronous approach, that is, with self-administered computer-based exercises. The screens were all aimed at carrying out rehabilitation and providing simplified feedback.
At the end of each session of exercises, a graphical representation of the subject’s progress was shown (Fig. 2C). This approach did not require the online presence of a therapist and was aimed at maximizing the independence that can be achieved in carrying out therapy. The telerehabilitation sessions were specifically structured to adapt the training to the different patients’ objectives and progress during the rehabilitation period. Therapists can also remotely monitor the data of the recruited subjects as well as communicate with them through the tablet application itself. The subjects affected by aMCI were invited to exercise, at least 5 times a week, for a minimum of 40 min/day, for a total program period of 4 weeks. The expected total time dedicated to the exercises was 800 min for each subject.
Tele-visit for educational and psychological assistance
The telemedicine platform was also implemented to host the application dedicated to the service of teleconsultation, dedicated to subjects with aMCI and their caregivers (Fig. 2D). This service was designed to offer tele-visits for educational intervention and psychological support, operated by the study team health care professionals involved in the project (physician/neuropsychologist/health care social worker). The teleconsultations were scheduled every 2 weeks. During each session, all participants had the opportunity to discuss any issues or discomfort they were facing. Health care professionals played a key role in supporting individuals with aMCI and their caregivers, offering information on strategies to cope with the disease and its associated challenges. They also informed participants about local services, facilities, and active organizations that could help create a supportive network. The goal of these activities was to provide information on the clinical aspects of the disease, management at home and in various social settings, and to offer support for emotional and relational issues.
Usability assessment
The primary outcome of the study was the assessment of the usability of the telemedicine and telerehabilitation platform, and related devices, evaluated by the subjects affected by aMCI, their caregivers, and the health care professionals (10 neuropsychologists and 10 health care social workers), involved in the study. Usability was assessed using the System Usability Scale (SUS) 22 (Supplementary Fig. S1). This scale is a simple, 10-item attitude Likert scale with five response options for respondents: from strongly disagree (1) to strongly agree (5), giving a global view of subjective assessments of usability. It was developed by John Brooke as a tool to be used in usability engineering of electronic office systems. A mean SUS score of 68 or higher indicates that the evaluated system has a good usability, whereas SUS scores above 80 correspond to excellent usability.23,24 All participants were asked to rate the usability of the telemedicine and telerehabilitation platform, called “system” in the SUS questionnaire.
Another parameter we considered was the tablet usage time for telerehabilitation activities, to investigate how user-friendly the system was perceived by the individuals, with the instructions they had been given. Usage time was calculated based on the following parameters: (1) The number of connections made, including information on start and end times; (2) the duration of each connection, expressed in seconds; (3) for each completed exercise, data on start time, stop time, and progression were recorded; and (4) the system also measured instances in which the tablet remained connected, but assigned exercises were not performed.
Finally, all participants (subjects with aMCI, caregivers, and health care professionals) completed a satisfaction questionnaire assessing their utilization of the system. Secondary outcomes of the study were changes in neuropsychological test scores of people with aMCI and in caregiver burden scores, after the telerehabilitation programs.
STATISTICAL ANALYSES
Statistical analyses were conducted using Epi Info version 7.2 (Epi Info™, Centers for Disease Control and Prevention, Atlanta, USA). Descriptive statistics were calculated for demographic variables, clinical characteristics, neuropsychological test scores, SUS scores, and telerehabilitation usage data (number and duration of sessions). Continuous variables are reported as mean ± standard deviation (SD), whereas categorical variables are presented as frequencies and percentages.
Before applying parametric tests, the distribution of continuous variables was evaluated for normality through the Shapiro–Wilk test. As no substantial deviations from normality were detected, parametric statistical tests were used.
Paired-samples Student’s t tests were applied to compare neuropsychological and clinical outcomes at baseline (T0) and after the 4-week telerehabilitation intervention (T1). Changes in global cognition, episodic memory, psychological symptoms, neuropsychiatric manifestations, and caregiver burden were analyzed.
Usability outcomes were examined using one-way analysis of variance (ANOVA) to compare mean SUS total scores and individual item scores across user groups (patients, caregivers, and health care professionals). When statistically significant differences were observed, Bonferroni-adjusted post hoc t tests were performed.
To investigate factors associated with system usability, univariate logistic regression analyses were conducted using a SUS score ≥ 68 as the dependent variable. Separate models were run for patients and caregivers. Independent variables included age, gender, and educational level, with stratification applied where appropriate to account for potential confounding.
Adherence to the telerehabilitation program was assessed by analyzing total usage time (min). Pearson correlation analyses were performed to examine associations between usage duration and demographic variables. Multivariate logistic regression models were subsequently used to evaluate the independent effects of age, gender, education level, and baseline MMSE score on engagement with the cognitive stimulation program.
All regression results are reported as odds ratios (ORs) with 95% confidence intervals (CIs). Statistical significance was set at p < 0.05 for all analyses.
Results
A total of 285 participants were enrolled in the study, including 144 subjects with aMCI and 141 related caregivers. The study achieved an overall retention rate of 93.7% (93% for patients’ group and 94.3% for caregivers’ group). During the study period, 10 patients (6 males and 4 females) discontinued participation due to health or family-related issues (n = 7), personal difficulties (n = 2), or loss of interest (n = 1). Eight caregivers (2 males and 6 females) dropped out because of the related patients’ discontinuation. The total attrition rate was 6.3%, mainly due to medical events or personal circumstances unrelated to the intervention. No participant dropped out due to dissatisfaction or difficulties with using the digital tools. The final sample included 134 patients (62 males and 72 females; mean age: 67.12 ± 12.92 years; mean education: 8.54 ± 3.45 years) and 133 caregivers (41 males and 92 females; mean age: 54.91 ± 14.65 years), whose data were analyzed for the study outcomes.
USABILITY
The overall usability score of the digital intervention was 79.03 ± 16.89 (mean ± SD), indicating almost excellent usability across all user groups (patients, caregivers, health care professionals, Fig. 3). Patients reported a mean score of 74.01 ± 17.42, caregivers 83.28 ± 14.53, and health care professionals 83.89 ± 18.83. In the whole study population, male users scored 78.89 ± 17.51, whereas female users scored 79.10 ± 16.62. Educational level influenced usability scores, with participants having 8 or fewer years of education rating the system with a SUS score of 75.82 ± 17.85, compared with 81.45 ± 15.77 for those with more than 8 years of education. Within subgroups, male caregivers reported the highest usability scores at 87.56 ± 12.52, followed by female caregivers at 81.55 ± 15.00. Female patients rated usability slightly higher than male patients, with scores of 74.61 ± 17.66 and 73.26 ± 17.30, respectively.
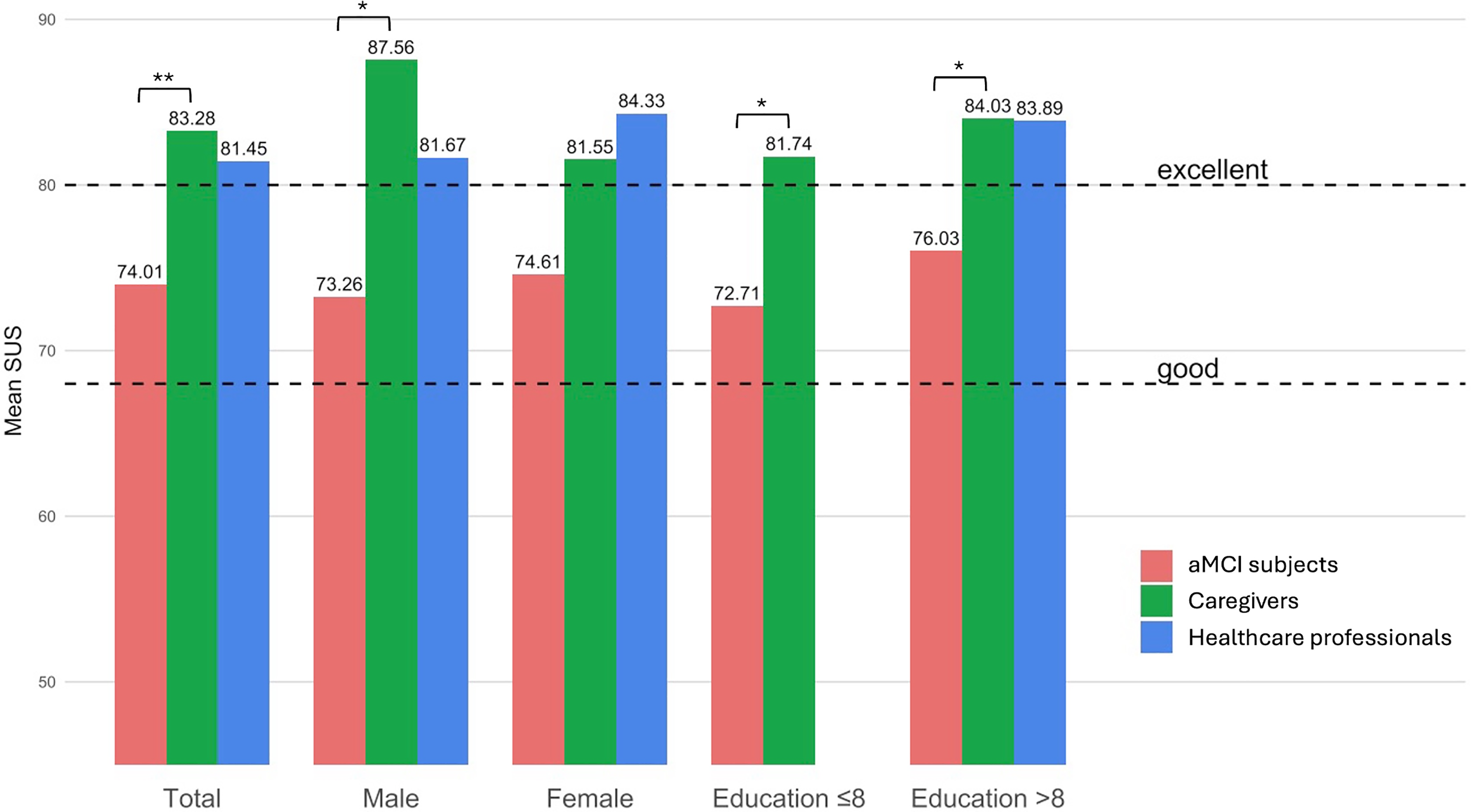
Mean System Usability Scale scores reported by aMCI subjects, caregivers, and health care professionals, across different subgroups (total, male, female, education ≤ 8 years, education < 8 years). Bars represent mean values. Dashed lines indicate thresholds for good usability (68) and excellent usability (80). Asterisks denote statistically significant differences between groups (* for < 0.05; ** for < 0.001). aMCI, amnestic mild cognitive impairment.
All these scores exceeded the standard usability cutoff of 68, confirming the general acceptability of these digital tools across demographics. In our analyses, the age threshold significantly associated with SUS score ≥68 was identified at 70 years (OR = 0.51, p = 0.017) for the aMCI subjects and at 65 years (OR = 0.22, p = 0.009) for the caregivers (Table 1).
Descriptive and Linear Regression Analyses for Amnestic Mild Cognitive Impairment Subjects and Caregivers Scoring System Usability Scale 68 or Higher
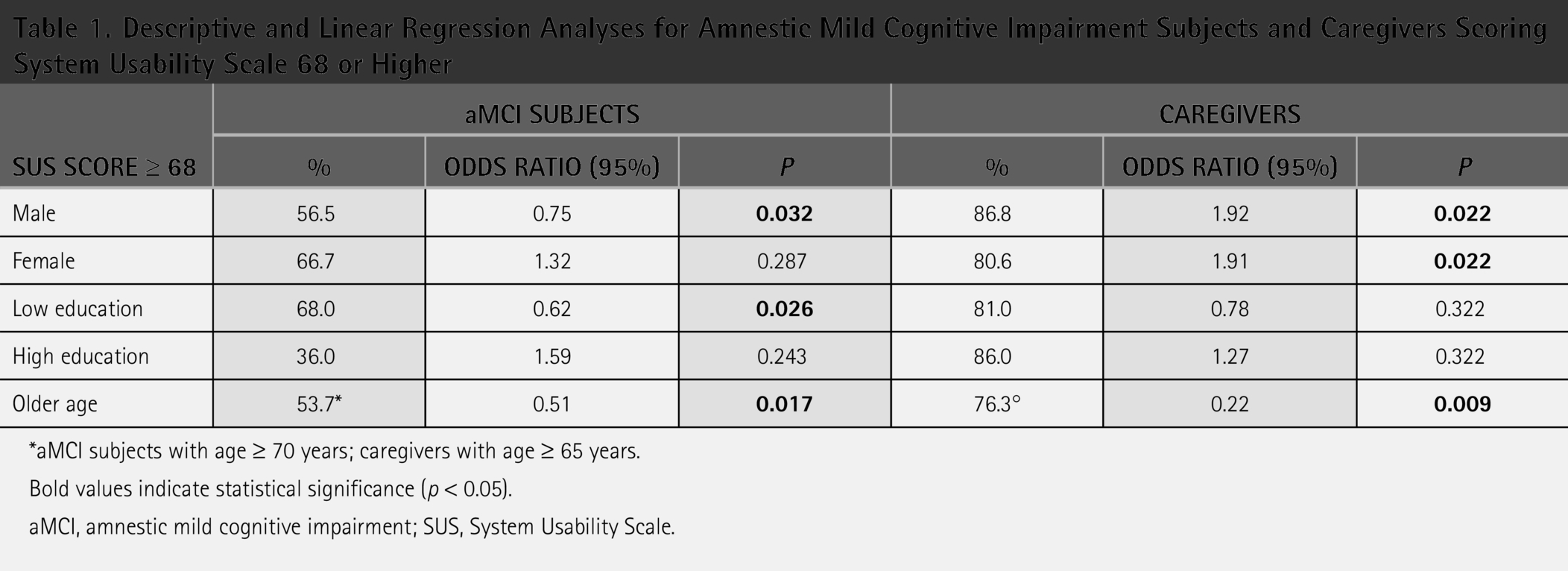
*aMCI subjects with age ≥ 70 years; caregivers with age ≥ 65 years.
Bold values indicate statistical significance (p < 0.05).
aMCI, amnestic mild cognitive impairment; SUS, System Usability Scale.
Higher SUS scores (≥68) were more frequent among female patients under 70 years of age and with higher education and in caregivers younger than 65 years, regardless of gender. Among patients, 62% scored above the cutoff, including 58% of female patients (OR = 1.32, p = 0.287), 57% of those with low education (OR = 0.62, p = 0.026), and 38% of those over 65 years (OR = 0.51, p = 0.017). Among caregivers, 73% of those under 65 scored above the cutoff (OR = 4.51, p = 0.0089), as did 68% with higher education (OR = 1.27, p = 0.322) and 69% of females (OR = 1.91, p = 0.022). These findings indicate that younger, female, and more educated users perceived the digital tools as more usable and accessible. Results of the ANOVA analysis, followed by Bonferroni post hoc t tests, for the mean scores of each answer on the SUS questionnaire are shown in Fig. 4.
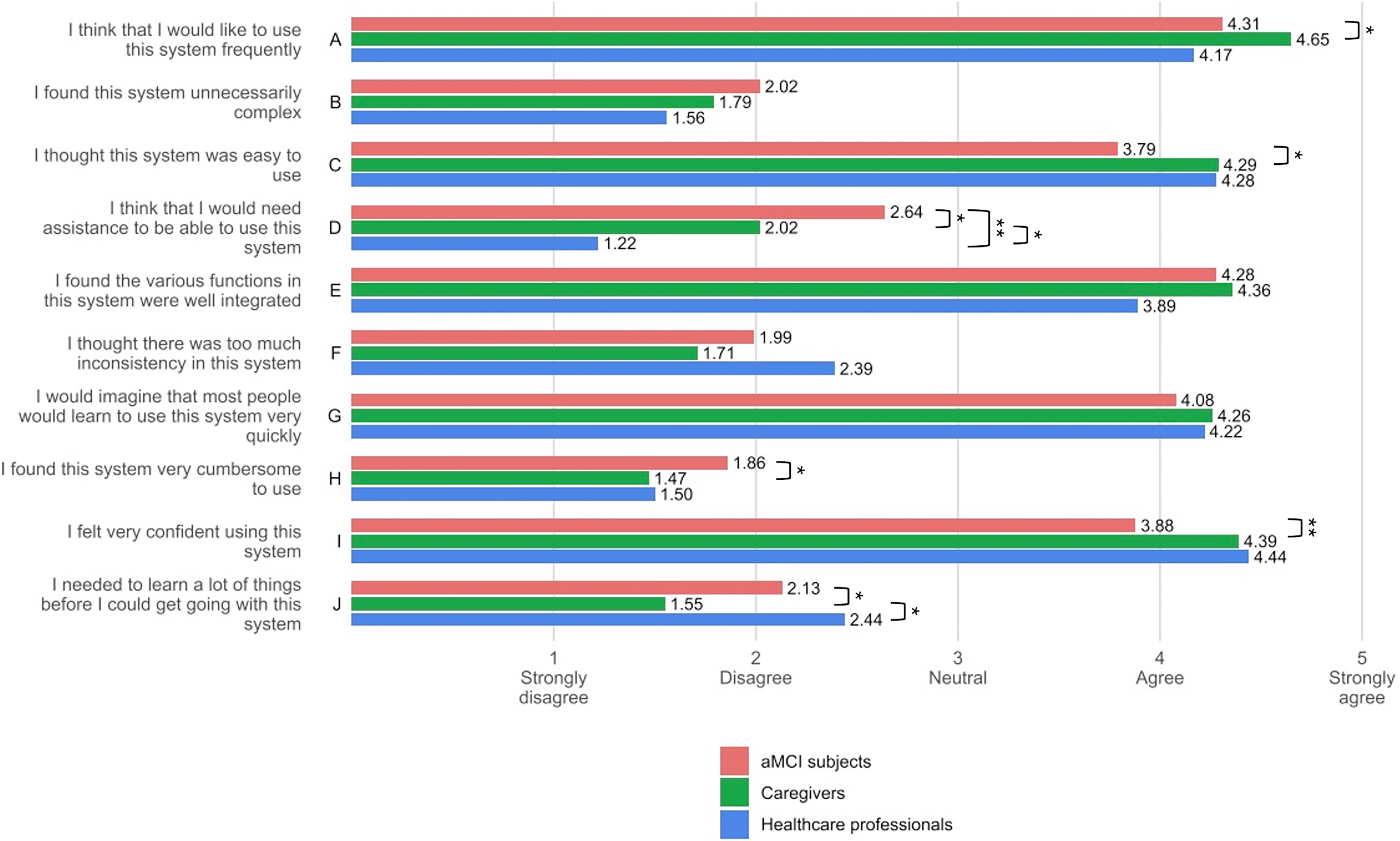
Mean System Usability Scale (SUS) item ratings on a 1–5 Likert scale for the 10 SUS statements (
Adherence with the cognitive stimulation program, delivered through the tablet, was measured by adherence to the recommended schedule: at least five sessions per week of a minimum of 40 min each, over 4 weeks (approximately 800 min). Usage data revealed that patients generally exceeded these expectations, with an overall mean usage time of 1,014.6 ± 588.6 min (range: 120–3,600 min). A univariate logistic regression analysis stratified by sex showed significant differences: male participants engaged for an average of 1,142.4 ± 664 min, compared with 906.6 ± 495.6 min among female participants (Pearson’s coefficient −0.18; p = 0.025). In contrast, education did not appear to be a significant factor: participants with higher education exercised for an average of 1,042.8 ± 521.8 min, whereas those with lower education for 999.3 ± 625.6 min (Pearson’s coefficient 0.11; p = 0.210). Age-wise adherence was consistent across groups, with participants under 65 years averaging 1,009.3 ± 518.15 min of activity, those aged 65–74 averaging 1,041.7 ± 586.8 min, and those over 75 averaging 952.5 ± 699.5 min (Pearson’s coefficient 0.12; p = 0.068). Multivariate logistic regression showed no significant associations between the duration of cognitive stimulation activities and age or education, whereas a trend was observed for gender (male) with OR equal to 2 (95% CI: 0.97–4.10; p = 0.05) (Table 2).
Multivariate Logistic Regression Analysis of the Associations Between Age, Gender, and Education Level and Duration of Telerehabilitation Sessions
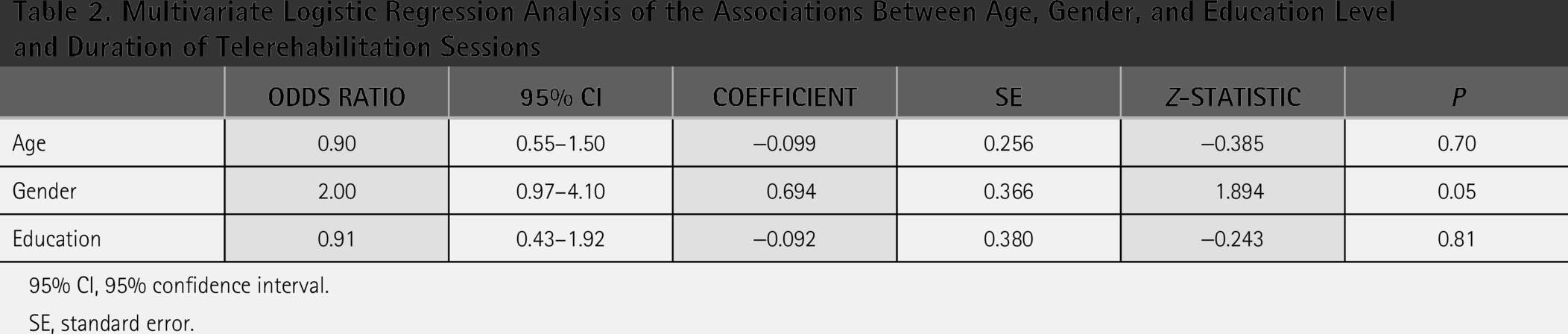
95% CI, 95% confidence interval.
SE, standard error.
SATISFACTION
Among subjects with aMCI, 99% reported a positive experience in this study, with 57.6% of them finding the used system easy to learn and 47.5% easy to use. A total of 80.8% expressed willingness to repeat the experience, which was considered as very useful by 87.9% of these subjects, and about 66% of them reported high satisfaction. Among caregivers, 100% reported a positive experience, with 71.6% finding the system easy to learn and 76.5% easy to use. About 95% of caregivers rated the intervention as very useful, 82.7% were willing to repeat the experience, and 72.8% expressed a high satisfaction. Subjects with aMCI and caregivers were also asked whether the experience was tiring or disturbing (aMCI: 2.0%, caregivers: 6.2%) and whether the time dedicated was appropriate (aMCI subjects: 70.7%, caregivers: 76.5%). Health care professionals reported a positive experience in all cases, with 90.0% finding the system easy to learn and 70.0% easy to use. High satisfaction was reported by 70.0% of them (Fig. 5).
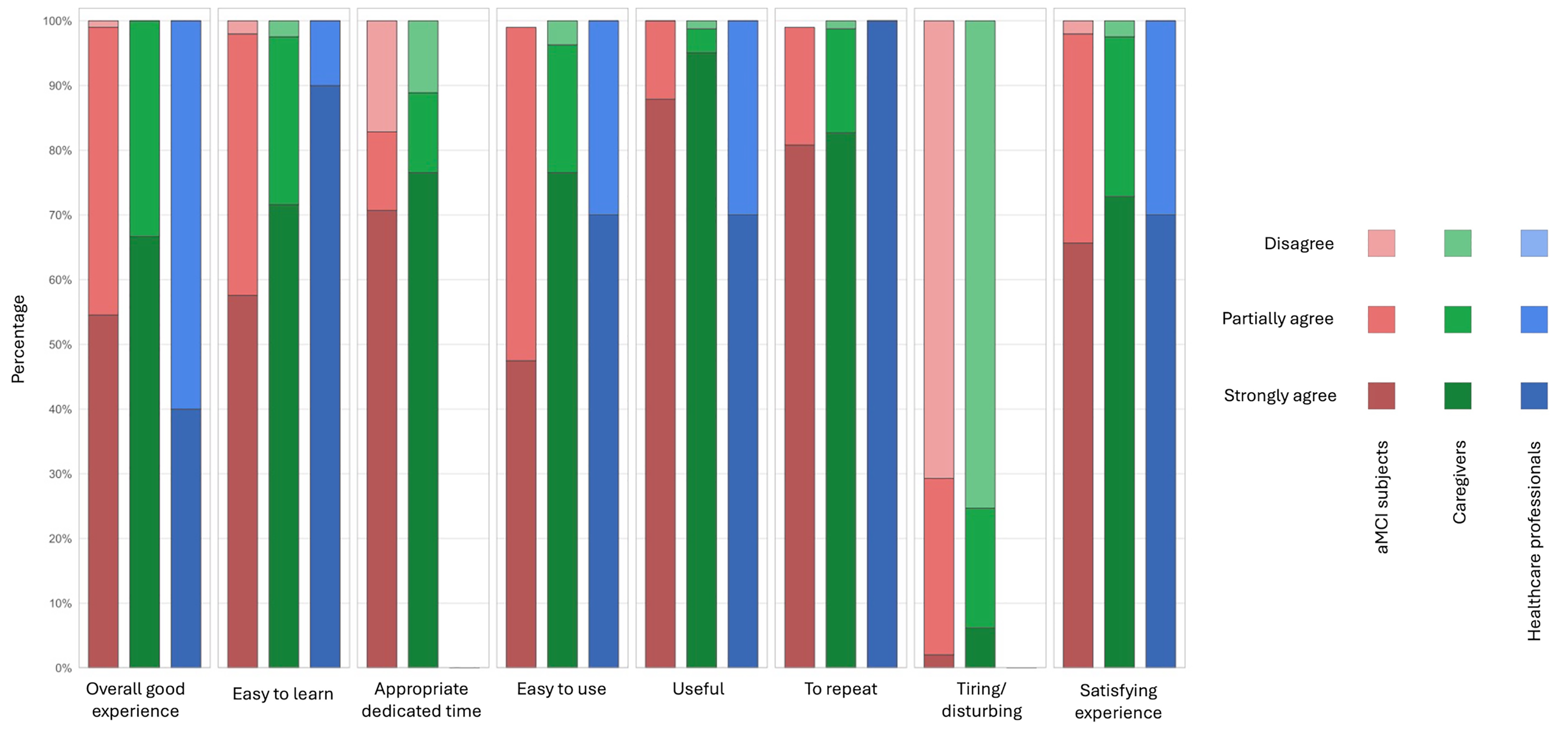
Satisfaction level assessment of the telemedicine system, divided by participant groups (aMCI subjects, caregivers, health care professionals). aMCI, amnestic mild cognitive impairment.
EFFICACY
Statistical analyses comparing clinical outcomes before and after the 1-month intervention demonstrated significant improvements across several domains (Fig. 6).
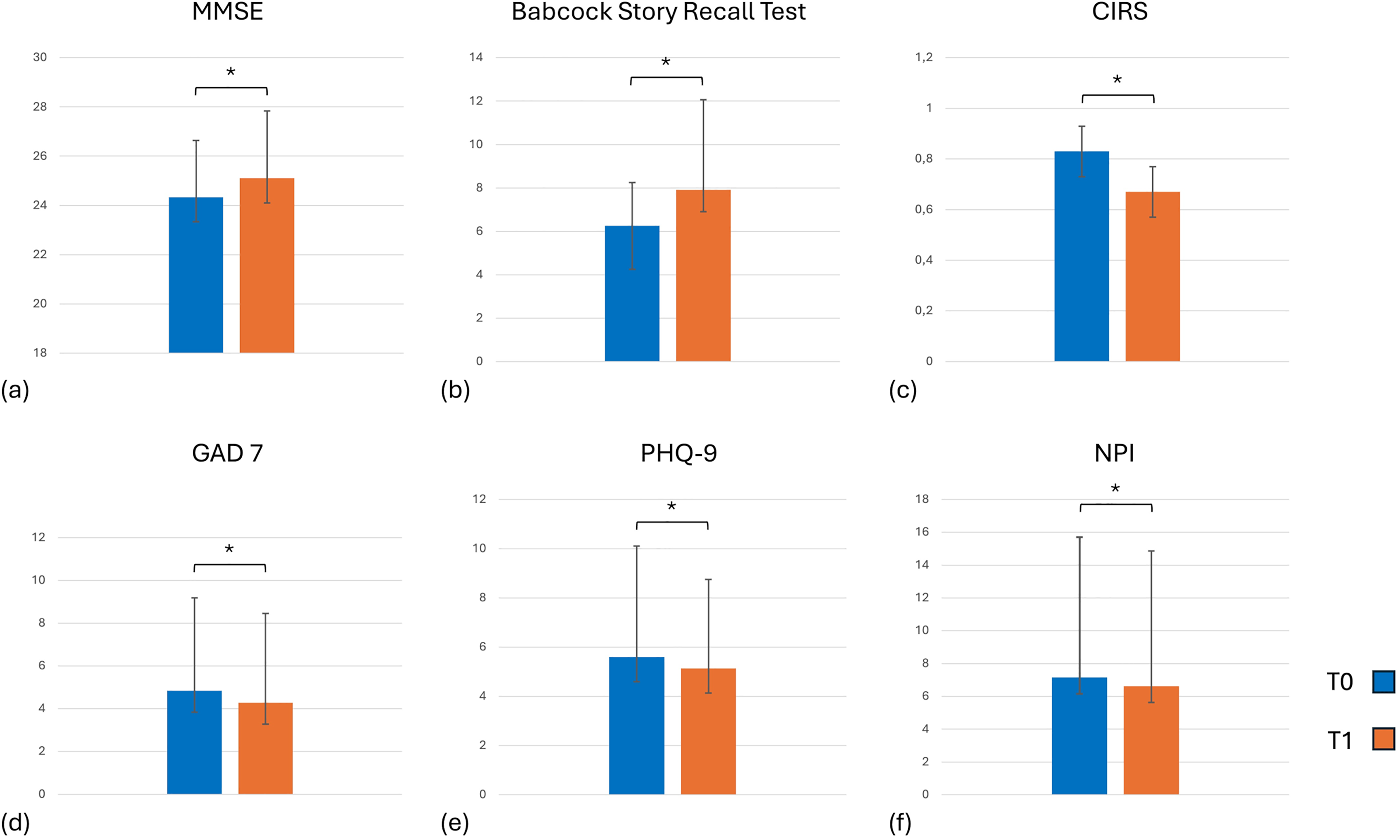
Mean pre- and postintervention scores on clinical measures: results showed statistically significant improvement (* for p < 0.05) within aMCI group:
Global cognitive function, assessed via the MMSE, improved from a mean ± SD of 24.33 ± 2.31 at baseline (T0) to 25.10 ± 2.74 postintervention (T1; p = 0.003). Episodic memory, evaluated with the Babcock Story Recall Test, increased from 6.25 ± 3.76 to 7.91 ± 4.16 (p = 0.001), and disease insight, as measured by the CIRS, improved from 0.83 ± 1.51 to 0.67 ± 1.34 (p = 0.031). Psychological well-being also showed measurable enhancement: anxiety scores (GAD-7) decreased from 4.84 ± 4.34 to 4.28 ± 4.18 (p = 0.006) and depression scores (PHQ-9) from 5.60 ± 4.51 to 5.14 ± 3.61 (p = 0.004). Neuropsychiatric symptoms, as assessed by NPI, declined in both frequency and severity, with scores decreasing from 7.15 ± 8.55 to 6.62 ± 8.24 (p = 0.023). Finally, caregiver burden, measured by the CBI, was significantly reduced, with mean scores decreasing from 9.57 ± 14.46 at T0 to 4.32 ± 10.37 at T1 (p < 0.001). As expected, CDR, ADL, and IADL scores did not show significant changes after the intervention, likely reflecting the short follow-up period and the relatively preserved functional status of the enrolled population. These findings highlight the feasibility, usability, and preliminary clinical efficacy of the digital intervention in supporting cognitive health and psychological well-being in patients with MCI, while also alleviating caregiver burden.
Discussion
This study evaluated the usability and preliminary clinical efficacy of a digital health intervention integrating a telemedicine platform with telerehabilitation tools for individuals with aMCI or early-stage dementia and their caregivers. Notably, it represents the first multicenter evaluation of an integrated telemedicine and telerehabilitation platform across multiple CCDDs in Calabria, a region where access to specialized cognitive care is often limited, particularly in rural and underserved areas. Overall, the findings provide valuable insights into the feasibility, acceptability, and potential clinical value of digital interventions within cognitive care pathways, especially in settings characterized by limited availability of specialized services.
Usability represents a key determinant of successful telemedicine implementation, as poorly designed systems may reduce adherence and compromise care delivery. In contrast, intuitive and user-friendly platforms can enhance engagement, reduce disparities, and improve the effectiveness of remote interventions. 25 In the present study, the telemedicine platform demonstrated good-to-excellent usability across all user groups, with SUS scores consistently exceeding the accepted threshold. These results indicate that the system was well accepted by patients, caregivers, and health care professionals, supporting its feasibility in real-world clinical settings.
Higher perceived usability was observed among younger, female, and more educated participants, a pattern consistent with previous literature on digital health adoption. Interestingly, male patients showed longer engagement times with the telerehabilitation exercises, whereas female patients and caregivers reported higher usability scores. These differences may reflect variations in time availability, role expectations, and daily responsibilities, as female participants often experience greater caregiving and domestic demands. 26 Older caregivers and those with lower educational levels reported more difficulties, highlighting the need for tailored training and ongoing technical support to ensure inclusivity for digitally vulnerable subgroups. 27 Despite these differences, overall adherence to the telerehabilitation program was high, with most participants exceeding the recommended training duration, suggesting that the intervention was intuitive and capable of sustaining engagement in routine practice.
Beyond usability, the intervention was associated with significant short-term improvements in multiple clinical domains, including global cognition, episodic memory, insight, anxiety, depressive symptoms, neuropsychiatric manifestations, and caregiver burden. Although the follow-up period was limited to 1 month, these findings suggest that digital telerehabilitation may offer benefits not only for cognitive functioning but also for psychological well-being and relational aspects of care. The observed reduction in caregiver burden is particularly relevant, as caregivers play a central role in treatment adherence and long-term patient outcomes. 28
The digital platform also facilitated a coordinated, multidimensional approach to care across multiple CCDDs, enabling health care professionals to deliver standardized yet personalized interventions. High satisfaction was reported by patients, caregivers, and professionals, who appreciated the system’s ease of use and perceived clinical utility. The willingness of all groups to repeat the experience supports the potential scalability and sustainability of this model within public health systems. 29
Limitations
Several limitations should be acknowledged. First, the study included only individuals with MCI, which may limit the generalizability of the findings to patients with more advanced cognitive decline. Second, the MMSE was used as one of the outcome measures; this tool is known to present a ceiling effect in individuals with MCI, potentially limiting its sensitivity to detect subtle cognitive changes. Third, the relatively short follow-up period and the sample size constrain conclusions regarding long-term efficacy and durability of the observed effects. Future studies should include longer follow-up periods, larger and more diverse samples, and cognitive measures with greater sensitivity to change.
Conclusions
In conclusion, this study provides encouraging evidence supporting the usability, acceptability, and preliminary clinical efficacy of a digital telemedicine and telerehabilitation platform for individuals with aMCI and their caregivers. These findings suggest that integrated digital solutions may represent a sustainable and scalable approach to support cognitive and emotional health, enhance caregiver support, and reduce health care disparities in aging populations. Future research is warranted to confirm long-term outcomes and optimize accessibility for broader user populations.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of “Sezione Area Centro, Regione Calabria” (protocol code n. 341, November 17, 2022).
Authors’ Contributions
Conceptualization: G.A. and R.D.L.; method development: G.A., R.D.L., G.C., and V.L.; bibliographic research: V.L., G.A., G.T., and G.C.; data production: G.C., V.L., R.C., N.C., R.B.B., F.G., M.L., P.I., G.F., F.A., L.A., and G.A.; writing—original draft preparation: V.L. and G.A.; data analysis and visualization: G.C., G.T., V.L., R.D.L., J.B., and N.I.; supervision: G.A., R.D.L., A.G., and M.P.B. All authors have read and agreed to the submitted version of the article.
Footnotes
Funding Information
This research was funded by the Italian Minister of Health, Fund for Alzheimer’s and other dementias, 2021–2023.
Data Availability Statement
The data used in this study will be made available upon reasonable request addressed to the corresponding author of this article.
Disclosure Statement
The authors declare no conflicts of interest.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.