
Abstract
Objective:
Although public interest in telemedicine is growing, limited research has examined the necessary conditions for its usage. Therefore, this study aims to identify these conditions in Japan and China.
Methods:
A self-developed questionnaire was administered between 2022 and 2023, yielding 787 valid responses in Japan and 840 in China. In addition, 241 Japanese and 194 Chinese supplemental responses were collected in 2025. Factor analysis and necessary condition analysis (NCA) were applied.
Results:
Based on the initial samples, eight factors were extracted: cost and accessibility, social influence, safety and reliability, adaptive readiness, technology confidence, perceived data security, facilitating conditions, and perceived usefulness. NCA revealed cross-national differences. Japanese participants mainly regarded perceived usefulness (d = 0.12–0.31) and facilitating conditions (d = 0.15–0.29) as necessary conditions, whereas Chinese participants perceived a broader set of prerequisites. Subgroup analyses further indicated that safety and reliability were the most critical necessary conditions for experienced users in both countries (Japan: d = 0.44; China: d = 0.28). Hierarchical clustering analysis further revealed three bottleneck trajectories of constraints: gradual-bottleneck users (progressive constraints), high-bottleneck users (sudden demand surges), and early-bottleneck users (persistent initial constraints). Crucially, the supplemental samples further confirmed the reliability and validity of the eight-factor structure and the temporal consistency of the necessary conditions for sustained usage.
Conclusion:
The findings highlight the need for tailored telemedicine strategies. In particular, maintaining safety and reliability represents a nonnegotiable prerequisite for sustained telemedicine usage in both countries. The developed instrument, combined with NCA, offers a transferable approach for identifying constraints and developing more adaptive and equitable telemedicine strategies.
Keywords
Introduction
Telemedicine is defined as the use of telecommunication technologies to support the delivery of medical, diagnostic, and treatment-related services, with distance being a critical factor. 1 This approach not only improves accessibility to healthcare services but also enhances efficiency in care delivery. 2 In addition, telemedicine successfully mitigates the increasing healthcare burden associated with aging populations and chronic diseases, reducing emergency rates among older adults.3,4
During the COVID-19 pandemic, research exploring the factors influencing the intention to adopt telemedicine surged. Many studies have applied the generalizable technology acceptance model of the unified theory of acceptance and use of technology 5 and validated the influence of factors such as performance expectancy,3,6 effort expectancy,6,7 social influence,8,9 and facilitating conditions.10,11 In addition, telemedicine security is crucial for its promotion, 12 whereas concerns about privacy and resistance to change pose obstacles.8,13 Earlier studies also suggest that prior experience affects the intention to continue using telemedicine.14,15 In this study, “telemedicine usage” is defined as encompassing both the intention to adopt telemedicine among nonusers and the intention to continue using it among experienced users, reflecting sustained usage. While prior findings are insightful, they primarily rely on sufficiency-based logic, overlooking whether such factors are necessary conditions for the intended outcome. 16 The necessity-based perspective introduces a fundamentally different, noncompensatory view of causality: the absence of a necessary condition can lead to failure even when other favorable conditions are present.17,18
To address this gap, the present study applies necessary condition analysis (NCA), 16 a technique specifically developed to detect conditions whose absence constrains outcomes. By complementing sufficiency-based approaches, NCA offers a more stringent lens for causal inference. This is particularly valuable for policy design: By identifying prerequisites, it supports targeted interventions in healthcare systems with scarce resources.7,19 To systematically examine the necessary conditions, it is crucial to capture service-specific features such as safety, convenience, and cost, 20 which are often overlooked by general technology frameworks. Accordingly, as a key contribution, this study develops a novel instrument specifically tailored to telemedicine, ensuring enhanced validity for NCA and providing a more context-sensitive understanding of barriers and enablers.
Given the divergent development paths of telemedicine markets worldwide, the necessary conditions for telemedicine usage are likely to differ. Japan and China provide a particularly relevant comparison, as they represent distinct stages of market maturity and penetration,
21
with China exhibiting a substantially higher level of both. Against this background, the present study aims to identify the necessary conditions shaping telemedicine usage, focusing on Japan and China. From a comparative perspective, the study addresses the following research questions:
What are the similarities and differences in public perceptions of telemedicine between Japan and China? What necessary conditions shape telemedicine usage across countries and population subgroups, and how do these conditions vary across constraint patterns? Do the necessary conditions for sustained usage remain consistent over time?
Methods
QUESTIONNAIRE DEVELOPMENT
To develop the questionnaire, we conducted a comprehensive literature review to identify key constructs shaping telemedicine usage. The instrument was developed with reference to established dimensions and their corresponding items that have been validated in multiple empirical studies. These included performance expectancy and perceived usefulness,2,22,23 effort expectancy and ease of use,2,22,24 social influence,24,25 facilitating conditions,2,26 security and privacy concerns,25,27,28 resistance to change, 29 accessibility, 25 and intention to use telemedicine. 2 For respondents with prior telemedicine experience, additional items measuring satisfaction were included. 25
The initial questionnaire, which was written in English, was translated into Japanese and Chinese through a process of translation and back-translation by native speakers. During this process, special attention was given to the clarity of technical terms to ensure accessibility for respondents, regardless of their prior experience. We also incorporated illustrative scenarios and simplified phrasing to minimize cognitive burden and ambiguity, ensuring that the questionnaire remained understandable even for those without prior telemedicine experience. A pretest was conducted both in Japan and China prior to the formal survey, involving approximately 20 respondents from each country. Participants provided feedback on question clarity, ease of understanding, and cultural appropriateness. Based on this feedback, several adjustments were made to better reflect telemedicine usage in local healthcare contexts. These revisions improved the overall validity and usability of the questionnaire across the two national settings.
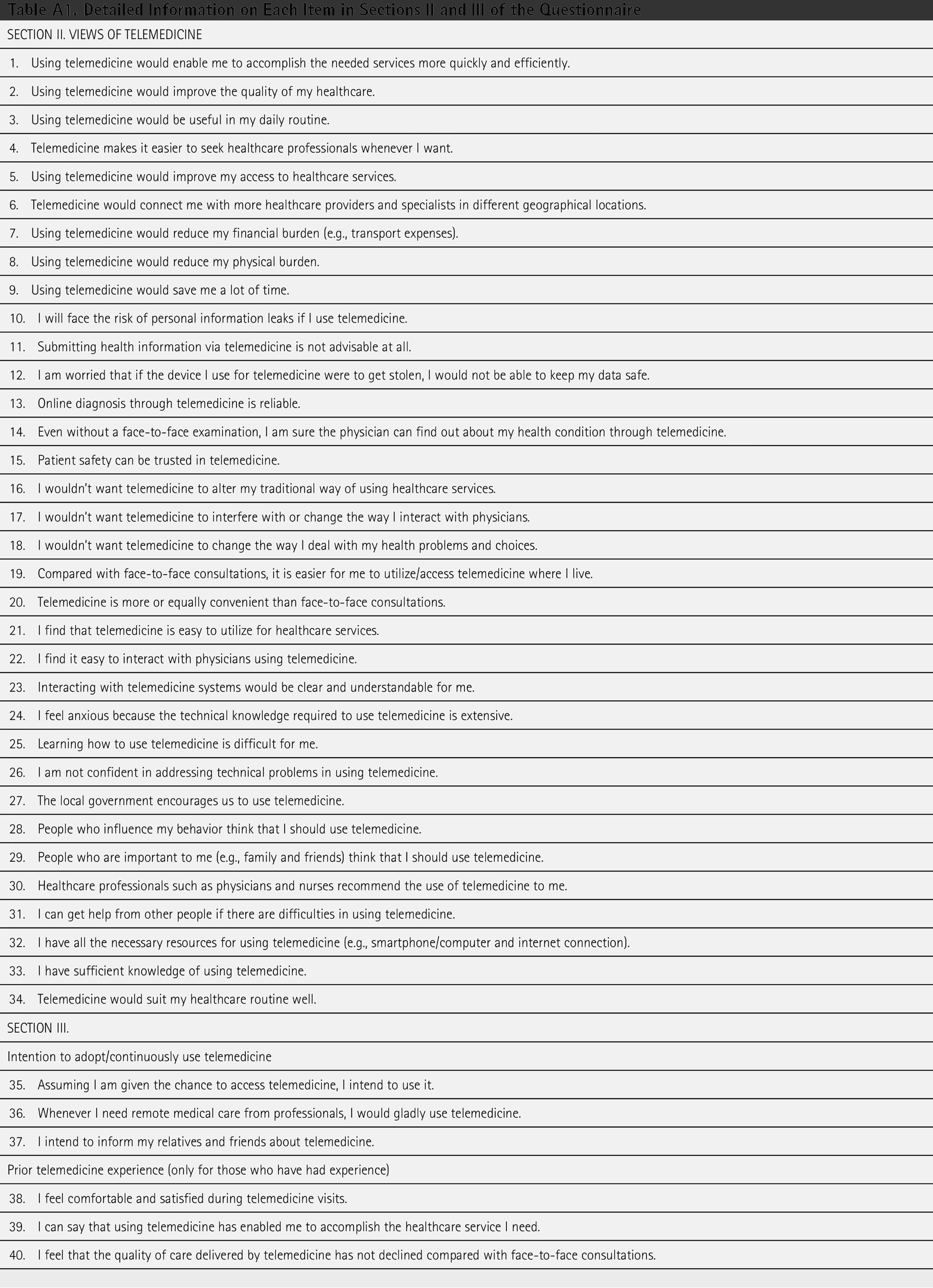
The final version of the questionnaire was divided into three sections. The first section collected demographic data. Age, gender, and residence were included, as they may influence technology acceptance and access conditions.30,31 Chronic disease status and visit frequency reflect healthcare needs, while prior telemedicine experience may shape users’ intention for future use.32,33 These variables were selected to capture differences in how people perceive and use telemedicine. The second section, which included 34 items, sought to gauge participants’ attitudes toward various aspects of telemedicine. Participants rated their agreement on a Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). The third section included six items, of which the initial three assessed participants’ intention to use telemedicine. The remaining three items targeted those with prior telemedicine experience and enquired about their usage experience. This section also employed a Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). Full details of each question in the second and third sections are provided in Appendix A.
SAMPLING AND DATA COLLECTION
The survey targeted the public in Japan and China, employing sampling strategies adapted to each national context. In Japan, during the initial study period, 798 responses were collected between December 2022 and March 2023, including 329 obtained via flyers distributed on university campuses and 469 through an online crowdsourcing platform (Lancers). To ensure data quality, timing checks, the long string index, and three attention-check items were applied. Specifically, for the Lancers sample, only users with a task approval rate exceeding 95% were included to ensure high-quality responses. After data screening, 787 valid Japanese responses were retained. In China, 1,444 responses were collected in May 2023 via a commercial survey platform (Wenjuanxing). Applying the same quality control procedures resulted in 840 valid responses.
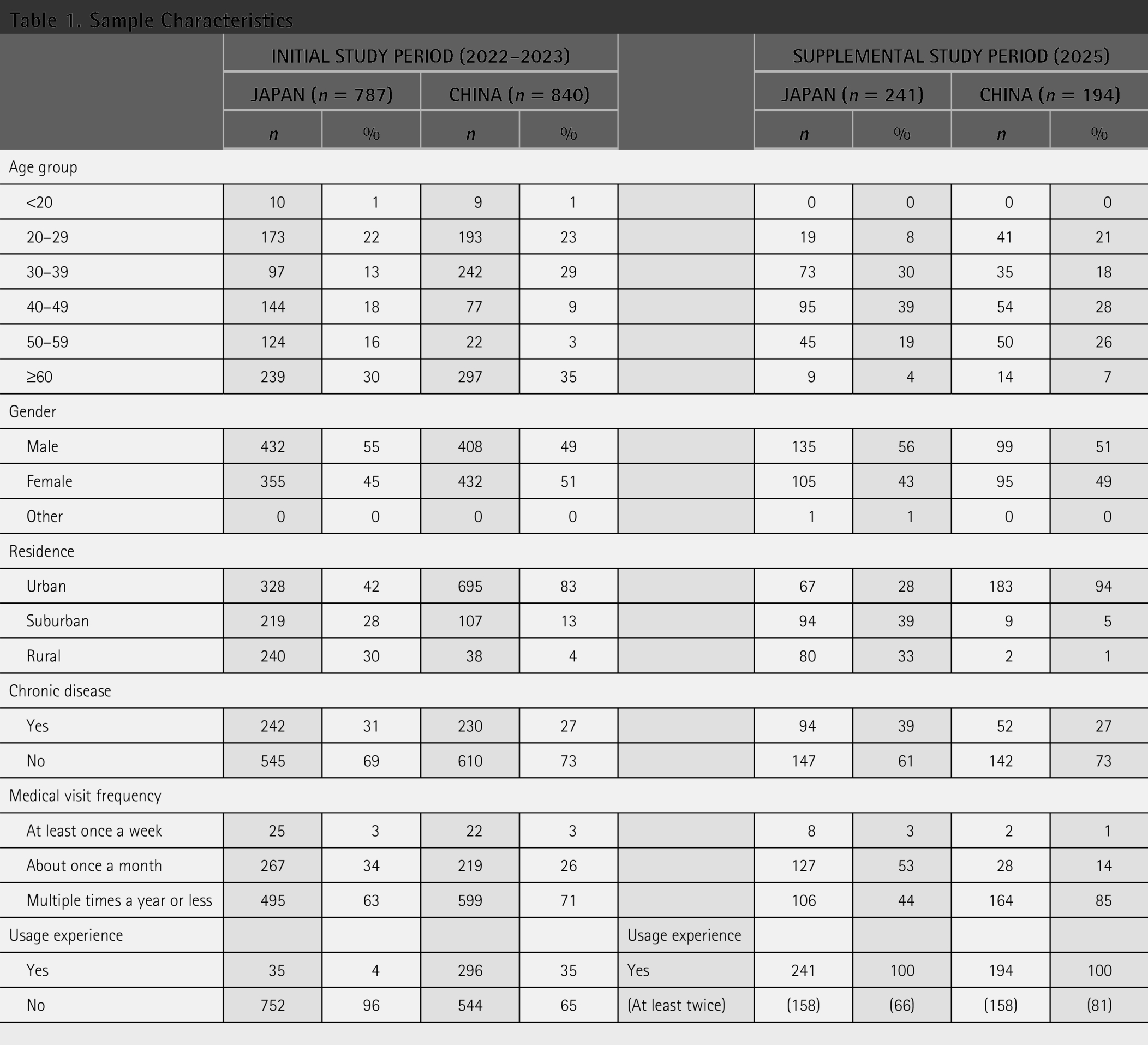
To examine the temporal consistency of the necessary conditions for sustained usage, a supplemental survey was conducted between November and December 2025, targeting experienced telemedicine users. In Japan, 257 responses were collected through Lancers, with 241 retained following data cleaning. In China, 299 responses were obtained via Wenjuanxing, resulting in 194 valid cases. Detailed sample characteristics are presented in Table 1. Ethical approval was granted by the Human Subject Research Ethics Review Committee of Tokyo Institute of Technology (now Institute of Science Tokyo) (Nos. 2022271, 2022416). Informed consent was obtained from all participants. Participation was voluntary and anonymous, and participants were free to withdraw at any stage.
Sample Characteristics
STATISTICAL ANALYSIS
The analyses were conducted primarily on the initial survey datasets. To extract factors influencing the intention to use telemedicine, we first performed exploratory factor analysis using maximum likelihood estimation with Promax rotation on the Japanese responses. Cronbach’s alpha was used to assess internal reliability. This was followed by confirmatory factor analysis to validate the factor structure across the Japanese and Chinese samples. Between-group comparisons of perceptions were performed using the Mann–Whitney U test, as normality was rejected by the Kolmogorov–Smirnov test.
To identify necessary conditions for telemedicine usage, NCA was applied. NCA is a technique designed to assess whether certain conditions must reach a minimum level for an outcome to occur by detecting empty spaces in scatter plots. In this study, ceiling lines were computed using the ceiling envelopment-free disposal hull (CE-FDH) method, which generates a stepwise, nondecreasing line along the upper-left boundary of the data. This method is recommended for its flexibility and suitability for various data types. 34 The effect size (d) was then calculated to quantify the proportion of the ceiling zone relative to the total area. According to established guidelines, a condition was deemed necessary if d exceeded 0.1, and the result was statistically significant (p < 0.01). 34 Subsequently, bottleneck analysis was conducted to examine how the minimum necessary levels of each condition varied across all population subgroups in Japan and China. Hierarchical clustering analysis was subsequently performed to identify representative patterns. Specifically, an agglomerative hierarchical clustering method using Ward’s linkage was applied to the bottleneck data separately for each country. Based on the dendrogram, Silhouette score, and Calinski–Harabasz index, three clusters were selected for each country, with one representative subgroup from each cluster used for the final visualization of bottleneck factor trends.
For the supplemental datasets, following confirmation of reliability and validity, NCA (CE-FDH method) was similarly applied. The results were compared with those of experienced users from the initial study period to examine the temporal consistency of the necessary conditions for sustained usage. All statistical analyses were performed using IBM SPSS Statistics 28, AMOS 28, Python, and RStudio.
Results
FACTOR STRUCTURE, RELIABILITY, AND VALIDITY
As explained in the Statistical Analysis subsection, the analyses were conducted primarily on the initial survey datasets. Exploratory factor analysis (maximum likelihood, Promax rotation) was applied to the Japanese sample. The scree plot and pattern matrix supported an eight-factor solution, explaining 63.20% of the variance. In this structure, several items set originally specified as separate constructs (e.g., safety and reliability) exhibited high correlations and coherent loadings and were therefore merged to reflect the empirically supported structure. The eight factors were named as follows: cost and accessibility, social influence, safety and reliability, adaptive readiness, technology confidence, perceived data security, facilitating conditions, and perceived usefulness. Reverse-worded items were recoded as positive dimensions for consistency. Details of component items and factor loadings are presented in Table 2.
Factors Extracted by the Exploratory Factor Analysis Applied to the Initial Japanese Dataset (n = 787)
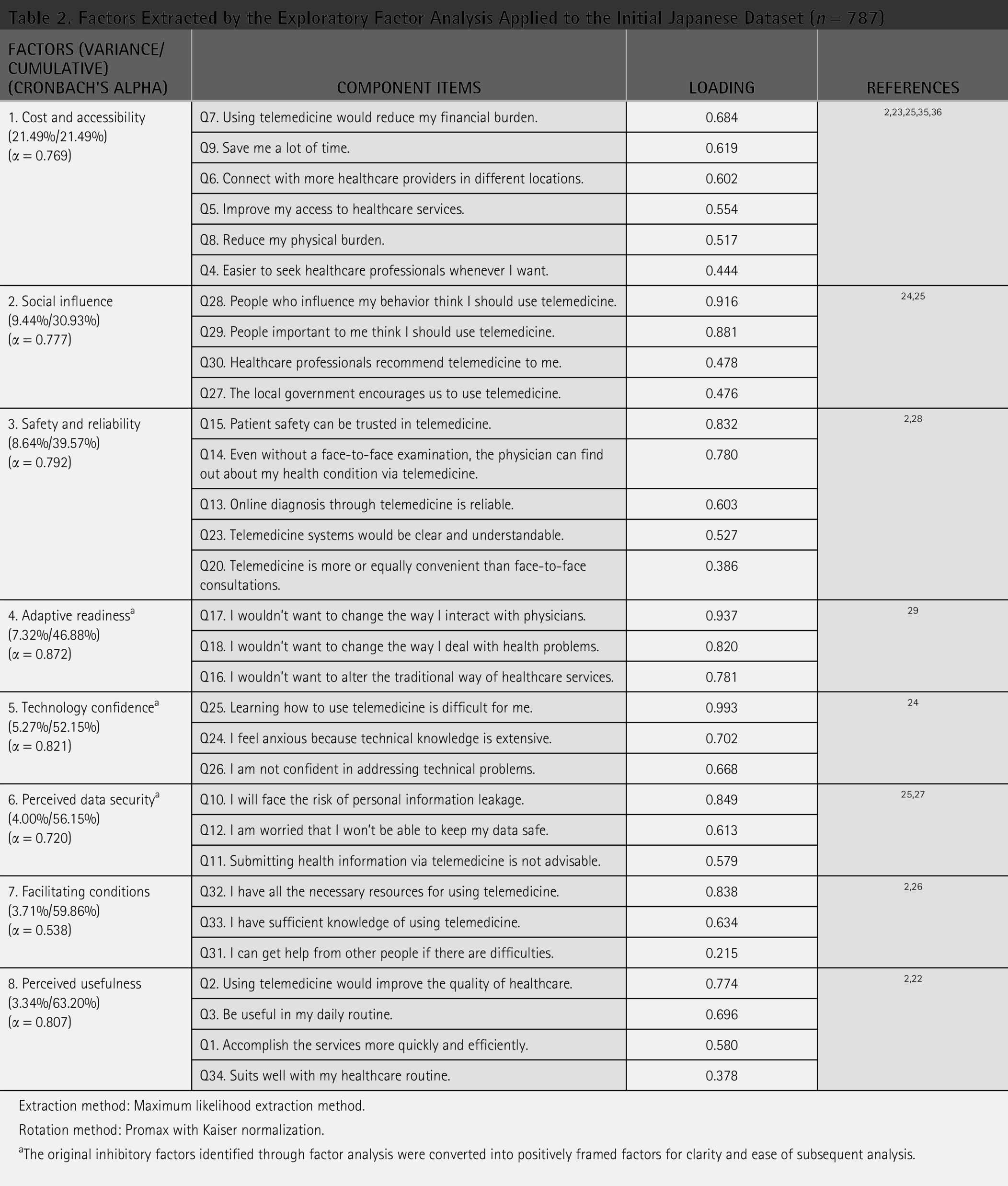
Extraction method: Maximum likelihood extraction method.
Rotation method: Promax with Kaiser normalization.
The original inhibitory factors identified through factor analysis were converted into positively framed factors for clarity and ease of subsequent analysis.
Confirmatory factor analysis indicated acceptable model fit in both the Japanese [Comparative Fit Index (CFI) = 0.887, the ratio of chi-square to degrees of freedom (CMIN/DF) = 3.500, and Root Mean Square Error of Approximation (RMSEA) = 0.056] and Chinese samples (CFI = 0.908, CMIN/DF = 2.843, and RMSEA = 0.047). Internal reliability was good or acceptable for seven factors (αJapan = 0.720–0.872; αChina = 0.607–0.844), 37 although facilitating conditions exhibited slightly lower reliability (αJapan = 0.538; αChina = 0.545). Together with consistency with prior literature,5,38,39 these results support the construct validity of the eight-factor structure.
COMPARISONS OF TELEMEDICINE PERCEPTIONS
Fig. 1 compares perceptions of telemedicine factors and usage intention between Japanese and Chinese respondents. Overall, Chinese participants reported significantly more favorable evaluations across almost all factors (p < 0.001). Apart from adaptive readiness, the remaining seven factors exhibited higher median scores and similar or narrower interquartile ranges (IQRs), indicating stronger and more consistent positive perceptions among Chinese respondents. Notably, social influence showed no overlap in IQRs between the two countries, revealing a clear perception gap in favor of China. In contrast, Japanese respondents scored higher only on adaptive readiness (p < 0.001), indicating greater openness to adopting new healthcare practices despite an otherwise more cautious overall stance. Usage intention was likewise higher and concentrated among Chinese respondents, reinforcing the stronger tendency for telemedicine usage in the Chinese context.
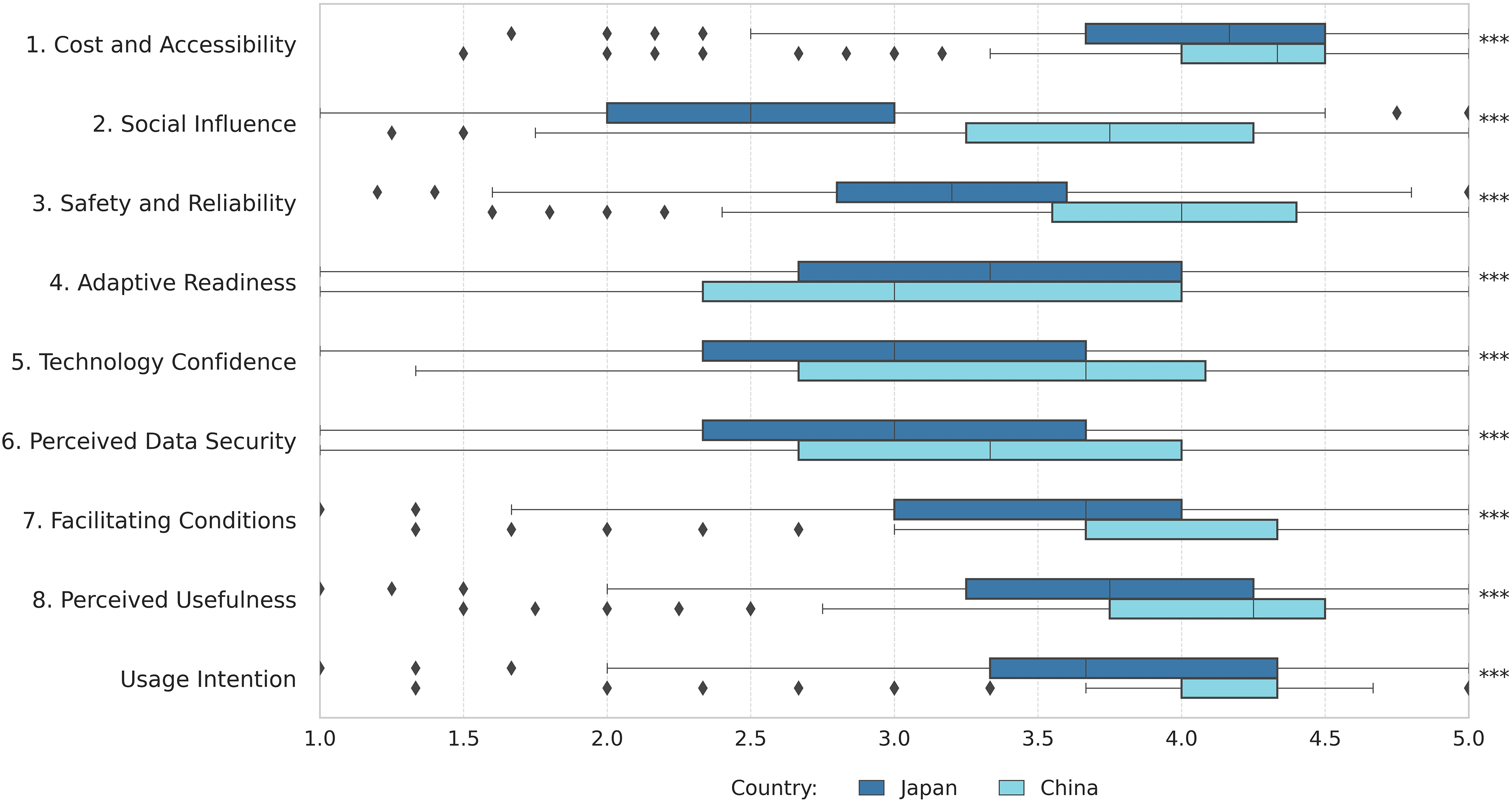
Perception comparisons of factors and usage intention between Japanese and Chinese (initial survey datasets). Box plots show perception scores for each factor and usage intention in Japan and China. Boxes represent the interquartile range (IQR), vertical lines within boxes indicate medians, and whiskers extend to data within 1.5 × IQR. Dots represent outliers. p indicates significant differences between countries based on Mann–Whitney U tests (***p < 0.001).
NECESSARY CONDITIONS FOR TELEMEDICINE USAGE INTENTION
Effect sizes of necessary conditions across population subgroups
Fig. 2 presents a heatmap of NCA effect sizes, illustrating the necessity strength of each factor across population subgroups in Japan and China. At the aggregate level, Japanese participants identified facilitating conditions (d = 0.12–0.31) and perceived usefulness (d = 0.15–0.29) as necessary conditions across most subgroups (p < 0.01), with effect sizes mainly in the medium range (medium: 0.1 ≤ d < 0.3; large: 0.3 ≤ d < 0.5). 16 In contrast, Chinese participants demonstrated a broader necessity profile, with facilitating conditions (d = 0.15–0.43), cost and accessibility (d = 0.17–0.35), social influence (d = 0.11–0.26), and safety and reliability (d = 0.17–0.29) identified as necessary by most subgroups (p < 0.01).
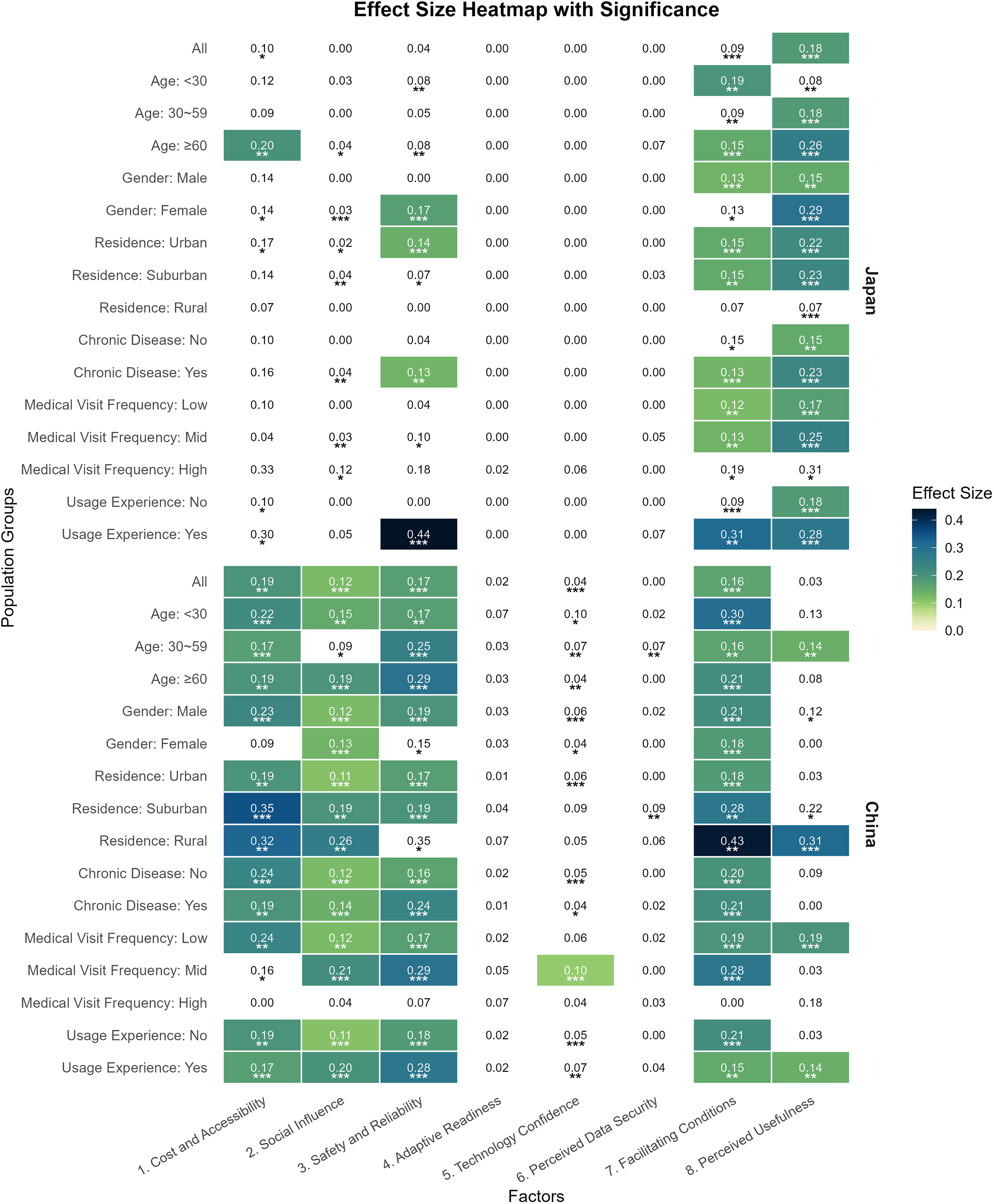
Heatmap of effect sizes and statistical significance from necessary condition analysis across population subgroups in Japan and China (initial survey datasets). The heatmap illustrates the effect sizes for each variable across demographic subgroups in Japan and China. Each cell displays the estimated effect size from the necessary condition analysis (NCA), with darker shades indicating stronger effects. Only results that are both statistically significant (**p < 0.01, ***p < 0.001) and have effect sizes higher than 0.1 are color-coded; nonsignificant or negligible effects are left blank. Subgroups are defined by age, gender, residence type, chronic disease status, medical visit frequency, and prior usage experience.
Subgroup patterns diverged further. In both countries, experienced users regarded safety and reliability as the most critical necessary condition (Japan: d = 0.44; China: d = 0.28; p < 0.001), reflecting heightened sensitivity to risk and quality following usage. No necessary conditions were identified among Japanese rural residents, whereas Chinese rural residents exhibited strong necessity requirements for cost and accessibility (d = 0.32; p < 0.001), facilitating conditions (d = 0.43; p < 0.01), and perceived usefulness (d = 0.31; p < 0.001).
Bottleneck trends across hierarchically clustered representative subgroups
To facilitate interpretation, representative population subgroups were extracted from the bottleneck data using hierarchical clustering. Three clusters were derived per country, yielding six representative subgroups for further analysis. Fig. 3 presents the clustering results and the corresponding bottleneck trends for the six subgroups and the overall population, illustrating how necessity levels change with increasing telemedicine usage intention.
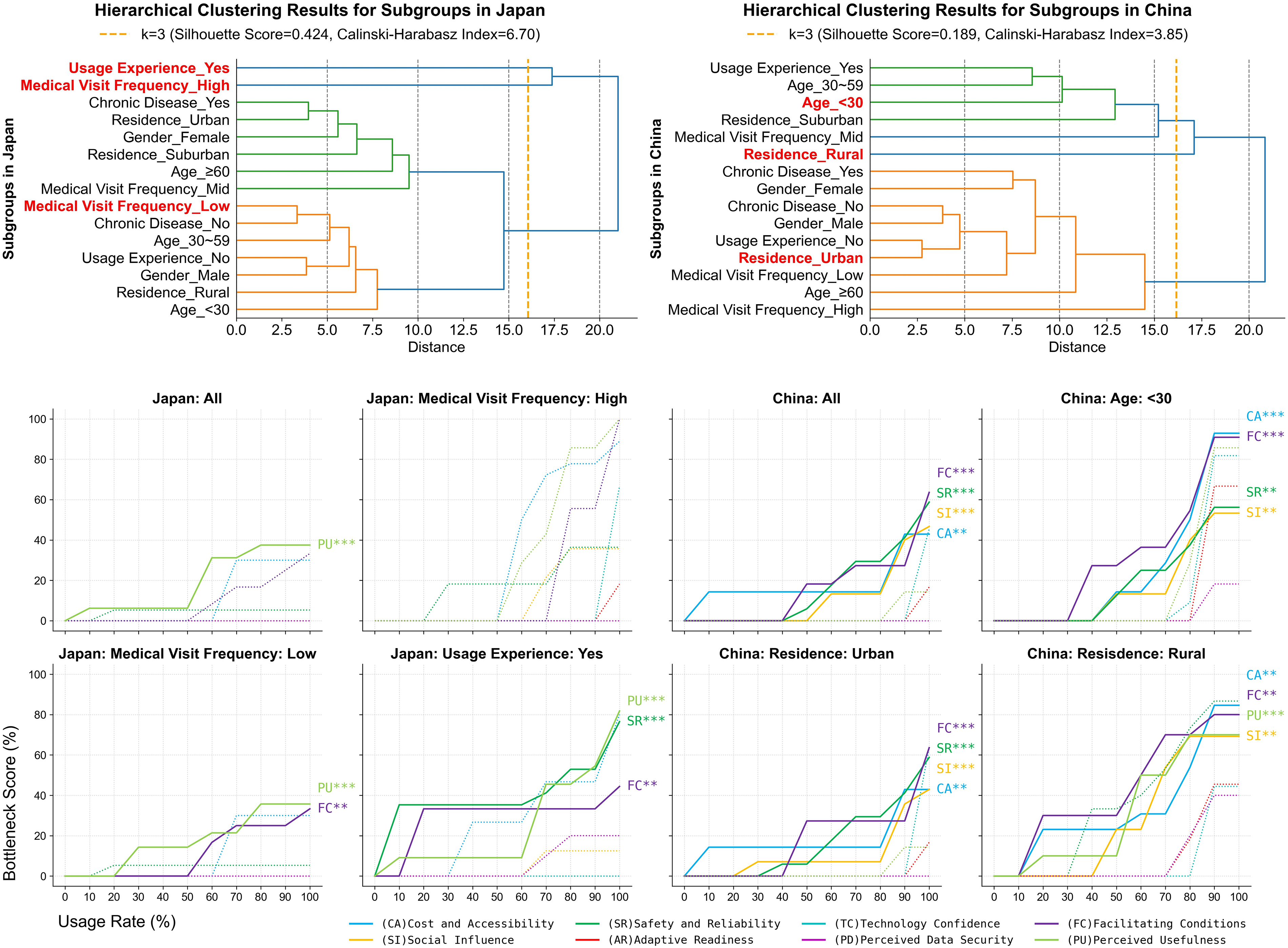
Hierarchical clustering results (top) and bottleneck factor trends for all populations and six representative population groups under varying levels of telemedicine usage intention (bottom) in Japan and China (initial survey datasets). The upper panel shows the hierarchical clustering results used to define representative population subgroups, while the lower panel presents bottleneck factor trends for these six representative groups and all populations in both countries. Solid lines indicate factors that are both statistically significant (**p < 0.01, ***p < 0.001) and have effect sizes above 0.1, whereas dotted lines indicate nonsignificant or negligible effects. Labels on the right highlight the necessary factors.
Overall, bottleneck trajectories were broadly similar across countries. As represented by low-frequency medical visitors in Japan and urban residents in China, most subgroups exhibited a gradual rise in bottleneck levels as usage intention increased, reaching a moderate necessity level (∼50%). These trajectories are closely aligned with the overall population trends, although Chinese subgroups displayed steeper and higher increases.
Two distinctive patterns were also observed. One pattern, represented by younger Chinese participants, showed low initial bottlenecks followed by a sharp increase, ultimately reaching high necessity levels, indicating stronger expectations for telemedicine usage. The most atypical trajectory, observed among experienced users in Japan and rural residents in China, exhibited early-emerging bottlenecks that increased steadily to high necessity levels, indicating structural constraints in the early stages of telemedicine usage.
Temporal consistency of necessary conditions for sustained telemedicine usage
For the supplemental datasets, the eight-factor structure demonstrated satisfactory internal reliability (αJapan = 0.706–0.907; αChina = 0.706–0.917). Confirmatory factor analysis further indicated acceptable model fit for both the Japanese (CFI = 0.887, CMIN/DF = 1.844, RMSEA = 0.059) and Chinese samples (CFI = 0.870, CMIN/DF = 2.205, RMSEA = 0.079). NCA was subsequently performed, and the results were compared with the initial findings, as presented in Table 3.
Comparison of Necessary Conditions between Initial and Supplemental Study Periods
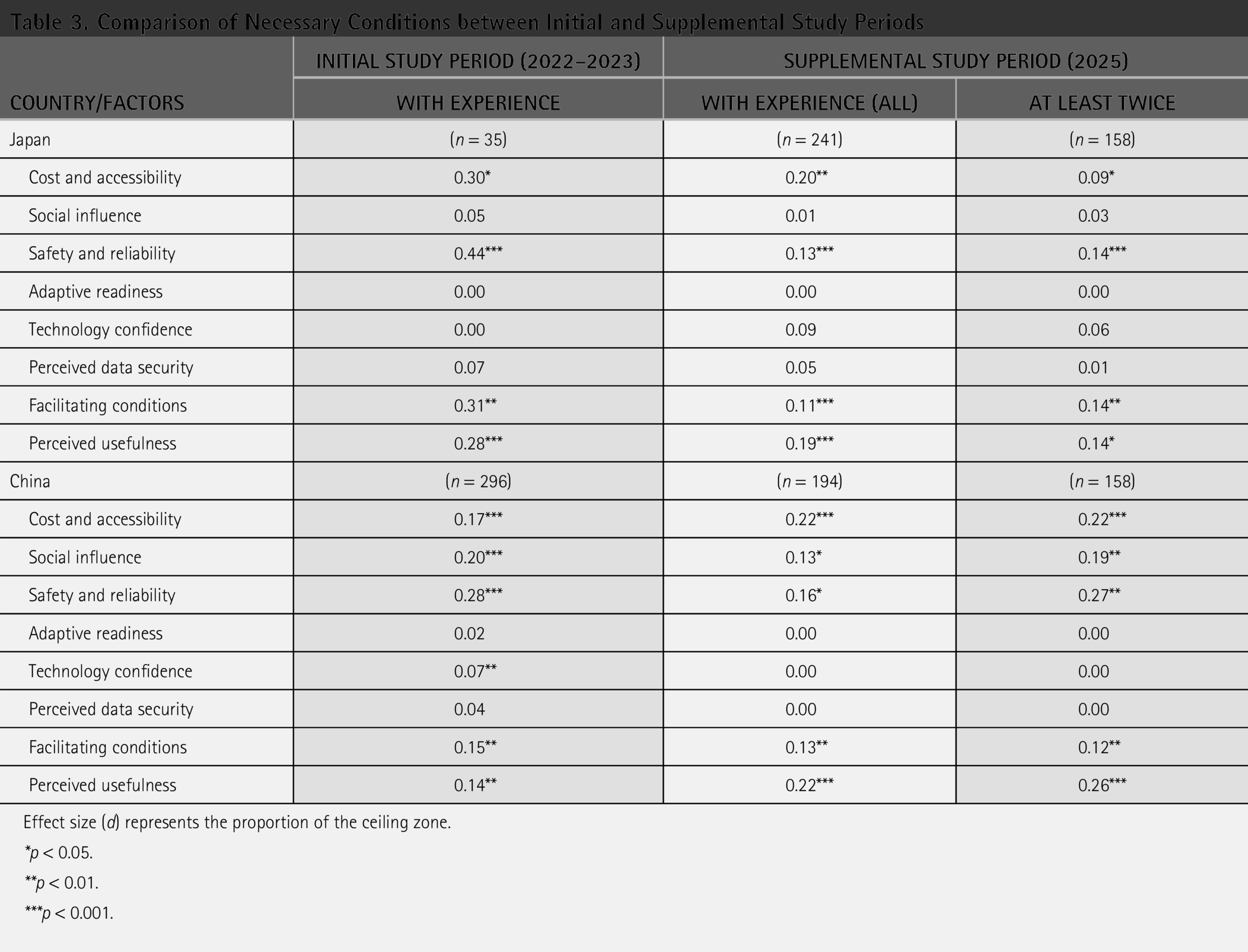
Effect size (d) represents the proportion of the ceiling zone.
*p < 0.05.
**p < 0.01.
***p < 0.001.
In both countries, the supplemental analyses confirmed the initial findings on necessary conditions for sustained telemedicine usage. In Japan, cost and accessibility, safety and reliability, facilitating conditions, and perceived usefulness remained necessary conditions, although effect sizes for safety and reliability and facilitating conditions declined from large to medium. In China, cost and accessibility, facilitating conditions, and perceived usefulness remained stable prerequisites, while social influence and safety and reliability continued to show necessity with slight fluctuations. Across both countries, results for users with at least two telemedicine experiences closely matched those of the broader experienced sample, with safety and reliability exhibiting the largest effect sizes, consistent with the initial findings. Detailed bottleneck trends are reported in Appendix B.
Discussion
CONTRASTING PERCEIVED SOCIAL INFLUENCE BETWEEN JAPAN AND CHINA
Among all factors, social influence showed the most pronounced cross-national difference. In China, government policies promoting telemedicine have been reinforced by consistent recommendations from general practitioners, 40 creating an environment where patients widely perceive telemedicine as an endorsed option. 41 In contrast, Japan’s abundant healthcare resources and a lack of policy urgency have slowed its integration. 42 Medical institutions are less inclined to recommend telemedicine, 43 resulting in weaker perceived social influence and more cautious patient attitudes.
NATIONAL AND SUBGROUP-LEVEL DIFFERENCES IN NECESSARY CONDITIONS
This study revealed clear cross-national differences reflecting each country’s institutional contexts. Chinese respondents perceived a wide range of prerequisites, likely stemming from the ongoing promotion of telemedicine against a backdrop of uneven infrastructure, which heightens sensitivity to multiple conditions.7,19 In contrast, Japanese participants, benefiting from long-standing healthcare resource stability, focused mainly on perceived usefulness. 44 Subgroup analysis further highlighted disparities, with Chinese rural residents emphasizing cost and accessibility, underscoring persistent urban–rural inequalities.45,46
Crucially, safety and reliability emerged as the nonnegotiable prerequisite for sustained usage among experienced users. As a medical technology, telemedicine must meet sufficient safety standards to sustain trust,12,47 a finding consistently observed in two survey waves.
UNDERSTANDING BOTTLENECK LEVEL TRAJECTORIES ACROSS REPRESENTATIVE SUBGROUPS
Three distinct trajectories emerged, reflecting differences in preparedness, expectations, and resource access. Gradual-bottleneck users represent the mainstream type. Observed across many subgroups, these users begin with few concerns and only recognize deficiencies after deeper engagement. This pattern was also supported by findings from Indonesia, where such issues emerged as usage deepened despite initial user satisfaction, 48 suggesting that stepwise improvements in service functionality can sustain use.
High-bottleneck users, typified by Chinese youth, exhibited a sharp “demand surge” at mid-to-high usage levels. Once intention reaches a certain level, their expectations regarding cost, accessibility, and facilitating conditions increase rapidly. These users often hold high service expectations, and if their concerns are not addressed promptly, there is a risk of negative experiences or withdrawal from usage. 49 The uptake of telemedicine among this group serves as a benchmark test for system capabilities.
Early-bottleneck users, including Japanese experienced users and Chinese rural residents, display constraints from the outset. Their dependence on enabling conditions points to structural barriers in trust and accessibility. 50 Average-based strategies risk overlooking such groups, 51 making early interventions critical for ensuring equitable access. 52
IMPLICATIONS
This study makes distinct theoretical contributions. First, by applying NCA with a tailored telemedicine-specific instrument, it offers a noncompensatory perspective that detects prerequisites often overlooked by generic adoption measures. Second, it introduces a typology of three bottleneck trajectories: gradual-, high-, and early-bottleneck users. This typology goes beyond static classification to explain when and how usage barriers emerge, providing a dynamic perspective on user heterogeneity.
The findings also offer guidance for more adaptive strategies. For mainstream users, gradual improvements in functionality can encourage continued use. For demand-sensitive groups such as young Chinese users, early provision of affordable pricing and supporting infrastructure, including reliable payment systems, can prevent disengagement and foster system innovation. For structurally disadvantaged groups, such as rural Chinese, proactive interventions targeting trust and tailored support are essential. Finally, to ensure sustained usage among experienced users, safety and reliability should be prioritized.
Limitations
This study has five main limitations. First, Cronbach’s alpha for facilitating conditions was occasionally low; future studies should further verify its internal reliability across different contexts. Second, the use of online surveys may have favored digitally literate respondents. While high internet penetration in Japan supports sample representativeness, 53 digital disparities in China, particularly between urban and rural areas and across age cohorts, 54 limit generalizability to digitally marginalized populations; mixed-mode sampling approaches are therefore recommended. Third, this study assessed general telemedicine usage intention, without distinguishing among specific application contexts (e.g., chronic disease management); future research should adopt context-specific designs. Fourth, although large-scale sampling helped mitigate extreme bias, it did not ensure full representativeness of national populations. However, the present study prioritized identifying constraint conditions, and analyses across two survey waves confirmed the reliability and validity of the findings. Accordingly, the findings are considered robust and consistent but should still be interpreted cautiously, especially for groups with limited digital access. Finally, socioeconomic and educational factors were not incorporated into the research design and should be included in future work.
Conclusions
This study identified the necessary conditions for telemedicine usage in Japan and China using a self-developed questionnaire and NCA. The results revealed an eight-factor structure and clear cross-national contrasts: Japanese respondents mainly emphasized perceived usefulness and facilitating conditions, whereas Chinese respondents required a broader set of prerequisites. Subgroup analyses showed that safety and reliability were nonnegotiable for experienced users in both countries. The study also identified three bottleneck trajectories: gradual-bottleneck users with progressive constraints, high-bottleneck users with sudden demand surges, and early-bottleneck users with persistent initial barriers. Crucially, results from the supplemental samples further confirmed the reliability and validity of the eight-factor structure, as well as for the temporal consistency of the necessary conditions for sustained usage.
Theoretically, this study advances telemedicine research by developing a telemedicine-specific instrument, extending the application of NCA, and proposing a typology of bottleneck trajectories. Practically, the findings support differentiated strategies, including incremental support for mainstream users, early engagement with high-expectation groups, and proactive interventions for structurally disadvantaged populations. Overall, the combined use of the developed instrument and NCA provides a transferable approach to supporting cross-national comparisons and informing the design of equitable and scalable telemedicine policies across healthcare systems.
Authors’ Contributions
H.W.: Conceptualization, data curation, formal analysis, investigation, visualization, methodology, and writing—original draft. K.S.: Conceptualization, data curation, investigation, and methodology. X.G.: Conceptualization, resources, supervision, funding acquisition, validation, methodology, and writing—review and editing.
Footnotes
Acknowledgments
The authors are grateful to those who participated in our surveys. The authors would also like to thank Xinyi Chang, PhD candidate at the Institute of Science Tokyo, for her support in the translation and back translation of the questionnaire.
Funding Information
This work was partly supported by the Japan Society for the Promotion of Science (grant number 24K07926). The funding body had no role in the study design, data collection, analysis, interpretation, or publication of the results.
Ethical Approval and Informed Consent Statement
Ethical approval was granted by the University’s Ethics Committee (Nos. 2022271, 2022416). Informed consent was obtained from all participants. Participation was voluntary and anonymous, and participants were free to withdraw at any stage.
Data Availability Statement
Data will be made available upon reasonable request.
Disclosure Statement
The authors declare no competing interests in this work.
Appendix A
Detailed Information on Each Item in Sections II and III of the Questionnaire
| SECTION II. VIEWS OF TELEMEDICINE |
|
Using telemedicine would enable me to accomplish the needed services more quickly and efficiently. |
|
Using telemedicine would improve the quality of my healthcare. |
|
Using telemedicine would be useful in my daily routine. |
|
Telemedicine makes it easier to seek healthcare professionals whenever I want. |
|
Using telemedicine would improve my access to healthcare services. |
|
Telemedicine would connect me with more healthcare providers and specialists in different geographical locations. |
|
Using telemedicine would reduce my financial burden (e.g., transport expenses). |
|
Using telemedicine would reduce my physical burden. |
|
Using telemedicine would save me a lot of time. |
|
I will face the risk of personal information leaks if I use telemedicine. |
|
Submitting health information via telemedicine is not advisable at all. |
|
I am worried that if the device I use for telemedicine were to get stolen, I would not be able to keep my data safe. |
|
Online diagnosis through telemedicine is reliable. |
|
Even without a face-to-face examination, I am sure the physician can find out about my health condition through telemedicine. |
|
Patient safety can be trusted in telemedicine. |
|
I wouldn’t want telemedicine to alter my traditional way of using healthcare services. |
|
I wouldn’t want telemedicine to interfere with or change the way I interact with physicians. |
|
I wouldn’t want telemedicine to change the way I deal with my health problems and choices. |
|
Compared with face-to-face consultations, it is easier for me to utilize/access telemedicine where I live. |
|
Telemedicine is more or equally convenient than face-to-face consultations. |
|
I find that telemedicine is easy to utilize for healthcare services. |
|
I find it easy to interact with physicians using telemedicine. |
|
Interacting with telemedicine systems would be clear and understandable for me. |
|
I feel anxious because the technical knowledge required to use telemedicine is extensive. |
|
Learning how to use telemedicine is difficult for me. |
|
I am not confident in addressing technical problems in using telemedicine. |
|
The local government encourages us to use telemedicine. |
|
People who influence my behavior think that I should use telemedicine. |
|
People who are important to me (e.g., family and friends) think that I should use telemedicine. |
|
Healthcare professionals such as physicians and nurses recommend the use of telemedicine to me. |
|
I can get help from other people if there are difficulties in using telemedicine. |
|
I have all the necessary resources for using telemedicine (e.g., smartphone/computer and internet connection). |
|
I have sufficient knowledge of using telemedicine. |
|
Telemedicine would suit my healthcare routine well. |
| SECTION III. |
| Intention to adopt/continuously use telemedicine |
|
Assuming I am given the chance to access telemedicine, I intend to use it. |
|
Whenever I need remote medical care from professionals, I would gladly use telemedicine. |
|
I intend to inform my relatives and friends about telemedicine. |
| Prior telemedicine experience (only for those who have had experience) |
|
I feel comfortable and satisfied during telemedicine visits. |
|
I can say that using telemedicine has enabled me to accomplish the healthcare service I need. |
|
I feel that the quality of care delivered by telemedicine has not declined compared with face-to-face consultations. |