
Abstract
Objective:
Human milk supports optimal health outcomes for infants in the neonatal intensive care unit; however, expressing milk is impacted by separation, stress, and time. We examined the impact of using videoconferencing with one’s infant while expressing milk on the volume, efficiency, human milk macronutrient content, and the milk expression experience.
Methods:
In this randomized controlled crossover trial (NCT03957941), mothers of premature infants expressed milk three times with videoconferencing and three times without. Milk volumes and expression time were self-recorded. Experience was assessed with the Breast Milk Expression Personal Experience (BMEE) subscale. Milk samples were analyzed using the Miris Human Milk Analyzer™. Data were analyzed using a panel data fixed-effects model to estimate within-person mean differences (MDs) between study arms in human milk volume, efficiency, macronutrient content, and BMEE scores.
Results:
A total of 39 women were enrolled in the study, 28 provided milk volume and efficiency data, 26 completed BMEE scores, and 24 provided milk samples. Videoconferencing improved the milk expression experience, with mean BMEE subscale scores higher with videoconferencing (MD 0.10; 95% confidence interval [CI]: 0.02, 0.18; p = 0.01). There was no difference in milk volume (MD −2.5 mL; CI: −11.9, 6.9; p = 0.6) nor efficiency (MD 0.3 mL/min; CI: −0.4, 0.9; p = 0.4).
Conclusions:
Videoconferencing with one’s hospitalized premature infant improves the pumping experience. However, the use of videoconferencing was not associated with significant effects on human milk expression nor efficiency.
Introduction
Human milk feeding is recommended for the vast majority of newborns as there are many immediate and long-term benefits for both lactating persons and their children. 1 For premature infants, receipt of mother’s own milk is associated with better developmental outcomes, 2 lower rates of retinopathy of prematurity, 3 sepsis,3,4 necrotizing enterocolitis, 5 and death. 1 For lactating individuals, not breastfeeding is associated with higher rates of morbidity and mortality, particularly from metabolic syndrome, cardiovascular disease, and breast and ovarian cancers.1,6,7
Improving human milk feeding for premature infants hospitalized in the neonatal intensive care unit (NICU) is complicated. Premature delivery is unexpected and associated with severe risk of morbidity and mortality in the infant and postpartum individual. 8 After the delivery, postpartum patients are often separated from their premature newborn and instructed to express human milk rather than feeding the newborn at the breast. Critically ill premature infants are frequently transferred to a higher level of care, NICUs, which may be a great distance from the home of the family, complicating visitation and breastfeeding at the bedside. Ongoing expression of human milk for a hospitalized infant can be stressful and time-consuming, which can be a barrier to prolonged provision of human milk during the NICU hospitalization.9,10 Expression of human milk and receipt of mother’s own milk improve maternal and infant health outcomes, even when pasteurized donor human milk is available.1,11,12 If expression of human milk were easier, enjoyable, and efficient, human milk feeding rates in the NICU might improve.
Being near or seeing one’s baby while expressing milk increases oxytocin secretion, which can increase milk volumes expressed and improve the efficiency of human milk expression.13,14 Video observation platforms have been widely implemented in many hospitals to connect families with their hospitalized child and care team, but there is a paucity of research on how these technologies impact human milk feeding. 15 Use of telemedicine has been described to improve certain health outcomes and access to care, 16 especially for patients in rural areas far from their clinical providers. 17
We previously published a study that explored how access to bedside videoconferencing impacted the NICU admission for families. 18 We found that hospitalized NICU patients and their families who had access to videoconferencing technology were more likely to be providing expressed human milk at NICU discharge. However, it was unclear if access to versus active use of videoconferencing while expressing milk impacted human milk feeding. In this randomized controlled crossover trial, we sought to test the impact of seeing one’s infant through videoconferencing on the volume or efficiency of human milk expression, the macronutrient content of expressed milk, and the breast milk expression experience. We hypothesized that use of videoconferencing to see one’s baby while expressing human milk would increase milk volumes expressed, shorten the time needed to express milk, improve the macronutrient content of the milk, and improve the experience of expressing milk.
Methods
Results of this trial are reported according to the Consolidated Standards of Reporting Trials (CONSORT) guidelines for randomized crossover trials, 19 see the CONSORT checklist (Supplementary Data).
SETTING
This study and recruitment took place in a large academic tertiary referral hospital with a 49-bed level 4 NICU in Northern California, with over 500 admissions per year, that receives patients from 33 counties from Central California to the Oregon and Nevada borders. The videoconferencing platform in the hospital is a Health Insurance Portability and Accountability Act (HIPAA)-compliant one-way videoconferencing technology developed by the study site that is available to all beds in the NICU. Families can connect to the platform via a web-based, password-protected portal 24 h/day to see their infant. Audio is not available due to privacy concerns. Enrollment for the study began in September 2019 and continued through May 2022. Milk expression and the collection of milk samples occurred outside of the NICU in a personal private setting (e.g., home, workplace, or at the Ronald McDonald house adjacent to the hospital). Data were self-reported by participants on paper data collection forms and collected by the study coordinator.
TRIAL DESIGN
This study was a randomized controlled crossover trial (ClinicalTrials.gov identifier: NCT03957941, registered May 13, 2019) where we compared how the use and nonuse of videoconferencing while expressing milk when separated from one’s infant impacted the following: (1) milk volume; (2) efficiency or total time of the milk expressing session; (3) macronutrient content of the milk, including fat, protein, carbohydrates, and energy (kilocalories); and (4) the parental breast pumping experience. We have reported separately on the qualitative results from this study. 20 Participants were randomized to either intervention or control on the first day, and then vice versa on the second day of data collection. The intervention arm used videoconferencing to see their hospitalized infant while expressing milk, and control was to express milk without videoconferencing. Participants were provided with written and pictorial instructions on how to use videoconferencing technology, when to express milk, documenting the volume of milk, and time to express milk. Participants collected data for three separate milk expression sessions in one intervention and one control day (total of six data collection points). All participants to exclude the first morning milk expression session, as volume is highest at that time and expression volumes were expected to be more consistent throughout the rest of the day. 14 We instructed participants to complete the intervention or control days with their second, third, and fourth milk expression sessions of the day. Participants were instructed to write down the start and stop times of their milk expression sessions.
For the fourth milk expression of the day, participants collected a sample of expressed milk. Participants were instructed to take their bottle of freshly pumped milk and swirl to incorporate the fat layer and then use a syringe to collect 5 mL from the middle of the bottle that was placed in an Eppendorf tube. The sample was frozen and then carried into the NICU where it was stored at −40°C until analysis was performed. The macronutrient analysis was done using the Miris Human Milk Analyzer (HMA)TM. Participants were instructed to separate their intervention and control days by at least 24 h for washout of the effect of videoconferencing. There were no changes to the study protocol during the study period. Following completion of each milk expression session and survey, participants were given an electronic $10 gift card.
DATA COLLECTION INSTRUMENTS
Macronutrient analysis of human milk was completed with the Miris HMA midinfrared transmission spectroscopy. Individual samples of 5 mL of human milk were collected from control and intervention milk expressing days. The 5ml volume was chosen to ensure that each milk sample could be analyzed in triplicate, to improve the precision of measured macronutrient and energy content.21,22
The breast milk expression experience (BMEE) survey was administered at the end of the intervention and control milk expressing sessions. The BMEE is a validated scale to measure the milk expression experience for lactating parents of term infants. This scale assesses three domains, including experiences of learning how to express milk, experiences of social support for expressing milk, and the overall personal experience of milk expression. 23 We administered questions from the BMEE subscale about the personal experience.
OUTCOMES
We hypothesized that use of videoconferencing while expressing milk would lead to a significantly higher volume of breast milk pumped, increased pumping efficiency, higher caloric density of expressed breast milk, and improved experience. The primary outcome of this study was the mean volume of breast milk expressed per pumping session. Secondary outcomes included pumping efficiency, human milk macronutrients, and the milk expression experience. Milk expression efficiency was defined as the volume of breast milk expressed divided by the minutes of the milk expression session. Human milk macronutrients included fat, protein, carbohydrate, and energy (kilocalories) contents and were measured from the milk collected during the fourth milk expression session on both intervention and control days. No changes to study outcomes occurred after the trial commenced.
DATA ANALYSIS
We aimed to enroll at least 40 mothers of preterm infants with a 1:1 allocation ratio. For 30 participants, six pumping sessions per participant provided 80% power, with alpha of 0.05, to detect a 4 mL mean difference (MD) in the volume of milk expressed while using videoconferencing versus not using (primary outcome). This volume was selected as an additional 4 mL of milk per pumping session throughout a 24-h period would elicit an additional 32 mL of milk per day of mother’s own milk for the hospitalized premature infant, which was deemed by the study team to be clinically relevant based on work previously completed by Acuña-Muga et al. 14
Demographic characteristics were analyzed using descriptive statistics to determine means and standard deviations or medians and interquartile ranges as appropriate given the distributions of the data. Adjusted MDs in study outcomes, our preferred effect size estimate, from our two-period crossover design were estimated with 95% confidence intervals (CIs) using a fixed-effects models for panel data, to permit rigorous accounting for our crossover design. The units of analysis were repeated measurements per person. All models included fixed-effects for subject identifier, to eliminate between-person differences and a time-varying dummy variable for study arm assignment (i.e., videoconferencing vs. no videoconferencing). Although we did not anticipate meaningful carryover effects, we conducted exploratory analyses to challenge this assumption. For each outcome, we fit models with and without an interaction term for the study arm assignment and a dummy variable for whether the patient was assigned to receive videoconferencing first, which allowed us to assess the carryover effects. We used the p value associated with this interaction term to determine if there were statistically significant sequence effects.
INCLUSION/EXCLUSION CRITERIA
Inclusion criteria were postpartum adult individuals 18 years and older expressing human milk and had birthed a premature infant (≤34 weeks of gestational age) admitted to the study site NICU. Eligible participants were approached after their infant was admitted for at least 7 days, if they had initiated pumping of human milk, had access to videoconferencing equipment (i.e., smartphone, tablet, or laptop), and were discharged from birth hospitalization at the time of enrollment. Exclusion criteria were individuals who were incarcerated, language preference other than English, gestational surrogate, or had any medical conditions precluding breastfeeding.
RECRUITMENT AND CONSENT
Participants were identified through electronic health record review and approached by the study research coordinator either in person or through telephone for consent. A standardized informed consent document was used for the consent process. After consent, demographic baseline data were collected and then the participant was randomized.
RANDOMIZATION, DATA COLLECTION, AND STORAGE
The study statistician generated a random allocation sequence in Stata. Sequential envelopes that contained the newly enrolled mother–infant pair’s group assignment were stuffed by an individual who was not involved in the study (intervention or control first). Blinding after assignment to intervention or control was not performed. Data were collected with written data sheets completed by participants, which were then transcribed into RedCapTM by the study research coordinator. Study data were stored in a password-protected worksheet on a shared HIPAA-compliant online cloud.
Results
We assessed 1,174 postpartum patients for eligibility, 927 did not meet the inclusion criteria, 19 declined to participate, and 190 were excluded for other reasons such as Child Protective Services involvement or inability to contact the lactating parent of the hospitalized newborn. Of the 927 who did not meet the inclusion criteria and were not approached by the research assistant, the majority were either born outside of the predetermined gestational age range or were born at an outside hospital.
Thirty-eight participants enrolled into the study and were randomized; 19 were allocated to videoconferencing while pumping first (intervention) and 19 were allocated to videoconferencing while pumping second (control). Of those who were allocated to videoconferencing first (n = 19), 11 completed the study. Of the eight individuals who did not complete the study, it was because they stopped pumping, did not return their milk samples, or were lost to follow-up. Of the 19 individuals allocated to pumping with videoconferencing second, 10 completed the study and 9 did not receive the allocated intervention because the participant either stopped pumping or was lost to follow-up, see CONSORT flow diagram (Fig. 1). At the time of enrollment, the mean age of participants was 30 ± 5 years with a premature infant of 29.5 ± 2.8 weeks old; 61.1% had given birth via cesarean section. Most patients were White (60.6%), privately insured (64.5%), married or with a live-in partner (81.3%), and holding an associate degree or higher (77.4%), see Table 1 for demographic characteristics.
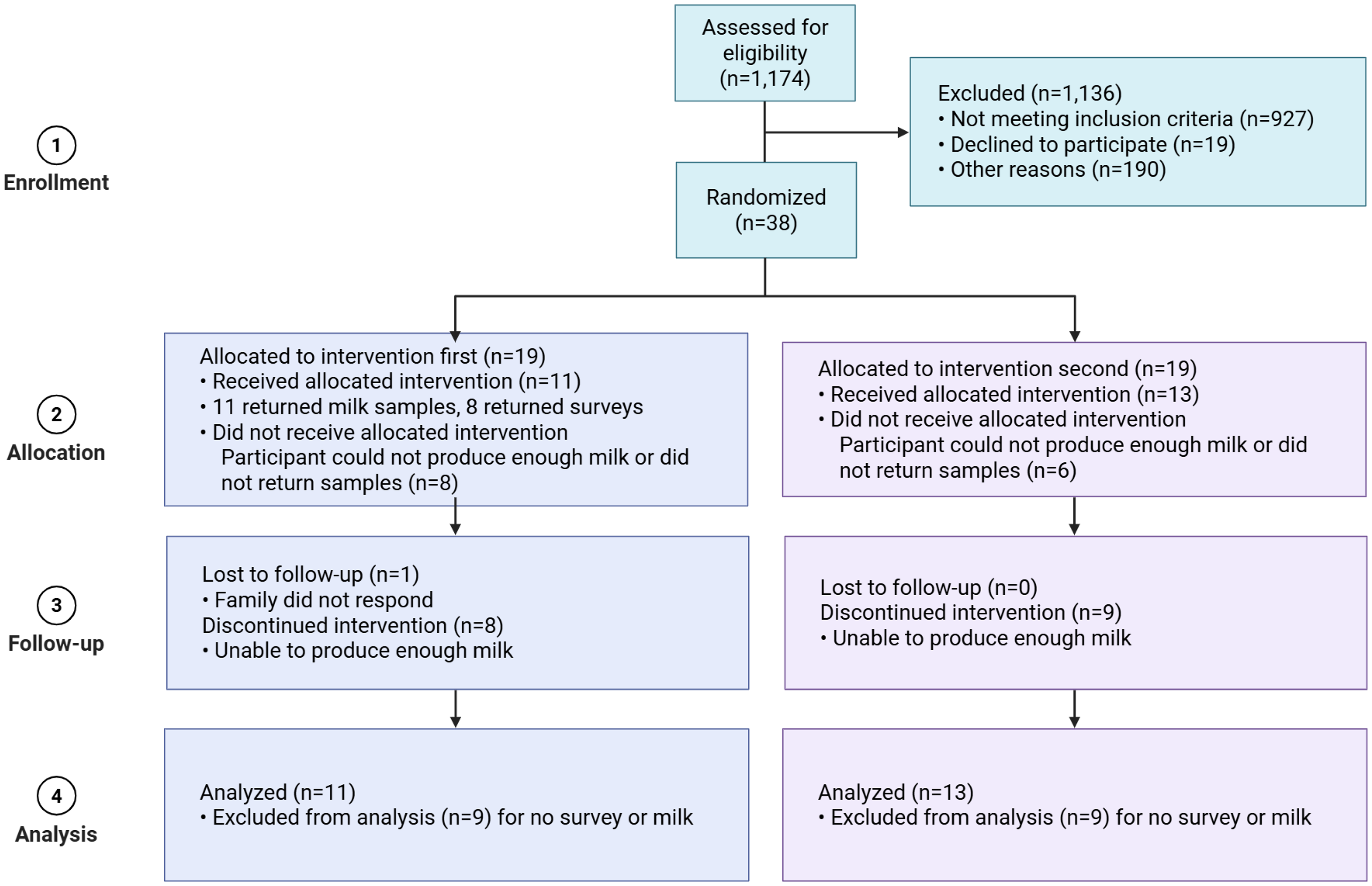
Consolidated Standards of Reporting Trials (CONSORT) flow diagram of videoconferencing while expressing milk randomized crossover trial. Created in BioRender. Hoyt-austin, A. (2026) https://BioRender.com/88ecdv2.
Demographic Characteristics of Study Participants (N = 39)
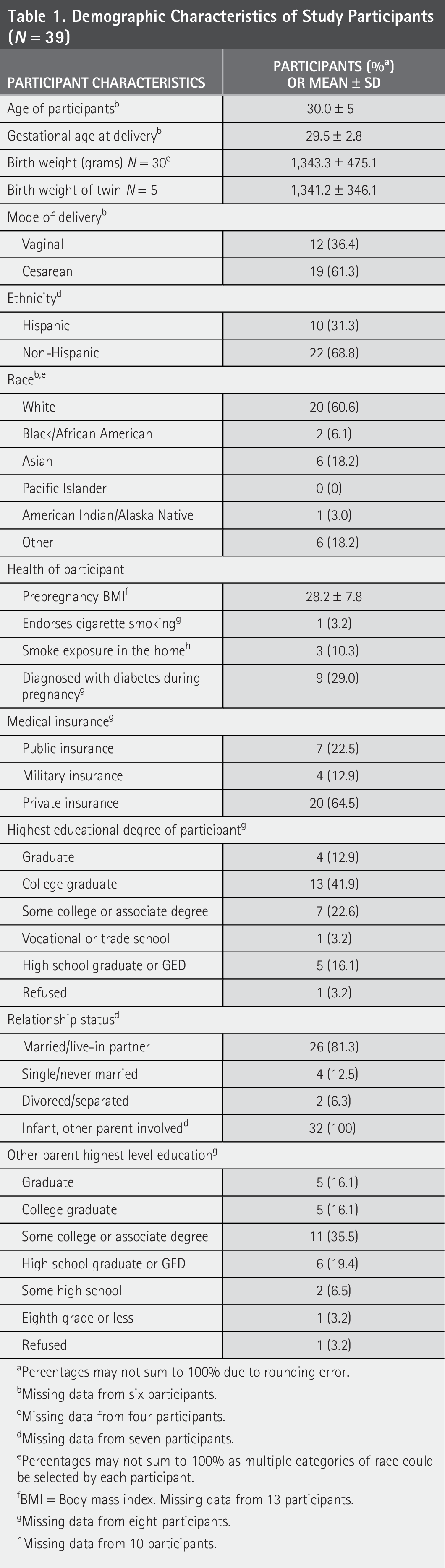
Percentages may not sum to 100% due to rounding error.
Missing data from six participants.
Missing data from four participants.
Missing data from seven participants.
Percentages may not sum to 100% as multiple categories of race could be selected by each participant.
BMI = Body mass index. Missing data from 13 participants.
Missing data from eight participants.
Missing data from 10 participants.
Of the 38 participants who consented to the study, 28 provided data on milk volume and efficiency, 26 completed BMEE surveys, and 24 provided milk samples for macronutrient analysis. We found that videoconferencing positively improved the experience of expressing human milk, with mean BMEE subscale scores 0.10 points higher with videoconferencing (95% CI: 0.02 to 0.18; p = 0.01), see Fig. 2. However, we did not find a statistically significant difference in human milk volume or efficiency with the use of videoconferencing while expressing milk. The MD for milk volume was −2.5 mL (CI: −11.9 to 6.9; p = 0.6) with the use of videoconferencing while expressing milk compared with no use of videoconferencing. The MD in time to pump, or pumping efficiency, was 0.3 mL/min (CI: −0.4 to 0.9; p = 0.4) when videoconferencing while expressing milk, compared with no use of videoconferencing.
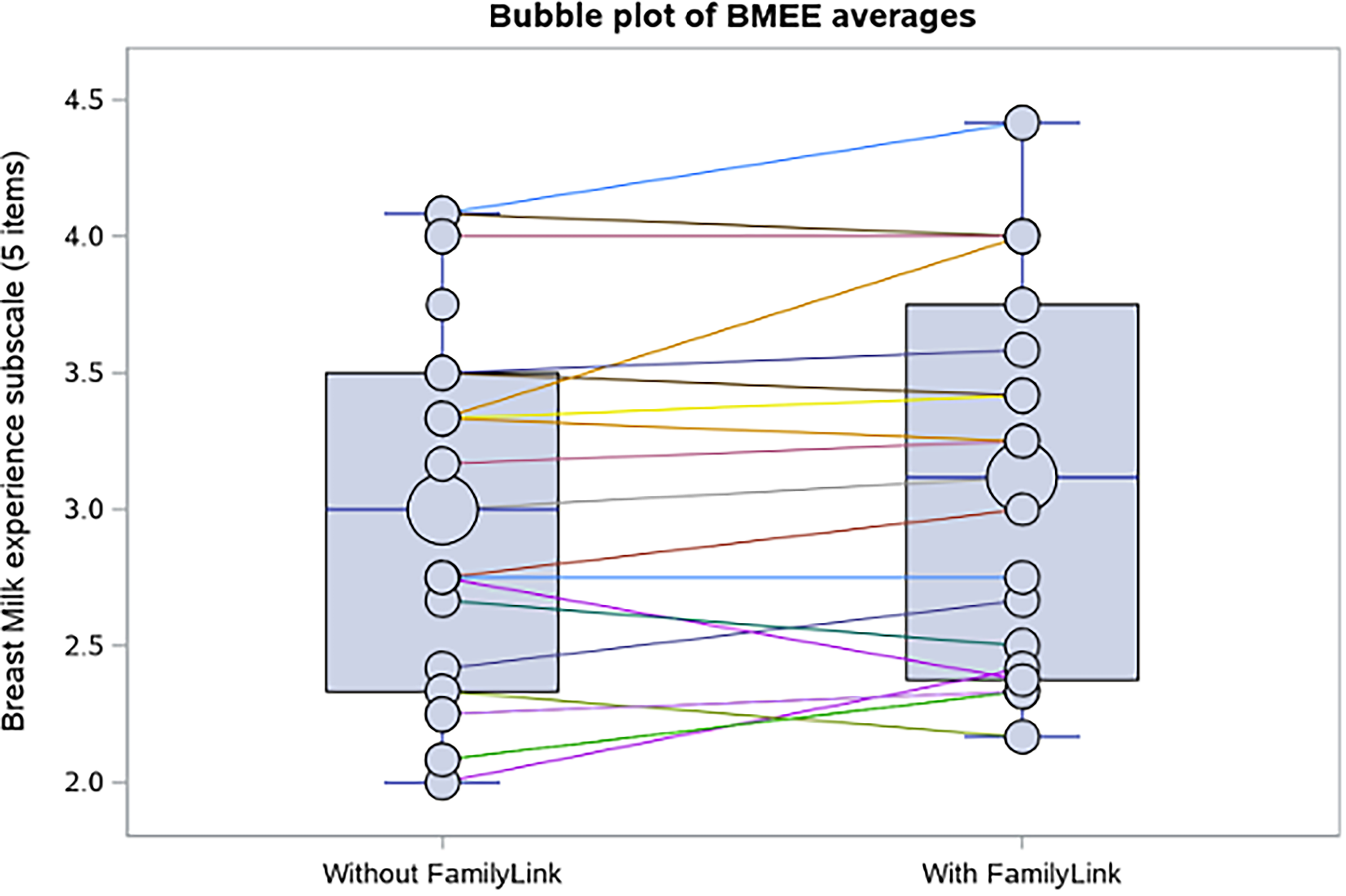
Breast Milk Expression Experience (BMEE) subscale demonstrating within-person increase in the mean BMEE score with use of videoconferencing (indicated by FamilyLink) when expressing milk versus not using videoconferencing while expressing milk. Small bubbles represent individual participants, and large bubbles represent the average BMEE score for all participants.
We analyzed our results for any effect of the crossover design, and there were no design effects for volume, efficiency, nor the BMEE. Human milk macronutrient content was impacted by the crossover design (Table 2). Those randomized to pump with videoconferencing first had statistically significant different within-person changes compared with those receiving videoconferencing last, resulting in milk with less fat (−0.52 g/100 mL, p = 0.0002) and less energy (−3.69 kcal/100 mL, p = 0.001) and more carbohydrates (0.2 g/100 mL, p < 0.0001) when videoconferencing. For participants who were randomized to the control (no videoconferencing) arm first, there was no statistically significant change in the macronutrient content of the milk.
Mean Difference in Macronutrient Content of Human Milk, Stratified by Study Design Effects
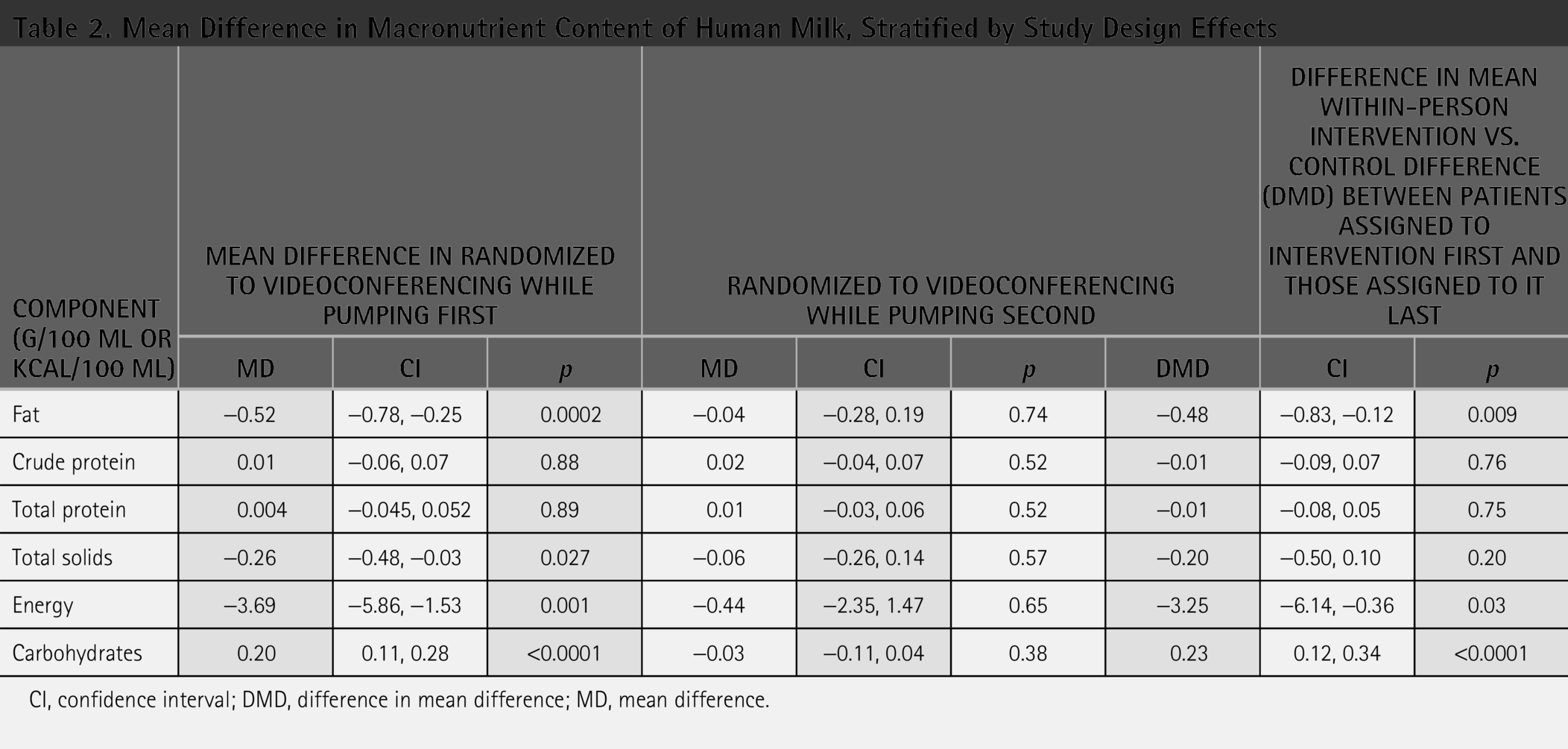
CI, confidence interval; DMD, difference in mean difference; MD, mean difference.
Discussion
In this randomized controlled crossover trial, we found that using videoconferencing to see one’s baby while expressing human milk improved the milk expression experience of mothers of hospitalized premature newborns. We did not find that use of videoconferencing significantly improved milk expression volume or efficiency.
Improving the pumping experience of postpartum individuals expressing human milk for their hospitalized premature infants is important, as parental human milk feeding improves health outcomes in this population, 24 and additional support for parents expressing milk for this population is needed. 25 In qualitative interviews of participants enrolled in this study, videoconferencing was well received and participants reported that seeing their baby while pumping was relaxing and helped with their bonding and connection with their baby. 20 Quantitative analysis of BMEE scores in this study confirmed that the use of videoconferencing improves the milk expressing experience for postpartum patients expressing human milk for their hospitalized premature infants. Our findings reflect prior work that demonstrates telemedicine improves patient experience, 16 and ours is the first study to describe that use of telemedicine while expressing milk improves the experience of mothers expressing human milk for their hospitalized premature infant.
We did not find that use of videoconferencing while expressing milk was associated with individual changes in milk volumes or time taken for participants to express milk. Previous work by our research group demonstrated that patients who had access to videoconferencing with their hospitalized infant had higher rates of human milk feeding at NICU discharge. 18 However, we found that volumes of human milk were not changed by use of videoconferencing when expressing milk. Notably, improving the overall human milk feeding rates is challenging and impacted by multiple domains, including external influences such as national and local policies, hospital practices, and family and friend support along with individual factors such as maternal health and breastfeeding self-efficacy. 26 Uscher-Pines et al. reported similarly in a large, randomized trial that the use of telelactation (telemedicine to connect patients to lactation support) did not impact overall breastfeeding exclusivity nor duration in their cohort. 27 However, the use of telelactation in their study improved breastfeeding outcomes in Black participants. Future study of the use of telemedicine in the NICU should examine how telemedicine may be used to close disparities in NICU care and ongoing human milk feeding.
We found that participants who were randomized to the intervention first had statistically significant differences in their milk, compared with the control session. Fat and energy (kilocalories) were lower in the videoconferencing pump and carbohydrates were higher. This difference was not seen in the participants randomized to the control sessions first. The most likely explanation for this observation is the small sample size. However, if such a difference in human milk macronutrients because of design effects were confirmed in future larger studies, possible mechanisms might include the impact of stress, anxiety, or the dynamic nature of human milk energy content. Prior work has demonstrated that stress and anxiety can impact milk macronutrients. 28 Also, human milk is well described to be dynamic with differences in energy content in foremilk versus hindmilk because hindmilk is more energy dense with a higher caloric density and more fat. 29
Strengths and Limitations
The strengths of this study include its novelty as the first randomized trial to test the impact of NICU videoconferencing on human milk feeding for hospitalized premature newborns. In addition, the study’s crossover design allowed for analysis of individual, rather than pooled, MDs on the impact of intervention on human milk feeding outcomes.
The limitations of this study include incomplete data collection for some participants; one reason for this was that our study began before the coronavirus pandemic and recruitment and retention of participants occurred during the height of the pandemic, limiting the ability to meet with potential participants face to face. 30 Other limitations were that participants self-reported their data and there was a brief 24-h washout period between the study arms (intervention and control), which may have contributed to the design effects seen with the macronutrient components. For this pilot trial, we used the manufacturer’s recommendations for milk analysis with the Miris HMA. However, there have been recommendations in the literature to optimize homogenization of the milk sample. 21 Future research could incorporate optimal homogenization to better analyze the extent to which visual observation impacts milk macronutrient composition.21,31
Conclusions
Telemedicine videoconferencing use in the NICU is widely implemented; however, the study of its impact on the experience of patients in the NICU and their health outcomes is limited. Our study is the first to report that using videoconferencing while expressing milk can be a strategy to improve the experience of expressing human milk for postpartum patients separated from their infant. Interventions to improve human milk feeding in the NICU are needed to increase the number of infants receiving mother’s own milk during hospitalization and improve neonatal morbidity and mortality. More work is needed to elucidate how this strategy can be used to improve the quantity, both in proportion of feeds and in duration, of mother’s/parent’s own milk that newborns receive during their birth hospitalization.
Authors’ Contributions
A.H.A. made substantial contributions to the acquisition, analysis, and interpretation of data, and drafted this article. I.T.M. made substantial contributions to the acquisition of these data. J.L.R. made substantial contributions to the interpretation of data in this study and substantively revised this article. D.J.T. made substantial contributions to the design of this study, analysis and interpretation of data, and substantively revised this article. C.J.C., M.A.U., and J.P.M. made substantial contributions to the conception and design of this study and substantively revised this article. K.K.R. made substantial contributions to the acquisition and analysis and interpretation of data, and substantively revised this article. L.R.K. and K.R.H. conceptualized and designed the study, mentored A.H.-A. in the oversight of data collection, and substantively revised this article.
All authors approved the submitted version of this article and have agreed both to be personally accountable for their own contributions and to ensure that questions related to the accuracy or integrity of any part of the work, even ones in which an author was not personally involved, are appropriately investigated, resolved, and the resolution documented in the literature.
Footnotes
Acknowledgments
The authors thank the participants in this study for their contribution to human milk research.
Funding Information
This project was funded by the UC Davis Children’s Miracle Network (PIs: L.R.K. and K.R.H.) and the Clinical and Translational Science Center Highly Innovative Award grant UL1-TR001860 (PI Dr. Ted Wun). The funders/sponsor did not participate in the work. A.H.A.’s work on this project was supported by the Quality, Safety, and Comparative Effectiveness Research Training in Primary Care (QSCERT-PC) Program funded by HRSA T32HP30037. A.H.A., J.L.R., and L.R.K.’s work is also supported by the National Center for Advancing Translational Sciences, the National Institutes of Health, through grant number UL1 TR001860. L.R.K. and A.H.A.’s effort was also supported by a Building Interdisciplinary Research Careers in Women’s Health award (K12 HD051958, PI Dr. Nancy Lane) funded by the National Institute of Child Health and Human Development (NICHD). J.L.R. was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, the National Institutes of Health, through grant number K23HD101550. The contents of this publication are solely the responsibility of the authors and do not represent the official views of the National Institutes of Health or HRSA.
Trial Registration
This trial was registered at ClinicalTrials.gov (NCT03957941) on May 13, 2019.
Disclosure Statements
All authors attest that they have no financial or personal conflicts of interest in this work.
Ethics Approval and Consent to Participate
This study was approved by the University of California (UC) Davis Institutional Review Board on December 21, 2019, reference number 1370355-4. Informed consent was obtained from all participants. This study was performed in accordance with the Declaration of Helsinki.
Consent for Publication
Not applicable as individual details, images, or videos are not included.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.