
Abstract
Background:
Technological advancements and legislation have led to the widespread use of electronic health records (EHRs) in the 21st century. Along with EHR implementation came improved health care quality, continuity of care, and data availability. However, EHRs are not without drawbacks. Physician burnout rates are rising, and EHRs are among the top causative factors. The consequences of burnout can offset the benefits of EHRs, prompting the health care community to seek solutions for the burnout epidemic. One proposed solution is to use artificial intelligence (AI) scribes, which utilize voice-recognition software to transcribe patient-physician interactions in real time, resulting in comprehensive documentation of the encounter. Since AI technology is in its infancy, limited research is available regarding provider perceptions and the real-world use of AI scribes. This study aimed to evaluate health care providers’ experiences with documentation burden and perceived quality of patient interactions while using an AI scribe in a telehealth setting.
Methods:
Participants used the AI scribe exclusively during telehealth encounters. Provider attitudes and experiences were measured across the 3-month pilot period to assess changes in documentation burden, workflow efficiency, satisfaction, and perceived impact on patient interaction quality.
Results:
Study results revealed that three-fifths of the providers experienced decreased burnout attributed to the AI scribe, and two-thirds of the providers reported enhanced satisfaction with documentation time and the time spent engaging with patients.
Conclusion:
Given our study results and the promising direction of AI technology, the use of AI scribes in the telehealth setting has the potential to mitigate burnout, improve the provider-patient relationship, and help restore patient-centered care.
Keywords
Introduction
As early as the 1960s, academic medical institutions began using electronic health records (EHRs) primarily for billing and scheduling.1,2 Broader utilization of EHRs occurred alongside the technological advancements of recent decades as storage capabilities improved and technology became more portable; however, widespread EHR adoption in the United States (U.S.) primarily occurred after the passage of the Health Information Technology for Economic and Clinical Health Act (HITECH; 2009)3,4 and the 21st Century Cures Act (2016). 5 These acts, which implemented financial incentives for EHR adoption, led to U.S. physician EHR utilization increasing from 4.7% in 2007 to 88% in 2021.6,7
The widespread implementation of EHRs has fostered progress toward improvements in health care quality, diagnostic accuracy, continuity of care, and data availability for government and research agencies while reducing redundancies and streamlining billing processes.8–11 Despite the successes of these acts, unintended and severe consequences also resulted, including increased administrative burden, disrupted patient-physician interactions, and extended work hours. As the percentage of physicians utilizing EHRs grew, so did the percentage of physicians experiencing burnout: an estimated 50–80% of physicians experience burnout, and EHRs rank among the top causative agents.12–19 The consequences of burnout offset the benefits of EHRs, as burnout contributes to higher health care costs, increased medical errors, and reduced patient satisfaction. 20 Widespread utilization of EHRs is unlikely to change; thus, the health care community is tasked with balancing the benefits of EHRs with their contributions toward physician burnout.
One proposed solution is the use of scribes. Traditionally, medical scribes are humans who assist physicians in the clinical setting by documenting patient encounters, entering orders, and completing the numerous tasks required to characterize an encounter for billing and coding purposes accurately. Although medical scribes have proven to help mitigate burnout, there are drawbacks to employing them. Scribes often experience high turnover rates, partly because they use this role as a stepping stone to higher-level careers and partly due to their own burnout. As a result, they may lack familiarity with medical terminology, which can lead to frustration and inefficiency among providers. Data also suggest that providers must see two to four more patients daily to make hiring a scribe financially sustainable. 21
In response to these limitations, artificial intelligence (AI) scribes have emerged as a newer addition to the health care workforce, offering many of the benefits of traditional scribes while addressing key limitations.22,23 Unlike human scribes, AI scribes can mitigate challenges related to recruitment and retention, support enterprise-wide scalability, and enable standardized documentation across clinical settings. 24 In addition, AI scribes create downstream opportunities for integration with clinical decision support tools and can improve revenue cycle efficiency through more consistent, complete, and timely clinical documentation.22,24
Building on these operational advantages, AI scribing leverages advances in natural language processing algorithms, real-time speech recognition, and contextual understanding to accurately capture and transcribe patient-physician interactions. This enhances clinical documentation efficiency and reduces the cognitive burden on providers. Current work suggests that physicians utilizing AI scribes experience decreased cognitive demands, temporal demands, and workload, thus reducing feelings of burden and burnout. 25 Additionally, AI scribes can integrate into already-existing EHRs, hence contributing to the previously-stated positives of EHR use and allowing patients to continue accessing their health data promptly, for government agencies and researchers to access data, and for physicians to collaborate on patient cases. Despite its relative infancy, AI-based scribing may offer a means of mitigating physician burnout driven by the growing documentation burden of EHR use.
While AI technology is promising, limited research exists on provider and patient perceptions, as well as the real-world use of AI scribes in clinical practice. Limited data exist on the impact of AI scribing tools on perceived scribe burden or the quality of provider-patient interactions, especially in telehealth contexts. Despite the growing integration of audio-video telehealth into clinical practice, meaningful patient engagement remains a significant challenge and barrier to widespread adoption of telehealth. Additionally, limitations in nonverbal communication, screen fatigue, and technical barriers can reduce the quality of provider-patient interaction.
Since managing documentation while maintaining clinical rapport is specially challenging during telehealth encounters, we hypothesized that by automating real-time clinical documentation, AI scribes can alleviate providers’ cognitive and administrative load, enabling them to redirect focus toward active listening, empathetic communication, and patient-centered decision-making. This shift can potentially enhance the telehealth experience for patients and providers, thereby increasing satisfaction and adoption of virtual care platforms.
Thus, this study was tailored to specifically examine the use of AI scribe technology in a telehealth setting to evaluate health care providers’ experiences related to documentation burden and their perceived quality of patient interactions during an initial 3-month deployment of an AI scribing tool.
Methods
IRB DETERMINATION
Institutional Review Board approval with Waiver of Documentation of Informed Consent was obtained from the University of Mississippi Medical Center prior to initiation of the study (UMMC-IRB-2023–381). At the beginning of each telehealth visit, the provider asked the patient for consent to the use of the AI scribe during the visit.
IMPLEMENTATION OF THE AI SCRIBE PROJECT
The AI scribe pilot was implemented to evaluate the feasibility and effectiveness of using AI technology to assist with clinical documentation. The process began with contracting an AI vendor (Ambience Healthcare, San Francisco, CA, USA) that had undergone thorough vetting by an independent third party to ensure compliance with security, privacy, and regulatory standards.
Clinicians were trained to use the system during patient encounters, with the AI scribe capturing and generating real-time clinical notes. During this pilot, the AI scribe was not integrated with the EHR system. Providers edited the AI-generated output and manually copied and pasted it into the electronic medical record (EMR). Throughout the pilot, feedback was systematically collected to assess accuracy, usability, and impact on documentation time. Adjustments were made iteratively to optimize the tool’s performance and ensure alignment with clinical documentation standards and privacy requirements. Table 1 illustrates the volume of telehealth encounters and that of encounters where the AI scribe was used.
A Weekly Count of Encounters Was Extracted from the EHR and from the Ambience System across 28 Weeks, with 1 Week Skipped. Thus, the Total Number of Weeks in Which Weekly Numbers Were Pulled is 27 (Week 1: September 8–September 14, 2024; Week 27: March 16–March 22, 2025). The Table Shows the Totals for All 27 Weeks

Column totals are displayed in bold text.
The study period for the survey was May 30, 2024 through September 11, 2024. The weekly encounter count described above did not occur during most of the survey study period. Column totals are displayed in bold text.
STUDY DESIGN
This study consisted of a pre/postsurvey design to examine provider attitudes toward using an AI scribe in the context of telehealth encounter-related documentation. All clinical encounters supported by the AI scribe were audio/video telemedicine visits. The goal was to evaluate changes in provider-reported experience, satisfaction, and perceptions of documentation burden and workflow efficiency. Surveys were administered at three time points: before initial use (baseline), 1 month after implementation, and 3 months post-implementation.
PARTICIPANTS
The study included 19 telehealth-based health care providers representing geriatrics, mental health, neurology, psychiatry, and urgent care specialties. The demographics of the survey study participants are shown in Fig. 1. Eligible participants were health care providers who engaged in telehealth visits and adopted the AI-based scribe tool as part of their clinical workflow. Providers were excluded from the analysis if they did not complete any survey or opted out of participation. There were no added risk or compliance concerns specific to mental health visits when using the AI scribe, as audio recordings were only retained until the note was generated or 7 days had passed, whichever occurred first.
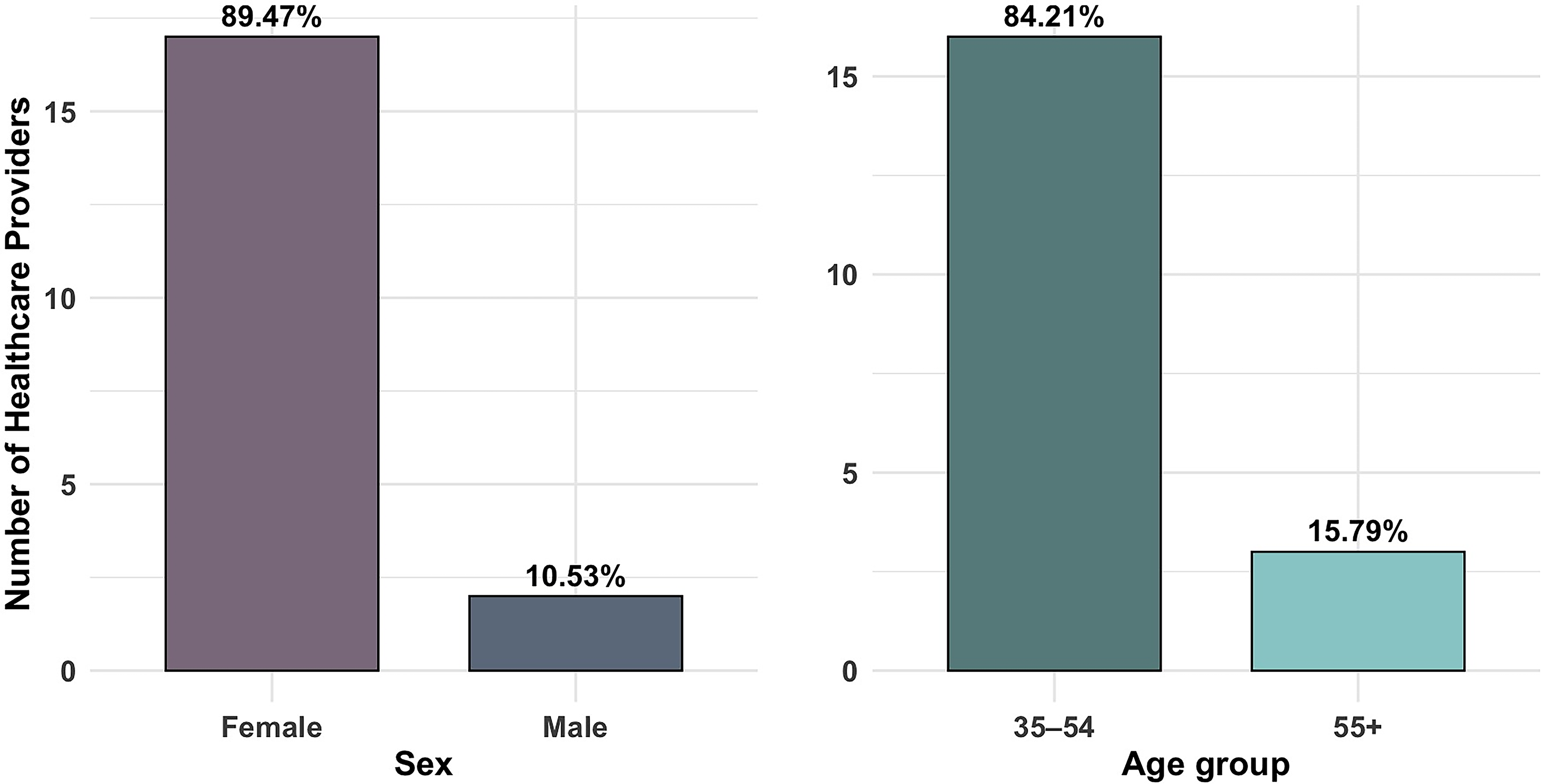
Health care providers showed demographic homogeneity with strong female representation and midcareer experience. Demographic characteristics of study participants showing distribution by sex (left panel) and age group (right panel). The study included 19 participants total, with 89.47% female (n = 17) and 10.53% male (n = 2). Age distribution showed 84.21% in the 35–54 age group (n = 16) and 15.79% in the 55 + age group (n = 3).
REDCAP
Study data were collected and managed using REDCap (Research Electronic Data Capture) electronic data capture tools hosted at the University of Mississippi Medical Center. REDCap is a secure, web-based application designed to support data capture for research studies, providing (1) an intuitive interface for validated data entry; (2) audit trails for tracking data manipulation and export procedures; (3) automated export procedures for seamless data downloads to common statistical packages; and (4) procedures for importing data from external sources. 26
SURVEY PROCEDURES
Ambience AutoScribe, an AI-powered scribing tool, was deployed to assist providers during telehealth encounters by automatically generating clinical documentation. Surveys were distributed via REDCap, which was also used for data storage and to link pre- and postsurvey responses using randomly assigned identifiers to ensure participant anonymity.
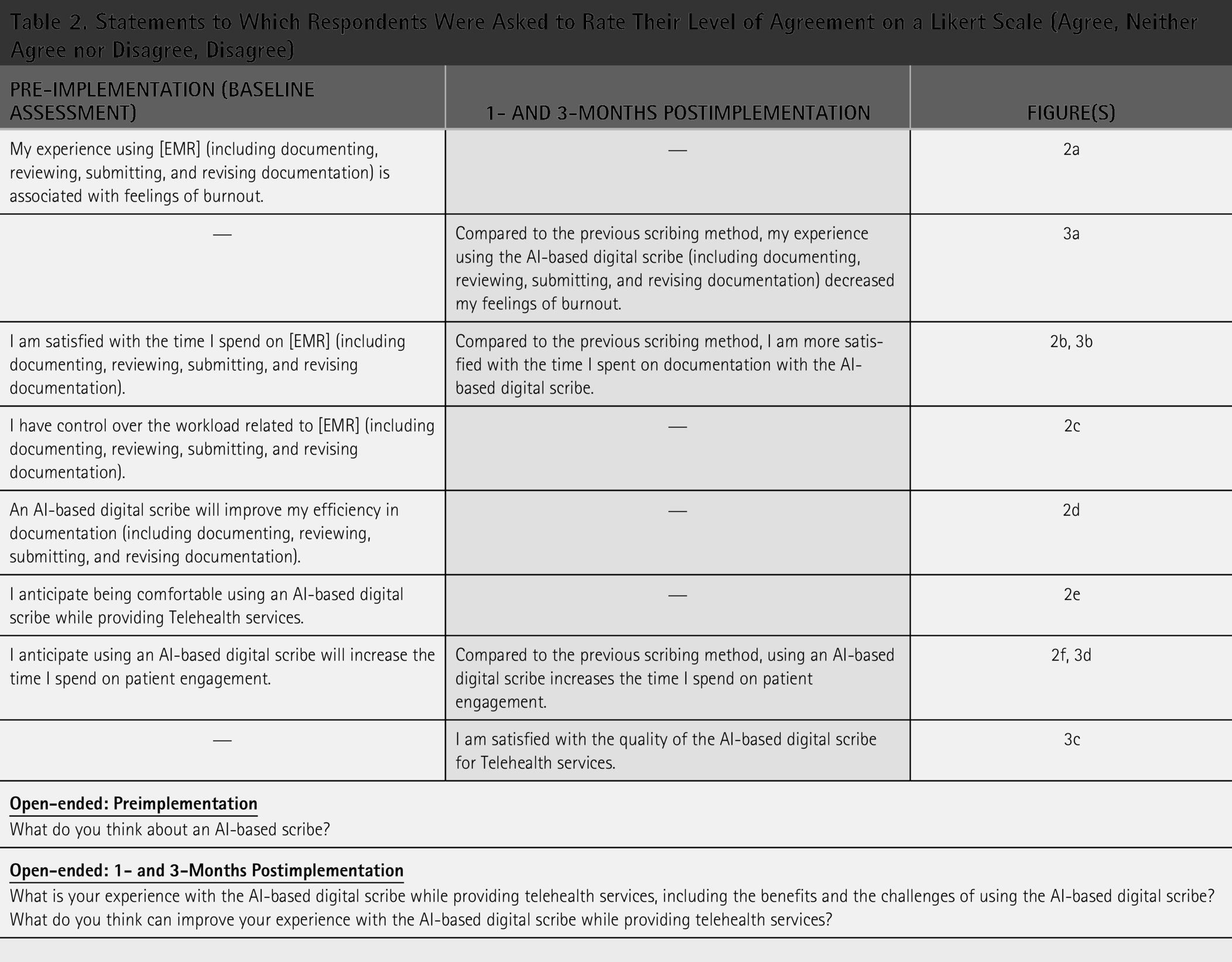
The presurvey was administered 1–2 weeks before the initial use of the AI scribe. Post-surveys were distributed 1 month and 3 months after adoption. The baseline survey assessed providers’ current documentation burden and expectations regarding the AI tool. The follow-up surveys evaluated satisfaction with the AI scribe, perceived impact on workflow, and quality of patient interaction. The exact questionnaire items are shown in Table 2.
Statements to Which Respondents Were Asked to Rate Their Level of Agreement on a Likert Scale (Agree, Neither Agree nor Disagree, Disagree)
OUTCOME MEASURES AND STATISTICAL ANALYSIS
The primary outcome was provider-reported satisfaction with documentation and workflow burden following implementation of the AI scribe. Secondary outcomes included provider-perceived usability of the AI tool and the impact of its use on the quality of patient interactions during telehealth visits. All outcomes were measured based on provider survey responses collected before AI scribe implementation and at 1- and 3-months postimplementation. Survey responses were summarized using descriptive statistics and percentages. Visualizations were developed to illustrate changes in attitude and highlight emerging patterns throughout the study period.
Results
TELEHEALTH ENCOUNTERS
Across the 27 weeks we reviewed, there were 5,388 telehealth encounters, of which 4,637 (86.1%) involved the use of the AI scribe. The use of AI scribe was high across most specialties, with psychiatry (96.7%) and urgent care (98.3%) reported using nearly all the time. In contrast, neurology had much lower AI scribe use (44.2%), highlighting differences in adoption of AI scribe (Table 1).
LIKERT RESPONSES: BASELINE
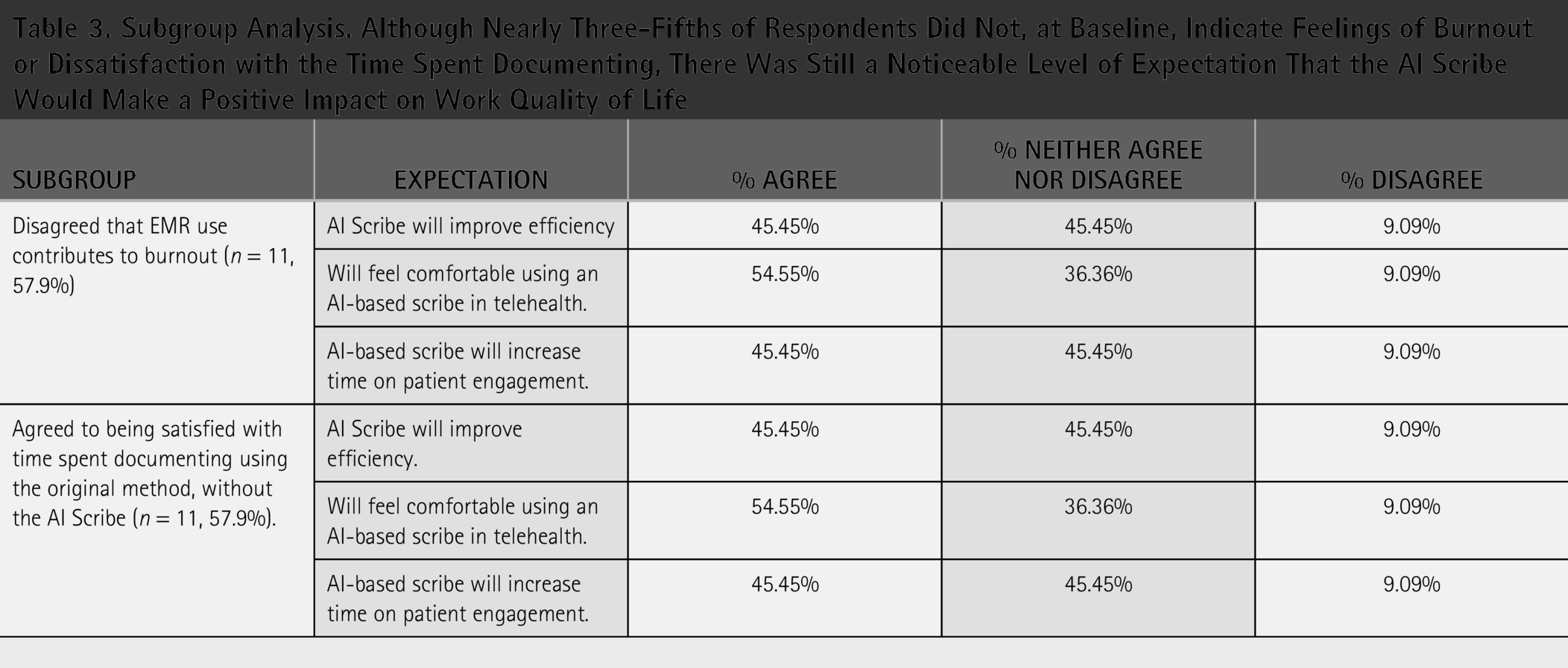
Our initial survey revealed that 57.89% of participating health care providers did not associate their experience with the EHR (including documenting, reviewing, submitting, and revising documentation) with feelings of burnout (Fig. 2a). As shown in Table 3, within this subgroup, 45.45% of respondents still expected improvements in efficiency and increased patient engagement. Notably, 54.55% of these providers anticipated feeling comfortable using the AI scribe while providing care via telehealth.
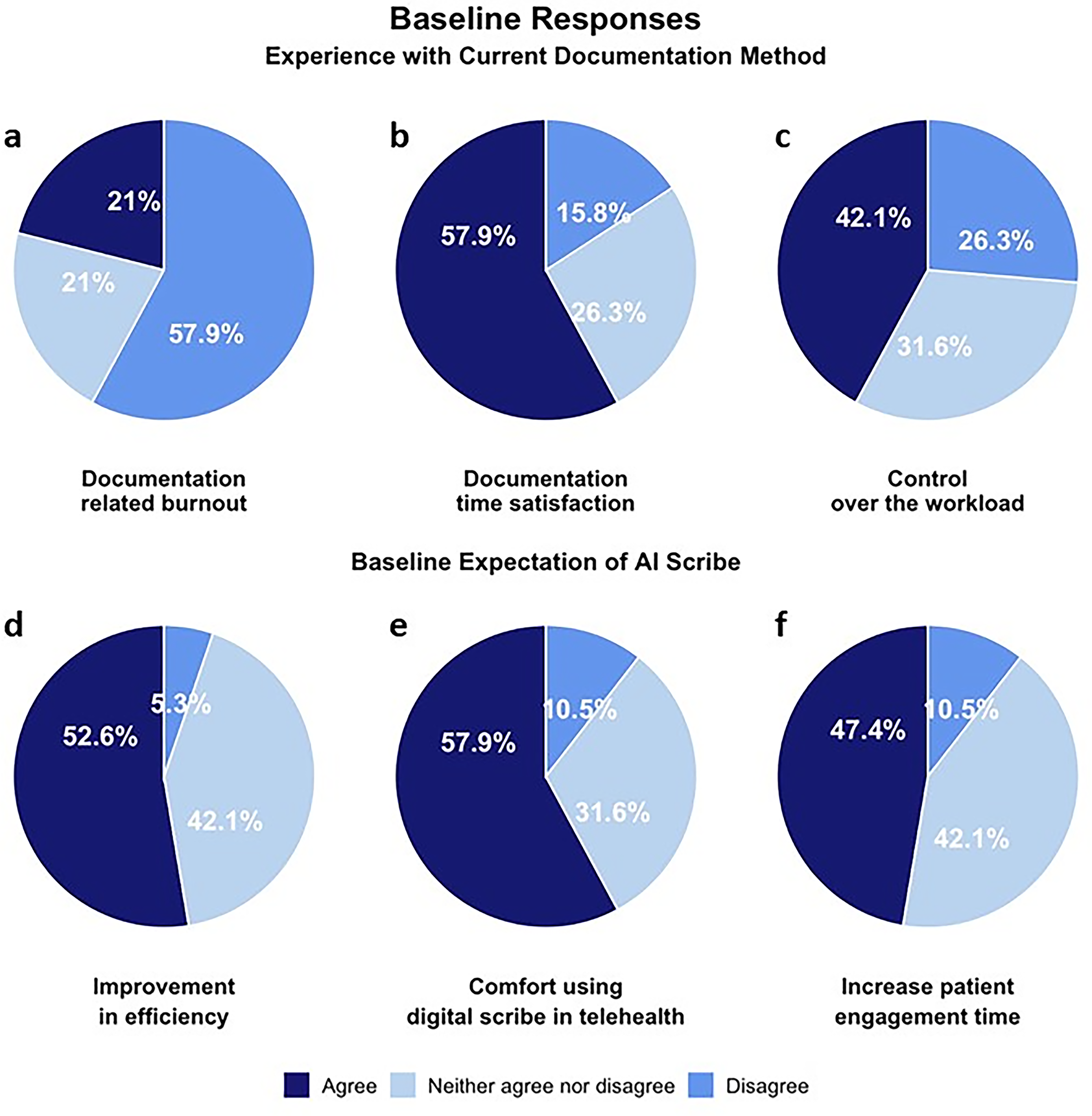
Health care providers showed mixed baseline satisfaction with documentation but expressed optimism about AI scribe potential. Baseline responses regarding current documentation methods and AI scribe expectations across six measures:
Subgroup Analysis. Although Nearly Three-Fifths of Respondents Did Not, at Baseline, Indicate Feelings of Burnout or Dissatisfaction with the Time Spent Documenting, There Was Still a Noticeable Level of Expectation That the AI Scribe Would Make a Positive Impact on Work Quality of Life
Panels 2b and 2c further illustrate the workload-related experience of the respondents at baseline. Though most providers (57.9%; Fig. 2b) were already satisfied with the amount of time spent documenting in the EHR, only 42.1% reported having control over their workload (Fig. 2c).
Figs. 2d to 2f serve as an index of the respondents’ likelihood of adopting an AI scribe. Around half of the respondents (52.63% and 47.37%, respectively) believed an AI-based scribe would enhance efficiency and allow more patient engagement time. Furthermore, 57.89% expected to feel comfortable using the AI scribe.
OPEN-ENDED RESPONSES: BASELINE
Next, we summarize the responses at baseline to open-ended portions of the survey (“What do you think about an AI-based scribe?”). Overall, the participants expressed optimism and openness toward using an AI-based digital scribe in telehealth, anticipating increased productivity and reduced documentation burden despite limited prior experience.
LIKERT RESPONSES: 1- AND 3-MONTHS POSTIMPLEMENTATION
Fig. 3a illustrates the perceived documentation-related burnout experienced by providers after incorporating the AI Scribe. After just 1 month of use, 53.85% of providers reported experiencing less burnout. This positive sentiment grew even stronger after 3 months, with 61.54% of respondents agreeing that they experienced less burnout after adopting the AI Scribe.
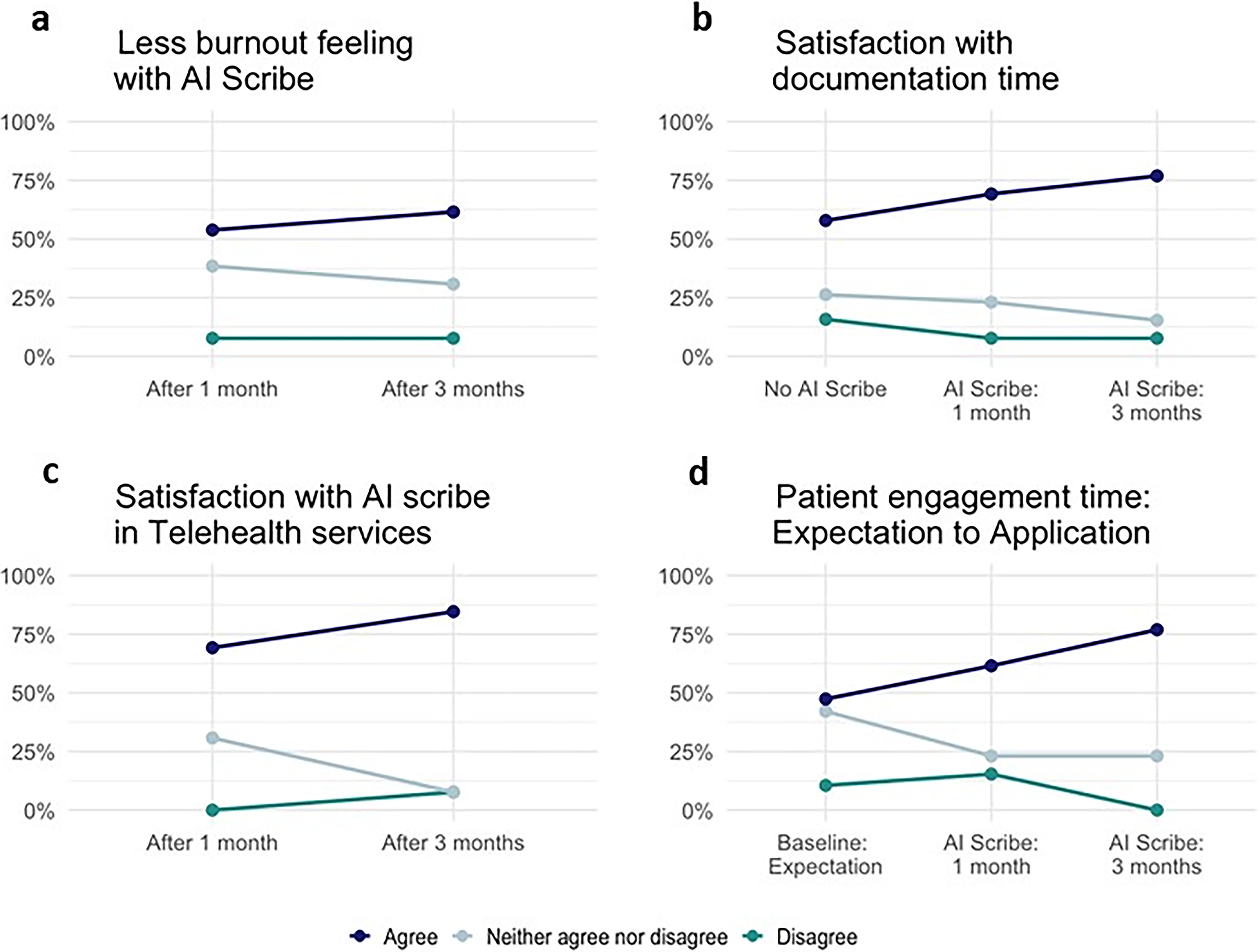
AI scribe implementation led to progressive improvements in provider satisfaction and reduced burnout over 3 months. Longitudinal changes in health care provider responses following AI scribe implementation across four measures:
Fig. 3b compares provider satisfaction with documentation time pre- and postimplementation of the AI scribe. Initially, 57.89% of providers were satisfied with documentation time before implementation. After 1 month with the AI Scribe, satisfaction increased to 69.23%, and it continued to rise, reaching 76.92% after 3 months of AI Scribe application.
Fig. 3c illustrates provider satisfaction with the quality of the AI Scribe. This satisfaction level increased over time, from 69.23% satisfaction after 1 month to 84.62% after 3 months of use.
Fig. 3d highlights provider optimism regarding the impact of AI Scribe on patient engagement (also shown in Fig. 1f). Before using the AI Scribe, 47.37% were optimistic about its ability to increase patient engagement. In contrast, 61.54% and 76.92% of providers agreed with the statement “Compared to the previous scribing method, using an AI-based digital scribe increases the time I spend on patient engagement” after using it for 1 month and 3 months, respectively.
OPEN-ENDED RESPONSES: 1- AND 3-MONTHS POSTIMPLEMENTATION
Finally, we summarize responses to the question, “What is your experience with the AI-based digital scribe while providing telehealth services, including the benefits and the challenges of using the AI-based digital scribe?” after 1- and 3 months of use; and “What do you think can improve your experience with the AI-based digital scribe while providing telehealth services?” at the conclusion of the study. In response to the first question, clinicians largely reported positive experiences, noting benefits such as reduced documentation workload, more patient engagement time, and accurate, structured capture of clinical information. However, they also encountered challenges, including difficulty capturing nonverbal cues (especially in psychiatry), generic or incomplete transcriptions, and technical issues. By 3 months, providers suggested improvements such as better system integration, enhanced transcription accuracy, improved speaker attribution, and greater editing flexibility, all while maintaining enthusiasm for future use.
Discussion
In summary, the 3-month pilot of the AI scribe demonstrated a clear positive shift in provider perception of the scribing tool. What began with varied initial responses regarding workload control, efficiency, and comfort with the tool concluded with most providers reporting reduced burnout and increased satisfaction with documentation time, patient engagement, and the quality of AI-generated notes.
In this article, we demonstrate the integration of an AI scribe into patient care during telehealth encounters, highlighting its potential to transform virtual care delivery. By automating clinical documentation in real-time, the AI scribe enables providers to focus more fully on interpersonal communication, eye contact, and active listening—key elements that are often diminished in digital consultations. The AI scribe has the potential to capture and organize patient information, generate summaries, and assist in formulating follow-up plans, which not only reduces clinician cognitive load but also provides an opportunity to engage patients more, leading to higher adoption of telehealth and increased access to care.
Several studies have demonstrated the benefits of AI scribes in improving efficiency, reducing provider burnout, and enhancing documentation quality during in-person outpatient visits.26–28 These investigations have focused mainly on traditional clinical settings where the patient and provider are colocated. However, to the best of our knowledge, no studies have exclusively examined the effectiveness of AI scribes in telehealth encounters where the provider and patient are not in the same geographic location. This distinction is essential, as communication dynamics, technological challenges, and workflow adaptations differ significantly in virtual care environments. Our study aims to fill this gap by evaluating the role of AI scribes specifically in the context of geographically separated provider-patient interactions, offering novel insights into their potential to support patient engagement in remote health care delivery.
Before our 3-month study period, we hypothesized that, similar to in-person providers, telehealth providers would experience less burnout and more positive patient interactions when utilizing an AI scribing tool. Interestingly, although most of our providers did not initially have negative perceptions of their current EHR, we observed positive outcomes in all areas—well-being, patient interaction time, and documentation time. By the 1-month mark, half of providers reported decreased burnout credited to AI scribe usage, and this number increased to 61.54% by 3 months. Additionally, two-thirds of providers reported increased satisfaction with the time spent on documentation and patient engagement. Notably, 84.6% of our providers expressed satisfaction with the quality of the AI scribe. Given these findings, we posit that using AI scribes is a viable option for enhancing physician satisfaction and well-being by reducing the time spent on documentation and increasing the time spent engaging with patients.
We recognize that the generalizability of our study is limited by its short time frame and small sample size (n = 19), with the majority of providers being younger than the average U.S. physician, who is 51.5 years old. 29 However, our study included providers in geriatrics and psychiatry who often have a lengthy and complex documentation demand. Visits within these specialties often require detailed histories, cognitive and behavioral assessments, medication reviews, and documentation of subtle clinical observations—all of which can make it difficult for providers to maintain meaningful patient engagement during telehealth encounters.
The note-taking burden can reduce eye contact, interrupt rapport, and limit the provider’s focus on the patient. Our study demonstrates that using an AI scribe meaningfully improves workflow efficiency and patient-provider interaction in these documentation-heavy fields. Given these findings, it is reasonable to expect those other specialties—particularly those with similar documentation demands—could also substantially benefit from integrating AI scribe technology into their telehealth workflows.
Providers who are already conducting telehealth visits are likely more comfortable with technology due to prior experience, which may have contributed to our participants’ baseline comfort with the original EHR and their reported ease of use with the AI scribing software.
LIMITATIONS
While the present study offers promising insights into provider experiences, its scope is limited by the absence of objective data measuring actual reductions in documentation time. The findings are primarily based on subjective provider feedback, which, while valuable, may be influenced by recall bias or individual expectations. Additionally, the study does not include patient perspectives, leaving a critical gap in understanding how the use of AI scribes may impact patient engagement or satisfaction during telehealth visits. Without evaluating patient-reported outcomes, it remains unclear whether perceived improvements in provider efficiency translate to a better experience for those receiving care. Finally, our study did not explore the cost-effectiveness of AI scribe implementation, a concern shared with human scribes and EHR utilization. However, this factor requires further study to inform provider decisions regarding the implementation of AI scribes into their practices. Future evaluation should also pay close attention to the integration of any AI scribe with the EHR that is used by the providers, which was not a feature of the present pilot.
Despite our study’s limitations, it is evident that the use of AI scribes in the telehealth setting can enhance patient engagement to increase adoption of telehealth visits and increased satisfaction among both providers and patients. As future studies further elucidate the benefits of AI scribes and their cost-effectiveness, we believe providers will recognize the potential of AI scribes to enhance work-related quality of life and the care they can provide to their patients.
Authors’ Contributions
L.B.K.: Conceptualization (supporting), supervision (supporting), data curation, formal analysis, investigation, methodology, project administration, writing—original draft, writing—review and editing; A.J.W.: Writing—original draft; A.C.E.: Writing—original draft; F.A.L.: Formal analysis, visualization; Y.-Y.L.: Methodology, formal analysis; T.D.: Data curation; V.T.: Writing—review and editing; V.K.N.: Writing—review and editing; C.S.: Conceptualization (lead), funding acquisition, supervision (lead), writing—review and editing.
Footnotes
Funding Information
This publication was made possible by the Health Resources and Services Administration (HRSA) of the US Department of Health and Human Services (HHS) as part of the National Telehealth Centers of Excellence Award (U66RH31459). The contents are those of the author(s) and do not necessarily represent the official views of nor an endorsement by the HRSA, HHS, or the U.S. Government.
Disclosure Statement
No competing financial interests exist.