
Abstract
Objectives
To examine the explanatory variables for consumers’ selection of either telephone consultation or video consultation for specific health conditions, using multinomial regression analysis conducted on a national survey dataset.
Methods
A cross-sectional survey was conducted involving a sample of Australian adults who had used a telehealth service in 2021. An online sampling service by Qualtrics® enabled the recruitment of consumers that represented the Australian population in terms of gender, age, location (state or territory), and place of residence (urban or remote). Data collected included demographics, recent telehealth experience, and preferences for telephone or video consultation for different scenarios including varying time lengths and reasons for seeking a general practitioner.
Results
A total of 1,069 consumers completed the survey. In-person consultations at a clinic were the top preference in all clinical scenarios presented, except when needing a prescription or to receive test results. In these cases, telephone consultation was preferred. General videoconferencing experience in day-to-day life increased the likelihood of consumers choosing video consultations over in-person clinic visits for their general practitioner appointments. In addition, consumers’ preferences for telephone consultations appear to be increased by internet connection issues and needing support to access technology.
Conclusions
This paper revealed that there are a variety of reasons influencing consumer preferences for health care modalities. It also demonstrated that increased exposure to videoconferencing increased consumer preferences for video consultations, particularly when seeking advice for chronic conditions, and decreased their likelihood of choosing telephone over in-person appointments, and that consumers avoid video consultations when they are experiencing technological issues or when they need support. The results of this survey give valuable insights into consumer preferences for telehealth and factors that may influence telehealth uptake within our health system.
Introduction
For a number of years, telephone and video consultations have been explored as an alternative to in-person health services. Services and research increased as a result of the COVID-19 pandemic, which put pressure on providers and health services to offer a telehealth alternative when consumers could not access in-person care due to the inability to leave their homes or infection risks associated with travel and in-person visits.1–4 Most papers report positive satisfaction and positive perceptions, indicating opportunity for continued growth in this area.5–7 Benefits from the continued use of telehealth technology have included increased access to health services, decreased costs for society, and safe, effective deliverance of care.5,8–10 In some cases, telehealth may be the only option for the efficient and effective provision of health services to remote or rural populations. 11 For these reasons, the sustained use of telehealth following the COVID-19 pandemic remains of great interest. 4
This study aims to build on current research by further exploring telehealth experiences for consumers across a range of reasons for visiting a general practitioner (GP) and assessing the likelihood of selecting telephone or video consultation modalities over in-person consultations in a variety of scenarios. The aim of this study was to examine the explanatory variables for consumers’ selection of either telephone or video consultations for specific health conditions, using multinomial regression analysis conducted on a national survey dataset. These findings will help inform decisions regarding telehealth service configuration, modality offerings to consumers for various scenarios, and future research to address perceived barriers to telehealth adoption.
Method
Data were collected using an Australia-wide cross-sectional survey conducted during February and March 2022. The aim of the survey was to gather information about telehealth preferences from a representative sample of Australians who had used telehealth within the previous year. The survey was anonymous, and recruitment was carried out by Qualtrics. Participant recruitment and demographics have been described in detail previously. 12 Telehealth refers to either video or telephone consultations for the purposes of this paper. Respondents are referred to as consumers throughout to align with the language recommended by the Australian National Health and Medical Research Council.
Participants
Consumers were recruited to be a representative sample of Australian adults via Qualtrics® online survey platform according to their age, gender, state or territory of residence, and location (metropolitan or nonmetropolitan). Consumers who had not used telehealth over the last year or who were under 18 years of age were excluded from the survey. Participants were presented with information about the survey prior to the first question and had to agree to the consent statement before they could continue.
Survey Questions
While the survey was extensive and included many different questions,12–14 this paper focuses on respondent demographic information, consumers’ most recent telehealth experience, and their stated preference for appointment types given a particular condition or reason for visiting their GP (Supplementary Data).
Respondents were then presented with the top 15 most common reasons for a GP visit (MCRfaGPV) and asked to indicate whether they would prefer that their appointment be in-person at home, in-person at a clinic, delivered by phone, or by video. 15 The top 15 MCRfaGPV were taken from the 2015–16 Bettering the Evaluation and Care of Health report. 15 These included hypertension (high blood pressure), general check-up, upper respiratory tract infection (chest infection), depression, diabetes, arthritis, back complaint, lipid disorder (high cholesterol), need a prescription, gastroesophageal reflux disease (reflux or heartburn), test results, anxiety, asthma, acute bronchitis/bronchiolitis (bad cough or chest infection), and urinary tract infection (UTI) ( Fig. 1 ).
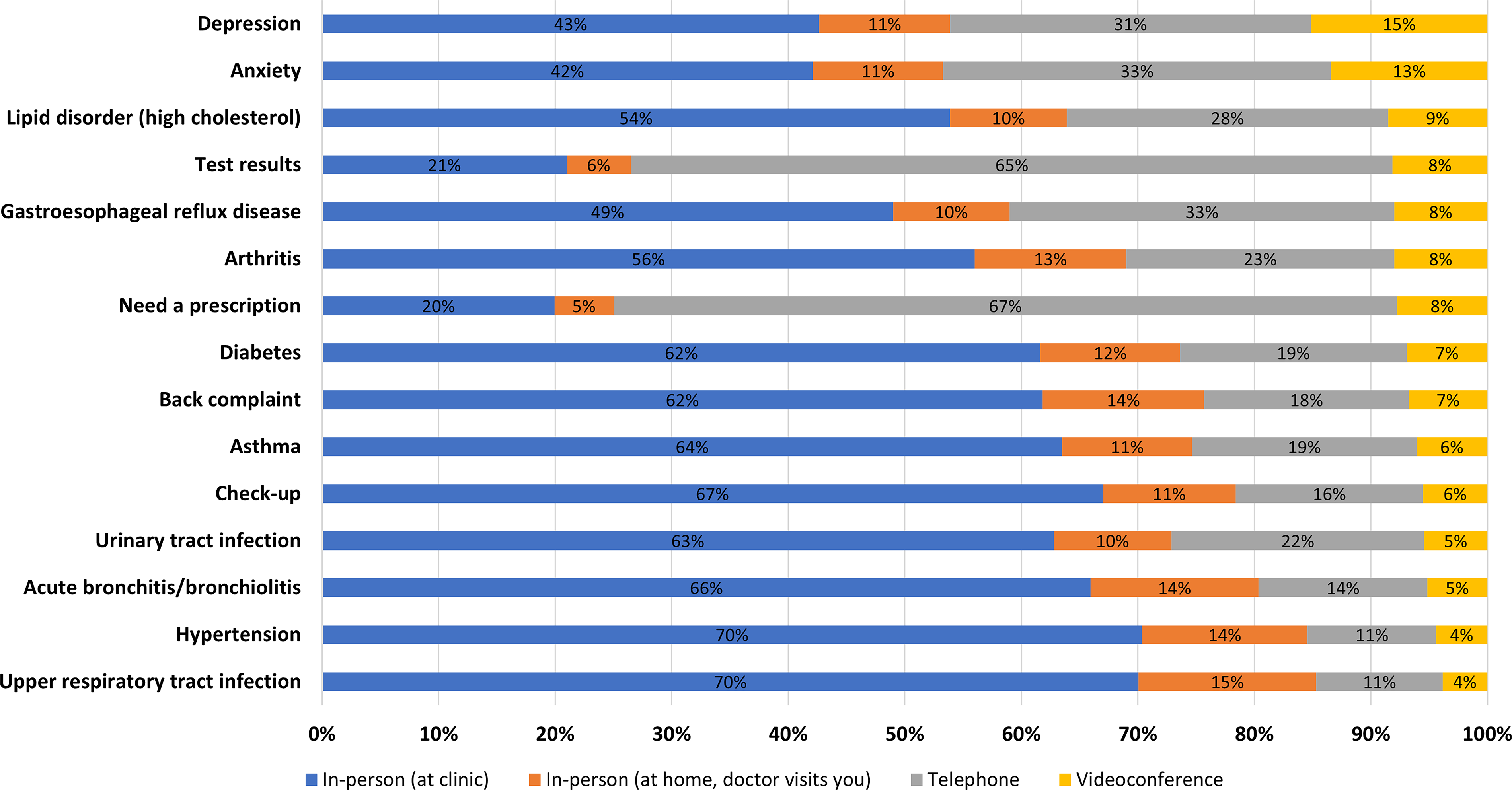
Appointment delivery mode preference for each of the MCRfaGPV.
Data Analysis
Multinomial logistic regression models were used to explore the ability of consumer or appointment characteristics to predict consumer preferences for telephone or video consultations for each of the 15 different MCRfaGPV. A total of 30 regression models were produced (15 MCRfaGPV for each of the two appointment modalities). Analysis was conducted in Stata 17.0. Results from the univariate models were used to determine the predictive ability of each variable prior to building a combined multivariate model. Relative risk ratio (RRR) results from the multivariate analysis were reported along with 95% confidence intervals, p-values, and a brief interpretation. Results for those who selected telephone and those who selected video consultations were reported separately, with further subcategories for each of the 15 reasons for accessing a GP. The RRR for each predictive variable was categorized as either having a positive effect on the likelihood of selecting that modality (telephone or video consultation), a negative effect on the likelihood, an effect that was not statistically significant, or being removed from the model to facilitate convergence (Tables 1 and 2). General trends across the 30 models have been described collectively for each modality, with the full model results provided in the Supplementary Data.
Whether Respondent Characteristics or Experience Increase or Decrease Their Likelihood for Choosing to Have a Telephone Consult for the MCRfaGPV

 Green arrows = statistically significant result where the variable resulted in an increased the likelihood of choosing a telephone consult compared with in-person consult.
Green arrows = statistically significant result where the variable resulted in an increased the likelihood of choosing a telephone consult compared with in-person consult.
 Red arrows = statistically significant result where the variable resulted in increased the likelihood of choosing a telephone consult compared with in-person consult; / = variable had to be removed from the model for it to converge; a blank cell indicates that association was not statistically significant (α of 0.05).
Red arrows = statistically significant result where the variable resulted in increased the likelihood of choosing a telephone consult compared with in-person consult; / = variable had to be removed from the model for it to converge; a blank cell indicates that association was not statistically significant (α of 0.05).
GP, general practitioner; UTI, urinary tract infection.
Whether Respondent Characteristics or Experience Increase or Decrease Their Likelihood for Choosing to Have a

Green arrows = statistically significant result where the variable resulted in an increased the likelihood of choosing a video consult compared with in-person consult.
Red arrows = statistically significant result where the variable resulted in increased the likelihood of choosing a video consult compared with in-person consult; / = variable had to be removed from the model for it to converge; a blank cell indicates that association was not statistically significant (α of 0.05).
GP, general practitioner; UTI, urinary tract infection; VIC, Victoria; NSW, New South Wales; QLD, Queensland; SA, South Australia; WA, Western Australia; NT, Northern Territory; ACT, Australian Capital Territory
Results
A total of 1,069 surveys were completed by consumers representing a range of age, geographic location, and socioeconomic status groups from all states and territories around Australia. 12
APPOINTMENT MODALITY PREFERENCES BY MCRfaGPV
Overall, consumers preferred consultations delivered in-person at a clinic for MCRfaGPV, except when needing a prescription (20%) or test results (21%). In these scenarios, telephone was selected as the preferred modality, with video consultations and at-home visits selected least often ( Fig. 1 ).
DRIVERS FOR TELEPHONE PREFERENCE
Consumers who had had previous telehealth experience were more likely to select telephone over in-person clinic for six of the MCRfaGPV (lipid disorder, asthma, back complaint, depression, check-up and arthritis) ( Table 1 ). Consumers with previous telehealth experience with their own clinician, compared with those who had only received this service in-person, were more likely to select telephone over in-person clinic visits for three of the MCRfaGPV (hypertension, lipid disorder, diabetes). Those who had a previous telehealth appointment with an allied health worker compared with an appointment with a GP were more likely to choose telephone over in-person clinic for four of the MCRfaGPV (lipid disorder, reflux, anxiety, and UTI).
Those who rated the technical quality of their telehealth call as “excellent” compared with “good” were more likely to choose telephone over in-person clinic appointments for five of the MCRfaGPV (lipid disorder, diabetes, reflux, arthritis, and UTI). Consumers who required support of any kind to participate in their telehealth consultation compared with those who did not, were more likely to choose telephone over in-person clinic for six of the MCRfaGPV (upper respiratory, arthritis, check-up, UTI, acute bronchitis, and lipid disorder). Every minute their previous telehealth appointment increased in length decreased the likelihood of consumers selecting telephone over in-person clinic consultation for three of the MCRfaGPV (upper respiratory, UTI, and prescription).
Those with previous video consultation experience (n = 250, 23%) compared with only telephone consultation experience (n = 819, 77%) for a medical appointment were less likely to select telephone over in-person clinic for nine of the MCRfaGPV (lipid disorder, diabetes, reflux, back complaint, depression, anxiety, check-up, arthritis, and test results). Consumers who reported using video consultation software a few times a month compared with never, were less likely to select telephone over in-person clinic for three of the MCRfaGPV (hypertension, asthma, acute bronchitis).
Demographically, there were no clear trends across all the MCRfaGPV for individuals demonstrating preferences for either telephone consults compared with in-person consultations or videoconsultations compared with in-person consultations (details in Supplementary Data).
DRIVERS FOR VIDEOCONSULTATION PREFERENCE
Individuals were most likely to select video consultation over in-person clinic when seeking treatment for anxiety (13%) or depression (15%) (see Fig. 1 ). Of the 15 MCRfaGPV, using general videoconsultation tools a few times a week increased the likelihood that individuals would select video consultation over in-person clinic for eight of the MCRfaGPV (lipid disorder, diabetes, reflux, depression, arthritis, prescription, and test results).
Those who found it difficult to travel to in-person appointments compared with those who did not were more likely to choose video consultations over in-person clinic appointments for three of the MCRfaGPV (reflux, arthritis, and test results).
Consumers were less likely to select video over in-person clinic consultations if their previous telehealth experience was with a specialist compared with a GP, with a mental health clinician compared with a GP, or if they reported needing support to participate in a telehealth appointment or had reasonable internet connection compared with unlimited internet connection.
DIFFERENCES BETWEEN TELEPHONE AND VIDEO CONSULTATION DRIVERS
The type of clinician that consumers engaged with (specialist, allied health, or mental health clinician) in their previous telehealth experience was likely to impact their preference for choosing either telephone or video over in-person clinic consultations. Having previous telehealth experience with a specialist, compared with a GP, negatively impacted the likelihood of selecting either telephone or video over in-person.
Higher ratings of the technical quality of the previous telehealth call were more likely to result in consumers preferring telephone consultations over in-person clinic visits, rather than video consultations over in-person clinic visits. Using videoconference technology at least a few times a month positively impacted consumers to preference video consultations and negatively impacted their preference for telephone, over in-person clinic visits. Needing support to access telehealth services increased the likelihood a consumer would choose telephone compared with video over in-person clinic visits. Age had a significant impact on the likelihood of consumers selecting telephone, but did not have any significant statistical impact on video consultation selection, over in-person. Education levels had a greater impact on the likelihood of selecting telephone compared with video, over in-person. Career selection resulted in a larger number of significant effects on consumers choosing telephone compared with video, over in-person. Income levels and location had some impact on telephone and video selections, over in-person clinic.
Discussion
This study aimed to examine explanatory variables for consumer preferences of either telephone or video consultations compared with in-person services across 15 reasons for visiting a GP. Our findings reveal that there are a variety of reasons why consumers may prefer telephone or video consultations compared with in-person clinics.
General videoconferencing experience in day-to-day life increased the likelihood of consumers choosing video consultations over in-person clinic visits for their GP appointments for eight of the MCRfaGPV, of which five are chronic conditions, and decreased the likelihood of choosing telephone for three of the MCRfaGPV. These findings align with a previous study conducted in Canada and the USA, which found exposure to videoconferencing technology makes it more likely for a consumer to have a positive experience with video consultations.12,16 On the other hand, a lack of access or familiarity with video technology and platforms and the perceived complexity of utilizing this technology have previously been found to contribute to lower preferences for video consultations.2,7,16 Preferences for video consultations for the management of chronic disease among consumers vary. A scoping review of studies found high acceptability and feasibility among consumers using videoconferencing for the management of various chronic conditions across various service providers, where most video consultations were under one hour. 17 In Australia consumers are not routinely offered video consultations when visiting GPs, meaning those needing to regularly visit their GP for chronic condition management sought out telephone consultations in these circumstances. 18 Given chronic conditions are more complex and routinely require longer consultations with more nuanced discussions, video consultations should be offered to consumers, particularly if regular follow-up appointments with their GP are required.
In a recent literature review, results from 79 studies demonstrated that video consultations were consistently superior or equal to telephone consultations for clinical outcomes. 19 However, this is not always reflected in consumer preferences in our study or the findings of others. One example is that consumers in a previous Australian study reportedly preferred telephone consultations over video for the management of chronic kidney disease. 20 It was found that previous telephone consultation experience was associated with increased trust and confidence in future telephone consultations. 20 However, 95% of consumers in this study had received a telephone consultation previously compared with less than one-third of survey respondents who had experienced a video consultation. 20 Numerous studies have shown that once a first video consultation has been experienced, video consultations receive more positive feedback from consumers compared with telephone.11,19,21–25
Our findings also suggest that increased familiarity and comfortability with video consultations may positively influence consumer preferences for video consultations in the future.
This shows that offering videoconferencing as a modality in primary care may increase consumers’ familiarity with this modality and increase their likelihood of choosing video consultations for future appointments. Trust and confidence in telehealth modalities have been associated with increased exposure to telephone consultations, 26 so it can be assumed that preferences for video consultation will change with increased exposure to video consultations. If health providers are looking to increase the number of clients who engage with video consultations, they may like to consider giving consumers the opportunity to do a trial video consultation.
LIMITATIONS AND FUTURE RESEARCH OPPORTUNITIES
Limitations of this study include the fact that the selected sample were all already registered with the Qualtrics® online survey platform, demonstrating that they are likely to have a basic level of familiarity and comfortability with online systems. We acknowledge that the sampling method is likely to have selected individuals who are potentially more technology literature and therefore may have an increased likelihood of accessing telehealth services. This means that consumers with very low access to or comfortability with technology were unlikely to be represented in this survey. It would be helpful in future research to do an offline survey to assess telehealth experiences and preferences for those who do not regularly engage in online platforms. As with any stated preference research, there is always the potential that an individual’s stated preferences will not match their ultimate behavior. Future work should seek to prospectively follow individuals to explore how their preferences relate to the care they choose to access and their eventual health outcomes.
A key limitation pertains to how our results only consider the overall effect direction of significant associations and do not explore the relative size of the effect for each variable. As such, the regression model included all variables of interest, and individual variables were not tested nor identified as confounders (excluding sex, age, and locality) or effect modifiers. Future research could also build on the explorations of this article by exploring further variables that may affect health consumer behavior, like psychological, technological, and contextual factors, like digital literacy and privacy concerns for individuals. In addition, the trends identified here could be explored using a deductive approach by mapping the preferences observed to a framework.
Conclusions
In conclusion, the results from this study provide an overview as to the current perceptions and preferences of Australians regarding telephone versus video consultations for telehealth services. These results demonstrate that consumers select modalities for a range of reasons. This highlights the need to include consumers in decisions regarding how they would like to receive their health care. Further research can expand on specific elements of this survey for a more in-depth analysis of the use of telehealth for particular health needs and service providers.
Authors’ Contributions
This article was conceptualized by C.L.S. and R.M.; data analysis and interpretation were undertaken by C.L.S., R.M., and L.J.N.; article drafting was conducted by C.L.S., R.M., and L.J.N., with critical appraisal and review by all authors.
Footnotes
Ethics Statement
Human research ethics approval was received from The University of Queensland Human Research Ethics Committee (2021/HE002634).
Data Availability Statement
The data that support the findings of this study are not publicly available due to their containing information that could compromise the privacy of research participants but are available from the corresponding author (C.L.S.) if prior ethics approval is received. Access to data regarding model outcomes was not included in this paper due to the size of the models; however, it is available upon request from the corresponding author (C.L.S.).
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
No funding was received for this article.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.