
Abstract
Purpose
: The COVID-19 pandemic disrupted health care worldwide. We evaluated telemedicine utilization in a pediatric surgery ambulatory setting before and during the pandemic to assess its impact on surgical access.
Methods
: We conducted a retrospective single-center cohort study of pediatric surgery ambulatory visits from 2019 to 2021. Visit modality, type, and complexity were collected. Socioeconomic and geographic variables included Community Needs Index (CNI) and United States Department of Agriculture rural–urban continuum codes. Chi-square, t tests, and multivariable logistic regression were performed.
Results
: Among 4,106 visits, monthly volume declined during the pandemic (median 192 vs. 151, p = 0.03), with fewer new patients (26% vs. 30%, p = 0.04). Telemedicine increased (46% vs. 3.6%, p < 0.001), with higher adoption among rural patients (61% vs. 43%, p < 0.001). The proportion of complex visits increased (high complexity: 13–35%, p < 0.001; highest complexity: 1–9%, p < 0.001). In multivariable analysis, utilization increased with rural residence (odds ratios [OR] 1.80, 95% confidence intervals [CI] 1.44–2.25). Utilization was lower among higher-income households (OR 0.90, 95% CI 0.86–0.94) and higher-deprivation communities (CNI OR 0.71, 95% CI 0.61–0.83; all p < 0.001).
Conclusions
: Telemedicine preserved access to pediatric surgical care during the pandemic, with increased use among rural patients. Lower utilization among both higher-income and higher-deprivation groups highlights complex inequities in access.
Introduction
The COVID-19 pandemic exposed and exacerbated longstanding challenges in delivering safe, equitable, and high-quality health care to children across the United States.1,2 In response, hospitals and clinics restricted nonemergent visits, implemented social distancing, and adopted new care delivery models to preserve continuity of care for children in both urban and rural settings. 1 Telemedicine emerged as a critical tool during this period, offering an efficient, cost-effective means of maintaining health care access. While initially deployed as an emergency response, telemedicine holds promise for addressing persistent gaps in health care access, particularly for underserved rural and socioeconomically disadvantaged populations.
However, the rapid expansion of telemedicine also introduced new challenges. Early evidence suggests that, like traditional in-person care, telemedicine utilization may vary across patient populations and may not fully mitigate existing disparities.2–8 Barriers such as limited broadband access, outdated technology, poor-quality video, and limited digital literacy may further exacerbate inequities, disproportionately affecting the underserved. 9
In addition, the pandemic shifted the clinical complexity of telemedicine encounters. Prior to the pandemic, telemedicine was primarily used for lower complexity visits such as routine postoperative follow-up and diagnostic result review, with high levels of provider and patient satisfaction.10,11 However, during the pandemic, telemedicine was increasingly utilized for a broader range of encounter types, including more complex consultations and new patient evaluations, as in-person access was limited. This expansion raised ongoing concerns about whether more complex virtual care might unintentionally exacerbate disparities for socioeconomically disadvantaged and rural patients, particularly if technological or resource barriers limit equitable participation.
Given these evolving patterns of use and persistent concerns regarding equity, we sought to examine telemedicine utilization within a high-volume pediatric surgical program. Specifically, we evaluated telemedicine use among rural and socioeconomically disadvantaged populations and assessed whether the complexity of telemedicine encounters changed during the pandemic. We hypothesized that telemedicine would help sustain access to specialized surgical care for children, particularly those facing the greatest barriers to in-person care.
Methods
STUDY DESIGN AND SETTING
We conducted a retrospective single-center cohort study evaluating telemedicine utilization within the pediatric surgery ambulatory clinic at a tertiary children’s hospital. The clinic serves as the primary pediatric surgical provider for a five-state regional catchment area. The study period spanned June 11, 2019, to June 30, 2021. The study protocol was approved by the Oregon Health & Science University Institutional Review Board with a waiver granted for exempt research involving human subjects (IRB #00022184).
STUDY POPULATION
All pediatric surgery ambulatory visits during the study period were included. Visit-level data were extracted directly from the electronic health record (Epic Health Systems, Verona, WI) and manually reviewed for accuracy.
STUDY PERIOD
The prepandemic period was defined as June 11, 2019, to March 10, 2020. The pandemic period was defined as March 11, 2020 (following the World Health Organization’s declaration of the COVID-19 pandemic), to June 30, 2021.
DATA COLLECTION AND VARIABLES
For each encounter, we collected visit modality (in-person or telemedicine-phone/video), visit type (new or established), and no-show status. Video-based visits were conducted via an Epic-integrated Zoom platform (Zoom Video Communications, San Jose, CA). Patient home zip codes were used to derive county-level rurality and socioeconomic measures.
Rurality was determined using the United States Department of Agriculture (USDA) 2013 Rural–Urban Continuum Codes (RUCC), which classify counties on a 9-point scale where 1 represents “counties in metro areas of 1 million population or more” and 9 represents “completely rural or less than 2,500 urban population and not adjacent to a metro area.” RUCC codes 1–3 were categorized as “metro” counties, and RUCC codes 4 and above as “nonmetro” counties. 12 Socioeconomic status was estimated using median household income based on United States Census Bureau’s 2006–2010 American Community Survey data, linked to the patient’s zip code. The Community Needs Index (CNI) was derived from the 2020 Dignity Health CNI database. The CNI is a composite score that incorporates five socioeconomic indicators contributing to health disparities: income, culture/language, education, housing status, and insurance coverage. CNI scores range from 1.0 to 5.0, with higher scores reflecting greater community need and higher risk for barriers to health care access.13,14
BILLING COMPLEXITY AND CPT CODE ANALYSIS
Billing codes were extracted for all outpatient encounters to assess visit complexity. Current Procedural Terminology (CPT) codes 99202-05 (new patient, variable complexity) and 99212-15 (established patient, variable complexity) were analyzed. The distribution of billing codes was compared between the prepandemic and pandemic periods to evaluate changes in encounter complexity.
STATISTICAL ANALYSIS
Descriptive statistics were used to summarize visit characteristics overall and between study periods. Continuous variables were compared using Student’s t tests, and categorical variables using Chi-square tests. Monthly telemedicine utilization trends were plotted across the entire study period.
A multivariable logistic regression model was constructed to identify independent predictors of telemedicine use. Candidate variables for inclusion in the model were selected a priori and based on data availability and clinical relevance, including pandemic period (prepandemic vs. pandemic), rural residence (metro vs. nonmetro), median household income, and CNI. Because both income and CNI reflect socioeconomic status, collinearity was assessed. Model results are reported as odds ratios (OR) with 95% confidence intervals (CI). To enhance interpretability, household income was scaled in increments of $5,000, such that the OR represents the effect of a $5,000 increase in income. Statistical significance was defined as p < 0.05. All analyses were performed using STATA version 18.5 (StataCorp LLC, College Station, TX).
Results
ENCOUNTER CHARACTERISTICS
A total of 4,106 pediatric surgery outpatient encounters were analyzed, including 1,746 prepandemic (June 11, 2019, to March 10, 2020) and 2,360 during the pandemic (March 11, 2020, to June 30, 2021). All encounters had complete data. As shown in Table 1, median monthly visit volume declined significantly during the pandemic, from 192 (interquartile range [IQR] 156–202) to 151 visits per month (IQR 112–185, p = 0.03).
Visit Characteristics Before and During Covid

IQR, interquartile range; RUCC, Rural–Urban Continuum Codes; CNI, Community Needs Index; SD, standard deviation.
TELEMEDICINE UTILIZATION
Telemedicine use rose sharply, from 3.6% of visits prepandemic to 46% during the pandemic (p < 0.001), increasing abruptly after March 2020 and remaining persistently elevated throughout the study period (Fig. 1). Among all telemedicine encounters (video and telephone), video visits accounted for the majority before and during the pandemic (76% vs. 55%, respectively). In-person visit volume declined from 96% prepandemic to 54% during the pandemic (p < 0.001). The proportion of new patient visits also fell during the pandemic (26% vs. 30% prepandemic, p = 0.04) (Table 1).
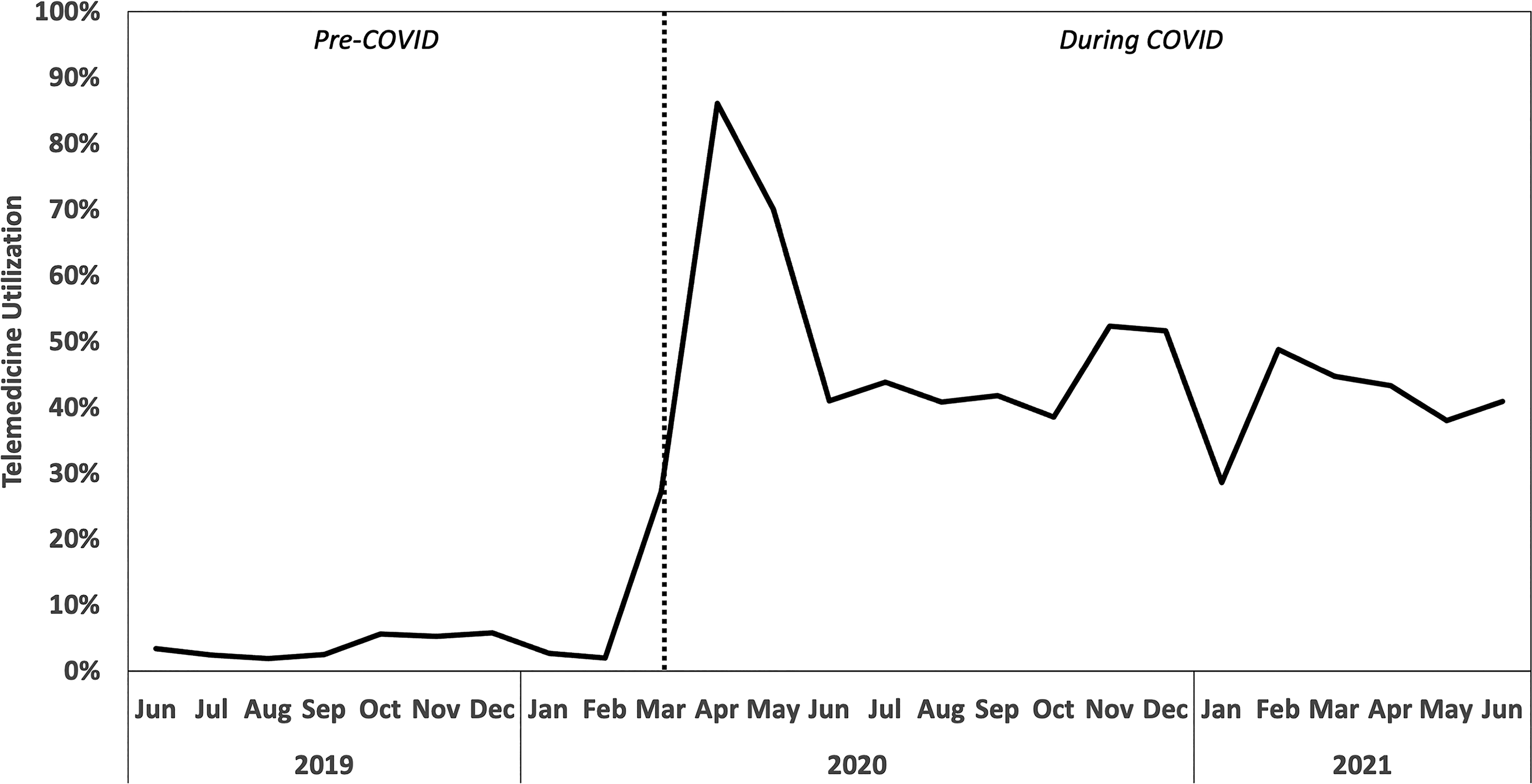
Trend in telemedicine utilization before and during COVID-19 pandemic. Monthly telemedicine utilization from June 2019 to June 2021, demonstrating a sharp increase following the onset of the COVID-19 pandemic (vertical dashed line). Utilization remained elevated throughout the pandemic period compared with the prepandemic baseline.
No-show rates were stable overall (6.2% prepandemic vs. 6.5% during the pandemic, p = 0.76). Prepandemic, telemedicine no-shows were higher than in-person (13.0% vs. 6.0%, p = 0.08), but during the pandemic this difference narrowed (telemedicine 8.8% vs. in-person 2.5%, p = 0.31) (Table 1).
RURAL–URBAN TELEMEDICINE UTILIZATION
Both rural and metropolitan patients increased telemedicine use during the pandemic, though rural patients showed the larger absolute increase (Fig. 2). Among rural patients, telemedicine utilization rose from 5.5% prepandemic to 61% during the pandemic (p < 0.001), while among metropolitan patients, utilization increased from 3.3% to 43% (p < 0.001) (Fig. 3). The proportion of rural and metropolitan patients remained stable between the two time periods (p = 0.32; Table 1, Fig. 2).
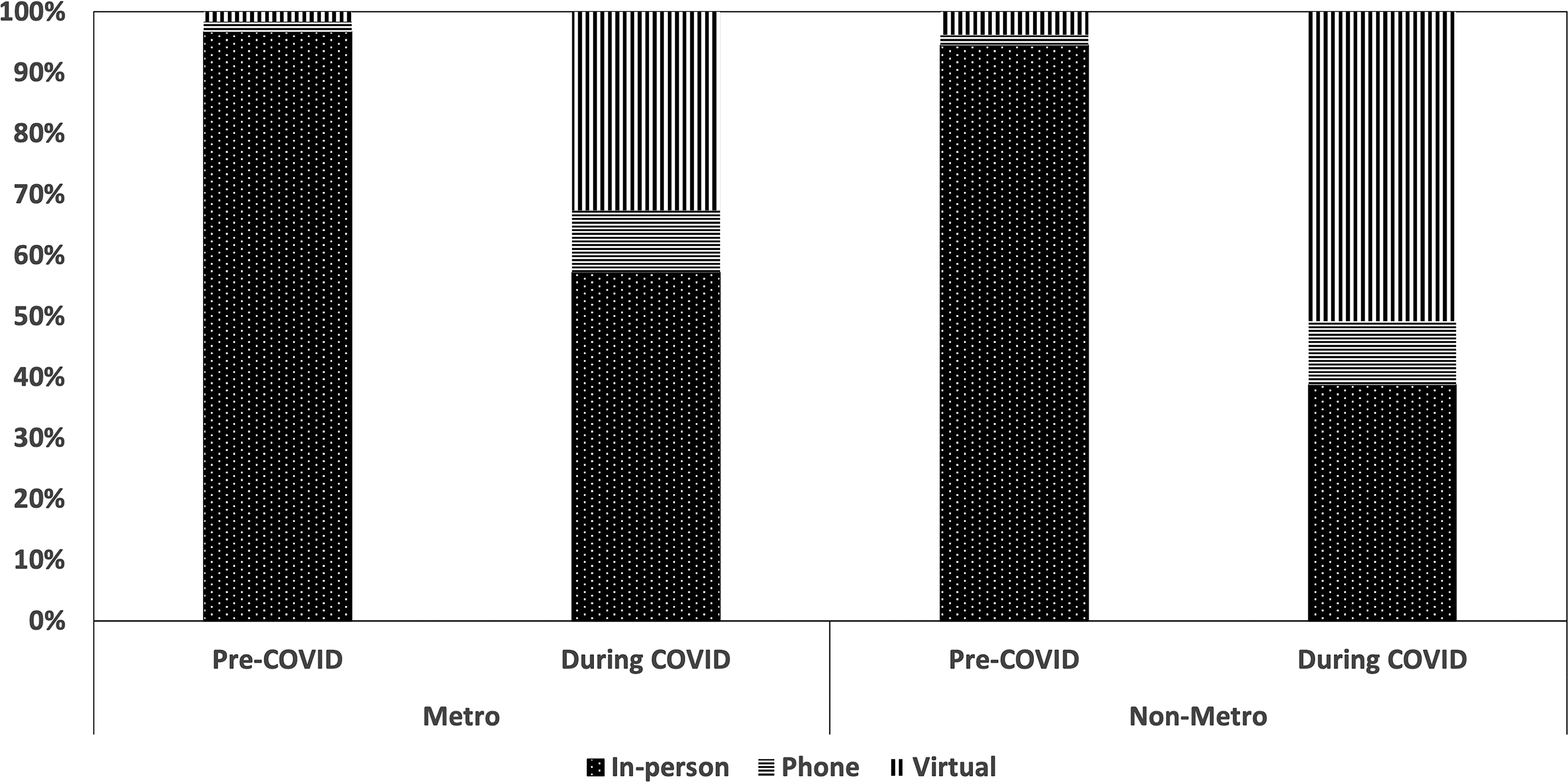
Telemedicine use by geography and pandemic period. Stacked bar chart showing the distribution of visit modality (in-person, phone, virtual) stratified by metropolitan (metro) and nonmetropolitan (nonmetro) patients before and during the COVID-19 pandemic. Telemedicine utilization increased during the pandemic for both groups, with higher adoption observed in nonmetropolitan patients. The composition of telemedicine visits also differed, with a greater proportion of phone visits among nonmetropolitan patients.
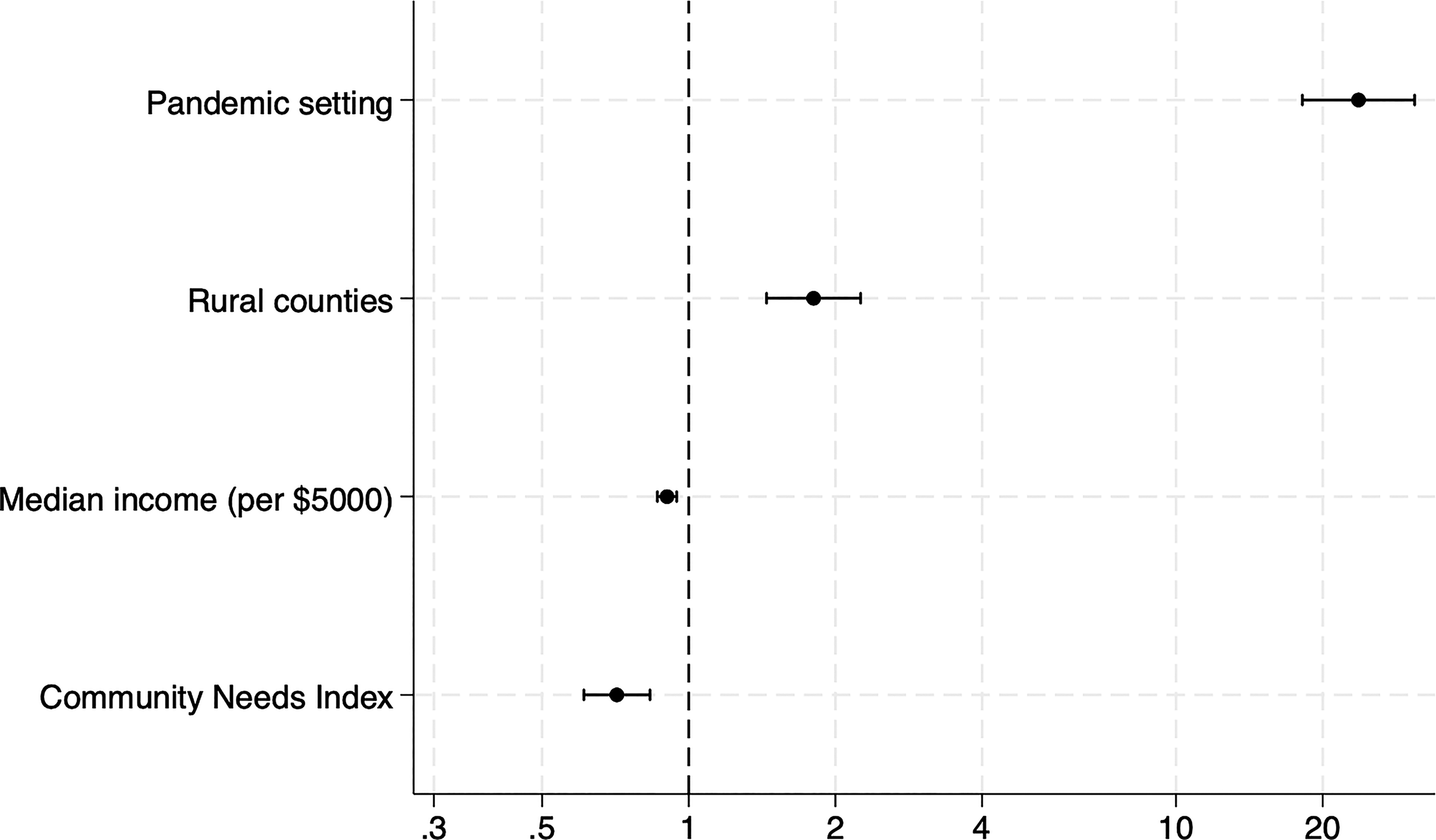
Adjusted odds ratios for factors associated with telemedicine utilization. Forest plot displaying adjusted odds ratios (OR) with 95% confidence intervals (CI) for predictors of telemedicine utilization from multivariable logistic regression. Covariates included pandemic period (pandemic setting), rural residence (rural counties), median household income (per $5,000), and Community Needs Index (CNI).
SOCIOECONOMIC STATUS
Socioeconomic measures did not differ significantly between periods. Household income, calculated as the mean of zip-code-level median household incomes, was $52,2071.12 (standard deviation [SD] $13,308.40) prepandemic and $52,277.57 (SD $12,771.47) during the pandemic (p = 0.62). Mean CNI scores were likewise unchanged (3.21 [SD 0.68] prepandemic vs. 3.21 [SD 0.71] pandemic; p = 0.75) (Table 1).
PREDICTORS OF TELEMEDICINE UTILIZATION
Multivariable logistic regression showed that the odds of telemedicine use were markedly higher during the pandemic (OR 23.69, 95% CI 18.17–30.88, p < 0.001) and among rural patients (OR 1.80, 95% CI 1.44–2.25, p < 0.001). Odds of telemedicine use decreased with higher household income, falling 10% for each $5,000 increase (OR 0.90, 95% CI 0.86–0.94, p < 0.001). Interestingly, odds also decreased with greater socioeconomic deprivation, declining 29% for each one-unit increase in CNI (OR 0.71 per unit increase, 95% CI 0.61–0.83, p < 0.001). Pearson correlation coefficient demonstrated moderate inverse correlation between CNI and income (−0.7, p < 0.001). However, variance inflation factor (VIF) values remained within acceptable limits (median income VIF = 2.17; CNI VIF = 1.99), supporting inclusion of both variables in the final model.
BILLING COMPLEXITY
Billing complexity, assessed by CPT distribution for both new (99202–99205) and established (99212–99215) patient encounters demonstrated stability in low-complexity encounters (p = 0.66). However, there was a significant shift in distribution across higher complexity visits. The relative proportion of moderate complexity visits declined (67% prepandemic to 43% during pandemic, p < 0.001), while the high and highest complexity visits increased significantly during the pandemic (high complexity: 13–35%, p < 0.001; highest complexity: 1–9%, p < 0.001).
Discussion
This retrospective cohort study highlights the pivotal role telemedicine played in preserving access to pediatric surgical care during the COVID-19 pandemic. Telemedicine use increased sharply and remained elevated throughout the study period. In multivariable analyses, odds of telemedicine use were higher among rural patients but lower for children from communities with greater socioeconomic deprivation, as measured by the CNI. Odds also declined with higher household income, indicating a complex relationship between socioeconomic factors and telemedicine utilization in our pediatric surgery population.
The rapid expansion of telemedicine during the pandemic has been well documented across medical and surgical specialties, including pediatric surgery.15,16 Virtual consultations reduce travel time and lost wages, lower hospital overhead, and maintain high levels of provider satisfaction. 17 At our institution, telemedicine adoption peaked at approximately 85% of visits early in the pandemic and stabilized at 30–50% of visits thereafter, higher than reported rates nationally. 18 We also observed an increased proportion of high-complexity patients managed via telemedicine. This success was likely facilitated by telemedicine infrastructure that was already in place prior to the pandemic, provider familiarity with virtual care, and the longstanding need to serve a large rural catchment area where families face substantial travel burdens.
One of our central findings was a high adoption of telemedicine by rural communities. Rural children demonstrated a greater absolute increase in telemedicine use compared with metropolitan patients, and rural residence remained an independent predictor of telemedicine use in multivariable analysis adjusting for covariates. As the primary surgical referral center for the state, we care for children from rural communities who face substantial barriers to specialty care. These barriers include financial strain from travel, higher rates of uninsurance, greater disease severity, and worse outcomes for common surgical conditions. 19 Telemedicine has long been recognized as a strategy to overcome geographic barriers, and our findings align with prior studies showing its potential to expand access for rural children. 20 Several factors facilitated rural uptake at our institution, including a flexible platform that allowed both video and audio-only visits and active promotion of these services.
Socioeconomic factors were also independently associated with telemedicine utilization. In multivariable analyses, higher household income was associated with lower odds of telemedicine utilization (OR 0.90, 95% CI 0.86–0.94), but community-level disadvantage, measured by CNI, was associated with lower telemedicine use (OR 0.71, 95% CI 0.61–0.83). Unlike household income, which reflects financial resources alone, the CNI is a composite index incorporating multiple social determinants of health, including income, education, language and cultural barriers, insurance coverage, and housing. 13 These broader community-level factors may explain why children with high CNI were less likely to access telemedicine, reflecting structural barriers such as limited broadband availability, unstable housing, or lack of digital literacy.
These findings contribute to a growing but mixed body of literature on socioeconomic disparities in pediatric surgical telemedicine access. A single-institution study of 9,149 pediatric surgery visits found that telemedicine utilization was less likely among patients who were publicly insured, lived closer to clinic, resided in disadvantaged neighborhoods (measured by Area Deprivation Index [ADI]), or were not white. 18 A larger study of 109,601 pediatric outpatient surgical care visits similarly reported lower utilization among Spanish-speaking, publicly insured, and nonwhite patients but identified higher odds of telemedicine visit completion among patients with higher Social Deprivation Index (SDI) scores (OR 1.41, 95% CI 1.27–1.58). 21 Collectively, these findings demonstrate substantial variability in which, and how, socioeconomic factors influence telemedicine use. Differences across studies likely reflect variation in how socioeconomic disadvantage is measured (household income vs. community indices such as CNI, ADI, or SDI), as well as differences in patient populations, institutional infrastructure, state-level telehealth policies, telemedicine platform flexibility (video-only vs. video and phone), and interpreter availability. This inconsistency highlights that the impact of telemedicine depends on the populations served and underscores the need for equity-focused approaches tailored to community context.
Limitations
This study has several limitations. The retrospective design limits our ability to establish causality, though our data demonstrate a substantial increase in telemedicine utilization, particularly among rural and low-income families. As a single-center study, our findings may not be generalizable to all institutions; however, many children’s hospitals face similar challenges in providing equitable surgical care across large and geographically diverse catchment areas. 22 Our measures of socioeconomic status were based on zip code-level income, census data, and the CNI, which may not fully capture household-level financial hardship or more nuanced aspects of social determinants of health. Categories based on socioeconomic status and rurality were by necessity based on historical indexes and may not accurately reflect current population metrics during the study period. In addition, we were unable to include variables such as race, ethnicity, language, insurance status, and age, which may further influence telemedicine utilization patterns and deserve further investigation.
Conclusions
The COVID-19 pandemic accelerated the widespread adoption of telemedicine in pediatric surgical care. Our findings suggest that telemedicine can serve as an important tool to expand access for children from rural areas and lower-income families who traditionally face barriers to in-person specialty care. However, we also identified persistent challenges for patients living in highly disadvantaged communities, highlighting that community-level disparities may continue to limit telemedicine adoption despite broader availability. While challenges remain, particularly related to digital infrastructure and equitable technology access, telemedicine appears likely to remain an integral component of pediatric surgical care delivery beyond the pandemic.
Authors’ Contributions
L.S., X.-Y.H., C.R.V., K.K., D.N., V.N., J.P.M., and M.J.: Conceptualization. L.S. and X.-Y.H.: Data curation. X.-Y.H., J.P.M., and M.J.: Funding acquisition. X.-Y.H., K.K., and D.N.: Investigation. L.S., X.-Y.H., C.R.V., V.N., J.P., and M.J.: Methodology. L.S., X.-Y.H., J.P.M., and M.J.: Project administration. L.S., X.-Y.H.: Software. V.N., J.P.M., and M.J.: Supervision. L.S., X.-Y.H., J.P.M., and M.J.: Validation. L.S., X.-Y.H., C.R.V.: Visualization. L.S., C.R.V., X.-Y.H., K.K., D.N., V.N., J.P.M., and M.J.: Writing—original draft. L.S., C.R.V., X.-Y.H., E.B., K.K., D.N., V.N., J.P.M., and M.J.: Writing—review and editing.
Footnotes
Author Disclosure Statement
No conflicts of interest.
Funding Information
This study was partially funded by the Western Regional Alliance for Pediatric Emergency Management (WRAP-EM) Consortium. WRAP-EM is generously funded by the Office of the Assistant Secretary for Preparedness and Response (ASPR, U3REP190616-01).
Data Availability
The data that support the findings of this study are not openly available due to reasons of sensitivity and are available from the corresponding author upon reasonable request. Data are located in controlled access data storage at Oregon Health & Science University.