
Abstract
Introduction:
The rapid expansion of telehealth, particularly during the COVID-19 pandemic, accelerated the development of technology-mediated movement interventions to support physical and psychological health. Among these, tele-dance interventions (TDI) emerged as accessible and scalable models of care; however, a comprehensive synthesis of the evidence supporting these interventions remains limited. This scoping review maps existing literature on the feasibility, acceptability, and health-related outcomes of TDI across diverse populations.
Methods:
Guided by Arksey and O’Malley’s framework and Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews guidelines, we conducted a systematic search of 6 electronic databases and identified 26 eligible studies employing quantitative, qualitative, or mixed-methods designs. Methodological quality was appraised using the Mixed Methods Appraisal Tool. All interventions were delivered synchronously via videoconferencing platforms and were primarily adapted from established in-person dance programs, typically incorporating warm-up activities, structured or improvisational movement, and cool-down phases.
Results:
Across studies, TDI were consistently feasible and well accepted among older adults, individuals with neurological conditions, and people living with chronic illness. Psychosocial benefits, including enhanced social connection, improved mood, and reduced loneliness, were commonly reported. Physical outcomes such as improvements in balance, gait, and strength were also observed, suggesting potential functional benefits relevant to rehabilitation and health promotion.
Conclusion:
TDI offer important advantages, including increased accessibility, flexible delivery formats, and scalability beyond in-person care. However, limitations include methodological heterogeneity, small sample sizes, underrepresentation of diverse populations, and limited long-term follow-up. Overall, TDI represent a promising telehealth modality, warranting future research emphasizing methodological rigor, inclusive design, hybrid delivery models, and implementation-focused evaluations.
Introduction
Dance has long been recognized as a powerful, multifaceted modality that advances physical and psychological well-being across the lifespan. As both artistic expression and purposeful physical activity, it blends aerobic and anaerobic exertion, rhythm and musicality, creativity and improvisation, and inherently social interaction, offering a distinctive route to health promotion.1,2 Within this broad umbrella, therapeutic dance refers to structured or improvisational movement practices drawn from varied dance styles to support physical wellness and emotional expression, whereas dance/movement therapy (DMT) is a psychotherapeutic modality that intentionally harnesses movement, creative process, and the therapist–client relationship to meet clinical goals. 3
Accumulating evidence shows that dance can enhance psychomotor functioning,4,5 elevate mood, and reduce distress, 6 support cognitive processes such as attention and executive function, 7 and improve overall quality of life. 8 These benefits have been reported across clinical and nonclinical groups, including people living with Parkinson’s Disease (PD), cancer, and age-related decline,9,10 as well as children and adolescents, for whom dance has been associated with gains in physical health (e.g., cardiovascular fitness, bone health) and psychosocial well-being (e.g., reduced anxiety and improved body image).11–13 Meta-analytic work further indicates that dance is at least as effective as, and sometimes superior to, structured exercise programs on a range of health outcomes, 14 underscoring its promise as a whole-person intervention.
Historically, most dance programs have been delivered in person, either individually or in groups. Yet the rapid expansion of digital technologies—accelerated by the COVID-19 pandemic—has pushed many health-promoting and arts-based interventions online.15–18 For dance specifically, synchronous (live, interactive) delivery is especially salient: the art form relies on moment-to-moment attunement, shared rhythm, mirroring, and immediate feedback, elements that asynchronous or purely self-guided formats may only partially capture. At the same time, tele-delivery can mitigate longstanding barriers to participation, such as transportation challenges, geographic isolation, scheduling constraints, or mobility limitations—factors that disproportionately affect older adults and those with chronic conditions. Prior telehealth research suggests that real-time, supported digital interventions can achieve high adherence and outcomes comparable with face-to-face care.19–22
Despite this momentum, most reviews of telehealth-supported physical activity still center on generalized exercise or fitness programs,23,24 leaving a gap in our understanding of how dance—an embodied, relational, and expressive modality—translates to live digital environments. Furthermore, the effectiveness of synchronously delivered telehealth dance interventions remains largely unexamined. Given the inherently embodied and relational nature of dance—an art form that is moment-to-moment, ephemeral, and deeply rooted in shared presence and interpersonal connection—real-time interaction may be particularly critical to preserving the therapeutic and expressive qualities of dance in virtual formats. Moreover, the field lacks an integrated picture of who is being served by tele-dance interventions (TDI), how interventions are being delivered (e.g., platforms, formats, facilitator types), what outcomes are being measured (e.g., physical, psychosocial, feasibility), and with what quality the studies are conducted. Questions about feasibility (e.g., technology barriers, adherence), acceptability (e.g., satisfaction, preference for online vs. in-person), safety, and long-term sustainability also remain underexplored—particularly outside the exceptional context of pandemic-related restrictions. To address these gaps, this scoping review synthesizes emerging literature on TDI aimed at promoting physical and/or psychosocial health.
Guided by Arksey and O’Malley’s framework 15 and reported according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR), 25 we mapped the characteristics of interventions (populations, settings, delivery methods, components), summarized feasibility and acceptability findings (including adherence, safety, and technology issues), and described reported physical and psychosocial outcomes. We included quantitative, qualitative, and mixed-methods studies to capture the breadth of evidence and illuminate how different methodological traditions have approached tele-dance. Finally, we identified methodological limitations, conceptual and practical gaps, and directions for future research, such as hybrid delivery models that integrate the accessibility of telehealth with the embodied richness of in-person dance.
Methods
DEFINITION
For this review, we defined TDI as any dance program, encompassing a variety of styles, delivered remotely in a synchronous manner. This delivery occurs between a patient or client and a dance intervention provider through a digital technology platform that facilitates live streaming or interactive communication.
SEARCH STRATEGY
The research team conducted a multi-stage systematic literature search following PRISMA-ScR guidelines. The initial search strategy was developed in consultation with a research librarian (SP) and conducted in March 2022 across six databases: PubMed, Scopus, Web of Science, IEEE Xplore, ACM Digital Library, and SPORTDiscus. Searches were limited to English-language publications. Search terms combined concepts related to dance and movement-based practices with technology-mediated or remote delivery, including: (dance OR ballet OR zumba OR flamenco OR tango OR “creative movement” OR “dance movement therapy” OR “dance therapy” OR five rhythms OR hip-hop OR breakdancing)* AND (technology OR virtual OR “remote delivery” OR computer OR digital OR “video conference*” OR video OR online OR telehealth OR synchronous OR telemedicine OR “internet-based” OR tele* OR Zoom OR Skype)*. The search strategy was translated and adapted for each database to accommodate differences in controlled vocabulary and syntax. Reference lists of key articles were also manually screened.
The initial search identified nine eligible studies, which were considered limited given the rapid expansion of telehealth research during and following the COVID-19 pandemic. Therefore, the identical search strategy was repeated in July 2024, with updated syntax where applicable and date limits applied from April 2022 to July 2024. This updated search yielded 16 additional eligible studies. To ensure the currency of the evidence, a final supplementary search was conducted in December 2024, identifying one additional eligible study.
Records from all search stages were pooled and deduplicated prior to screening. Titles and abstracts were screened for relevance, followed by full-text review using consistent eligibility criteria across all search waves. Screening, full-text review, data extraction, and methodological appraisal for newly identified records were conducted using the same procedures established in 2022. In total, 26 studies met the inclusion criteria and were included in the final scoping review.
SELECTION OF ARTICLES
Articles were eligible if they met the following criteria: written in English; reported primary research using quantitative, qualitative, or mixed-methods designs; and described a telehealth-based dance intervention aimed at promoting physical and/or psychosocial health outcomes. No restrictions were placed on the dance genre. To ensure a minimum evidentiary standard, only primary studies published in peer-reviewed journals were included.
We excluded articles that: (a) examined dance interventions delivered exclusively through asynchronous methods (e.g., prerecorded videos such as YouTube classes); (b) focused solely on online or video game–based movement without human facilitation (e.g., Dance Dance Revolution, Wii Fit); (c) described technical or professional dance training rather than health-related interventions; or (d) provided only anecdotal descriptions without empirical analysis of outcomes. After removing duplicates, two reviewers independently screened titles and abstracts for relevance. Full texts of potentially eligible studies were then assessed against the predefined criteria to determine final inclusion.
DATA EXTRACTION
All data were reviewed and extracted by two reviewers in a standardized manner using a purposefully designed template. The following data were extracted from the studies: first author, year of publication, country, study design, study population (sample size, age, gender), intervention characteristics (duration, frequency, intervention components, dance style, delivery platform, and control/comparison group), all outcomes measured, and key findings. Extracted data were checked by the first author, and any disagreements were resolved by discussion and consensus. Data were descriptively analyzed and presented narratively in relation to the review questions.
ASSESSMENT OF METHODOLOGICAL QUALITY
The methodological quality of the included studies was assessed using criteria adapted from the Mixed Methods Appraisal Tool (MMAT), 26 which is designed for use in systematic reviews incorporating qualitative (QUAL), quantitative (QUAN), and mixed-methods (MM) studies. The MMAT includes design-specific criteria for QUAL, QUAN randomized controlled trials (RCTs), QUAN nonrandomized studies, and MM designs, enabling appraisal of methodological features relevant to each study type.
Each criterion was independently rated by two reviewers as “yes,” “no,” or “unclear.” Consistent with common practice, one point was assigned only when both reviewers rated a criterion as “yes.” Although the MMAT developers advise caution in generating overall numeric scores, summary ratings were used in this review to facilitate comparison across studies. Given the absence of a definitive cutoff, we classified quality into three levels for descriptive purposes: low (1–2), medium (3–4), and high (5).
ANALYSIS AND SYNTHESIS OF THE RESULTS
The included studies were classified as QUAL, QUAN, or MM by three reviewers, based on the study design identified by the study authors and on the nature of the findings. 27
Results
STUDY SELECTION AND CHARACTERISTICS
The first two searches via databases identified 6,548 studies. After duplicates were removed, the resulting 2,821 citations were screened by reviewing their titles and abstracts. A total of 2,708 citations were excluded, resulting in 113 citations potentially meeting eligibility criteria. A total of three reports were sought for retrieval. Of these, 112 full texts were obtained and reviewed, while one could not be retrieved. After reviewing the full-text articles, 87 studies were further excluded. Articles were reviewed but excluded for reasons such as: being in-person rather than tele-based; not involving a dance intervention; utilizing video game or VR platforms; focusing on general fitness programs; targeting dance technique improvement rather than health outcomes; being review articles; employing asynchronous delivery formats; or primarily reporting process evaluations. The third search, conducted in December 2024, identified one additional study. Across all searches, 26 articles published between 2016 and 2024 were included in the final analysis, representing a total sample size of 942 participants. The overall study selection process is depicted in the PRISMA flow diagram ( Fig. 1 ).

PRISMA flowchart. PRISMA, Preferred Reporting Items for Systematic reviews and Meta-Analyses.
OVERVIEW OF INCLUDED STUDIES
Table 1 summarizes the characteristics of the 26 TDI studies included in this review. Fourteen employed QUAN designs (54%), five were QUAL (19%), and seven used MM approaches (27%). Among QUAN studies, four were RCTs, six were nonrandomized, and four were descriptive. Most QUAL studies utilized thematic analysis,32,34,36,52 with the exception of Shim et al., 48 which adopted a framework analysis approach. MM studies primarily used single-group pre–post designs, except for Seidler et al., 47 which employed a two-arm quasi-experimental design comparing in-person and telehealth delivery formats. Humphries et al. 37 and Rugh et al. 46 shared a common study protocol but investigated distinct research questions. Studies were primarily conducted in the United States (n = 9), followed by the United Kingdom (n = 4), Australia (n = 3), Canada (n = 3), Brazil (n = 2), and one study each from Germany, Denmark, India, Japan, and Sweden.
General Characteristics and the Intervention Components of the Included Studies
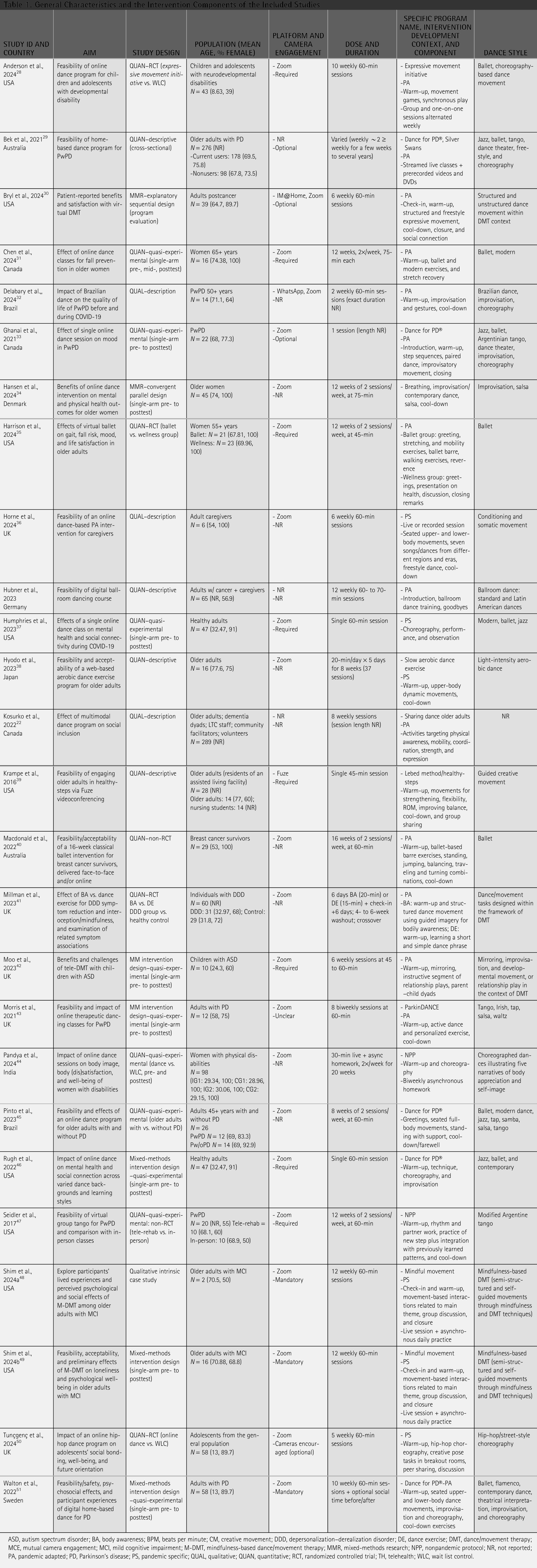
ASD, autism spectrum disorder; BA, body awareness; BPM, beats per minute; CM, creative movement; DDD, depersonalization–derealization disorder; DE, dance exercise; DMT, dance/movement therapy; MCE, mutual camera engagement; MCI, mild cognitive impairment; M-DMT, mindfulness-based dance/movement therapy; MMR, mixed-methods research; NPP, nonpandemic protocol; NR, not reported; PA, pandemic adapted; PD, Parkinson’s disease; PS, pandemic specific; QUAL, qualitative; QUAN, quantitative; RCT, randomized controlled trial; TH, telehealth; WLC, wait list control.
Publication trends indicate a gradual increase in TDI studies before 2020, followed by a sharp rise during and after the COVID-19 pandemic, culminating in peak publication activity in 2024 ( Fig. 2 ).
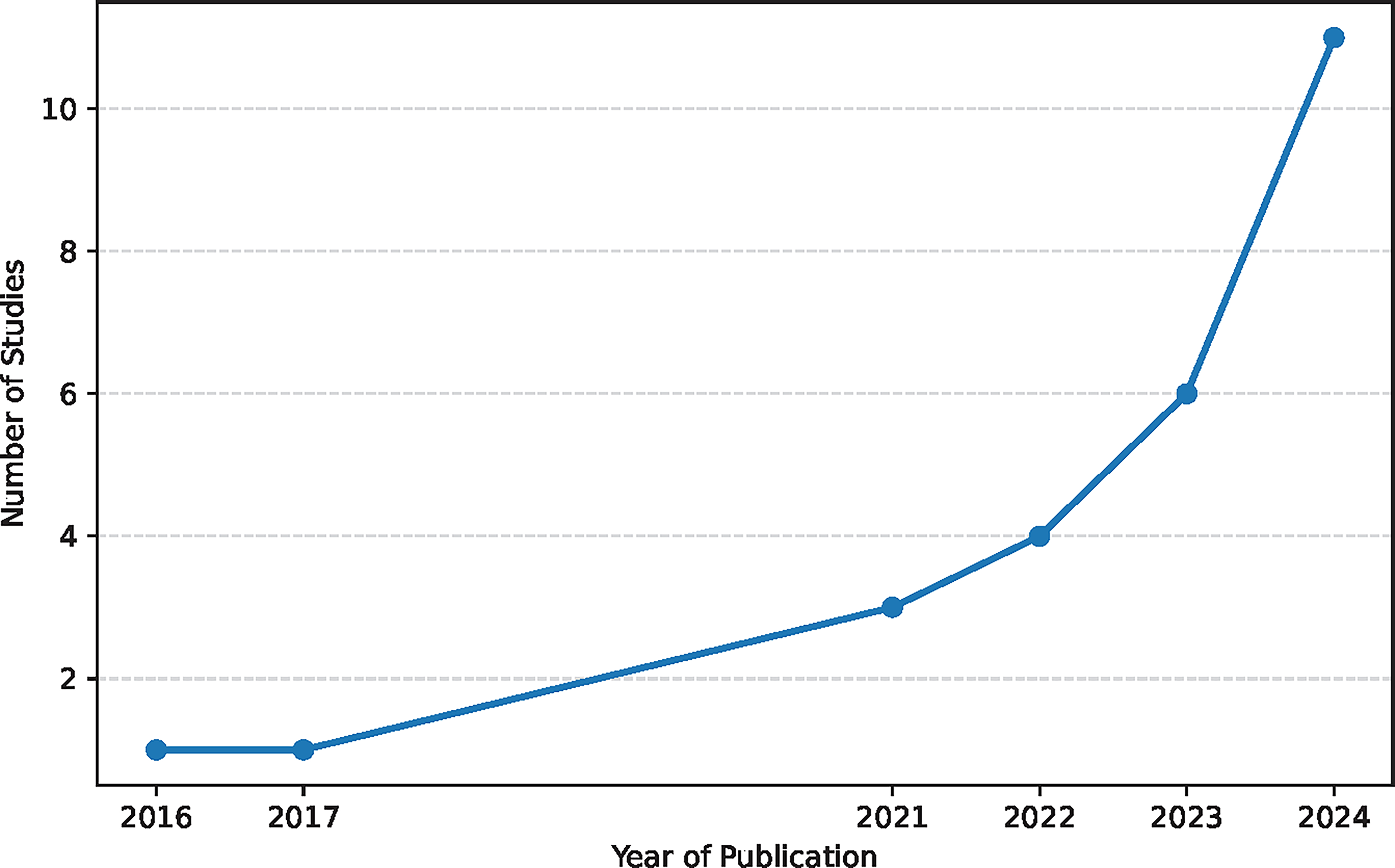
Number of Studies by Year.
STUDY POPULATIONS
Studies represented diverse populations across the lifespan ( Fig. 3 ): 14 studies (54%) included individuals with neurological or age-related cognitive conditions, 7 of which focused specifically on Parkinson’s disease. Five studies (19%) involved healthy older adults, three (12%) targeted individuals affected by cancer, and four (15%) focused on healthy adults. Three studies (12%) examined children or adolescents, including those with autism or developmental disabilities, and adolescents participating in an online group dance program. The remaining studies addressed women with physical disabilities, adult caregivers, and adults with depersonalization–derealization disorder.

Participant Populations.
Participant ages spanned from early childhood to older adulthood (mean ages 8.6–77.6 years), although most studies (approximately 85%) focused on adult or older adult populations. Among the 24 studies reporting gender, participants were predominantly female (median 73%). Sample sizes ranged from 2 participants to 289. Ten studies (38%) did not report participants’ race or ethnicity. Nearly three-quarters of the studies (73%) were conducted during the COVID-19 pandemic, contextualizing the prominence of remote delivery approaches.
INTERVENTION SETTINGS AND DELIVERY FORMATS
Most interventions (92%) were delivered in group-based formats, often emphasizing collective movement, social engagement, and shared expressive experience. Only a small number of studies incorporated individual or dyadic components to accommodate specific populations (e.g., children with autism or developmental disabilities). Across studies, group delivery remained the predominant format regardless of age group, clinical condition, or dance genre. Four studies (15%) offered single-session interventions, whereas the remainder implemented multiweek programs lasting between 6 and 20 weeks. Interventions were primarily led by dance instructors or multidisciplinary teams, and five studies (19%) explicitly identified credentialed dance/movement therapists as facilitators or framed the program as DMT-based.
DANCE PROGRAM CHARACTERISTICS BY POPULATION
Dance program structures varied based on the target population and intervention goals. Programs for older adults incorporated ballet, modern dance, aerobic movement, improvisational tasks, and mindfulness-based DMT. Session lengths ranged from brief 20-minute daily practices to biweekly 75-min classes delivered over 12 weeks, reflecting wide flexibility in dosing and structure. Programs for individuals with PD frequently adapted the Dance for PD® curriculum, integrating warm-ups, choreographed sequences, improvisation, and expressive movement. Session durations varied from single 20-min introductory classes to twice-weekly 60-minute sessions delivered over extended periods ranging from 6 weeks to 12 months.
Cancer-focused programs employed either ballet or DMT-based frameworks, emphasizing gentle movement, expression, and embodied coping. These programs typically involved 45- to 75-min sessions delivered once or twice weekly across 6–16 weeks. Interventions for individuals with other clinical conditions, such as neurological or psychological disorders, similarly integrated expressive movement, structured choreography, and mindfulness-informed practices. Programs involving children, adolescents, and individuals with developmental disabilities emphasized attunement, mirroring, playful movement exploration, and structured or semi-structured choreography to support social engagement and communication. These interventions were generally offered once weekly for 6–10 weeks, with session lengths of 45–60 min and occasional use of individual or dyadic formats to accommodate participant needs.
Finally, programs for women with physical disabilities employed choreographic narratives and expressive movement themes within 60-min, twice-weekly sessions delivered over 20 weeks. Across all populations, session content commonly combined structured dance elements (e.g., warm-ups, choreography, technique-based sequences) with improvisation, creative tasks, and group reflection.
DELIVERY PLATFORMS AND SETTING
Zoom was the dominant delivery platform (88%), with Fuze and Acrobat Connect each used once, while three studies (12%) did not specify the platform. Six studies (23%) employed multimodal delivery, combining live-streamed and prerecorded content with in-person interactive components. Intervention settings included at-home participation, residential facilities with remote instruction, and hybrid arrangements in which participants gathered in shared physical spaces with remote facilitation. Camera-use policies varied: 11 studies (42%) required cameras to remain on, 2 studies (8%) explicitly permitted optional camera use, and the remaining studies (50%) did not specify their expectations.
DATA COLLECTION METHODS
Across the included studies, quantitative data were obtained using standardized self-report instruments (n = 8), study-specific questionnaires (n = 5), and structured logs (n = 12). Physical performance data were collected in six studies31,34,35,40,47,51 through objective assessments such as gait velocity, sit-to-stand tests, 6-minute walk tests, and upper-limb mobility measures. Twelve studies administered validated mental health and psychosocial questionnaires. Qualitative data were collected through interviews, focus groups, and open-ended survey responses, allowing for exploration of participants’ subjective experiences.
STUDY OUTCOMES AND FINDINGS
The studies evaluated a diverse array of outcomes, including feasibility and acceptability of TDI, physical and cognitive functioning, and psychosocial benefits ( Table 2 ). Below are summarized results organized by specific outcome categories.
Summary of Feasibility, Outcomes, and Delivery Experience

BA, body awareness; DE, dance exercise; DD, depersonalization–derealization; NS, no significant; QOL, quality of life; –, not assessed.
FEASIBILITY AND ACCEPTABILITY
Overall, TDI were consistently described as feasible and acceptable. Positive feedback predominated across studies, with participants frequently describing interventions as beneficial and recommendable.
ADHERENCE AND ENGAGEMENT
Adherence and engagement were reported in 18 studies (69%). High adherence was documented in several interventions, including 100% attendance in ParkinDANCE 40 and a median adherence of 97.4%. Reported completion thresholds were met by most participants in Walton et al., 51 where 91% attended ≥70% of sessions. Attendance rates of 77.6% and 75% were noted for ballet 40 and mindfulness-based DMT 41 programs, respectively. Seidler et al. 47 reported comparable attendance across online (87%) and in-person (84%) formats. Lower adherence was observed in Moo and Ho, 42 in which three of five dyads discontinued early. Tunçgenç et al. 50 reported high session engagement but noted attrition between baseline (n = 58) and postintervention (n = 33); attrition analyses showed no baseline differences between completers and noncompleters across most psychosocial measures.
TECHNOLOGICAL ACCEPTANCE AND ISSUES
Ten studies (38%) addressed technological acceptance. Participants generally adapted quickly to online platforms, though challenges included unstable internet connections, small screen sizes, audio–video lag, and limited digital literacy. Most issues were resolved after initial sessions. One study 42 reported participant withdrawal due to technology-related motivational fatigue.
ADVERSE EVENTS AND SAFETY
Seven studies explicitly reported safety outcomes, all indicating no significant adverse events. Minor anticipated effects (e.g., muscle soreness) were noted. Seventy-three percent of studies did not report on safety monitoring, limiting interpretation.
PARTICIPANT PREFERENCES FOR ONLINE VERSUS IN-PERSON DELIVERY
Only a small number of studies directly assessed preferences for online versus in-person delivery. Quantitative data indicated that most adults with Parkinson’s disease preferred in-person sessions (61.9%) over virtual formats. 33 Bek et al. 29 similarly reported strong support for in-person classes, with 70.8% of participants favoring a hybrid model that combined in-person programming with home-based digital practice.
Qualitative findings across several studies29,32,34,42 also indicated a preference for in-person engagement due to perceived benefits such as greater energy, presence, and social connection. Notably, Moo et al. 42 found that autistic participants expressed a clear preference for in-person sessions, citing relational depth and embodied attunement, while still acknowledging the accessibility benefits of tele-intervention.
PHYSICAL PERFORMANCE AND MOTOR OUTCOMES
Several studies reported improvements in physical health and motor function following participation in interventions. Among individuals with PD, studies have found improvements in balance, gait, posture, flexibility, and mobility.29,31,47,51 Specifically, interventions such as Dance for PD® and tango-based programs were associated with reduced motor symptom severity, increased gait velocity, and improved postural control.31,47,51
Positive changes were also reported in strength and functional mobility outcomes, including sit-to-stand performance, step tests, and upper- and lower-body strength assessments.31,35,40 For example, older adults and cancer survivors demonstrated improvements in chair stand repetitions, shoulder range of motion, and aerobic capacity following participation.35,40 Digital dance sessions were additionally associated with reduced sedentary behavior and increased physical activity levels.40,49 Although some studies did not observe significant between-group differences across all objective measures,28,31 overall trends indicated enhanced physical functioning in both self-reported and performance-based outcomes.
PSYCHOSOCIAL BENEFITS
Across the studies included, a wide range of psychosocial benefits were frequently reported. Several studies documented increases in mood, positive affect, and emotional well-being,30,32,33,37,48,49,51 as well as reductions in anxiety, distress, and depressive symptoms.30,37,49,51 Other reported outcomes included enhanced self-esteem, motivation, and experiences of joy,30,37,43,48 and increases in mindfulness, self-awareness, and interoceptive awareness.41,48,49 Findings from an adolescent sample 50 extended psychosocial evidence to younger populations, demonstrating significant increases in social bonding, overall well-being, hope, and future outlook. Improvements in social bonding were associated with gains in well-being.
Social connection was reported across multiple studies, with participants noting increased feelings of connection and inclusion, including in remote formats.32,45,46,51,52 Several studies described interventions as opportunities for creative expression and shared enjoyment, fostering a sense of community and enhancing overall well-being.43,48,54
Qualitative reports also indicated improvements in overall wellness, resilience, and emotional support, particularly during periods of isolation and stress during the COVID-19 pandemic.36,42,51 Although some studies noted challenges, such as reduced opportunities for spontaneous social interaction or initial technology-related difficulties,51,53 these barriers were generally outweighed by the psychosocial benefits.
ADVANTAGES AND DISADVANTAGES OF DIGITAL DELIVERY
Several studies reported advantages of digital delivery, including increased accessibility for individuals with transportation, mobility, or scheduling barriers.29,30,32,43,48,49 Home-based participation allowed for convenience, flexible pacing, and integration into daily routines. In some cases, regular online sessions provided structure during the COVID-19 pandemic and supported consistent engagement.38,51 Additional benefits included enhanced privacy and opportunities for repeated practice.
Reported disadvantages included technical challenges such as unstable internet connections, limited digital literacy, inadequate devices, and insufficient physical space.29,33,51 Reduced motivation without in-person structure and fewer opportunities for spontaneous social interaction were also noted. Instructors reported difficulty forming rapport and monitoring movement quality in remote formats. 52 Some participants perceived reduced physical challenge and expressive range compared with in-person settings.40,51
STUDY QUALITY
All included studies were appraised using the MMAT. Twelve studies (46%) met all appraisal criteria and were rated as high quality.28,31,34,36,38,45,46,48,49,51–53 Thirteen studies (48%) were rated as moderate quality,29,30,32,33,35,37,39–42,44,47,50 and one study (4%) was rated as low quality. 43
Four QUAL studies34,36,48,52 were appraised using the qualitative MMAT checklist, and all received the maximum score (5/5). Fourteen QUAN studies were appraised using quantitative MMAT criteria, including four RCTs,28,35,41,44 six nonrandomized studies,31,33,37,40,45,47 and four descriptive quantitative studies.29,38,39,53 Across QUAN designs, MMAT scores ranged from 3 to 5, with frequently missing information related to confounding variables, treatment fidelity, and participant response rates.
Seven studies used MM designs. Of these, three46,49,51 were rated as high quality, while four30,35,42,50 were rated as moderate quality due to limited qualitative completion rates, incomplete reporting of confounders or treatment fidelity, or attrition at follow-up.
Discussion
This scoping review synthesized evidence from 26 studies evaluating TDI across physical, psychosocial, and cognitive outcomes. Collectively, the findings indicate that TDI are generally feasible and well accepted and are associated with improvements in physical functioning, mood, social connectedness, and emotional well-being across populations. At the same time, the literature is characterized by methodological limitations, inconsistent reporting, and limited demographic diversity, underscoring the need for more rigorous and theoretically informed research as tele-dance moves beyond its pandemic-driven expansion.
Most studies focused on older adults, particularly individuals with PD or age-related cognitive decline. This pattern aligns with broader telehealth trends, as these populations frequently face barriers to in-person participation, including mobility limitations, transportation challenges, and caregiver burden.55–57 Although some studies included cancer survivors, caregivers, individuals with developmental disabilities, children and adolescents, and healthy adults, these populations remain underrepresented. Consistent with telehealth equity concerns,58,59 most studies did not report race or ethnicity, men were underrepresented, and few interventions explicitly addressed digital literacy or unstable internet access, raising concerns that TDI may inadvertently reinforce existing digital inequities if equity considerations are not intentionally integrated into design and recruitment.
Many TDI were adapted from established in-person programs, such as Dance for PD®, demonstrating the flexibility of translating embodied, arts-based practices to remote contexts during the COVID-19 pandemic, when rapid implementation was essential. 60 The majority maintained structural components characteristic of in-person classes, including warm-up sequences, structured or improvisational dance activities across genres, and cool-down phases. Some interventions emphasized formalized styles, including tango and classical ballet, underscoring the breadth of modalities incorporated into tele-dance. This blending of structured and improvisational approaches highlights tele-dance’s inherent flexibility and parallels the successful adaptation of other creative arts therapies to remote contexts.61,62 However, relatively few interventions were explicitly grounded in DMT theory or telehealth-specific frameworks, and key design features, such as camera-use policies, in-home safety considerations, and strategies for supporting remote embodied attunement, were inconsistently reported. Future TDI development would benefit from integrating DMT theory, 63 embodiment and synchrony research, 64 therapeutic alliance scholarship, 65 and implementation science to inform interventions intentionally designed for remote delivery rather than adapted from in-person formats.
Across studies, feasibility and acceptability were high, with strong adherence, favorable satisfaction ratings, and minimal adverse events, mirroring findings from tele-exercise and tele-creative arts therapies.62,66 Nevertheless, adherence varied by population. Notably, substantial dropout in a study involving autistic children and dyads 42 suggests that synchronous delivery may impose cognitive or sensory demands that are less compatible with some neurodivergent participants. Technological barriers—including audio disruptions, video lag, unstable connections, and limited physical space—were commonly reported and are consistent with broader telehealth literature. 67 These patterns highlight the importance of proactive engagement strategies, such as structured onboarding, flexible pacing, hybrid delivery formats (e.g., combination of prerecorded and live sessions), individualized participation goals, caregiver involvement, and ongoing technical and relational support.29,42,51
Preferences regarding delivery format further contextualize these findings. Although participants valued the convenience and accessibility of remote sessions, in-person or hybrid formats were generally preferred when available. Participants consistently described in-person dance as offering heightened embodied presence, shared energy, and relational attunement that were difficult to fully replicate online. These experiences align with DMT scholarship emphasizing nonverbal synchrony and shared movement rhythms as foundational to therapeutic alliance and emotional resonance.63,64 In line with emerging telehealth models, 68 TDI may therefore be most effective when conceptualized as part of a flexible continuum that integrates remote, in-person, and hybrid options tailored to individual needs and contexts.
TDI were associated with meaningful physical and motor improvements, particularly balance, gait, strength, and motor symptom severity among individuals with PD and older adults, consistent with tele-exercise literature.66,69 Psychosocial outcomes were similarly robust, with improvements in mood, anxiety, self-esteem, and motivation reported across studies. Social connectedness emerged as a central mechanism, with participants describing TDI as spaces of shared creativity and mutual support despite physical distance. These findings align with evidence that synchronous, arts-based telehealth interventions can foster social cohesion and emotional resilience.67,70,71
Despite these benefits, digital delivery introduced distinct challenges. Reduced spontaneity, fewer informal social interactions, and limitations in instructors’ ability to monitor safety and movement quality were commonly noted. Some participants perceived online sessions as less physically engaging or expressive, suggesting that TDI may operate through mechanisms that differ from those of in-person dance. Elucidating these mechanisms, particularly those related to embodiment, sensory engagement, and relational synchrony, represents an important direction for future research.
Finally, although group-based formats predominated and effectively supported social connection, individualized and dyadic tele-dance formats remain underexplored. Evidence from tele-music, tele-art, and tele-drama therapies suggests that individualized approaches may be especially beneficial for participants with sensory sensitivities, mobility limitations, or highly personalized therapeutic goals.61,72–74 Future research should examine hybrid models that integrate group-based and individualized formats to enhance personalization, accessibility, and therapeutic responsiveness.
The overall methodological quality of included studies was mixed. Although nearly half of the studies met all MMAT criteria and were rated as high quality, a comparable proportion were rated as moderate, and one study was rated as low quality. Common methodological limitations included small sample sizes, lack of control or comparison groups, inconsistent outcome measures, limited reporting of intervention fidelity, unclear handling of confounding variables, and minimal long-term follow-up. These limitations constrain the strength of causal inferences and limit comparability across studies. MM studies, while valuable for capturing participant experiences, frequently demonstrated imbalances between qualitative and quantitative components, such as incomplete qualitative integration or attrition at follow-up. Collectively, these findings underscore the need for more rigorous study designs, including adequately powered RCTs, pragmatic and hybrid effectiveness–implementation studies, standardized outcome reporting, and systematic fidelity assessments to strengthen the evidence base for TDI.
Overall, the evidence suggests that TDI represent a promising and adaptable modality for promoting physical and psychosocial health. However, realizing their full potential requires moving beyond rapid pandemic adaptations toward intentional tele-design grounded in embodiment theory, telehealth research, and implementation science. Priorities for future research include inclusive recruitment, culturally responsive design, theoretically grounded protocols, hybrid delivery models, and rigorous methodological approaches. As digital and hybrid care continue to expand, TDI may play an important role in supporting whole-person health, particularly when offered alongside in-person opportunities that preserve the relational and embodied richness of dance.
Limitations
Several limitations should be considered when interpreting the findings of this scoping review. First, the review intentionally focused on synchronous, live-streamed TDI targeting physical or psychological health outcomes. Consequently, asynchronous formats, self-guided digital programs, and exergame-based dance interventions were excluded, limiting the generalizability of findings to other forms of digitally delivered dance.
Second, consistent with the purpose of scoping reviews, this synthesis was designed to map the scope and characteristics of an emerging field rather than to estimate intervention effects or determine efficacy. Although methodological quality was appraised using the MMAT, studies were not weighted or excluded based on quality, and variability in study rigor and reporting precludes strong causal inferences.
Third, most included studies were conducted during the COVID-19 pandemic, which may limit the transferability of findings to routine, nonpandemic contexts. Participants’ engagement, access, and willingness to participate in tele-dance may have been shaped by public health restrictions, heightened isolation, and limited availability of in-person alternatives.
Additional limitations relate to heterogeneity across studies, including differences in study designs, participant characteristics, intervention duration and structure, instructor training, camera-use policies, and outcome measures. This variability constrained cross-study comparisons and limited the ability to identify optimal intervention components. Moreover, reporting on intervention fidelity, safety procedures, and implementation context, such as staffing, technological support, costs, and physical space considerations, was often limited, restricting assessment of scalability and real-world implementation.
Finally, although this review sought to capture both participant and facilitator perspectives, only one study 49 explicitly examined interventionists’ experiences. Given the central role of facilitators in ensuring safety, engagement, and therapeutic attunement in tele-dance, future research should more systematically examine facilitator training, support needs, and implementation challenges to inform sustainable and equitable delivery models.
Conclusion
This scoping review shows that TDI are generally feasible, safe, and acceptable, with consistent benefits for mood, social connection, and aspects of physical functioning across diverse populations. To advance the field, future research should employ rigorous and inclusive study designs, ensure consistent use of validated outcome measures, and examine long-term and hybrid delivery models that extend beyond pandemic-era adaptations. Given the complementary strengths of virtual and in-person formats, developing flexible, person-centered models will be essential for meeting varied needs, preferences, and access levels. Continued attention to methodological quality, contextual factors, and equity will be crucial to realizing tele-dance’s promise as an adaptable, accessible, and widely scalable health-promoting intervention.
Footnotes
Acknowledgments
The authors thank Dr. Nalini Prakash for her assistance with the initial literature search and early screening of records, and Ms. Chelsea Faulkner, Ms. Madeline Kling, and Ms. Jaclyn Lo for their assistance with study screening and methodological quality assessment.
Authors’ Contributions
M.S. conceived of and designed the study. S.G.P. developed the search strategy. D.S., C.L., E.U., and M.S. performed the literature search, screening, full-text review, and assessment of the study quality. M.S. and D.S. wrote the draft article. M.S., E.U., and S.G.P. contributed to the revision, editing, and approval of the final article.
Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
No funding was provided for the research.