
Abstract
Purpose:
Over the past several years, states began formally enacting telehealth policies to avail audio-only services for those unable to receive care in-person or over video. Such policies may be especially important in community-based health centers (CHCs) where, when telehealth is provided, it is primarily via audio-only. This retrospective study examined whether codified policies for Medicaid reimbursement and payment parity of audio-only telehealth were associated with greater use of telehealth.
Methods:
Electronic health records for Medicaid-insured adults 18–64 years with visits to primary care (n = 700,051) and to behavioral health care (n = 95,136) in 433 primary care and 279 behavioral health care CHCs from April 1, 2021, to March 31, 2023, were analyzed. We collected policies using standardized legal mapping methods to identify audio-only telehealth policies having: (1) no reimbursement for telehealth, (2) reimbursement for telehealth, but no payment parity, or (3) reimbursement for telehealth, at parity.
Results:
One-third of primary care visits were telehealth, most of which were audio-only. Two-thirds of behavioral health care visits were telehealth, half of which were audio-only. Primary care visits in states with audio-only telehealth reimbursement policies not at parity were 4.8 percentage points more likely, and behavioral health care visits in states with reimbursement at parity were 3.2 percentage points more likely to use telehealth.
Conclusions:
While audio-only telehealth reimbursement only modestly impacted overall telehealth utilization, Medicaid policies remain one of the few mutable factors important for primary care and behavioral health care access among safety-net populations.
Introduction
Although use of telehealth, including audio-only and video visits, has declined since the first months of the COVID-19 pandemic,1,2 it is now an accepted and regular part of primary and behavioral health care in the United States (U.S.). Telehealth has the potential to improve access to primary and behavioral health care, particularly for individuals facing barriers such as unreliable transportation, greater distances to providers, or inability to take time away from work or family. These barriers disproportionately affect patients seeking care in community-based health centers (CHCs),3,4 also referred to as safety-net clinics, which primarily care for uninsured and Medicaid insured patients.5,6
Many patients served by CHCs face structural limitations that hinder their ability to use telehealth, particularly video-based services. This includes patients who live in rural areas, those without access to broadband internet, those who are lower-income, uninsured, older, Hispanic, Black, or have limited English proficiency.7–17 Such differences in telehealth use are evident in both primary care and behavioral health care clinics. Consequently, audio-only telehealth has emerged as a critical modality for health care access in low-resource settings, including CHCs.10,17–19
At the beginning of the public health emergency, temporary changes to telehealth reimbursement policies, particularly for Medicaid, enabled broader access to video and audio-only services. 20 While Medicare and Medicaid currently reimburse for video telehealth services in all states, Medicaid reimbursement for audio-only services remains inconsistent, with many temporary provisions set to expire (or have already expired) in some states.21,22 Some states have codified these policies into law, including provisions for payment parity, ensuring continued access to audio-only services for those unable to receive care in-person or via video and enabling CHCs to serve as distant site providers.21,23 However, clinics in states without codified reimbursement policies face uncertainty around reimbursement and must weigh against the time and cost of investing in these services. 22 Despite the importance of these policies, research on their impact remains limited, especially among populations that stand to benefit the most from them, low-income, Medicaid-insured patients receiving care in CHCs. Existing studies on the association between telehealth reimbursement policies and telehealth use are mixed, with some showing a positive association and others showing no clear link.24–31 The available studies all found that telehealth policies were associated with significant, positive increases in the use of telehealth among privately insured individuals or the general population.24–27 Fewer studies have examined the association between these policies and telehealth use among populations experiencing barriers to accessing care. One prepandemic study found that more expansive telehealth reimbursement policies were not associated with increased odds of video telehealth use compared with no video use. 25 Additionally, these policies were not associated with increased video telehealth utilization among low-income, rural, Hispanic, Black, or those uninsured or covered by public insurance. 25
A more recent study found that adoption of state Medicaid reimbursement for audio-only telehealth services was associated with a higher probability that mental health treatment facilities offered telehealth, but facilities serving Medicaid enrollees were less likely to provide telehealth services. 27 Notably, none of these studies examined the impact of these policies on specific telehealth modalities (audio versus video), nor did they focus on CHC or other lower-resourced populations.
There is a critical gap in understanding how audio-only telehealth reimbursement and payment parity policies impact the use of telehealth generally, or the use of audio-only telehealth services, particularly among Medicaid-insured patients receiving care in CHCs. The aims of this study address that gap by examining whether (1) codified Medicaid reimbursement policies for audio-only telehealth and (2) payment parity for Medicaid-insured audio-only services are associated with the probability of a telehealth encounter (vs. in-person encounter) and with the probability that a telehealth encounter used audio-only telehealth (vs. video). We analyzed primary care and behavioral health CHC visits separately because uptake of telehealth differs across these two specialties.32,33 We hypothesized that the codification of laws into permanent reimbursement for audio-only telehealth, with or without payment parity, would incentivize clinic and provider investment in telehealth systems and workflows. While video telehealth had long been reimbursable by Medicaid, we anticipated that additional reimbursement for audio-only telehealth would result in increased provision and use of telehealth overall, in particular audio-only telehealth. To our knowledge, this is the first study to evaluate the impact of codified audio-only telehealth reimbursement policies on audio-only telehealth use among CHC patients.
Methods
STUDY DESIGN AND SETTING
This retrospective study used electronic health record (EHR) data from the Accelerating Data Value Across a National Community Health Center Network (ADVANCE) Clinical Research Network, a member of PCORnet®. ADVANCE is a multicenter collaborative led by OCHIN, which integrates outpatient EHR data and community-level data, resulting in a longitudinal dataset. 34
This study utilized data from 433 primary care and 279 behavioral health community-based clinics across 20 states that were live on OCHIN’s EHR throughout the study period (April 1, 2021 — March 31, 2023). Clinic types were categorized through a combination of internal identifiers. We considered all encounters that occurred in primary care clinics to be primary care encounters and all encounters from behavioral health care clinics to be behavioral health encounters.
We linked Rural-Urban Commuting Area (RUCA) files from the United States Department of Agriculture Economic Research Service, the U.S. Census, and EHR data. Our study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for observational studies. 35
STUDY POPULATION
We restricted our study to adults who were ≥18–64 years of age and insured by Medicaid at the date of their visit to one of the study primary care or behavioral health CHCs. We excluded adults 65 years and older because they are also eligible for Medicare. We chose the study period starting after the first wave of the COVID-19 pandemic to reflect a time after state-level “stay at home” orders had ended and after most states had opened COVID-19 vaccinations to all adults. 36 The unit of observation was the visit.
DEPENDENT VARIABLES
Visits were classified by encounter type (in-person or telehealth) and telehealth modality (audio-only or video). Encounter type and telehealth modality were identified using an algorithm developed through informed interviews with internal OCHIN clinicians, clinical informaticists, EHR developers, and billing specialists and used a combination of scheduling data, encounter data, and billing codes and modifiers. 37 This algorithm prioritized billing codes and modifiers, first, followed by a field created by OCHIN and added to the EHR in March 2021. An appointment cannot be made without completing this field (in-person, video, or audio). The field is populated for the clinician at the start of the encounter and modifiable if the visit modality changes.
INDEPENDENT VARIABLES
EHR data were used to identify patient age, sex (male, female), race (Asian; Black; White; other race including American Indian/Alaska Native, Native Hawaiian/Pacific Islander, multiple races; and unknown race), ethnicity (Hispanic, non-Hispanic, unknown ethnicity), primary language (English, Spanish, other language), patient percent Federal Poverty Level (FPL) at most visits (mostly <138% FPL, mostly ≥138% FPL, unknown at all visits), and patient Charlson Comorbidity Index score at study start (0, 1, 2, 3, 4+). We linked patient ZIP codes from the EHR to RUCA codes to categorize patient rurality at each visit based on classifications established by the University of Washington Rural Health Research Center 38 (urban, large rural, small and isolated rural, unknown). Similarly, we linked ZIP codes to Census data to identify the percent of neighborhood with broadband access (by quartiles: <81%, 81.0%−86.5%, 86.6%−90.3%, and >90.3%). For visits with a missing ZIP code, we used the ZIP code from the patient’s previous visit or, secondarily, the ZIP code from the next visit.
EXPOSURE VARIABLES
As described in the larger study protocol, legal mapping research methods were identified Medicaid reimbursement policies and policy provisions, including requirements for payment parity for audio-only services. 19 Audio-only telehealth policies were identified through text searches of legal documents including executive orders, Medicaid policy statements, session laws, etc. Two team members independently coded documents for effective policy dates and provisions. Legal and clinical experts were consulted on inconsistencies before coming to a final consensus. A three-level variable was created using the codified policies, and visits were categorized as (1) audio-only telehealth was not reimbursed, (2) audio-only telehealth was reimbursed, but not at parity, and (3) audio-only telehealth was reimbursed at parity. The first category was used as the omitted reference, and separate indicators for the second and third categories were included in the models as key covariates.
ANALYTIC METHODS
We described encounter characteristics by encounter type and telehealth modality in primary care clinics and behavioral health clinics, separately. We then examined the percentage of encounters that were covered by Medicaid audio-only telehealth reimbursement without payment parity, those with payment parity, and those with neither. We estimated four separate regressions, two using the sample of visits from primary care community-based clinics and two using visits in behavioral health community-based clinics. In each setting, we estimated the association between the reimbursement and payment parity indicators (described above) with encounter type (in-person versus telehealth). We estimated their association with telehealth modality (audio-only versus video) among the subset of telehealth encounters. Models controlled for clinic fixed effects, time (measured as number of quarters from the study start), and the above patient and visit covariates. Because clinics are nested within states, the use of clinic fixed effects accounts for state-level unobserved, time-invariant factors as well.
We estimated linear probability models to facilitate the interpretation of the regression estimates. We calculated robust standard errors and used two-sided significance tests with p < 0.05 as the threshold for statistical significance.
Analyses were conducted using Stata version 18.0 (Stata Corporation). This study was deemed exempt by the Advarra Institutional Review Board.
Results
DESCRIPTIVE DATA
During the study period, a total of 3,530,166 primary care visits by 700,051 patients and 929,768 behavioral health visits by 95,136 patients were completed. Nearly one-third (32.6%) of primary care visits and two-thirds (66.5%) of behavioral health visits were conducted via telehealth ( Table 1 ). In primary care and behavioral health clinics, a greater percentage of visits were conducted by telehealth among patients who were female, Asian, lived in an urban area or a neighborhood with the greatest level of broadband access. Among completed telehealth visits, 62.7% of primary care visits and 49.1% of behavioral health visits were audio-only.
Encounter-Level Characteristics Comparing in-Person to Telehealth in Primary and Behavioral Health Community-Based Health Centers
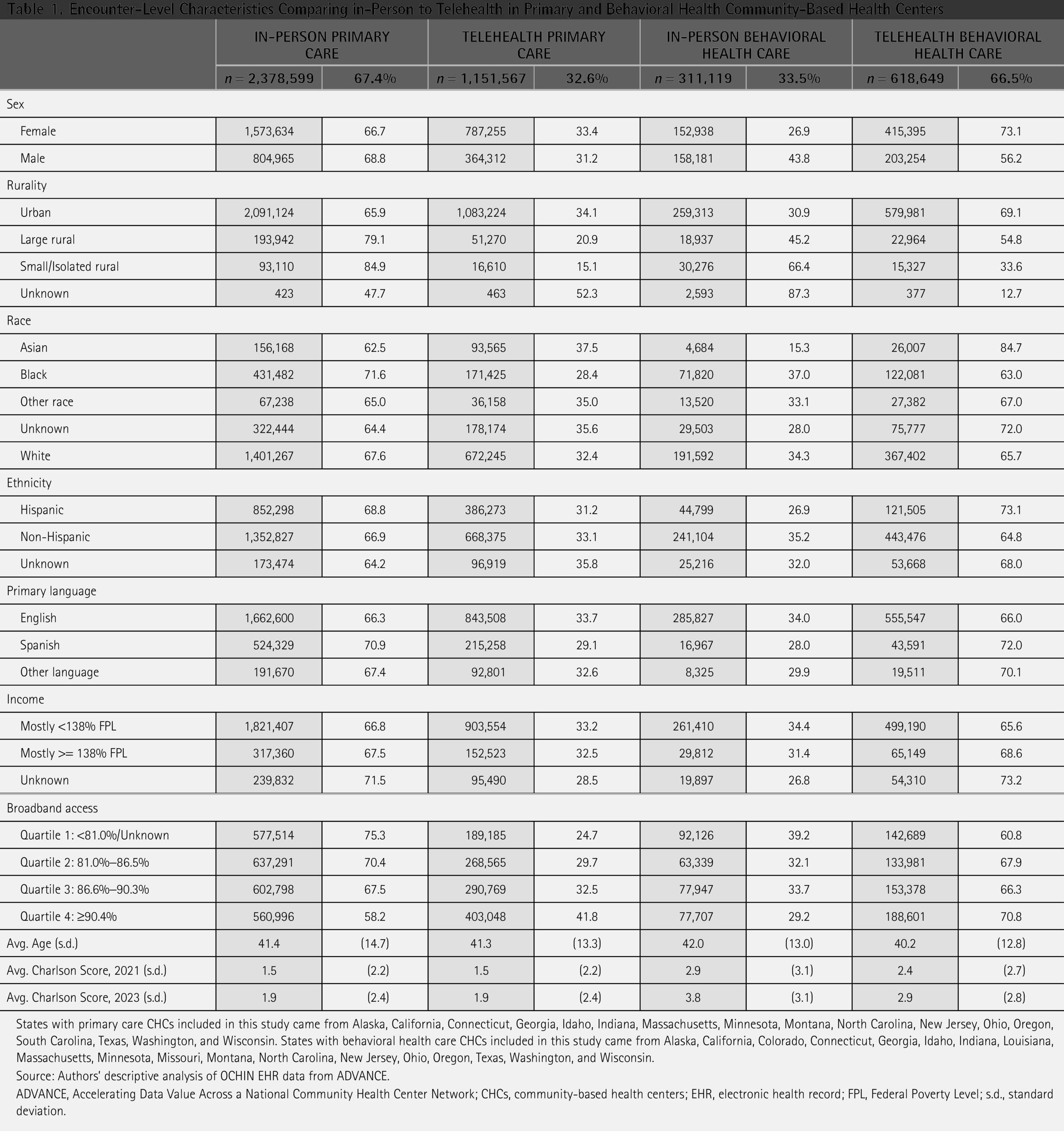
States with primary care CHCs included in this study came from Alaska, California, Connecticut, Georgia, Idaho, Indiana, Massachusetts, Minnesota, Montana, North Carolina, New Jersey, Ohio, Oregon, South Carolina, Texas, Washington, and Wisconsin. States with behavioral health care CHCs included in this study came from Alaska, California, Colorado, Connecticut, Georgia, Idaho, Indiana, Louisiana, Massachusetts, Minnesota, Missouri, Montana, North Carolina, New Jersey, Ohio, Oregon, Texas, Washington, and Wisconsin.
Source: Authors’ descriptive analysis of OCHIN EHR data from ADVANCE.
ADVANCE, Accelerating Data Value Across a National Community Health Center Network; CHCs, community-based health centers; EHR, electronic health record; FPL, Federal Poverty Level; s.d., standard deviation.
In our study, 58.5% of primary care visits were conducted in a state that had not yet codified reimbursement for audio-only telehealth visits for Medicaid-insured patients, while 41.5% of visits were conducted in a state that had codified reimbursement laws for audio-only telehealth, with 91% of reimbursed audio-only telehealth visits (37.8% divided by 41.5%) reimbursed at parity ( Table 2 ). Among behavioral health visits, 74.9% were in states with codified audio-only reimbursement policies, and 58.0% of reimbursed audio-only telehealth visits were reimbursed at parity. At the start of the study period, 11 states reimbursed audio-only telehealth, whereas 30 reimbursed audio-only telehealth by the end of the study period, 11 of those at parity ( Fig. 1 ).

Number of states that adopted audio-only reimbursement policies and audio-only reimbursement policies over the study period: April 1, 2021–March 31, 2023. Source: Authors’ descriptive analysis of OCHIN EHR data from ADVANCE and legal mapping of state Medicaid telehealth reimbursement policies. ADVANCE, Accelerating Data Value Across a National Community Health Center Network; EHR, electronic health record.
Primary Care and Behavioral Health Care Visits Covered Versus Not Covered by Audio-Only Telehealth Policies

Source: Authors’ descriptive analysis of OCHIN EHR data from ADVANCE and legal mapping of state Medicaid telehealth reimbursement policies.
REGRESSION RESULTS
After accounting for patient and neighborhood factors and clinic fixed effects, state codification of reimbursement for audio-only telehealth services was positively associated with telehealth compared with in-person visits in both primary care ( Fig. 2a ) and behavioral health ( Fig. 2b ) CHCs. Compared to primary care visits in states with no audio-only telehealth reimbursement policies, primary care visits in states with audio-only telehealth reimbursement policies not at parity were 4.8 percentage points (PP) more likely to be telehealth (95% confidence interval [CI], 2.3, 7.3, p < 0.001) ( Fig. 2a ). Compared with the 32.6% baseline probability that primary care visits were conducted via telehealth rather than in-person, this increase corresponds to a 15% relative increase in the likelihood that primary care encounters are telehealth. While not statistically significant, we found a positive association between reimbursement at parity compared with no reimbursement and the probability of telehealth versus in-person visits (1.4 PP, p = 0.082) within primary care CHCs.

(
In behavioral health clinics ( Fig. 2b ), we found that compared with no reimbursement, reimbursement at parity was associated with a 3.2 PP (95% CI: 0.3, 6.1, p = 0.003) increase in the use of telehealth versus in-person, but reimbursement not at parity was not significantly associated with this outcome (−0.8 PP, p = 0.687).
Among the subset of visits in primary care clinics conducted by telehealth, reimbursement for audio-only telehealth at parity compared with no reimbursement was associated with a 4.8 PP increased probability (95% CI: 2.0, 7.7, p = 0.001) of audio-only versus video visits, representing an 8% relative increase over the baseline probability of 62.7% ( Fig. 3a ). We found no significant differences in telehealth modality in behavioral health clinics between telehealth visits in states with reimbursement either not or at parity compared with telehealth visits in states with no reimbursement ( Fig. 3b ).
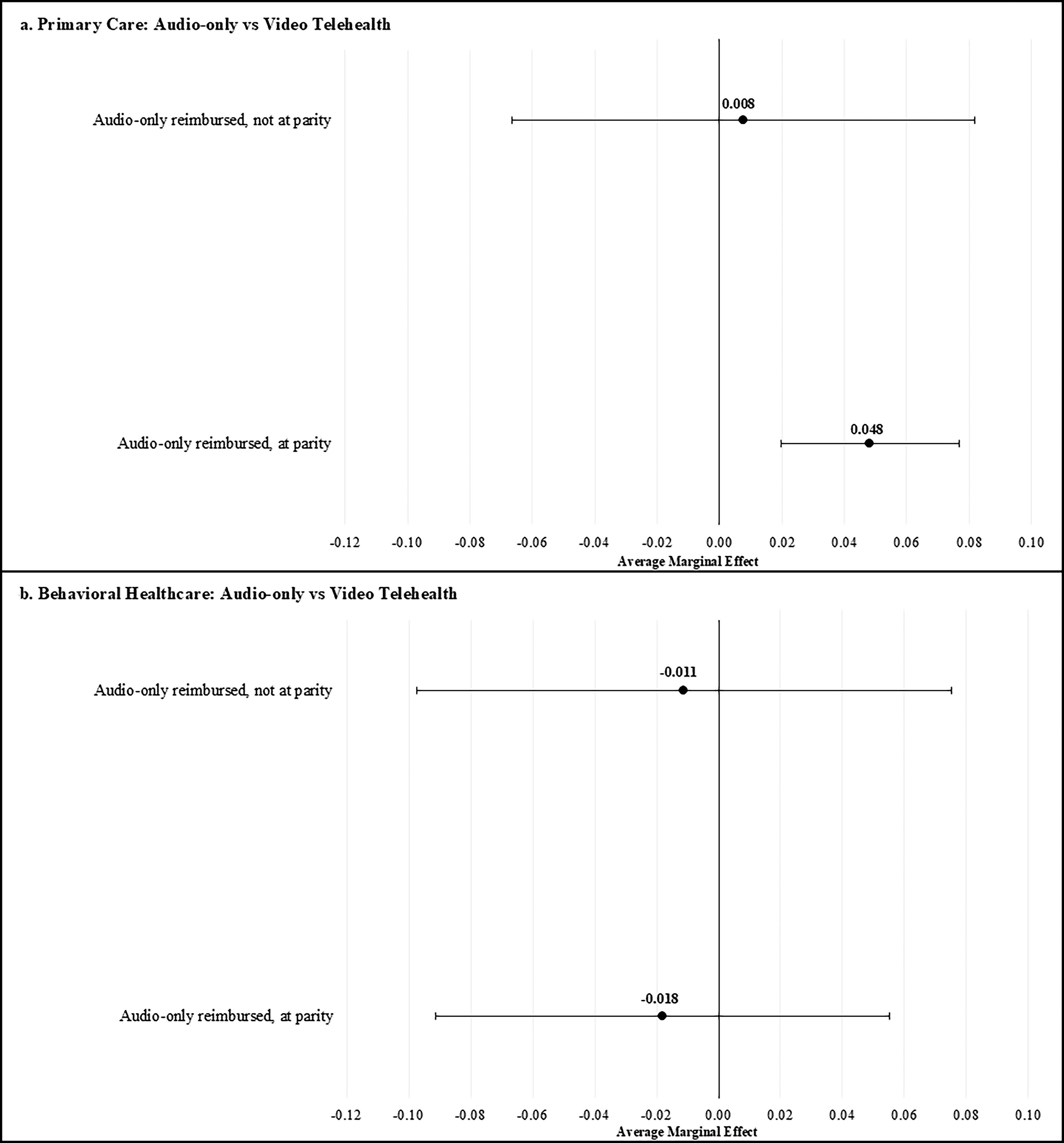
(
Discussion
For both primary care and behavioral health CHC visits, we found that codified reimbursement (versus no reimbursement) generally had a positive, albeit small (3–5 PP), effect on increasing the likelihood of telehealth versus in-person visits. While all study states had COVID-19 pandemic-related flexibilities allowing for audio-only services, codification of reimbursement policies likely signaled to clinicians and clinic administrators that audio-only telehealth is a stable and legitimate mode of care delivery that is likely to persist beyond the temporary provisions. Perceived policy permanence may foster greater confidence among providers to invest in workflow and staffing strategies that support telehealth, including audio-only telehealth. Our findings are consistent with prior research,24,26 extending findings to CHCs in a postpandemic era.
Using rigorous legal mapping methods and EHR data from CHCs across 20 states, this study is among the first to examine the impact of postpandemic state-level Medicaid reimbursement policies on telehealth and the first, to our knowledge, to examine the impact of these policies on telehealth modalities (e.g., audio-only versus video telehealth). Previous studies examining the impact of telehealth policies on the use of telehealth have mostly been restricted to privately insured patients, relied on survey or claims data, or were conducted prior to the widespread adoption of telehealth resulting from the COVID-19 pandemic.24–27 The only previous study on the impact of telehealth reimbursement policies on low-income, uninsured, and publicly insured patients, those predominantly served by CHCs, found no association between telehealth policies and use of telehealth. 25 The differences in our findings could be due to the fact that the previous study occurred prior to the widescale adoption of telehealth and the fact that uninsured and Medicaid-insured patients were not as well represented in the survey.
We did find differences between primary care and behavioral health CHCs with regards to the impact of reimbursement at parity for audio-only telehealth policies on use of audio-only telehealth (versus video). In primary care clinics, these policies were positively associated with the use of audio-only telehealth as compared with video. Primary care clinics have historically relied heavily on telephone calls to respond to a variety of patient requests, such as urgent problems (e.g., symptom triage) and brief chronic-condition care (e.g., medication refills). 32 A prior study on clinician perceptions of telehealth found that clinicians in primary care settings rated audio-only telehealth visits equivalent to video telehealth visits and were more likely to recognize some of the challenges facing patients in using video technology. 39 Audio-only telehealth policies that support reimbursement at parity, however, had no effect in behavioral health clinics. Our lack of findings in behavioral health clinics could be due to clinician preference. While primary care clinicians saw no difference between the two modalities, prior research found that mental health care clinicians preferred video over audio-only when using telehealth. 27 For mental health visits, clinicians may prefer video-enabled visual cues, and patient may prefer the comfort and privacy of communicating from home.
It is widely accepted that the removal of policy barriers to telehealth alone will not provide a solution to improving access to telehealth services.25,40,41 In our study, the effects of Medicaid reimbursement and payment parity of audio-only telehealth visits on telehealth utilization and audio-only use were modest. Other clinician, organizational, and patient-level factors may have greater effects.42,43 Despite this, reimbursement policies are often noted as important in the post-COVID longevity of telehealth in the United States and are mutable factors, unlike most patient characteristics that have been shown to impact use of telehealth.9,10 It will be important to continue to monitor the impact of these policies with the end of the public health emergency policies, leaving clinicians and clinics in states that have not codified these policies into law without the ability to reimburse for audio-only telehealth visits. Additionally, future research should explore the impact of these policies on patient use of telehealth and telehealth modalities for hybrid care, recognizing that patients may utilize a combination of these in-person and telehealth to receive care as well as quality of care for audio-only visits.
LIMITATIONS
There were several limitations in this study. First, temporary public health emergency reimbursement for audio-only telehealth visit policies was in place in all study states at the time of analysis. In such cases, clinician behavior may be driven by temporary reimbursement policy practices rather than by permanent policy codification. While we are unable to determine clinic-level awareness of telehealth reimbursement policies, use of clinic fixed effects accounts for not just clinic, but also the state, unobserved time-invariant factors. Second, telehealth modality is difficult to ascertain from EHR data and other databases. 44 This study utilized an algorithm developed through consultation with experts with internal knowledge of billing, design, and actual use of these systems.
Conclusion
In our large retrospective EHR analysis of CHCs across 20 states, we observed positive associations between codification of Medicaid reimbursement and payment parity policies and telehealth utilization among primary care and behavioral health clinics. While positive policy associations were seen for telehealth utilization overall, policies were only associated with audio-only telehealth utilization specifically in primary care CHCs. Other factors (e.g., insurance status) continue to play a role in the use of telehealth and telehealth modality, especially among patients who are low-income and the clinicians that serve them. It will be important to continue to understand the impact of these policies on use of telehealth, as temporary reimbursement provisions have expired.
Authors’ Contributions
A.E.L.: Conceptualization, methodology, analysis, data curation, writing—original draft, writing—review and editing, funding acquisition. J.J.E.: Conceptualization, methodology, writing—review and editing. S.L.E.: Conceptualization, methodology, writing—review and editing. L.B.L.: Conceptualization, resources, writing—original draft, writing—review and editing, supervision, funding acquisition.
Footnotes
Disclosure Statement
The authors declare no other conflicts of interest.
Funding Information
This work is supported by grants from the Agency on HealthCare Research and Quality (K01HS028732) and by the National Institute of Mental Health (1RF1MH133436-01). L.B.L. is supported by VA HSR&D Career Development Award (IK2HX002867). The views expressed are those of the authors and do not represent the views of the National Institutes of Health, U.S. Department of Veterans Affairs, or the United States Government. The research reported in this work was powered by PCORnet®. PCORnet has been developed with funding from the Patient-Centered Outcomes Research Institute® (PCORI®) and conducted with the Accelerating Data Value Across a National Community Health Center Network (ADVANCE) Clinical Research Network (CRN). ADVANCE is a Clinical Research Network in PCORnet led by OCHIN in partnership with Health Choice Network, Fenway Health, University of Washington, and Oregon Health & Science University. ADVANCE’s participation in PCORnet is funded through PCORI Award RI-OCHIN-01-MC.