
Abstract
Introduction:
Comprehensive evaluation of teledermatology systems includes socioeconomic assessment. In 2021, we implemented an intervention to improve the use of teledermatology in the health care area of Alicante-Hospital General. This study aimed to evaluate the socioeconomic impact of our intervention by comparing the costs and waiting times associated with teledermatology compared with conventional in-person care.
Material and Methods:
We designed a cost-effectiveness study from a health care system perspective using 2021 data. The monetary variables included the costs of the materials, application software, and training associated with teledermatology, as well as the costs of the consultations in both modalities. Our clinical outcome variable was waiting time until evaluation by a pediatric dermatologist. Using these data, we calculated an incremental cost-effectiveness ratio, then performed a sensitivity analysis. We also calculated the break-event point between the two modalities, based on the percentage of remote resolution of teleconsultations.
Results:
There were 357 teleconsultations in 2021, and we estimated 3,108 conventional referrals. The average per-patient cost of teledermatology was EUR 22.97 more than conventional care, with a cost-effectiveness ratio of EUR 0.21/day saved, which increased to EUR 0.35/day saved in the sensitivity analysis. To balance the costs of the two modalities, 84% of teleconsultations would need to be resolved remotely.
Conclusions:
Teledermatology is more expensive than conventional in-person care but is a cost-effective option from a health care system perspective.
Introduction
Health expenditure is increasing due to technological advances and a rising demand for health services. The available resources are limited and insufficient to ensure the well-being of all people. Economic studies provide evidence for deciding where to direct these resources.1,2
One key objective of implementing telemedicine, and by extension teledermatology, is to improve health care quality while also increasing diagnostic efficiency through a reduction in the number of visits and costs of services. However, few economic studies have evaluated asynchronous (store-and-forward) teledermatology.
3
An economic evaluation compares the cost of a novel intervention with that of an existing or conventional intervention. An economic study of teledermatology involves determining the type of economic analysis, describing the economic perspective of the analysis, making a detailed list of the costs involved, and performing a sensitivity analysis.
3
The costs associated with teledermatology can be classified as follows.
Fixed health care costs (costs unaffected by greater or lesser use of the tool), such as the cost of the application created specifically for teledermatology. Variable health care costs, such as the value of the professional’s time spent on the consultation.
3.
Costs incurred by patients or society, such as the cost of transportation to the health care center. The cost of contracting private companies.
1
The perspective of an economic analysis depends on the costs included. A societal perspective covers costs for the health care system as well as costs incurred by patients and society, while a health care perspective only includes costs for the health care system.
In 2021, we designed an intervention to improve the insufficient use of teledermatology among primary care pediatricians in the health care area of Alicante-Hospital General. The intervention comprised a series of actions to improve the availability and infrastructure of the system, as well as a personalized training program for primary care pediatricians who had access to the tool. It is important to assess whether this measure has been effective. Evaluations of teledermatology systems should cover user satisfaction, educational capacity, and economic impact. 4 For this study, we focused on the socioeconomic impact of the pediatric teledermatology intervention implemented in our health care area.
MATERIAL AND METHODS
We designed a cost-effectiveness study to compare teledermatology with conventional in-person care in the pediatric population. We planned the analysis from a health care system perspective. Monetary variables included the following costs.
Cost of material: a fixed cost invested in cameras and memory cards, which we considered to have an average life of 3 years.
5
Cost of the teledermatology application: another fixed cost covering the development of the teledermatology application for both pediatric and adult patients. We included the total expenditure in our analysis, regardless of whether the application was used for both patient groups, and we took into account the 13 years of use since its implementation in 2008. Training costs: a fixed cost including the price of talks given to primary care pediatricians by dermatologists and the price of a photography course for primary care pediatricians. Cost per consultation: a variable cost based on the number of consultations carried out and including the following costs listed in article 29.1-9 of the Spanish Fees Act 20/2017.
6
Initial in-person visit with the pediatrician Teleassessment by the dermatologist Telephone call made by the pediatrician to provide the teleassessment results In-person visit with a dermatologist
The teledermatology process consists of an in-person visit and a telephone call with a primary care pediatrician, plus a teleassessment by a pediatric dermatologist. If an in-person dermatology assessment is necessary, the process has an added cost. Conventional care includes an in-person visit with a primary care pediatrician plus an in-person visit with a general dermatologist. A small proportion of children are referred to a pediatric dermatologist for further assessment; however, we did not include the cost of these additional visits in our economic evaluation. We estimated the annual number of conventional dermatology referrals in children using data collected in 2007. 7 For teledermatology, we used data from consultations that took place in 2021. Fig. 1 summarizes the referral process for each modality, as well as the costs and waiting times involved.
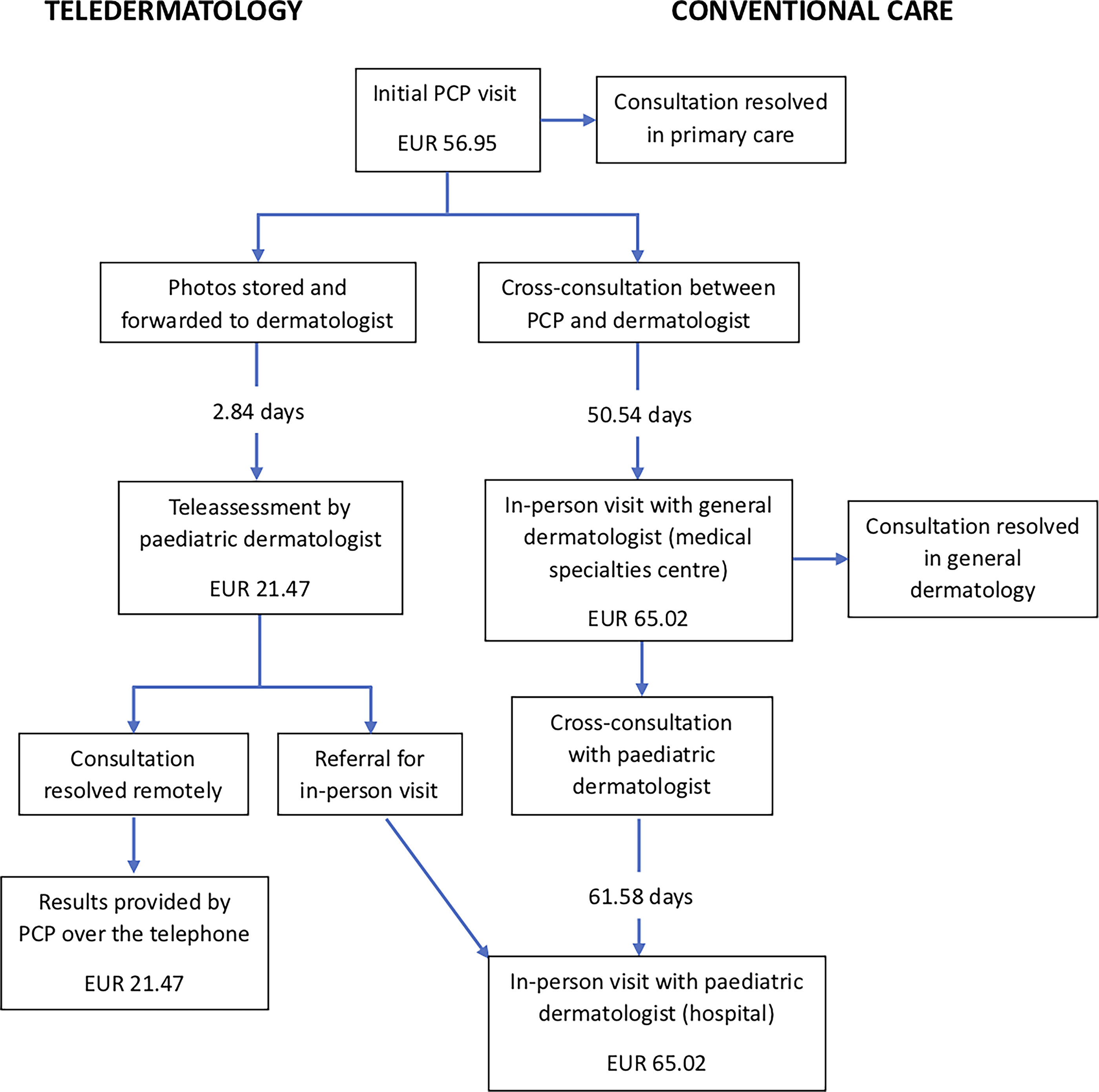
Patient flow for each of the consultation modalities. On the right, conventional dermatological care; on the left, teledermatology. PCP, primary care pediatrician.
Because our analysis focused on costs to the health care system, we excluded costs incurred by patients and society. We also excluded the cost of internet, gas and electricity, and maintenance of the facilities because these are sunk costs that will be incurred with or without teledermatology. Table 1 summarizes the costs included in our economic analysis.
Annual Costs Involved in Teledermatology Versus Usual Dermatological Care
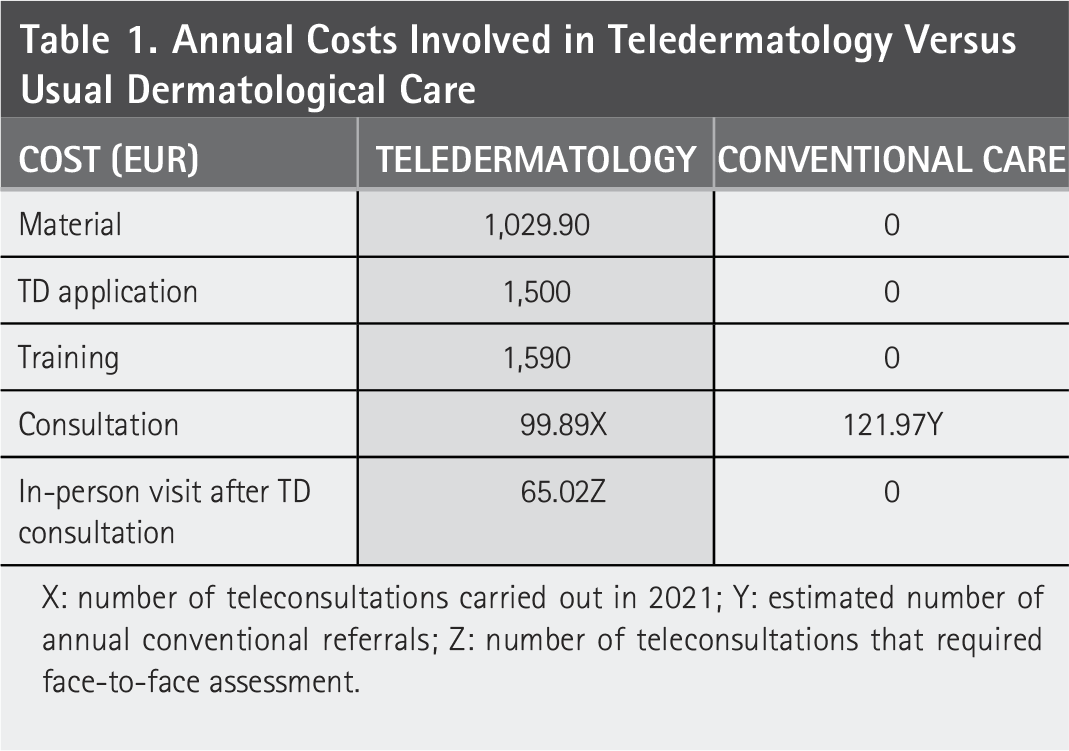
X: number of teleconsultations carried out in 2021; Y: estimated number of annual conventional referrals; Z: number of teleconsultations that required face-to-face assessment.
Our clinical outcome variable was waiting time from the initial in-person visit with a primary care pediatrician to (remote or in-person) assessment by a pediatric dermatologist. For teledermatology, we calculated the mean waiting time for all patients, as the images are forwarded directly from primary care to a pediatric dermatologist. For conventional care, we calculated:
mean time from referral by a pediatrician to in-person assessment by a general dermatologist (using data from all patients); and mean time from in-person assessment by a general dermatologist to in-person assessment by a pediatric dermatologist (using data from the consultations not resolved in general dermatology).
We then added these means to obtain a clinical outcome that was comparable to that of teledermatology (see Fig. 1 ).
We decided that if our analysis showed teledermatology to be more expensive than conventional care, we would calculate the incremental cost-effectiveness ratio, defined as the mean incremental cost divided by the mean incremental waiting time saved, expressing the results as additional cost in euros per patient per day saved until assessment by a pediatric dermatologist. This would be followed by a sensitivity analysis to test whether our cost-effectiveness estimate was robust to variations in a specific assumption (number of teledermatology consultations leading to in-person referrals). This sensitivity analysis would involve repeating the cost-effectiveness calculation but assuming 50% fewer in-person consultations prevented by teledermatology (and thus an increased average cost of teledermatology), while keeping all other parameters constant. We decided not to test an even less favorable assumption (more than 50%) because the lowest reported rates of remote resolution in dermatology are around 50%.8,9
An additional objective of our study was to determine the break-even point, or the number of remote resolutions required for teledermatology consultations to incur the same costs as in-person consultations (considering the variation in the price of teleconsultations depends on the number of in-person visits avoided).
Approval of these methods was granted by the Alicante—General Hospital health care department ethical committee.
Results
Our records show that 357 pediatric teledermatology consultations took place in our hospital in 2021. In 173 cases (48.5%), there was no need for an in-person dermatology assessment. We estimated 3108 conventional referrals for in-person dermatology consultations. 7 Table 2 presents the costs included in our economic analysis of each modality.
Cost of Teledermatology Versus Conventional Dermatological Care in 2021
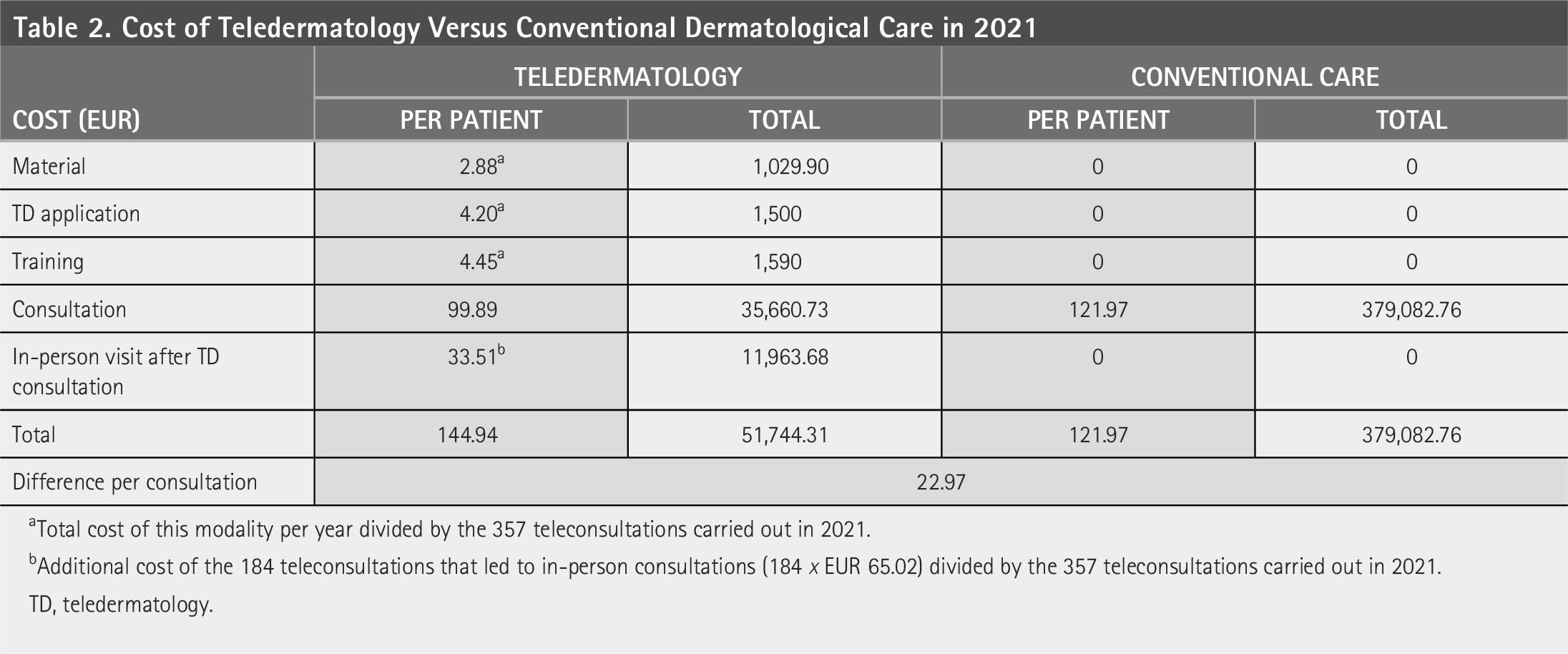
aTotal cost of this modality per year divided by the 357 teleconsultations carried out in 2021.
bAdditional cost of the 184 teleconsultations that led to in-person consultations (184 x EUR 65.02) divided by the 357 teleconsultations carried out in 2021.
TD, teledermatology.
The mean waiting time for the 357 teleconsultations was 2.84 days (range: 0–13 days). For conventional care, the mean waiting time was 112.12 days: 50.54 days until assessment by a general dermatologist and another 61.58 days until assessment by a pediatric dermatologist, according to hospital records ( Fig. 1 ). The incremental cost-effectiveness ratio was EUR 0.21 per patient per day saved, which means each day of waiting time prevented because of teledermatology cost an extra EUR 0.21 ( Table 3 ).
Cost-Effectiveness Study of Teledermatology Versus Conventional Dermatological Care
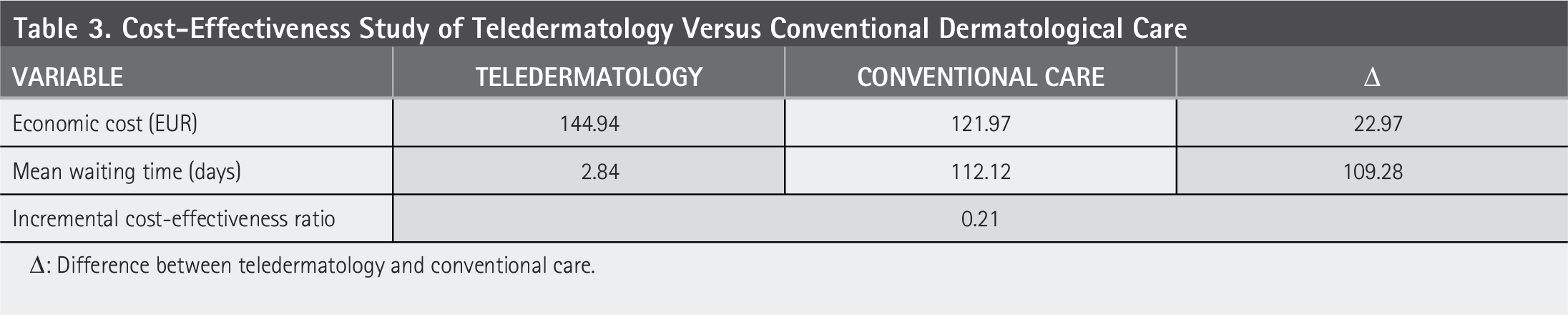
Δ: Difference between teledermatology and conventional care.
For the sensitivity analysis, we assumed that only 86 (rather than 173) of the 357 teleconsultations were resolved remotely (50% fewer). In this scenario, the remaining 271 teleconsultations led to an in-person visit with the dermatologist, increasing the average cost of teledermatology ( Table 4 ).
Sensitivity Analysis: cost of Teledermatology Versus Conventional Dermatological Care in 2021 Assuming There Were 50% Fewer Teledermatology Consultations Resolved Remotely
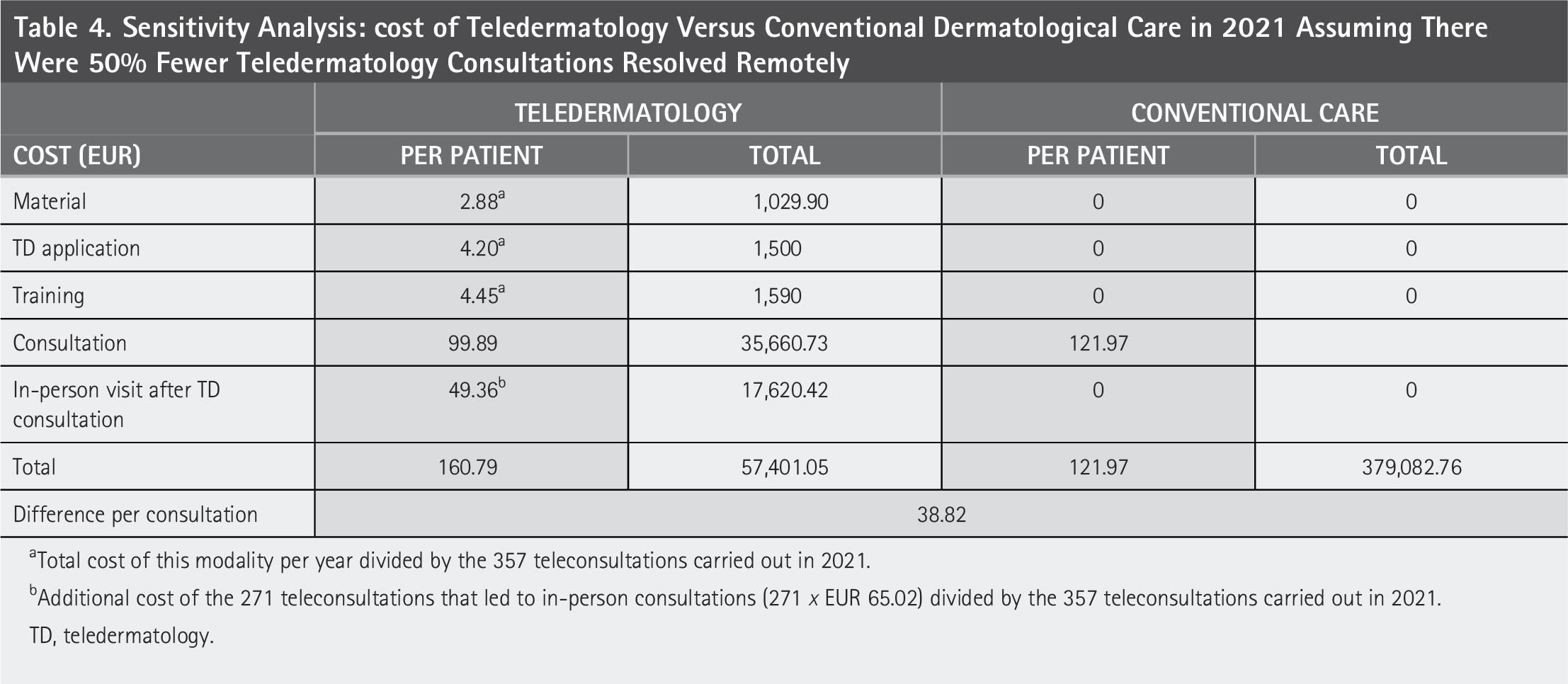
aTotal cost of this modality per year divided by the 357 teleconsultations carried out in 2021.
bAdditional cost of the 271 teleconsultations that led to in-person consultations (271 x EUR 65.02) divided by the 357 teleconsultations carried out in 2021.
TD, teledermatology.
Therefore, using the same waiting time data as in the main cost-effectiveness analysis, we calculated an incremental cost-effectiveness ratio of EUR 0.35 per patient per day saved ( Table 5 ).
Sensitivity Analysis: cost-Effectiveness Study of Teledermatology versus Conventional Dermatological Care Assuming There Were 50% Fewer Teledermatology Consultations Resolved Remotely
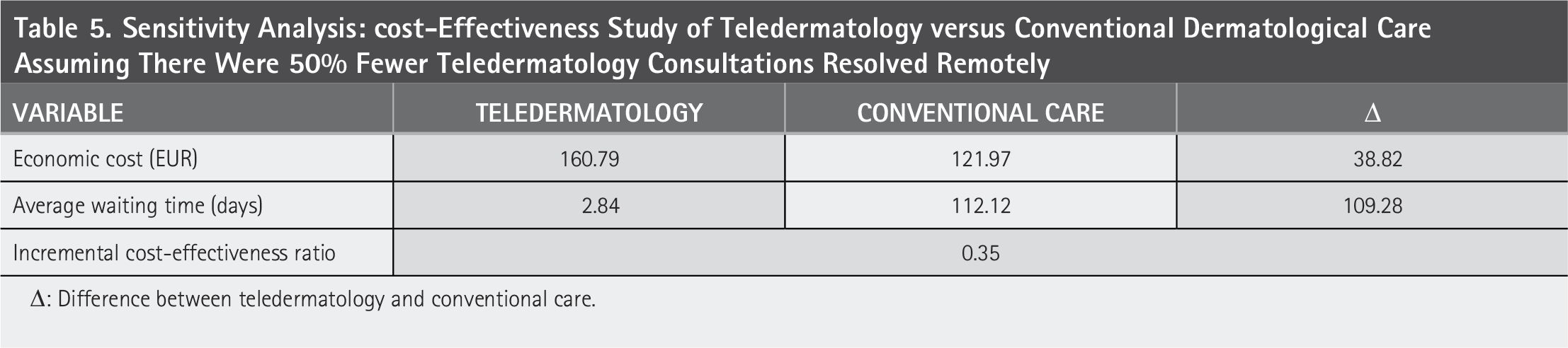
Δ: Difference between teledermatology and conventional care.
To calculate the break-even point between the two modalities, we used the equation 65.02 (357—x)/357, where x is the number of consultations resolved remotely, and therefore 357—x is the number of teleconsultations that lead to an in-person visit, with an additional cost of €65.02.
111.43 + 65.02 (357—x)/357 = 121.97
X = 299.13 ≅ 300
We estimated that for the cost of teledermatology to equal the cost of conventional dermatology care, 300 of the 357 teleconsultations that took place in 2021 (84%) would have to have been resolved remotely.
Discussion and Conclusions
It is difficult to compare the published economic data on teledermatology for various reasons. First, some studies adopt a societal perspective (including costs incurred by patients and society as well as costs to the health care system) while others focus on direct health care costs. Second, the expenses analyzed within each perspective vary and are often based on estimates or approximations. Third, there is considerable heterogeneity in terms of effectiveness measures (quality of life, satisfaction, reduction of waiting times, etc.). Finally, socioeconomic analysis is often a secondary objective.
Many studies have found teledermatology to be cheaper, or at least not more expensive, than in-person consultations.10,11 One study published in 2009 by Pak et al. found that teledermatology achieved similar clinical effectiveness for a lower total cost.12,13 The data from a more recent publication by Datta et al. tell a similar story. 14 Another study from 2025 found teledermatology to be cheaper and more effective in quality-adjusted life year terms. 15 In addition, economic studies considering only costs to health care systems have associated teledermatology with significant savings. 16 In their analysis of estimated personnel costs, Yang et al. found that teledermatology could save between USD 10 an USD 52.65 per consultation compared with a scenario in which teledermatology did not exist. 17
Three studies based in Spain concluded that teledermatology was cheaper than conventional dermatology care from a societal perspective, but that this advantage was smaller when considering only costs to health care systems. Vidal-Alaball and colleagues reported total savings of EUR 11.40 per patient, which decreased to EUR 2.30 per patient when costs incurred by patients and society were removed from the analysis 18 ; and López-Villegas and colleagues reported savings of EUR 23.74 per consultation from the societal perspective, which reduced to EUR 8.61 when analyzed from the health care system perspective. 19 Moreno and colleagues carried out a cost-effectiveness study and used as a measure of effectiveness the waiting time until consultation in each of the modalities. Their results favored teledermatology, which was more effective (76.31 days saved) and cheaper (EUR 49.59 less). 20
In our analysis of direct health care costs, teledermatology was more expensive that conventional care, with a price difference of EUR 22.97 per consultation. Adopting the societal perspective seems to produce more favorable results for teledermatology;18,19 however, if we extrapolate to our analysis the previously reported cost reduction attributable to societal and patient factors, teledermatology is still the more expensive option. Eminovik and colleagues carried out a cost-minimization analysis starting from the assumption that both modalities had similar clinical efficacy. They reported that teleconsultations were EUR 33 more expensive. 5 The authors also performed a scenario analysis, which showed store-and-forward teledermatology would be the cheaper option if the distance to the dermatologist were greater than 75 km, or if teledermatology prevented more than 37% of in-person consultations. In our study, for teledermatology to be cheaper than conventional referral, more than 84% of in-person referrals would have to be prevented, which is 35.1% more than the proportion of cases resolved remotely in our sample. Some studies have reported remote resolution in more than 84% of cases,21–23 which could be achieved through training of teledermatology professionals. However, we believe that forcing such a sharp increase in prevented in-person referrals could lead to medical negligence, so this would be an unsuitable approach for lowering the costs of teledermatology in the short term.
For our cost-effectiveness analysis, we used as a measure of effectiveness the time saved to assessment by a pediatric dermatologist. We estimated an incremental cost-effectiveness ratio of EUR 0.21 per patient per day saved, which indicates teledermatology is a cost-effective option in our setting because the benefit is worth more than what it costs. Similarly, in 2003, Whited and colleagues obtained a ratio of USD 0.17 per patient per day saved. 24 We also included a sensitivity analysis, reducing the proportion of teledermatology consultations resolved remotely by 50%. In this scenario, we estimated an incremental cost-effectiveness ratio of EUR 0.35 per patient per day saved, which still favors teledermatology.
There are other relevant expenses or savings that were not taken into account in our study. For example, Whited and colleagues discussed in their review how telemedicine offered primary care physicians valuable learning opportunities without the high cost of conventional training. 3 Another consideration is that the upfront costs of implementing a teledermatology system (purchasing equipment, obtaining software licenses, and training professionals) make it more expensive in the beginning, but these expenses become “cheaper” over the years. 16
One limitation of our study is that we did not consider costs to patients and society, since the costs of travel and productivity losses vary greatly. Many children traveled to in-person visits on free public transport or on foot, and many were accompanied by unemployed or retired people. Another limitation of our economic study is the cost estimate for in-person consultations, as we did not take into account possible hospital referrals for patients requiring specialized dermatological care. Had we taken these costs into account, the estimated economic advantage of teledermatology would have been greater.
In conclusion, teledermatology is a cost-effective tool from the perspective of health care systems, as it reduces dermatology waiting lists and prioritizes pathologies that require early attention at a low cost.
Footnotes
Author Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
No funding was received for this study.