More Than Just a Video Call: The Secret Ingredients of Tele-SNF Success
Radhika Malhotra MD, Bryan B McCarty MD, Leeva Matthew MD, Brittany Armstrong, Jonathon Berkowitz MD
Northwell Health
Primary Email:rmalhotra2@northwell.edu
Background: Telehealth care models in skilled nursing facilities (SNFs) vary widely, and their success is often attributed to the type of physician or technology involved. However, Northwell Emergency Telehealth Services (NETS) challenges this assumption through its Tele-SNF program, which prioritizes collaboration between emergency medicine physicians and SNF staff. In September 2023, NETS took over virtual care for the Orzac Center for Rehabilitation from an e-ICU service, presenting an opportunity to evaluate and improve virtual care delivery through education and process redesign.
Methods: This quality improvement study employed an observational design. After NETS assumed responsibility for the Tele-SNF program, the team implemented a comprehensive education initiative for nursing staff at Orzac. This included:
In-service training on telehealth consultation procedures.
Simulation exercises focused on role-playing and physical exam training.
Medical education emphasizing early identification of sepsis and appropriate escalation.
The educational content was delivered through in-person visits and virtual sessions, designed to both train staff and align telehealth workflows with existing SNF operations. Program effectiveness was measured by comparing emergency department (ED) admission rates before and after implementation of the education initiative.
Results: Initially, ED admission rates increased after transitioning from ICU physicians to emergency medicine (EM) physicians: (1) Pre-Education: 35% ED admission rate (n=155) and (2) Post-Education: 20% ED admission rate (n=162). This 15% reduction followed the rollout of targeted education, informed by internal quality reviews conducted by an internal medicine physician.
Discussion: The study reveals that physician type alone does not determine the success of a virtual SNF program. Instead, a multifactorial approach—including staff education, strong interprofessional collaboration, and process improvements—is critical. By aligning the telehealth team with SNF workflows, enhancing clinical awareness (e.g., early sepsis recognition), and fostering active communication between remote physicians and onsite nurses, the Tele-SNF program achieved a significant reduction in ED transfers. These findings suggest that virtual care success hinges not on technology or specialty alone, but on systemic alignment, trust-building, and continuous quality improvement.
Increasing access to HIV care through telehealth coordination strategies
Chandler Douglas MA, Erin Starzyk PhD, MPH
JSI Research & Training Institute
Primary Email:chandler_douglas@jsi.com
Background: The abrupt pivot to telehealth in 2020 did not allow for strategic and intentional identification, implementation, and evaluation of telehealth coordination strategies (TCS); particularly for populations experiencing barriers to digital access. In response, the Telehealth Strategies to Maximize HIV Care initiative, launched in August 2022, and funded by the Health Services and Services Administration’s HIV/AIDS Bureau through Part F Special Projects of National Significance, provided a critical opportunity to evaluate how TCS can address the digital divide. TCS aim to increase a clinic's capacity for high-quality, accessible, and sustainable telehealth delivery, and ensure that patients have the information, resources, and support necessary to effectively engage in telehealth services. This initiative focused on identifying and increasing the use of TCS to improve linkage to care, retention in care, and health outcomes for people with HIV who receive services through the Ryan White HIV/AIDS Program (RWHAP).
Methods: To examine the impact of TCS, the project’s multi-site evaluation measured both implementation and client outcomes, including the impact of TCS on RWHAP clinics, providers, and clients. Data collection tools and procedures were designed to capture a variety of measures and data sources to triangulate the Results: and provide a comprehensive picture of the intervention experience. The evaluation approach used the RE-AIM framework to organize and document implementation science findings and address the well-documented research-to-practice gap that negatively impacts outcomes. The key evaluation questions were: (1) To what extent did the TCS enhance the utilization of telehealth for HIV care over the project period; (2) To what extent did telehealth utilization and TCS differ across populations disproportionately impacted by HIV; (3) To what extent did telehealth utilization and TCS contribute to the improvement of health outcomes and quality of life for RWHAP clients; (4) What are the core elements, facilitators, and barriers associated with TCS at the patient, provider, and clinic levels; and (5) What resources and supports are needed to implement telehealth and TCS to increase and access and ensure sustainability?
Results: To support the implementation of TCS, all sites adopted a cross-training telehealth model and integrated telehealth coordinators into their workflows. Over the project period, sites increased their use of TCS by 105.9% (from 17 to 35). Sites enrolled 542 patients. The average age was 49, 61% identified as Black/African American, 41% as Hispanic/Latino, and 87% were under 250% of the FPL. Results: demonstrated improved patient experience: satisfaction rose from 4.42 to 4.48, and comfort significantly increased from 3.23 to 3.34 (p=0.03). On the helpfulness scale, highly valued TCS included appointment walkthroughs (4.59) and patient portal setup (4.55), with 92.3% of patients interested in future telehealth use. Critically, movement across the care continuum was observed: 59.1% of non-virally suppressed patients reached viral suppression, and 88.9% without an active ART prescription-initiated treatment. The project findings validate that telehealth is an essential access strategy, with TCS supporting clinical success and patient investment.
Discussion: Findings show that TCS effectively increase access to telehealth in HIV primary care settings, enhance patient satisfaction, and reduce barriers. Increased understanding of patients’ perceived barriers to accessing telehealth and effective strategies for addressing these barriers supports improved telehealth delivery. In particular, digital navigation strategies tailored to meet the needs of priority populations within the RWHAP, including aging populations and low-income individuals, promotes increased telehealth access by addressing the digital divide. In addition, TCS effectively addressed barriers to retention in care. The findings of this project provide critical information in determining the resources and supports (e.g., workflows, policies and procedures, and staff training and support) necessary for sustainable telehealth program planning.
AI-powered markerless motion capture in rehabilitation: enhancing patient experience and engagement
Shayen Bhatia
Prime Health care
Primary Email:drsunnybhatia@gmail.com
Background: Rehabilitation is critical following strokes, injuries, and surgery, yet nearly half of patients fail to complete their prescribed therapy. This lack of adherence Results: in slower recovery, persistent disability, and reduced quality of life. The barriers are multifaceted—patients often perceive exercises as monotonous, progress is not readily visible, and access to therapy remains inequitable, particularly in under-resourced settings. Existing motion-capture technologies can quantify movement and provide feedback but are typically expensive, complex to set up, and impractical for widespread use in community or outpatient environments. Affordable, scalable solutions that enhance engagement and objectively measure progress are urgently needed to improve patient experience, adherence, and outcomes across diverse populations.
Methods: To address these barriers, an AI-powered, markerless motion-capture platform was implemented in two hospital-based rehabilitation clinics. The system uses a single consumer-grade camera and proprietary neural networks trained in rehabilitation-specific movements to detect joints, quantify motion quality, and provide real-time visual and auditory feedback. This pilot evaluated the platform’s impact on patient experience and usability as part of standard therapy sessions. Seventy-nine patients participated across 150 encounters, representing a range of neurological and musculoskeletal conditions. Patients completed 214 post-session surveys evaluating motivation, confidence, usability, and perceived support using a 0–4 Likert scale. Therapists provided structured feedback regarding ease of integration, patient engagement, and clinical workflow impact.
Results: Feedback was overwhelmingly positive. Seventy-seven percent of patients reported improved control over movement, 66% experienced less fear of injury, and 82% felt more confident in their recovery. Motivation increased in 88%, and 75% reported tangible improvements in strength, balance, or range of motion. Seventy-eight percent demonstrated enhanced body awareness, 76% greater ability to walk or continue rehabilitation independently, and 74% improved participation in work, school, or social activities. Usability ratings were high (95%), and nearly all participants (98%) cited strong encouragement and engagement from their therapy team. Physical therapists (n=16 survey responses from ∼9 providers) reported moderately positive experiences. All therapists (100%) agreed patients valued the technology and found it easy to use. However, only 40% believed it reduced patient anxiety (vs. 72% of patients reporting anxiety reduction). Positive feedback emphasized value for progress tracking and patient engagement, particularly for gait analysis with assistive devices in acute rehabilitation settings. No adverse events were reported.
Discussion: AI-powered markerless motion capture effectively transforms rehabilitation into an engaging, data-driven, and motivating process. By providing objective feedback and progress visualization through simple, scalable technology, it directly addresses long-standing challenges of disengagement and inequitable access. The Results: demonstrate that digital health innovations can meaningfully improve patient experience, therapist satisfaction, and functional recovery, supporting a new paradigm of accessible, AI-enhanced rehabilitation. This AI-powered innovation demonstrates how digital technology can extend equitable access, reimagine rehabilitation, and improve outcomes globally. Larger studies incorporating both patient and provider perspectives are warranted to confirm these Results.
Screening for undiagnosed perinatal depression using telemedicine
Christine Chien MD1, Sina Haeri MD, MHSA2, Vijay Balakrishnan MBA2
1Carle Foundation Hospital and 2Ouma Health
Primary Email:chien.chr@gmail.com
Background: Suicide is a leading cause of preventable maternal deaths, accounting for up to 20% of deaths postpartum. Perinatal depression is on the rise in the United States, affecting 1 in 5 pregnant people. Untreated depression has profound and lasting harm on maternal and infant health, and recognition of early warning signs is crucial to intervening before a mental health crisis occurs. As pregnancy care transitions from the clinic to the digital platform, more investigation is needed on the efficacy of depression screening via telemedicine.
Methods: We conducted a retrospective review of new perinatal patients referred by Managed Care Organizations (MCOs) between May 1, 2023, and July 10, 2025, across multiple states. The Edinburgh Postnatal Depression Scale (EPDS) was administered at each telemedicine encounter, with scores ≥10 considered positive. Patients screening positive were offered virtual behavioral health care. Outcomes were compared by patients' preferred language.
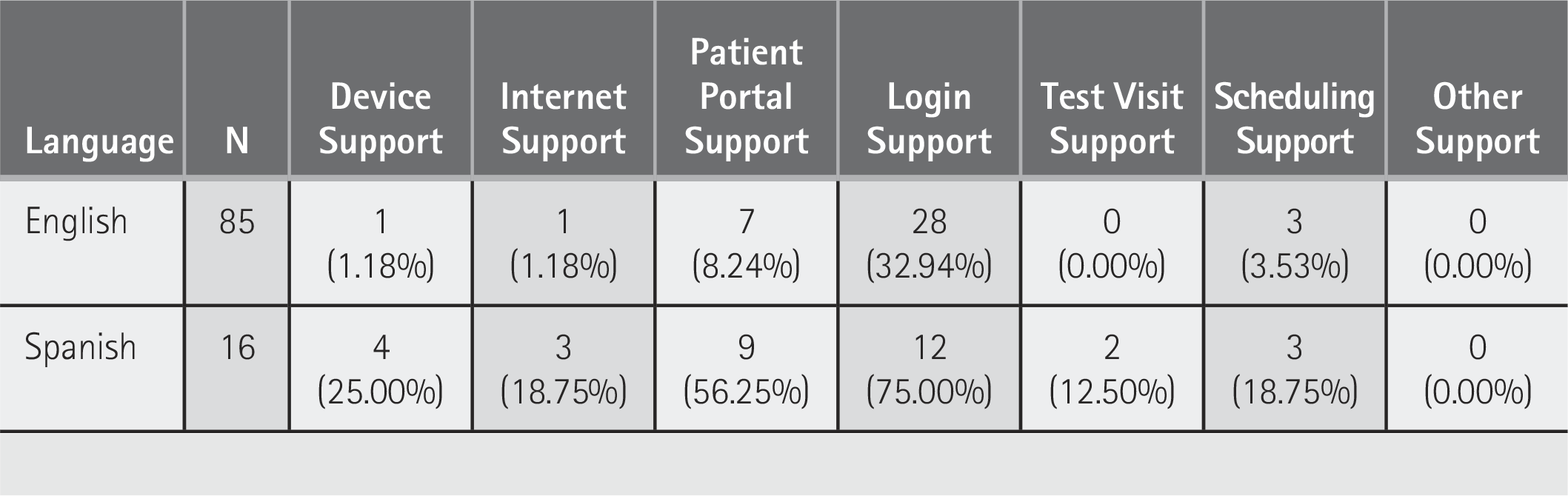
Results: Of 2,291 perinatal patients, 28.5% screened positive for depression. Nearly half (46.0%) of those with positive screens had no prior diagnosis identified by their prenatal care provider at intake. Among patients screening positive, 49.4% were successfully enrolled in virtual behavioral health services. Language disparities were evident: 24.6% of English speakers screened positive compared with 13.3% of non-English speakers.
Discussion: Telemedicine-based screening in Medicaid patients referred from maternity deserts uncovered a high rate of undiagnosed perinatal depression, with nearly half lacking prior recognition. Integration of routine depression screening into antepartum or postpartum visits expands behavioral health access and can bridge critical gaps in underserved populations. This highlights the capacity for telemedicine to address under-recognized contributors to maternal morbidity and mortality.
Exploring the Perceived Ease of Use of a Pharmacy Telebooth Post Pandemic Among Seniors in DC
Brigitte Kwinze Smith PhD, Mary Awuonda PhD, Earl Ettienne PhD, La'Marcus Wingate PhD, Adaku Ofoegbu PhD, Carrie Crowther, Kany Bonnaire, Weetsnie Eloy BS, Ivan Mbam, BS
Howard University
Primary Email:kwinzeb@yahoo.com
Background: The United States (U.S.) has one of the leading health care systems in the world, but scores poorly on many key health measures due to many challenges. However, the pandemic-related shutdown of in-person services forced patients to remote care. Telehealth has been a solution to the growing demand for services and is being implemented as an efficient cost-effective means of delivering health care services. A key factor in the success of telehealth interventions is patient acceptance of the new technology. Given the proven benefits of telehealth as an intervention, its low reported acceptance rate among seniors raises a concern. Currently there is a gap in literature on the development of a new community anchored tele pharmacy practices among seniors. This study aims to examine the predictive effect of factors on perceived ease of use (PEOU) of an innovative medication therapy management (MTM) tele pharmacy service among seniors from wellness centers in Washington DC.
Methods: This was a cross-sectional study conducted among seniors at their wellness centers in Washington DC post pandemic. The primary aim was the acceptability of a community-anchored MTM tele pharmacy called SeeUrPharmacist through a proposed pilot feasibility study. The second aim was an examination of the predictive effect of sociodemographic factors, antecedent factors on PEOU of the new technological system. A validated questionnaire, borrowed from the literature, was used to determine the telehealth acceptability (TA). The first part of the study was to examine whether seniors would be willing to use the telebooth if placed at their center. The second part of the study measured TA as telehealth perceived ease of use rate among seniors at their wellness center. The study recruited 105 participants who took the questionnaire from September to December 2024. Descriptive statistical analysis was conducted for all study variables. Simple and multiple linear regression analysis were conducted to assess predictive factors of perceived ease of use of the telebooth post-pandemic. All statistical analysis was conducted using SPSS version 28 at an alpha level of 0.05.
Results: Of the 105 respondents, 72.4% were female, the mean age was 72.6 ± 7.5 years. 88.6% reported unemployed, 88.6% were African Americans, 71.4% reported using Medicare part D and part C. 57% who tested the SeeUrPharmacist systems self-reported that it was easy to use and does not require a lot of their mental effort. 94.3% of participants agree to use the telebooth if one is placed at their senior wellness center. The majority of the comments were positive and provided a glimpse of possible impediments to implementation of the telehealth MTM services at the centers. The feasibility study findings indicated that telehealth Improved access to care and availability of pharmacy services to seniors and helped save money and time. Meanwhile, lack of touch and holistic quality of care, technology difficulties, and literacy difficulties were challenges faced by seniors. The dependent variable was regressed on predicting variables. Findings indicated that anxiety (B= -1.213, t=-6.334, P < 0.001), system self-efficacy (B= 2.669, t=18.321; p< 0.001), age (B= -1.233, t=-2.108; p< 0.038). And Perception of External Control (B= 1.086, t=8.853; p< 0.001) had significant impacts on Perceived Ease of Use of the new system.
Discussion: The majority of these seniors were willing to use the telebooth if one is placed at their wellness center. This study found that system self-efficacy, perceptions of external control, computer anxiety, and age were significant predictors of the SeeUpharmacist PEOU. These findings were consistent with literature. Thus, it was important to determine individual predictor factors on seniors’ PEOU of the new technology. This study has some limitations that restrict the generalization of the results. Some recommendations were made. First, increase health care access by allowing more internet connections/devises among seniors, creating space for more seniors’ privacy, and offering trainings on online care and how to use new technologies. Second, there is a need for future studies that focus more on the acceptability of pharmacist-led telehealth platforms with the aim of reducing legal and physical barriers that limit pharmacists’ services in the U.S. health care system.
Advancing Telehealth Readiness Through a Student-Led Digital Health Coaching Model
Sonal Batra MD, MST,1 Camille Jefferson BSc,1 Ashley Stevenson BS, MS,1 Sara Belay MPH,2 Manuel Rebol PhD, BSc, MSc,1 Neal Sikka MD1, Colton Hood MD, MS1
1The George Washington University and 2Luminas, LLC
Primary Email:sonal@gwu.edu
Background: Telehealth effectiveness relies on patients’ ability to access, understand, and use digital tools—a challenge for communities facing socioeconomic barriers and limited digital health literacy. Residents in Washington, DC’s Wards 7 and 8 experience persistent health disparities that hinder equitable participation in telehealth. To address these gaps, our institution partnered with the largest local network of Federally Qualified Health Centers (FQHCs), the DC Department of Aging and Community Living, and community organizations to implement a digital health coaching initiative. The program aimed to enhance patients’ digital health literacy, focusing on their patient portal as a gateway to telehealth access and engagement. Simultaneously, it provided experiential learning for students from underrepresented Background: s in health care, building a workforce prepared to advance digital health equity.
Methods: Eighteen students from local health career pathway programs were trained as digital health coaches, with 16 deployed to three FQHCs serving Wards 7 and 8 in Washington, DC. Coaches—primarily high school and college students from underrepresented or low-income backgrounds—conducted individualized 20–30-minute sessions assisting patients in downloading, registering, and navigating their patient portal. Coaching also included instruction on broader digital skills essential for telehealth participation, such as managing email, passwords, and online communication. Across nine months (January–September 2025), coaches delivered 321 total coaching sessions. Coaches administered a brief survey instrument at the end of each session to assess satisfaction, confidence, and perceived readiness to use telehealth platforms. Coaches completed onboarding and exit surveys evaluating training and experience. We report the impact of the program. This project was funded by a grant awarded to Sibley Memorial Hospital by the DC Department of Aging and Community Living.
Results: Of 321 completed sessions, 226 were provided to residents of Wards 7 and 8 (the remainder to residents of other area locations). Participants averaged 55 years of age, representing a range of 16 to 92 years. Following coaching, 98% of participants reported increased confidence in digital skills, 97% expressed high satisfaction, and the program achieved a net promoter score of 92, indicating strong likelihood of recommendation. Among student coaches, 89% engaged in at least one coaching session and 92% reported satisfaction with the experience. Qualitative feedback highlighted improved patient comfort with telehealth tools and strengthened student understanding of health care delivery systems. Coaches valued community engagement and exposure to digital health technologies, noting the program’s positive impact on career readiness.
Discussion: This initiative demonstrated a scalable and sustainable approach to increasing telehealth readiness in digitally underserved communities while fostering workforce diversity. By coupling patient education and empowerment with student development, the model effectively bridged digital access gaps that limit telehealth utilization. As regulatory changes and health care modernization accelerate, programs that enhance patients’ digital confidence are essential to achieving equitable telehealth adoption. Building on these outcomes, future efforts will expand into acute care settings as well as other community-based locations, incorporating patient navigation and broader digital inclusion strategies to strengthen telehealth access across the care continuum.
Characteristics of telehealth education/training for health care professionals and trainees
1Virginia Commonwealth University, 2Medical University of South Carolina, and 3Rams in Recovery
Primary Email:conor.duffy@vcuhealth.org
Background: The duration, content, and activities included in telehealth education/training interventions are inconsistent across institutions. Existing interventions range from single sessions to longitudinal curricula spanning multiple years. Common topics in telehealth education/training include communication skills, legal and ethical issues, and navigating telehealth technologies. Prior research suggests that telehealth education/training interventions are more likely to use didactic (e.g., lectures) than experiential approaches (e.g., standardized patient visits). However, some evidence suggests experiential training is more effective in building self-efficacy and clinical skills. Despite the proliferation of telehealth training programs, no comprehensive study has examined the characteristics and gaps across multiple health care disciplines and institutions simultaneously. This research examines trends in the characteristics of telehealth education/training experienced by health care professionals and trainees across institutions in the United States.
Methods: We recruited samples of licensed health care professionals and health care trainees using Prolific, an online recruitment platform. We targeted six groups of health care professionals—physicians, nurses, nurse practitioners, physician associates, social workers, and clinical/counseling psychologists—as well as trainees from each of these groups. Health care professionals were required to have prior experience delivering synchronous telehealth visits to participate in this study. Trainees were required to be in the clinical stage of one of the following training programs: Doctor of Medicine (MD), Doctor of Osteopathic Medicine (DO), Bachelor of Science in Nursing (BSN), Master of Science in Nursing (MSN), Doctor of Nursing Practice (DNP), Physician Assistant (PA), and Master’s or Doctorate programs in clinical/counseling psychology or social work. Eligible participants who enrolled in the study completed an online survey administered through Qualtrics. This survey included questions on demographics, professional characteristics, and prior telehealth education/training. This research reports descriptive statistics on participants’ formal education/training in telehealth.
Results: Samples of 69 licensed health care professionals and 70 health care trainees completed our questionnaire. Among health care professionals, 63.8% reported receiving telehealth education/training in their training program (median = 6 hours) and 82.6% in a professional setting (median = 16 hours). Sixty percent of trainees had received telehealth education/training in their training program (median = 4.5 hours), and 65.7% had received it in professional settings (median = 4 hours). For health care professionals and trainees, respectively, the most common activities included in education/training were asynchronous lectures (65.2%, 54.3%), while relatively few health care professionals and trainees participated in standardized patient visits via telehealth (27.5%, 40.0%). The most common topics addressed in education/training included conducting assessments/evaluations via telehealth (75.4%, 61.4%), communication skills (62.3%, 47.1%), ethical considerations (59.4%, 61.4%), and history taking/chart review (49.3%, 57.1%). In comparison, the topics addressed least frequently were navigating telehealth platforms (29.0%, 28.6%), performing physical examinations (33.3%, 30.0%), and resolving technological difficulties (39.1%, 21.4%).
Discussion: While most participants in this study reported that they have received telehealth education/training during their training program and/or professional career, our findings revealed several gaps in existing telehealth education/training. Prior research suggests that troubleshooting technological difficulties and performing physical examinations are aspects of telehealth delivery where health care professionals lack confidence, yet these were among the topics addressed least frequently in participants’ prior telehealth education/training. Additionally, our Results: indicated that these interventions focus on didactic education rather than experiential training, despite evidence suggesting that experiential training is more effective in building skills and confidence. These findings provide an evidence-based framework for institutions to redesign telehealth education/training, potentially improving provider confidence and patient care quality. Future telehealth education/training should incorporate technological troubleshooting and physical examination skills while placing a greater emphasis on experiential training.
Telehealth education/training needs: A qualitative examination of health care professionals and trainees
1Virginia Commonwealth University, 2Medical University of South Carolina, and 3Rams in Recovery
Primary Email:conor.duffy@vcuhealth.org
Background: Medical education institutions and health care systems have increasingly adopted telehealth education/training in recent years. However, it is unclear whether existing interventions address health care professionals’ and trainees’ needs and prepare them to use telehealth in practice. Prior research suggests that health care professionals lack confidence in troubleshooting technological difficulties, performing physical examinations, and communicating effectively with patients in telehealth visits. However, much of this evidence was generated in the early stages of the COVID-19 pandemic. Five years removed from the start of the pandemic, it is necessary to revisit health care professionals’ and trainees’ needs for telehealth education/training. This qualitative research assesses telehealth education/training experiences and needs among a sample of health care professionals and trainees across institutions in the United States to better examine unmet needs within the existing training environment.
Methods: Licensed health care professionals and health care trainees were recruited via Prolific, an online recruitment platform. We recruited licensed physicians, nurses, nurse practitioners, physician associates, social workers, and clinical/counseling psychologists, as well as trainees from each of these groups. Health care professionals were required to have prior experience delivering synchronous telehealth visits to participate in this study. Trainees were required to be in the clinical stage of one of the following training programs: Doctor of Medicine (MD), Doctor of Osteopathic Medicine (DO), Bachelor of Science in Nursing (BSN), Master of Science in Nursing (MSN), Doctor of Nursing Practice (DNP), Physician Assistant (PA), and Master’s or Doctorate programs in clinical/counseling psychology or social work. Eligible participants who enrolled in the study completed an online survey administered through Qualtrics. This survey included questions on demographics and professional characteristics, as well as open-ended questions assessing experiences with telehealth education/training and needs for further education/training. A team of three independent coders analyzed these open-ended responses using reflexive thematic analysis.
Results: A sample of 139 participants (69 licensed health care professionals, 70 health care trainees) completed our questionnaire. The research team generated the following qualitative themes: 1) existing telehealth education/training does not fully address health care professionals’ and trainees’ concerns, 2) telehealth education/training should emphasize troubleshooting skills, 3) training/education and real-world experience facilitate greater self-efficacy, and 4) one size (generic training) does not fit all. While existing telehealth education/training interventions help to build telehealth knowledge and skills, many participants’ most significant concerns about telehealth delivery were not adequately addressed by their education/training. Specifically, many participants reported feeling unprepared to navigate unexpected technological difficulties, complex medical scenarios, and patients with low digital literacy during telehealth visits, and that experiential training (e.g., standardized patient visits) is beneficial in building these skills. Training should be tailored to the specific contexts (e.g., medical specialty, typical patient population) in which health care professionals and trainees use telehealth.
Discussion: Our findings suggest that many health care professionals’ and trainees’ concerns around telehealth delivery have not been sufficiently addressed by their education/training. Improvements to telehealth education/training are necessary to better prepare health care professionals to use telehealth. Telehealth education/training curricula should emphasize technological troubleshooting skills and tailor education/training to the specific contexts in which health care professionals and trainees use telehealth. Additionally, experiential training, such as standardized patient visits, is beneficial for preparing health care professionals and trainees to use telehealth. In contrast, didactic education alone is insufficient to prepare them to use it in practice. Future research should build upon this work by examining telehealth education/training experiences and needs among specific health care professional groups and medical specialties.
Does use of digital health technologies improve asthma?
Kandia Lewis PhD, Cynthia Zettler-Greeley PhD, Kathryn Blake PharmD, David Fedele PhD, ABPP
Nemours Children's Health
Primary Email:kandia.lewis@nemours.org
Background: More than half of children with asthma, a common chronic lung disease, have uncontrolled asthma. Uncontrolled asthma is costly and disrupts lives as it can lead to significant morbidity and health care utilization. Digital health technologies may assist caregivers in managing their child’s asthma, ultimately leading to improvements in their child’s health. This study examined the Nemours app, a digital health application designed to facilitate access to care and assist caregivers with asthma management. The purpose of this study was to evaluate: 1) whether more app use predicted better asthma outcomes, 2) which app features predicted better asthma outcomes, and 3) whether caregiver and child demographics correlated with (a) more app use and (b) better asthma outcomes.
Discussion: Preliminary findings indicate caregivers across socioeconomic, racial, and ethnic Background: s utilized digital health technologies to help manage their child’s asthma. Families receiving Medicaid tended to log into the app more than those who did not receive Medicaid, suggesting digital health may be an important tool for families with low-income. The most frequently utilized features used to manage child asthma, messages and asthma tracker, may help facilitate communication between caregiver-children and their care teams. Moreover, caregivers who sent more messages to their child’s provider tended to have higher health literacy scores at the end of the study, indicating app-facilitated communication may help enhance outcomes. This study demonstrates how integrating digital health technologies into asthma care may lead to improved pediatric asthma outcomes. Findings highlight potential benefits of using digital health technologies to provide care among diverse patient populations.
Expanding pediatric access: An agile virtual immediate care model
Tara Seider, APN-NP, Bridget Hillman, Dana Schinasi MD
Ann and Robert H. Lurie Children's Hospital of Chicago
Primary Email:tseider@luriechildrens.org
Background: We developed a flexible, hybrid scheduling model for virtual immediate care (VIC), blending on-demand and scheduled visits to increase access, optimize utilization, and support high-quality virtual care. Since launching four years ago, we have refined the model using data-driven adjustments to balance patient volume, wait times, and provider capacity. By allocating scheduled visit slots alongside responsive on-demand coverage, the VIC model improves operational efficiency and aligns with best practices. This presentation will outline key strategies for implementing and sustaining a VIC program, including the rationale and efficiency benefits of a hybrid model, Methods: for matching provider resources to fluctuating demand, digital tools that streamline operations, and associated financial and operational impacts. Attendees will gain practical insights into a patient-centered, data-driven model that strengthens care delivery and supports sustainable, adaptable services.
Methods: Drawing from in-person urgent care workflows, we developed online scheduling decision trees to guide families to appropriate self-scheduled telemedicine visits. The provider pool was expanded using a moonlighting model to support efficient and scalable staffing. Agile scheduling aligns provider shifts with real-time demand, reducing underutilization while preserving clinician flexibility. Utilization dashboards enable continuous monitoring of visit volume, staffing patterns, and performance metrics, and standardized billing workflows ensure accurate charge capture. The model supports timely patient access, promotes provider satisfaction, and maintains a sustainable program margin after compensation.
Results: Since December 2021, VIC has delivered more than 4,000 virtual appointments, broadening access for families across Illinois and reducing unnecessary emergency department visits. The agile model enables real-time demand management, reducing provider downtime and increasing access. Utilization dashboards and operational data improve efficiency and support financial sustainability. The program consistently meets target utilization rates needed to maintain a strong margin after provider compensation, ensuring timely access, high satisfaction, and high-quality care. Approximately 15% of patients are new to the organization, with VIC functioning as a safety net for patients without a primary care provider or those who left the emergency department without being seen. Escalation workflows and billing processes facilitate transitions to in-person care when needed. MyChart integration enhances access, flexibility, and satisfaction. The ability to adjust appointment availability in response to trends and surges supports stable, high-quality care without operational strain.
Discussion: The agile, hybrid VIC scheduling model balances on-demand and scheduled visits to expand access, optimize utilization, and align with best practices. Strategic resource allocation supports operational efficiency and institutional goals while maintaining care quality. Attendees will learn flexible, data-driven approaches for designing models that improve access and sustainability. Future directions include adapting the model for populations with urgent behavioral health needs. The VIC hybrid model demonstrates continuous improvement and illustrates how virtual care teams can remain adaptable while optimizing efficiency and quality in pediatric telehealth.
Tracking the Pulse of Telehealth Evolution: A 16-Year Longitudinal Analysis of Technical Assistance Topics
Elizabeth Krupinski PhD
Emory University
Primary Email:ekrupin@emory.edu
Background: The Southwest Telehealth Resource Center (SWTRC), funded by the Health Resources and Service Administration’s Office for the Advancement of Telehealth, started offering technical assistance (TA) in 2009, receiving requests for assistance over a wide spectrum of topics. Since 2009, there have been significant changes in the way telehealth is offered, forces driving adoption (e.g., COVID pandemic), patterns of reimbursement, legislation, and other factors. We hypothesize that, reflecting these changes, the volume of TA requests for specific topics has changed over the past 16 years as telehealth has evolved and become more established. Tracking and analyzing changes in the volume of requests for help in establishing or expanding telemedicine programs is a critical leading indicator of health care system transformation, policy impact, market demand, and operational readiness. Monitoring these changes not only serves to help with SWTRC’s strategic planning efforts but also may provide actionable intelligence for policymakers, funders, technology providers, and health systems seeking to accelerate access to virtual care.
Methods: Since the inception of the TRC program, HRSA has required regular activity reports and has worked with all 14 TRCs to create a standard set of reportable TA topics. These have changed over the years but overall have maintained core themes and topics that can be merged into the current ones. Data from September 2009 when the program started through the end of November 2025 were included in the present analysis. Initial analyses examined overall trends across years, and subsequent analyses examined trends in specific topics across the years. As some categories were added over the years, data only represent the years in which those data were collected. There were some categories that were merged for these analyses due to low frequencies (e.g., mental/behavioral health merged into clinical, broadband into technology).
Results: The most common topics across years were general information questions (22.79% of all requests/year on average) that required follow-up to get more specific; followed by training and/or our training program (22.79%); and questions about what does SWTRC do/offer (19.5%). The next 3 most common topics were legal (7.12%), technology (6.71), and clinical (5.16%); followed by financial/billing (4.53%), COVID (4.39%), strategic planning (4.26%), tools/templates (3.72%), and evaluation (6.71). There were notable trends by topic. COVID was added in 2020 when it peaked at 16.36%, dropping to 7.14% in 2021 and less than 1%/year through 2025. General information questions predominated 2010 -2018 (range 313.54% - 78.67%), then dropped (4.85% - 20.75%). Legal questions were low 2010 – 2018 (0% - 14.87%) then increased (6.82% - 17.55%) starting in 2019. Technology questions remained constant 2010 – 2022 (1.39% - 8.44%) then increased in 2023 (11.81%-13.59%). Strategic planning questions were not frequent 2010 – 2018 (0% - 1.45%) then increased thereafter (4.53% - 15.79%). Requests for tools/templates peaked in 2020 (16.36%) then tapered off (0.53% - 7.14%). Financial/reimbursement remained steady across the years (2.45% - 7.25%) as did evaluation (0.23% - 5.83%).
Discussion: Technical assistance through organizations like the SWTRC emerged in the mid-2000s and these organizations remain valuable resources for those building and/or expanding telehealth programs. Some interesting trends over the past 16 years include fewer generic inquiries about telehealth or the SWTRC, and more focused initial questions on specific topics, reflecting broader awareness and knowledge about telehealth in more recent years. The increase in legal questions is not surprising given the significant changes in regulations, especially since COVID, although the lack of significant increase in financial questions was surprising – although the two are closely related so often get asked in terms of the legal side of the issue. COVID clearly had an impact, particularly on strategic planning and requests for tools/templates – readymade items that could be implemented quickly and without the need to develop or modify. Tracking trends in assistance topics provides some insight into the state of telehealth use and maturity, and helps the SWTRC strategize its future directions and foci.
Leveraging patient-reported experiences to improve enrollment in a virtual behavioral health program
Caitlin Koob PhD, MS, OTR/L, Emily Johnson PhD, Andrew Alkis MD, Candace Sprouse-McClam PhD, LISW-CP (S), LCSW, Katie Kirchoff MSHI, Jennifer Dahne PhD
Medical University of South Carolina
Primary Email:cak240@musc.edu
Background: Psychiatric collaborative care management (CoCM) effectively addresses mental and behavioral health, due to its implementation in primary care settings and its reliance on 1) team-based care, 2) population-focused approach, and 3) measurement-based care. However, CoCM uptake in rural communities remains challenging for a variety of reasons, including the ongoing shortage of behavioral health providers within local communities. Therefore, our telehealth-enabled CoCM program seeks to improve access and quality of mental and behavioral health services across rural South Carolina. Following our pilot study and expansion to 44 primary care clinics statewide, the purpose of this study was to describe barriers and facilitators to telehealth CoCM patient enrollment from patients’ perspectives.
Methods: This study was part of a larger quality initiative to improve the enrollment and sustained involvement of patients with mental and behavioral health concerns in rural South Carolina, based on their experiences with the CoCM program from referral through sustained enrollment. This mixed-Methods: evaluation involved data from multiple sources, including patient’s electronic health records and patient-reported experiences among those who decided to enroll and those who did not enroll, via surveys (Nf119) and interviews (Nf13), to inform program improvements and leverage data-driven decisions. Patient’s demographic characteristics and information regarding their participation in CoCM (i.e., referral, days enrolled, graduation) were extracted from the electronic health record. Descriptive statistics and rapid qualitative data analysis were conducted to comprehensively evaluate targeted outcomes.
Results: Over the past year, CoCM has grown to serve 44 primary care clinics statewide, compared to 18 clinics previously. From 06/01/2023 through 06/30/2024, 303 patients were referred to CoCM and enrolled (58.4% of total referred patients), and 112 of enrolled patients (37.0%) graduated from the program. Of those who enrolled, patients participated in CoCM for a mean of 164 days. Enrolled patients largely reported experiencing improvements in their mental health since joining CoCM (62.5%) and highlighted benefits of the telehealth-enabled delivery, accessibility, flexibility, and program support in their decision to enroll and maintain their involvement in the program over time. The majority of those who did not enroll reported that they did not remember receiving program information from their primary care provider (58%), but a similar program would be beneficial to their health and well-being (68%).
Discussion: Feedback from referred patients, including those enrolled and not enrolled in the CoCM program, can inform data-driven decisions to improve accessibility, patient outcomes, and long-term scalability. Last fall, CoCM transitioned from grant funding to standard billing practices, and its impact continues to grow with the program. Next steps include robust analyses of patient-reported data (i.e., sleep and mood trackers, clinical screening tools) in a patient-facing telehealth platform. Additional sustainability measures include revenue per program participant, rather than reliance on grant funding, and revenue growth rate (month-over-month) from program participants. Further work is needed to describe the utility of the CoCM program, understand its impact on patients’ health care access, and evaluate the sustainability of this model.
Redesigning Access: A Virtual Approach to Specialty Care Delivery
Caitlin Koob PhD, MS, OTR/L, Jillian Harvey PhD, MPH, Dunc Williams PhD, MHA, Kit Simpson, DrPH, Katie Kirchoff, MSHI, Peter Gardella MBA, BSN, RN, Cortney Belton MBA, BSN, RN, James McElligott MD, MSCR, Dee Ford MD, MSCR
Medical University of South Carolina
Primary Email:cak240@musc.edu
Background: Patients often face significant barriers to accessing in-person specialty care, leading to long delays and poor health outcomes. Waitlists for specialty care can extend up to six months. Further, providers in in-person settings frequently experience high workloads, limited flexibility, and resource constraints, contributing to dissatisfaction and emphasizing the need for alternative care models to support provider well-being. To address these challenges, we developed and implemented a virtual specialty service line to improve access and reduce wait times, while considering patient and provider preferences for service delivery. This model offers fully virtual care across high-demand specialties and primary care, while coordinating in-person services (i.e., labs, imaging, and pharmacy) in the patient’s local community. The purpose of this study is to evaluate the impact of a virtual specialty program on physician productivity and patient utilization across all specialties.
Methods: This study is part of a larger quality initiative to evaluate the impact of a virtual specialty program on patient, provider, and systems outcomes, compared to in-person visits. These analyses focus on various measures of patient utilization and provider productivity and rely on multiple data sources, including patients’ electronic medical records and physician productivity (i.e., relative value units, or RVU, data), to evaluate the multi-level outcomes of a virtual specialty program compared to in-person clinic visits. Key outcomes examined in this study include an array of patient utilization metrics, including visit type (using Current Procedural Terminology [CPT] codes), average appointment wait times, percentage of new and returning visits, and provider RVUs. For these analyses, each visit was categorized as being provided by a virtual specialty or in-person clinic provider and compare patient utilization metrics across specialties. Descriptive statistics were used to compare virtual specialty care and in-person utilization. By examining key performance indicators, we explore how to reduce barriers to specialty care, enhance multi-level outcomes, and improve efficiency.
Results: Occurring between January and June 2025, our sample is comprised of 65,920 visits, including 10.0% virtual visits and 90% in-person visits, across all specialties. Blue Cross Blue Shield was the most common payer for patients who received virtual visits (40%), while Medicare covered 49% of in-person visits. Neurology was the most common specialty service received in-person (26%), and Endocrinology was the most common for virtual visits (28%). The most common service type across all specialties and visit type was for an established patient visit with moderate complexity (CPT Code 99214; 37% of virtual visits and 35% of in-person, respectively). Second, 22% of virtual visits were for new patients (CPT code 99204) and 14% of in-person visits were for (14%) for established patients with high complexity (CPT code 99215), potentially pointing to appropriate allocation of in-person and virtual specialty services based on patient need.
Discussion: Offering a virtual-only specialty service can significantly improve access for patients, especially in underserved or rural areas with significant specialty provider shortages. Our data shows high utilization of virtual visits for specialties, suggesting strong demand. While specific procedures require in-person care, virtual specialty services may expand access to new patient populations, improve continuity, reduce wait times, and optimize resource allocation. Strategic implementation could lead to more effective health care delivery and better patient outcomes. Ongoing analysis will examine physician productivity, visit outcomes (e.g., cancellation, no-show rates), patient satisfaction, and provider satisfaction across virtual and in-person groups.
Evaluating the impact of a virtual nursing model on nurse-reported experiences and outcomes
Caitlin Koob PhD, MS, OTR/L, Jillian Harvey PhD, MPH, Dunc Williams PhD, MHA, Kit Simpson, DrPH, Katie Kirchoff, MSHI, Peter Gardella MBA, BSN, RN, Emily Warr MSN, RN, Dee Ford MD, MSCR
Medical University of South Carolina
Primary Email:cak240@musc.edu
Background: Systemic gaps in health care delivery in the United States have created workforce issues that impact patient outcomes and costs. As a result, there is growing concern for an estimated deficit of 3.2 million health care workers by 2026 nationwide; in one state, 39% of surveyed nurses reported intentions of leaving their job within one-year.
To address these concerns, a Virtual Nursing model (VRN) was developed as an innovative care delivery model, leveraging teams of remote, virtual nurses to support bedside nurses in providing care via technology. This VRN model was rapidly implemented across 36 units within a large academic medical center. This study evaluates the perceived value and attitudes towards this VRN model from bedside and virtual nurses’ perspectives, following its pilot implementation.
Methods: Bedside and virtual nurses’ perceptions of the VRN program were evaluated, using an internally developed electronic survey. This survey was designed among an interdisciplinary operational and research team to evaluate bedside and virtual nurses’ perceived value and attitudes towards the rapidly implemented VRN model, following its pilot implementation. From May 22nd through September 9th, 2025, this survey was distributed among 692 nurses (650 bedside nurses and 42 virtual only contract nurses) across all VRN units. Notably, contract nurses were excluded from this sample. Surveys were delivered via a Research Electronic Database Capture (REDCap) link to the nurse’s institutional email address, and two follow-up reminders were sent to optimize response rate. A total of 143 surveys, including 113 bedside nurses and 30 virtual nurses (17.3% and 69% response rates, respectively), were analyzed. Descriptive statistics and rapid qualitative data analysis were conducted to comprehensively evaluate targeted outcomes.
Results: Overall, nurses had a mean of 13.22 (SD=13.4) years of experience. Virtual nurses, specifically, had a mean of 8.1 (SD=4.4) months of VRN experience. Further, the majority of nurses’ reported team-based care (63%) and time saved, particularly on admission documentation (61%) and more time for rounding (54%), as benefits. Additionally, 29% of nurses reported improved satisfaction and 27% felt the patient experience improved since VRN implementation. Most nurses also reported being very satisfied with VRN (61%) and 87% of bedside nurses said it slightly or significantly decreased workload. Nurses ranked various uses of VRN as a 4 or 5 on a 1-5 scale (with 5 being the most impactful), including admissions (92%), discharges (36%), quality documentation/surveillance (31%), patient education (25%), and care planning (20%). Reflecting quantitative findings, virtual nurses reported that this “team” approach to nursing “is the future,” and that this role has allowed them to “stay in the field that [they love].” Further, bedside nurses also reported that VRN “restored [their] faith in bedside nursing,” “has made the work day so much better,” and is the “first organization [they’ve] worked with that took steps to reduce [workload burden].”
Discussion: This study is situated within a larger, multi-level evaluation of the VRN model’s impact on patient, provider, and systemic outcomes. Favorable perceptions of the VRN model from bedside and virtual nurses indicate feasibility of continued VRN expansion across innovative use-cases, including high-touch departments such as emergency departments and intensive care units. Further, the ongoing multi-level evaluation may consider the financial return on investments, such as improved throughput and/or decreased turnover rates across units with VRN support, and the effect of prioritizing the VRN queue for optimal efficiency—improving satisfaction among patients and providers alike.
Operations of a virtual nursing unit: Understanding activity patterns, time spent, and identifying opportunities
Caitlin Koob PhD, MS, OTR/L, Kit Simpson DrPH, Jillian Harvey PhD, MPH, Dunc Williams PhD, MHA, Katie Kirchoff MSHI, Peter Gardella MBA, BSN, RN, Emily Warr MSN, RN, Dee Ford MD, MSCR
Medical University of South Carolina
Primary Email:cak240@musc.edu
Background: Following COVID-19, national health care executives have raised concerns for the state of the current nursing workforce and its ability to meet service demands. Nationally, departure rates among nurses rose by 13% in one-year. South Carolina (SC) has the second highest projected nursing shortage in the U.S., estimating loss of 16.6% of registered nurses by 2030. Virtual nursing programs (VRN) are evolving, offering an innovative care delivery model to support retention and alleviate workload burden for bedside nurses. Still, prior research has largely focused on single-site implementation, with little understanding of provider-level outcomes or operational management of such programs. In a large health system in SC, a VRN program was rapidly implemented across 36 units in 2024. The purpose of this study is to understand patterns of VRN activities, including the distribution of time spent (in minutes), and consider opportunities for prioritization within a VRN queue.
Methods: This study involved a retrospective analysis of VRN data from January to June 2025 across 36 units systemwide, following the rapid expansion period. Data for these analyses were triangulated from multiple sources, including information from patients’ electronic health records and program tracking within the Research Electronic Data Capture System (REDCap).
Primary outcomes include VRN utilization data, service unit types provided by VRN, and time spent per VRN task. Service unit types describe the support provided by VRN, including tasks related to admission, discharge, care plan, education, quality-of-care surveillance, and documentation compliance. Descriptive statistics were used to understand patterns of VRN support across service types, identify the number of services combined in visits, and estimate the mean number of minutes spent performing each type of task. Analyses were conducted using SAS v.9.4.
Results: From January through June 2025, VRN provided support for 23,516 admissions, including 58,793 specific tasks. Overall, VRN supported 60.2% of total hospital admissions. VRNs primarily provided support for admissions (65%), quality-of-care surveillance and associated tasks (18%), and discharges (17%), and often provided multiple types of care within one visit. Over the six-month period, the amount of VRN support provided, assuming standard 2,080 work hours per FT/year and 80% productivity, would require 10.2 full-time nurses. Across service types, visits lasted a mean of 36.8 minutes (SD=27.0) with longer visits time for admissions alone (M=34.6, SD=26.9), or 44.7 minutes when combined with care planning or education. Quality-of-care visits lasted a mean of 9.3 minutes (SD=6.5), or 23.8 minutes with education. Discharge visits lasted a mean of 25.5 minutes (SD=12.3), or 23.0 minutes (SD=11.4) with education. Lastly, 61.8% of discharges occurred in < 3 hours from time of order with VRN support, indicating an opportunity to impact throughput metrics and contribute to the financial viability of the VRN program.
Discussion: VRN programs were largely developed for operational and workforce support and, while these programs effectively offset time-consuming tasks and continue to evolve nationally, there is a growing need for metrics to manage VRN teams and increase health care efficiency in inpatient care. This work provides a baseline understanding of VRN support allocation within one health system; however, further research is needed to understand its impact on multi-level outcomes. Specifically, our Results: point to the need for future research to evaluate the system-level impact of VRN support on a myriad of quality, workforce, and financial metrics. Ongoing efforts may consider prioritizing the VRN queue to measure impact on specific outcomes (i.e., timeliness of discharge), examine the impact of VRN support on nursing workload, and the cost-effectiveness of VRN in improving nursing-sensitive quality measures and throughput.
Acceptability of AI generated synthetic health literacy videos
Neal Sikka MD1, Rachel Harbut BA1, Lisa Fitzpatrick MD1, Alice Dragnea PhD2, Shi Feng PhD2
1Grapevine Health
2George Washington University
Primary Email:neal.sikka@grapevinehealth.com
Background: As artificial intelligence (AI) becomes increasingly integrated into health care communication, understanding patient trust and willingness to act on AI-driven recommendations has emerged as a critical area of research. While AI has shown promise for some health care functions, its effectiveness hinges on patients' perception of credibility, relatability, and trustworthiness. Prior studies reveal a complex interplay between trust, perceived competence, and the emotional dimensions of health care communication. They highlight the need for deeper investigation into how patients perceive AI vs human guidance, particularly how these perceptions influence behavior and follow-through. The objective of this study is to determine if participants’ rankings across different dimensions (trust, quality, clarity, preference) differ in their evaluation of health literacy videos made using live recordings of a real doctor vs synthetic outputs generated with their AI avatar.
Methods: We developed 3 sets of paired, short, health literacy videos with either live recordings of a doctor or their AI avatar. In both versions, a prompt was posed via a live recording of a community member and edited with the doctor's message. After IRB approval, we used an online platform (Prolific, London UK) to identify interested users who were directed to a Qualtrics survey, completed a consent form, completed a personality traits instrument, recorded if they had diabetes or hypertension, and whether they had a PCP. Participants were randomized to see “this page left intentionally blank” or “the primary care video was made with AI” starting screen. Then they were presented 3 videos in random combinations to watch and complete stacked rankings for each combination of videos on the dimensions of trust, preference, clarity, and quality. Participants received $5 in compensation for spending on average 10.5 minutes on research activities. Demographics data were collected from Prolific.
Video combinations & topics, Ntn = nutrition, PC = Primary care, HTN = Hypertension, A = live recorded, B = AI avatar
ID
Video 1
Video 2
Video 3
1:
Ntn A
PC A
HTN A
2:
Ntn A
PC A
HTN B
3:
Ntn A
PC B
HTN A
4:
Ntn A
PC B
HTN B
5:
Ntn B
PC A
HTN A
6:
Ntn B
PC A
HTN B
7:
Ntn B
PC B
HTN A
8:
Ntn B
PC B
HTN B
Results: Participants (Nf254) were 55% female; 43% Black, 45% White; had a median age of ∼39; and reported having 57% hypertension, 71% diabetes, and 95% regular PCP. We excluded participants who did not watch all 3 videos from the analysis, leaving 204 participants. Given the interdependence of rankings in the study design, a Linear Mixed Model (LMM) that accounted for random effects of the topics and videos was used to test the null hypothesis that mean rankings of live recorded and AI avatar videos are the same (alpha =0.05). Equivalence testing using two one sided tests (TOST) was used setting less than 0.33 difference in ranking as equivalent. Demographic factors were accounted for as random effects in the LMM, allowing for the isolation of the effect of video type (live recorded vs. AI avatar) from participant-level or topic-level variance. For each outcome, trust, quality, clarity, and preference, between real and synthetic video, rankings were statistically equivalent (all p-values< 0.05).
Discussion: Improving health literacy remains challenging due to suboptimal assessment Methods: and resource-intensive interventions. AI generated video content provides mechanisms for enabling scalable, personalized patient education; however, this approach must maintain patient trust to succeed. In our study, participants ranked videos utilizing AI avatars of real doctors as equivalent to those using real doctors across measures of trust, clarity, preference, and quality, regardless of video topic. This study shows that human based AI avatars are acceptable messengers that support the use of synthetic health video content to tackle health literacy challenges. Further studies should evaluate the feasibility of prompt based AI characters, impact of AI use disclosures, and influence of other related contextual information in health literacy on patient perceptions and likelihood to take action.
C-TRaP: Turning Evidence into Better Care for Everyone, Everywhere in the Era of AI
Amir Erfan Zareei Shams Abadi MS1, Parthaw Goswami BS1, Praveen Rao PhD1, Dima Dandachi MD, MPH1, Sue Boren PhD1, Benjamin Casterline PhD1, Lindsey Kuiper PhD2, E. Rachel Mutrux BA1, Svara Narain MS2, Hubert Miller PhD1, Mirna Becevic PhD1
1University of Missouri 2University of Mississippi Medical Center
Primary Email:becevicm@umsystem.edu
Background: Access to high-quality and timely health care remains a persistent challenge in rural areas and other low-resource non-academic health care settings. Barriers include geographic isolation, insurance coverage, and other socio-economic factors. The University of Missouri-based Missouri Telehealth Network (MTN), with decades of experience in telehealth education, delivery and research, recognized the critical need for rigorous evidence on how telehealth influences patient outcomes, costs, and policy. In response, the Center for Telehealth Research and Policy (C-TRaP) was established in September 2025, with the support from the Health Resources and Services Administration (HRSA), to generate data-driven insights for shaping scalable and transformative telehealth practices and policies in rural areas.
Methods: C-TRaP brings together a multidisciplinary team of researchers, clinicians and policy experts from the University of Missouri (School of Medicine, Sinclair School of Nursing, College of Health Sciences, and College of Engineering), Michigan State University, and the University of Mississippi. The Center’s strategy encompasses five projects: evaluating remote patient monitoring (RPM) for congestive heart failure (HF) patients in readmission reductions, analyzing telehealth utilization among rural Medicaid beneficiaries pre and post COVID-19 pandemic, examining the impact of clinician participation in Project ECHO (Extension for Community Health care Outcomes) on prescribing behavior, identifying adoption drivers and barriers across 34 ECHO hubs, and developing a secure, privacy-reserving federated learning (FL) repository to facilitate de-centralized AI model training on telehealth and ECHO data from participating providers.
Results: While C-TRaP is newly established and most of the data collection and analysis is still ongoing, it has already mobilized resources and infrastructure. Thanks to the HRSA grant, the team has built partnerships across multiple disciplines and institutions, aligned research priorities, and began the work. We will present our preliminary Results: from one of the five projects at the next SEARCH conference in 2026.
Discussion: C-TRaP represents a strategic, evidence-based response to address the challenges in rural telehealth delivery in the era of AI. By integrating RPM, machine learning, administrative claims data and collaborative care models like Project ECHO, the center aims to not only improve clinical outcomes but also inform policy that supports sustainable telehealth expansion. The use of FL may provide a new model for secure, scalable data sharing in health care, mitigating privacy concerns, and enabling rich predictive analytics. Over time, findings from C-TRaP have the potential to influence telehealth reimbursement and regulatory frameworks, best practices at local, state and national levels – ultimately improving quality of care for patients in rural and low-resource areas.
Digital Inclusion: A Critical Component of Telehealth Education
1Ellmer School of Nursing at Old Dominion University and 2Medical University of South Carolina
Primary Email:kgarber@odu.edu
Background: While telehealth has been shown to increase access to care, reduce cost, and improve outcomes, failure to consider digital equity and existing disparities may worsen inequities rather than improve them. It has been suggested that the digital divide is now a social determinant of health and that digital skills and connectivity are super social determinants of health. Ensuring effective telehealth requires providers to be well-informed about the impact of digital literacy, the digital divide, digital health literacy, cultural competency, and accessibility on successful patient outcomes. Yet, many are not familiar with these essential concepts. This presentation will provide a high-level overview of these important factors and highlight essential components of telehealth education to ensure inclusive, accessible virtual health care for all.
Methods: Pediatric-focused advanced practice providers at a national conference were presented with insights on digital disparities as new social determinants of health. They were educated on essential considerations for inclusive telehealth to enhance digital health equity. Content included a focus on the digital divide, digital literacy, accessibility, and cultural competency, with guidance on how to overcome digital disparities (DD). The importance of viewing their plan of care through the patient’s worldview was emphasized. Throughout the session, participants were asked to answer questions electronically to gauge their existing knowledge of these concepts. Upon completion of the session, their overall perceived improvement in knowledge of the topic was assessed with one question, along with completion of an evaluation of the presenters and the session as a whole.
Results: Approximately 56% (27/50) of participants responded to the questions. Most attendees (44%) reported practicing telehealth for 3-5 years, 17% indicated 1-3 years, 28% less than one year, 6% 5-10 years, and none over 10 years. The majority (67%) reported no education on telehealth prior to providing virtual care. Of those who reported telehealth education, only 5% indicated that it included DD. The majority (68%) recognized DD as a new social determinant of health. Most (76%) reported that their practice does not routinely examine a patient’s access to the internet or devices, and 82% do not assess a patient’s digital literacy before scheduling a telehealth visit. Half of the participants (52%) did not recognize that Federal laws regarding accessibility apply to telehealth, with only 34% reporting having adaptive features in their technology. Additionally, few practices use digital navigators (8%). All (100%) respondents indicated that as a result of the session, their knowledge of the subject increased, though only 97% indicated they would apply the content to their telehealth practice. The overall rating for the session was 4.68/5 and 4.67/5 for each speaker, respectively.
Discussion: Digital disparities can significantly impact access to virtual care. Telehealth education must include this essential content. Educating providers with didactic content about digital disparities and digital equity allows providers to acquire and apply knowledge that is essential to ensuring inclusive and accessible virtual care for all. All attendees expressed increased knowledge as a result of the session. Telehealth education for current and future health care providers must include content on digital disparities and mechanisms to overcome these barriers to ensure that all patients can benefit from telehealth.
Cellphone Access and Telehealth Utilization Among People Experiencing Homelessness
Background: Telehealth is increasingly used to expand health care access; however, its effectiveness depends on reliable access to communication technology. People experiencing homelessness (PEH) face unique technological barriers that may limit engagement with telehealth services.
Methods: This pilot study examined cellphone access, telehealth utilization, and perceived barriers among sheltered and unsheltered PEH attending free community clinics in Virginia Beach, Virginia. Data was collected via an orally administered survey. Telehealth use was compared between individuals using government-issued versus non–government-issued cellphones, and barriers were analyzed by housing status.
Results: Seventy-four participants were surveyed; 53% were sheltered and 47% were unsheltered. Cellphone access was reported by 97% of sheltered participants compared with 74% of unsheltered participants. Significant barriers to telehealth utilization included the cost of devices (p = 0.013), limited ability to charge phones (p = 0.048), and lack of mobile data (p < 0.001). Participants using non–government-issued cellphones were more likely to use audio-only telehealth services than those using government-issued devices.
Discussion: Although many PEH report having access to a cellphone, structural and technological barriers continue to limit telehealth use. These findings highlight the need for targeted interventions addressing device affordability, charging access, and data availability to ensure telehealth can function as an equitable health care delivery model for PEH. Results: are exploratory and limited by sample size.
Cultivating Telehealth Skills: The Art of Educating Nurse Practitioner Students
1Medical University of South Carolina and 2Old Dominion University
Primary Email:chikehar@musc.edu
Background: Telehealth has demonstrated its ability to expand access to high-quality health care and decrease health care disparities, leading to improved patient outcomes. Preparing health care providers on the appropriate use of telehealth is critical. Telehealth education and experiential learning opportunities promote its adoption into practice and increase satisfaction for patients and providers alike. Although telehealth education is increasingly being integrated into nurse practitioner (NP) education, few curricula are comprehensive, and many may not address all competencies within their programs. This presentation will provide a high-level overview of how telehealth competencies were scaffolded within an NP program.
Methods: Telehealth modules focused on NP telehealth competencies were integrated into the NP curriculum at a southeastern college of nursing. The modules were standalone components within each course and aligned with the courses’ foci. NP telehealth competencies included: Definitions, Digital Disparities, Technology & Equipment, Laws & Regulations, Security & Privacy, Telehealth Etiquette & Professionalism, and Virtual Physical Exam Skills (with/without peripherals). Completion of the telehealth modules was mandatory but did not affect the students’ overall course grade. The satisfaction survey was voluntary. Most modules consisted of a pre-/post-knowledge assessment, pre-recorded lectures and resources, and a satisfaction survey. The final advanced care and reasoning clinical course incorporated a simulated telehealth visit during the students’ objective structured clinical examination (OSCE), where students had to demonstrate virtual exam skills without the use of telehealth peripherals. Some students volunteered to participate in another simulated telehealth visit during the last two semesters of the program, which involved working with a telepresenter (prelicensure student) and telehealth peripherals.
Results: Between 2018 – 2025, approximately 573 NP students have completed most of the telehealth modules (dependent upon when modules were introduced into their plan of study). There was an overall increase in knowledge pre- to post-lecture. Completion of the voluntary satisfaction surveys ranged from 34 to 327 participants, most reporting high satisfaction with the content, an overall increase in comfort, and intent to use telehealth post-graduation. A majority (82%) of students (n = 34) who participated in the virtual exam embedded into their OSCE appreciated the opportunity to practice patient-guided physical exam techniques in a low-risk environment and felt the module better prepared them for the experience. NP (n = 21) and prelicensure students (n = 42) who participated in the simulation using telehealth peripherals reported a greater appreciation in working with nursing students outside their program of study, increasing interdisciplinary patient-centered collaboration and team functioning. Prelicensure students expressed appreciation for improving their patient history skills by working with standardized patients in a primary care environment.
Discussion: Scaffolding telehealth components throughout the program of study within an NP program allows students to learn and retain telehealth knowledge that is invaluable within the primary care setting. Didactic education is enhanced further with the introduction of simulated synchronous telehealth visits, further reinforcing the use of telehealth soft skills and improving communication skills with patients and telepresenters. All students expressed the need for telehealth education and encouraged continued opportunities to translate didactic lessons learned into experiential activities to further enhance appreciation and understanding.
Using a Telehealth Hackathon as a Method to Teach Innovation
Background: Innovation is essential to develop new Methods: to improve patient care, prevent disease, and promote health, it remains a challenge to existing health care providers and systems. Progress in health care requires new technologies, procedures, and organizational change. Despite the increasing need for innovation in health care, there remains limited research on innovation and even less on how to prepare future health care providers to innovate. Hackathons have emerged as a structured method for active learning. These events have been shown to produce creativity, promote teamwork, and facilitate the generation of new ideas. This method should be used to apply innovation to solve complex problems and focus on solution design.
Methods: A one-day Hackathon for DNP practice and leadership students was conducted. Didactic content included: The Overview of Telehealth and Current Trends and the Nurse’s Role in Innovation. Students were placed in groups of 5-7 that had a mix of practice and leadership roles and were presented with a case study involving a rural hospital losing money due to the complexity of its patient population and recidivism following surgical discharges. Students were informed that a foundation was awarding them $300,000 for the first year to “solve” the problem. Each group went to a “telehealth room” staffed with a product representative from a national telehealth company. Students had 2-hours with the equipment and representative to “solve” the problem with the device. They were challenged to consider cost, staffing, ease of use, deployment, and return on investment. They were challenged to consider cost, required staff, ease of use, deployment, and return of investment. Telehealth equipment and representatives were from the following companies: 1) Amwell, 2) Teledoc, 3) Medwand, 4) Smartmeter, 5) Tytocare, and 6) TheTeleDentist. Following the 2-hour hack, students returned to pitch their plan to “Sharks” consisting of Chief Nursing Officers, a Hospital Innovation Officer, a Medical Telehealth Director, an Engineer, and a director of a national professional organization. The best pitch was selected by the sharks.
Results: The hackathon has been conducted twice over two years. Fifty-seven DNP students have participated in the Hackathons, along with six product representatives from national telehealth companies. A quantitative and qualitative survey evaluated participants perceptions/outcomes. The hackathons have been well received by both students and vendors. Most students rated their experience related to the innovative process, group/teamwork, and telehealth as excellent with one-third rating the experience of pitching their plan as excellent and 44.5% rating it as very good. Vendors also rated their experience as excellent (66.7%) or very good (33.3%). Qualitative responses consistently indicated a positive experience with growth in innovation, teamwork, collaboration, public speaking, telehealth knowledge, and clinical application to improve patient outcomes.
Discussion: A hackathon using telehealth as the modality for innovation is a fun and impactful teaching methodology. Embracing this format promotes experiential opportunities for developing critical skills related to innovation, design thinking, and problem solving. As a result of the hackathon the university has developed a relationship with one of the vendors to conduct FDA clearance testing, one vendor has since moved their product into one of the ‘sharks” organizations, and several students have taken part in other innovative tech projects. Educating faculty on the intricacies of this format will ensure successful replication and positive outcomes across institutions. This presentation will provide an overview of the Hackathon structure/and flow, share student and vendor outcomes, and highlight how to secure national vendors at no cost.
Innovative AI-Powered Kiosk: Boosting Off-Hours Care for Unhoused Patients with Symptom Assessment
Tina Gustin DNP, APRN, CNS, FAAN, Faryaneh Poursardar PhD
Old Dominion Univerrsity
Primary Email:tgustin@odu.edu
Background: Emergency rooms are often used by unhoused patients when clinics are closed, even for non-urgent symptoms, leading to high costs for hospitals and financial burdens on public programs like Medicaid. Many unhoused patients are uninsured, resulting in limited reimbursement. Old Dominion University’s Ellmer School of Nursing operates faculty-led, student-run free clinics within organizations serving the unhoused. These clinics save local health systems money but only operate three days a week, limiting patient access. Consequently, many patients turn to emergency departments, creating avoidable costs and overcrowding. To address this gap, ODU’s nursing and computer science teams are developing a symptom-assessment kiosk for use outside clinics during off-hours. The kiosk will guide users through care levels, including self-care, making an appointment, or visiting the ER, with plans to integrate real-time telehealth. This approach aims to reduce health care costs while ensuring patient health, safety, and autonomy.
Methods: The development of our symptom-assessment kiosk followed a comprehensive, interdisciplinary approach, prioritizing the needs of insecurely housed and unhoused individuals. We began by conducting focus group sessions to gather insights into their health care challenges and literacy levels. Doctor of Nursing Practice students curated content, ensuring it was both clinically accurate and easy to understand, while regular meetings with nursing and computer science faculty helped align technical and health care needs. The kiosk, designed with simplicity in mind, uses a multiple-choice framework to guide symptom selection, reducing confusion and enhancing accuracy. It employs a retrieval-augmented generation (RAG) approach, retrieving relevant medical information from a curated knowledge base, which is then processed by a generative AI model. This model assesses symptom severity and generates a clear guidance plan with practical steps, warning signs, and recommendations for care. The output avoids medical jargon, aiming for simple, accessible language. Operating autonomously during off-hours, the kiosk provides consistent guidance, promoting appropriate emergency service use and reducing unnecessary ER visits, thus enhancing health care access and outcomes.
Results: The initial use of the kiosk prototype demonstrated its ability to function impeccably, guiding users effortlessly from symptom selection to severity assessment and plan generation without human intervention. The kiosk successfully handled a range of symptoms, curated from both emergency and non-emergency scenarios found on hospital websites, to provide clear recommendations. By differentiating urgent from non-urgent situations, the kiosk effectively advised higher-risk users on the need for emergency services while guiding non-severe cases to wait until the clinic reopens. In these cases, it offered clear self-care advice and cautionary signs instead of suggesting unnecessary ER visits. The structured, multiple-choice interface minimized ambiguous input, ensuring consistent functionality. The output was concise, easy to comprehend, and free from medical jargon, emphasizing patient safety and vigilance. These observations suggest that the kiosk can offer meaningful guidance during off-hours. It holds significant potential to reduce unnecessary ER visits among unhoused patients, promoting efficient resource use and improved patient outcomes.
Discussion: This project highlights the impact of interprofessional collaboration and student involvement in developing health care solutions. The kiosk aids unhoused patients in making informed care decisions when clinics are closed, using simple symptom choices and AI guidance to determine when emergency room visits are necessary versus when it is safe to wait for clinic hours. While not designed to diagnose or replace medical staff, the kiosk identifies warning signs and offers clear, plain-language steps. This strategy can reduce unnecessary emergency visits, thereby lowering costs for hospitals and public health systems, while prioritizing patient safety. With further testing in clinical settings, this tool could effectively enhance care access for underserved communities during off-hours. Feedback has led to the inclusion of an avatar for emotional engagement. We are exploring additional funding and grant opportunities and increasing student participation. This project not only shows success in development but also offers valuable real-world experience at the intersection of AI, technology, and health care.
Americans’ opinions on interstate telehealth policy: a survey study
Natalie Anixter BS, Taliesin St. James BA, Mitchell Creinin MD
UC Davis Health
Primary Email:nranixter@health.ucdavis.edu
Background: Telehealth laws vary across the United States, but states and medical licensing boards commonly require physicians to be licensed in the state where the patient is physically located during the visit. This policy allows medical licensing boards, whose duty is to protect consumers of medical care from unqualified professionals, to uphold local standards of care. In a world of expanding telehealth options, patients’ views on physician location have not been explored. We aimed to assess Americans' opinions on physician location during a telehealth visit and the ability to receive care across state lines when needed.
Methods: We conducted a cross-sectional survey from October 16-17, 2025 using Survey Monkey Audience, a platform that allowed us to reach a demographically diverse, probability-based panel that reflects the broader U.S. adult population with a goal to obtain a minimum of 750 usable responses. We created a draft survey, used artificial intelligence to aid with editing to improve ease of comprehension for the general public, and then obtained and incorporated feedback from six volunteers ranging in age and education level who did not have health care Background: s. The survey collected demographic data and included four questions about telehealth policy and services. We included all surveys with at least one telehealth question response and used Fisher’s exact testing for all analyses.
Results: We received 770 eligible responses; each respondent did not answer every question. Most respondents (588/763, 77.1%) believed patients should be able to see a doctor in any state using telehealth and the official location of an interstate telehealth visit should be the patient’s state (571/768, 74.4%). The survey asked respondents to imagine they needed to see a doctor while visiting another state; 384/768 (50.0%) chose to see a new doctor in-person while 50% preferred a telehealth visit with their own doctor in their home state. Lastly, respondents were told they were diagnosed with a rare condition, and the nearest specialist was in a neighboring state but not licensed in their home state; 679/766 (88.6%) reported feeling comfortable attending follow-up visits by interstate telehealth. When stratifying responses by prior telehealth use, those who used telehealth before more commonly believed patients should be able to see a doctor in any state via telehealth (444/558 [80%] vs 133/190 [70%], p=0.009), believed the official location should be the patient’s state (424/557 [76%] vs 131/191 [69%], p=0.04), and felt comfortable with interstate telehealth follow-up visits (513/558 [92%] vs 149/191 [78%], p< 0.0001).
Discussion: These findings suggest that most Americans favor the ability to get telehealth care unrelated to the state their doctor is licensed, and most specifically indicate that laws restricting care to the state in which the patient is located limits their ability to seek their best or preferred provider. Most respondents believe the location of a telehealth visit should be the state of the patient. Although prior experience using telehealth was associated with stronger support for interstate access, both telehealth naive and experienced groups strongly favored these sentiments. Even among participants without telehealth experience, more than two-thirds believed patient location should dictate the site of the visit. Ultimately, interstate telehealth restrictions don’t align with patient needs and may require updating in the absence of evidence that physician qualification and expertise vary by licensure state to state.
Correlation of perinatal depression and social determinants of health among pregnant Medicaid recipients
Christine Chien MD1, Vijay Balakrishnan MBA2, Sina Haeri MD, MHSA2
1Carle Foundation Hospital and 2Ouma Health
Primary Email:chien.chr@gmail.com
Background: Suicide is a leading cause of preventable maternal deaths, accounting for up to 20% of deaths postpartum. Perinatal depression is on the rise in the United States, affecting 1 in 5 pregnant people. Untreated depression has profound and lasting harm on maternal and infant health, and recognition of early warning signs is crucial to intervening before a mental health crisis occurs. As pregnancy care transitions from the clinic to the digital platform, more investigation is needed on the efficacy of depression screening via telemedicine.
Methods: We conducted a retrospective cohort study of new patients referred by Managed Care Organizations (MCOs) between May 1, 2023, and July 10, 2025, across multiple states. The Edinburgh Postnatal Depression Scale (EPDS) was administered at each encounter, with scores ≥10 considered positive. Social determinants of health (SDOH) were screened using the standardized tool, PRAPARE, covering housing, food, utilities, access to medications, phone, baby supplies, childcare, and employment. Chi-square analysis compared depression rates by presence of needs; logistic regression assessed predictors.
Results: Among 2,337 patients, 31.3% had at least one SDOH need. Depression was significantly more common among those with needs (43.9% vs 21.5%, p< 0.01). Higher rates of depression were found within each SDOH category. In multivariable analysis, unmet needs for medications (OR 2.18, 95% CI 1.59–2.99, p< 0.01), baby supplies (OR 1.44, 95% CI 1.08–1.93, p=0.01), and employment (OR 2.22, 95% CI 1.44–3.44, p< 0.01) remained significant predictors.
Discussion: Perinatal depression and unmet SDOH needs were strongly interrelated in Medicaid patients from maternity deserts. Screening should be bidirectional: patients with depression should be evaluated for SDOH, and those with unmet needs should be screened for depression. Incorporating validated SDOH tools such as PRAPARE into careflows can reduce disparities and improve maternal outcomes.
Care team perspectives on telehealth-enabled rapid ART re-start: Mixed-Methods: findings from the ACCELERATE study
Rami Rifi MD1, Kristine Allen BS1, Hilal Abdessamad MD1, Thomas Deem MSN, FNP-BC, AAHIVS2, Blair Thedinger MD, AAHIVS3, Rachael Hernandez PhD1, Dima Dandachi MD, MPH1
1University of Missouri, 2Gilead Sciences, Inc., and 3KC CARE Health Center
Primary Email:r.rifi@health.missouri.edu
Background: Despite the availability of antiretroviral therapy (ART), HIV remains a major public health issue in the US. A significant proportion of people with HIV (PWH) do not receive ART due to a variety of reasons, including poor engagement in HIV medical care. Telehealth has the potential to improve access to real-time specialty care, especially for underserved and rural populations and may alleviate barriers including stigma and access issues. The ACCELERATE study aims to rapidly relink PWH who are out-of-care (OOC) in the state of Missouri by utilizing a Data-to-Care analysis to identify and reach OOC PWH, leveraging telehealth (TLH) to provide rapid access to an HIV provider within 24 hours of contact. Following this appointment, a 30-day starter pack of a single tablet pre-approved HIV ART regimen (bictegravir/emtricitabine/tenofovir alafenamide) is mailed to the patient. Understanding health care professional’s attitudes toward TLH is essential for evaluating the acceptability, feasibility, and sustainability of the ACCELERATE model for re-linkage to HIV care.
Methods: The ACCELERATE study is an implementation multisite study conducted in real-world clinical settings in 4 distinct health care systems distributed across the state of Missouri. We used a convergent parallel mixed-Methods: design to integrate quantitative survey data with qualitative interview findings, allowing for triangulation to strengthen our analysis. Site staff who are involved in administrative or clinical aspects of the intervention were recruited. A provider survey, using 5-point Likert-scale items, was administered at baseline and at Week 48 to evaluate attitudes toward the telehealth component of the study. Descriptive statistics (means, standard deviations, and frequencies) were generated to summarize provider characteristics and baseline perceptions. Paired-samples t-tests were used to assess changes in perceptions over time among providers with complete data at both timepoints. We conducted qualitative one-on-one semi-structured interviews with 11 schedulers, nurses, pharmacists, and providers. A total of 14 interviews were completed because 3 participants were interviewed twice, at which point thematic saturation was reached. Audio recordings were manually transcribed and two team members used MaxQDA to code transcripts and then refine codes and themes through an iterative analysis.
Results: Ten health care providers completed baseline surveys (60% male; 50% physicians, 30% fellows, and 20% advanced practice providers); 7 completed week-48 surveys. At baseline, more than 50% agreed/strongly agreed that TLH reduces patient costs, saves patient time, improves patient satisfaction, provides safe care, is more efficient than in-person visits, and overall benefits outweigh the negatives. Providers were generally neutral regarding perceptions of whether TLH reduces medical errors and improves patient–provider relationship. In the 48-week survey, providers’ perceptions of TLH improved and analysis showed a positive trend in perceptions, which reached statistical significance even with this small sample (n=7, p = 0.045). Interviews echoed this overall positivity, with codes related to TLH strengths applied more frequently and mentioned by more staff. Interviews highlighted convenience, flexibility, and improved accessibility. Providers described greater patient comfort and ability to “meet patients where they are at”. Qualitative data revealed some limitations among a minority of participants, including technical challenges, concerns about privacy, losing hands-on care, and reduced human connection.
Discussion: Providers showed favorable baseline perceptions of telehealth, particularly regarding efficiency and reduced patient burden to HIV care. Confidence in the overall value of telehealth increased further after one year of implementation of the ACCELERATE study. Qualitative findings reinforced this positive trajectory, with providers more frequently describing telehealth’s strengths than its limitations and emphasizing its convenience, flexibility, and ability to reduce access barriers. These findings indicate that telehealth is acceptable, feasible, and perceived as beneficial for re-linking PWH who are out of care, supporting its integration as a key component of rapid re-start HIV care models.
Telehealth re-engagement for people with HIV: Barriers, acceptability, and user experience in the ACCELERATE study
Rami Rifi MD1, Kristine Allen BS1, Hilal Abdessamad MD1, Thomas Deem MSN, FNP-BC, AAHIVS2, Blair Thedinger MD, AAHIVS3, Rachael Hernandez PhD1, Dima Dandachi MD, MPH1
1University of Missouri, 2Gilead Sciences, Inc., and 3KC CARE Health Center
Primary Email:r.rifi@health.missouri.edu
Background: Re-engaging people with HIV (PWH) who have fallen out of care (OOC) remains a critical challenge in efforts to reduce HIV morbidity, mortality, and transmission. PWH who are OOC often experience multiple and intersecting barriers including stigma, financial and transportation difficulties, as well as timely access to care. The ACCELERATE study was designed to address these barriers by using Data-to-Care analysis Methods: to identify OOC PWH in Missouri and offering a telehealth (TLH) visit with an HIV provider within 24 hours of contact. Following the TLH visit, participants are mailed a one month starter pack of a pre-approved single tablet antiretroviral regimen (bictegravir/emtricitabine/tenofovir alafenamide), enabling immediate HIV treatment initiation. To better understand readiness for this rapid-start model, we evaluated barriers to care and patient perceptions of TLH at the time of enrollment.
Methods: The ACCELERATE study is a multisite implementation study conducted across 4 distinct health care systems in the state of Missouri. PWH were considered OOC if they had not seen an HIV care provider for ≥6 months and had not received ART for ≥1 month, as determined through EMR review and participant self-report. Upon enrollment, PWH completed a baseline quantitative survey assessing demographics, barriers to care, telehealth usability, and visit satisfaction. They were then followed for 48 weeks. Descriptive analyses were conducted using means and frequencies to summarize demographic characteristics, access barriers, and telehealth perceptions. To complement quantitative data, we also conducted 6 qualitative interviews. Audio recordings were transcribed verbatim, and two analysts independently coded transcripts in MaxQDA, refining codes and themes through an iterative process. We conducted a focused analysis of content related to telehealth experiences. A convergent parallel mixed-Methods: framework integrated quantitative and qualitative data, supporting triangulation and reinforcing the analytical robustness.
Results: Overall, 65 participants were enrolled in the study (mean age 43 years [SD = 10.7], 21.5% female, 33.3% Black, 76.5% non-Hispanic). 51 completed the TLH visit and baseline survey; TLH visits took an average of 23.22 minutes, 33.3% switched from video to phone visits due to technical failures. The top 3 barriers for falling OOC were feeling depressed or overwhelmed (72.5%), lack of insurance (54.9%), and competing personal or family responsibilities (51.0%). All video users reported that the platform was easy to use. Among those who required instructions (30%), all indicated that the provider’s office gave the necessary guidance; 76.5% rated their visit satisfaction as high. In interviews, participants consistently viewed TLH as convenient and efficient, highlighting reductions in logistical burdens such as transportation and missed work. Interviews also revealed barriers not fully captured in surveys including: discomfort with virtual communication, privacy concerns, and occasional technical issues. Many felt comfortable communicating via telehealth and described strong patient–provider relationships. Others noted that certain situations (when physical exam or emotional support were needed) were better suited to in-person visits.
Discussion: TLH-based rapid re-engagement was overall highly acceptable to PWH who were OOC and addressed key logistical barriers such as transportation and scheduling constraints. While most participants reported positive telehealth experiences and strong satisfaction with TLH, qualitative findings highlighted important context-specific considerations, particularly privacy concerns, comfort with virtual communication, and the need for in-person evaluation in some clinical or emotional scenarios. These Results: demonstrate the feasibility of the ACCELERATE model to provide immediate medical services through TLH followed by rapid re-start of antiretroviral therapy, offering a promising strategy to facilitate timely re-engagement in HIV care for individuals who have been OOC. However, optimizing its implementation will require attention to technological support and patient preferences to ensure equitable and person-centered re-engagement in HIV care.
Evaluating an mHealth Messaging Intervention to Promote Diabetes Self-Management
Anna Nguyen PhD, RN1, Valerie Eschiti PhD, RN2, Zsolt Nagykaldi PhD1, Thanh Bui MD, DrPH1, Tam Nguyen PhD, RN2, Angelina Nguyen PhD, RN3, Katherine O’Neal PharmD, CDCES1, Hanxia Li MS1, Michael Machiorlatti PhD1, Kathleen Dwyer, PhD, RN1
1University of Oklahoma Health Campus, 2Boston College, and 3Baylor University
Primary Email:anna-nguyen@ou.edu
Background: Mobile health (mHealth) technologies present a transformative opportunity to deliver diabetes self-management education and support (DSMES) in ways that are scalable, cost-effective, and accessible beyond traditional clinical settings. Despite their promise, mHealth solutions remain underutilized among culturally diverse populations, leaving significant gaps in diabetes care. Vietnamese Americans, in particular, encounter persistent barriers such as language differences and cultural nuances that limit engagement with conventional DSMES programs. These challenges underscore the urgent need for innovative, culturally tailored interventions that leverage mHealth platforms to bridge access gaps and empower patients in their self-management journey. This pilot study aims to evaluate the feasibility, acceptability, and preliminary efficacy of a fully automated, culturally adapted mHealth messaging intervention designed to deliver DSMES to Vietnamese Americans with Type 2 diabetes (T2D).
Methods: An explanatory sequential mixed-Methods: design was employed, guided by the Practical, Robust Implementation and Sustainability Model (PRISM) framework. Feasibility and acceptability were measured by participation rate of eligible clinics and patients, patient message response rate, and retention rate. Focus groups were conducted to assess adoption and sustainability. A pilot single-arm, prospective interventional trial was conducted with a sample of 88 Vietnamese American adults with T2D from 10 primary care clinics. Surveys were administered at baseline and every 3 months over 12 months. Repeated measures ANOVA assessed changes in clinical outcomes at 3, 6, 9, and 12 months. Qualitative data from in-depth interviews and focus groups were thematically analyzed to validate and expand on quantitative findings. Integrated analysis using joint display enabled meta-inferences across data sources.
Results: Among 88 participants (mean age 68 years; range 35–86 years). The intervention did not significantly affect glycated hemoglobin A1c (HbA1c) (p=0.631) but demonstrated a statistically and clinically significant reduction in low-density lipoprotein (LDL) (p=0.001) and improvement in exercise performance (p=0.044). Qualitative data from 45 patient interviews reached data saturation, with 80% describing the intervention as “convenient” and “helpful.” Clinic staff (n=18) participated in three focus groups endorsed the intervention as acceptable and feasible. Mixed Methods: analysis confirmed high feasibility (83% clinic participation, 100% clinic retention) and acceptability (90.9% patient retention). Key barriers to sustainability included limited staffing and supply infrastructure at participating clinics.
Discussion: This mHealth-based DSMES intervention demonstrated feasibility and acceptability among Vietnamese Americans as patients in primary care settings. Although glycemic control improvements were modest, findings highlight the promise of culturally tailored mHealth messaging for diabetes self-management. Findings also highlight that clinic staff workload impacted feasibility, and clinic workflow significantly affected the sustainability of the intervention. Future research should refine intervention components to optimize long-term outcomes and evaluate scalability through larger clinical trials.
Evolution in behavioral health providers’ use of telehealth in Minnesota from 2020 to the present
Jonathan Neufeld PhD1, Megan Loew PhD2
1University of Minnesota and 2Minnesota Department of Health
Primary Email:jneufeld@umn.edu
Background: The use of various telehealth technologies has revolutionized health care over the course of the past 5 years. Nowhere is this more clear than in the field of behavioral health, where up to half of all encounters now take place online via video or phone, and many providers are even exploring service provision via text messages. How the use of these technologies grows and changes is of critical interest to the clinicians, researchers, administrators, and innovators in the behavioral health domain. What provider types are using telehealth? How much are they using it, and how has utilization changed over the past 5 years? Is it growing? Diminishing? Do providers working in some types of settings use it more than those working in other types of settings? Do provider characteristics like age, gender, geography, discipline, or specialty affect how often various technologies are used? How are workforce satisfaction and future career plans related to telehealth use?
Methods: We used the state of Minnesota’s health care workforce annual survey to explore various ways in which telehealth use by behavioral health clinicians has changed over the past five years, according to clinicians themselves. Findings from recent public reports and surveys will be included and summarized alongside our current, original research showing how self-reported utilization of telehealth has changed its distribution across various provider types and work settings over time. Additional analyses will contextualize behavioral health providers as a group within the Minnesota health care workforce and differentiate various practice settings regarding their use of telehealth technologies. Specific trends will be highlighted and discussed.
Results: Preliminary Results: suggest that telebehavioral health grew rapidly in 2020-21 up to a level of at least some utilization among almost all behavioral health clinicians. Since then, telehealth frequency has decreased, but those decreases have not been uniform across disciplines, age cohorts, and regions of the state. Tables and graphs summarizing these patterns of variation will be presented, with a particular focus on how the private practice community’s use of telehealth has developed over time.
Discussion: Telebehavioral health is arguably the most mature telehealth specialty. Patterns of development and dissemination within behavioral health may foreshadow coming developments in other specialties. Moreover, acute workforce shortages are present in the behavioral health domain and are likely to continue for the foreseeable future. Adaptations in the use of telebehavioral health by younger cohorts of professionals may show potential benefits in other specialty domains.
Reduced Hospitalizations During Nurse-Led Remote Monitoring for Heart Failure: A Quality Improvement Initiative
Carly Brown PharmD1, Neil Maneck MS2, Tanya Tucker BSN, RN2, Cynthia Broome BSN, RN2, Saurabh Chandra MD, PhD, MBA2, Donald Clark MD, MPH2
1University of Mississippi School of Pharmacy and 2University of Mississippi Medical Center
Primary Email:cbb5542@umc.edu
Background: Congestive heart failure (CHF) is a leading cause of hospitalization, readmission, and adverse patient outcomes. Remote patient monitoring (RPM) is a promising strategy to enhance early recognition of decompensation, improve engagement, and support guideline-directed medical therapy (GDMT). However, prior studies evaluating the use of RPM among patients with CHF have utilized varying protocols and yielded mixed results. Given the burden of CHF at the University of Mississippi Medical Center (UMMC), we evaluated the association between our RPM program and hospitalizations as a quality improvement (QI) initiative.
Methods: As part of this QI initiative, we conducted a retrospective chart review of patients active in the CHF RPM program between January 2023 and July 2025. Patients were referred at hospital discharge, during post-discharge transitional care management (TCM) phone calls, or during ambulatory visits. Patients received a home telemonitoring kit that included a blood pressure cuff and scale for daily reporting. The RPM platform was accessed via a mobile app or, when needed, a tablet with a data plan. Onboarding involved device training, disease education, and nurse-led medication reconciliation. GDMT and education were documented based on the 2022 AHA/ACC/HFSA CHF guidelines, and diuretic adjustments were coordinated with the treating cardiology team when weight changes were reported. Daily biometrics were reviewed in real time by nurses, and they conducted monthly outreach calls to discuss trends, GDMT adherence, and potential barriers. Of 103 enrollees, 83 completed onboarding and were included in the analysis. The primary outcome was hospital days per year (HDPY), an annualized measure of proportion of days in the hospital, comparing the 12 months prior to enrollment with the period during RPM participation.
Results: Among the 83 patients who completed onboarding, HDPY declined from 13.36 days in the 12 months prior to enrollment to 7.17 days after onboarding and during RPM participation, an absolute reduction of 6.19 days and relative reduction of 46.3% (p = 0.028). Referral sources included 43% from inpatient discharge, 36% from ambulatory visits, and 21% from post-discharge TCM encounters. Mean and median follow-up during RPM participation were 341 and 220 days, respectively.
Discussion: A CHF RPM program with real-time biometric review, nurse-led onboarding, and monthly outreach was associated with nearly 50% fewer hospital days per year. Key features included structured patient education, accessible technology, and continuous communication among RPM nurses, patients, and the cardiology team. These Results: highlight RPM as a practical, team-based strategy to enhance care delivery and reduce utilization in CHF at UMMC. To strengthen this QI initiative, future efforts will focus on improving enrollment, optimizing retention, and more fully integrating RPM into routine clinical workflows. Broader evaluation across other centers and application to additional chronic conditions may further define the clinical and financial impact of such programs.
Reducing COPD Hospitalizations and ED Visits Through Remote Monitoring: A Quality Improvement Project
Carly Brown PharmD1, Adam Isaac MD2, Neil Maneck MS2, Cynthia Broome BSN, RN2, Saurabh Chandra MD, PhD, MBA2, Andrew Wilhelm MD2
1University of Mississippi School of Pharmacy and 2University of Mississippi Medical Center
Primary Email:cbb5542@umc.edu
Background: Chronic obstructive pulmonary disease (COPD) is one of the costliest chronic conditions in the United States, with direct annual costs exceeding $50 billion. Much of this burden stems from hospitalizations and readmissions for COPD exacerbations, which represent the third leading cause of 30-day readmissions nationwide. Outcomes are disproportionately worse among rural and underserved populations, where COPD prevalence, hospitalizations, and mortality are significantly higher. Mississippi is particularly affected, ranking among the states with the highest COPD burden. At the University of Mississippi Medical Center (UMMC), we identified frequent COPD-related hospitalizations as a major quality gap. This quality improvement project was designed to evaluate whether integrating remote patient monitoring (RPM) with nurse follow-up and pharmacist-led medication optimization could reduce hospital and ED utilization while reinforcing preventive care for our patients with COPD.
Methods: A retrospective quality improvement project was conducted at UMMC using data collected through the electronic medical record (EMR). Thirty patients with COPD were enrolled in the RPM program between January 2023 and August 2025. Each patient accessed an app via their smartphone or received a tablet to record daily oxygen saturation and respond to symptom-based questions. Reported changes or worsening symptoms were automatically flagged, prompting nurse outreach to assess for exacerbations and, if indicated, escalate to the pharmacist to initiate the exacerbation protocol. Nurses also conducted monthly follow-up calls to reinforce self-management and monitor trends, while pharmacists performed medication reviews at baseline and every three months to align therapy with GOLD guidelines, review vaccinations, and address smoking history. Baseline demographics included MMRC score, GOLD classification, and COPD phenotype. The primary outcome was the difference in hospitalizations and ED visits for COPD exacerbations per year before RPM enrollment compared with during enrollment. Secondary outcomes included discharge reasons, frequency of exacerbation protocol initiation, and other adherence measures.
Results: Among the 30 patients enrolled, the RPM program was associated with a substantial reduction in acute care utilization. Hospitalizations and ED visits for COPD exacerbation declined from 2.2 per year prior to enrollment to 0.7 per year during RPM participation, a decline of 68% (p < 0.001). Secondary outcomes demonstrated strong engagement: 73% of monthly nurse reviews and 77% of pharmacist reviews were completed. Nurses made 63 intervention calls in response to abnormal biometrics or symptom reports, with 22 escalations to pharmacists leading to initiation of the exacerbation protocol. At enrollment, patients had an average MMRC score of 3.4, 97% had GOLD Class E COPD, and the most common phenotypes were chronic bronchitis and emphysema. Average enrollment duration was 6.2 months, with 41% of patients discharged due to noncompliance.
Discussion: Implementation of an RPM program for high-risk COPD patients at UMMC was associated with significant reductions in hospitalizations and ED visits, supported by strong patient engagement and coordinated nurse and pharmacist interventions. Key drivers included daily symptom and oxygen saturation monitoring, timely nurse outreach, and pharmacist-led medication optimization. These findings suggest that RPM can strengthen quality of care, improve patient outcomes, and support value-based care by reducing costs and enhancing efficiency. While promising, these Results: reflect a single-institution initiative and may not be generalizable to other settings. Future improvement cycles will focus on sustaining these gains, exploring opportunities to expand the RPM scope by including tele-pulmonary rehabilitation and additional telehealth support services, and investigating factors contributing to non-compliance, including digital disparities, workflow, or disease-related barriers.
Training Pharmacy Learners for Telehealth Practice: A Preceptor Model for Remote Patient Monitoring
Carly Brown PharmD, Meagan Brown PharmD, BCACP
University of Mississippi School of Pharmacy
Primary Email:cbb5542@umc.edu
Background: Pharmacists play an integral role in managing chronic conditions, and early exposure to team-based care models enhances learner readiness for collaborative practice. The expansion of telehealth and remote patient monitoring (RPM) in chronic disease management has created a need for pharmacy learners to develop competency in virtual care workflows. However, standardized training approaches for integrating learners into telehealth services are very limited. To address this gap, we developed a structured telehealth rotation and preceptor model to embed student pharmacists and residents into an established RPM program supporting hypertension and diabetes management at the University of Mississippi Medical Center. The purpose of this project was to provide learners an opportunity to enhance competency in telehealth communication, virtual clinical decision-making, and data-driven monitoring while supporting service capacity and continuity of care.
Methods: A telehealth experiential rotation was developed through partnerships with the Mississippi Department of Health’s American Society of Health-System Pharmacists (ASHP)-accredited postgraduate year one (PGY1) residency program and the University of Mississippi School of Pharmacy. Residents participated longitudinally, initially one day per week for 12 months and later two days per week for six months following program refinement. Advanced Pharmacy Practice Experience (APPE) students completed a one-month, 40 hour/week rotation. Learners received standardized training in virtual communication, documentation, biometric interpretation, and medication management protocols. Upon completion of orientation, learners reviewed biometric summaries, developed care plans, conducted telephone encounters, and completed documentation for preceptor co-signature. Interactions included initial medication reviews, diabetes reviews, and hypertension reviews, with call volume depending on patient enrollment. The preceptor provided supervision and feedback to support progressive autonomy for learners. Evaluation included ASHP learning-experience evaluations, APPE site evaluations, and preceptor assessments focused on clinical skills and communication.
Results: From 2021–2025, 12 residents and 22 APPE students completed the telehealth rotation, contributing over 8000 learner hours. The preceptor model effectively integrated learners into RPM workflows without disrupting operations or compromising patient safety. Most progressed from observation to independent patient interactions within two weeks. APPE evaluations (n=22) rated the rotation 5.0/5.0 for orientation, structure, and communication. Learners also reported strong skill development in interviewing (4.9), assessment and monitoring (4.95), and therapeutic planning (4.7–4.8). Residents rated all ASHP core elements “Consistently True,” citing continuity of care, rapport-building, clinical independence, and a supportive learning environment. Learners valued frequent patient interaction, interprofessional collaboration, and structured RPM workflows. Preceptor evaluations reflected progressive independence in biometric interpretation, treatment plan development, and documentation.
Discussion: This structured telehealth rotation and preceptor model successfully integrated pharmacy learners into an RPM program while maintaining safety and workflow efficiency. Learners advanced quickly to completing independent telehealth encounters and demonstrated strong gains in communication, assessment, and treatment plan development. High evaluation scores highlight the model’s effectiveness in preparing learners for virtual care. Implementation also revealed the importance of early training in motivational interviewing and strategies to navigate the absence of visual cues and varying home environments. Attention to these challenges can further strengthen learner readiness and optimize telehealth educational models. Future efforts will focus on broadening telehealth training opportunities, including increasing APPE rotation availability and integrating additional telehealth services beyond RPM to enhance workforce readiness.
Team-Based Telemonitoring for Hypertension and Diabetes in Academic Family Medicine
1University of Mississippi School of Pharmacy and 2University of Mississippi Medical Center
Primary Email:cbb5542@umc.edu
Background: Hypertension and diabetes mellitus are highly prevalent chronic conditions in primary care and require frequent monitoring to prevent complications. In Mississippi, where nearly all counties are medically underserved, workforce shortages further challenge chronic disease management. Remote patient monitoring (RPM) offers a strategy to support timely intervention, extend primary care capacity, and promote patient engagement. Academic family medicine clinics also serve as training environments where RPM can expose residents and pharmacy trainees to team-based, technology-enabled care. This study evaluated the effectiveness of an interprofessional RPM program for hypertension and diabetes and described its integration within resident and trainee education.
Methods: We conducted a retrospective cohort study of adult patients enrolled in RPM programs for hypertension or diabetes mellitus at the University of Mississippi Medical Center Family Medicine clinics between January 2020 and April 2024. RPM services were integrated into routine care and supported by an interdisciplinary team including clinical pharmacists, pharmacy residents and students, registered nurses, family medicine residents and attending physicians, and collaborating specialists. Patients who completed the program with available baseline and follow-up measures were included in the analysis. For hypertension, goals were individualized BP thresholds (< 130/80 mmHg or < 140/90 mmHg), and the diabetes program targeted mean pre-prandial glucose < 140 mg/dL. Primary outcomes were changes in systolic and diastolic BP for the hypertension cohort and hemoglobin A1c for the diabetes cohort. Paired t-tests assessed within-patient change.
Results: Of 237 patients enrolled, 94 completed the program and were included in the analysis. In the hypertension cohort (n = 70), mean systolic BP decreased from 139.8 mmHg to 128.4 mmHg (−11.4 mmHg, p = 0.0001) and mean diastolic BP from 81.5 mmHg to 76.7 mmHg (−4.8 mmHg, p = 0.0434). Among those with uncontrolled baseline BP (n = 43), systolic reduction was greater (−14.6 mmHg, p = 0.0004). In the diabetes cohort (n = 24), mean hemoglobin A1c decreased from 9.79% to 8.37% (−1.42%, p = 0.0192). Program documentation demonstrated consistent involvement of medical residents and pharmacy trainees in RPM review, medication reconciliation, and interprofessional decision-making, although educational outcomes were not assessed.
Discussion: A team-based RPM program embedded within academic family medicine care was associated with clinically meaningful improvements in BP and glycemic control among patients who completed the program. The integration of pharmacists, nurses, and medical residents supported comprehensive chronic disease management and created a practical interprofessional learning environment. Although not formally evaluated, the educational participation of residents and pharmacy trainees highlights the potential for RPM to serve as both a care delivery innovation and a platform for interprofessional and telehealth skill development in academic primary care.
Stressful life events and barriers to prenatal telehealth care: A PRAMS analysis
Cari Bogulski PhD,1 Hannah McCoy MPH,1 Mahip Acharya PhD,1 Rosario Silva MPH,1 Don Willis PhD2
1University of Arkansas for Medical Sciences and 2University of Arkansas, Fayetteville
Primary Email:cbogulski@uams.edu
Background: Adequate prenatal care is associated with positive postpartum and birth outcomes. However, barriers to prenatal care access persist. Additionally, stressful life events have been associated with both poor perinatal health outcomes and inadequate prenatal care, suggesting that patients who have experienced these stressful events may be in need of interventions to increase access to prenatal care. Telehealth is a feasible and acceptable tool to increase access to multiple types of health care services, including prenatal care, supplementing some in-person care visits to reduce such burdens as time and transportation on prenatal patients. However, telehealth services also have barriers to access, which need to be assessed and addressed if telehealth is to be used effectively. The associations between stressful life events and perceived barriers to prenatal telehealth care are currently not well understood, and identifying this relationships could inform future prenatal care interventions.
Methods: We utilized publicly-available data from Phase 8 of the Pregnancy Risk Assessment Monitoring System Automated Research Files, including core questionnaire items and the Maternal COVID-19 Experiences supplemental questionnaire, which was administered only in 2020 and 2021. We included only those respondents who: 1) completed the Maternal COVID-19 Experiences supplemental questionnaire, 2) provided valid responses to at least one of the fourteen stressful life events items, and 3) reported receiving only in-person prenatal care, as only those respondents were asked about barriers to prenatal telehealth care. Our outcome variables of interest were: lack of availability of virtual appointments from my provider, lack of a private or confidential space to use, preference for in-person care, and lack of technological resources (which collapsed the following four barriers: lack of telephone, cellular data/minutes, computer/device, or internet service). Only respondents with complete cases for outcome and independent variables were included. Four survey-weighted logistic regression models were fit to assess the association between stressful life events and four specific telehealth barrier outcomes.
Results: We found that, relative to non-Hispanic White respondents, Hispanic respondents were less likely to report a lack of available appointments (aOR = 0.76, 95% CI: [0.59, 0.98]), a lack of private or confidential space (aOR = 0.29, 95% CI: [0.12, 0.67]), and less likely to express a preference for in-person care (aOR = 0.67, 95% CI: [0.52, 0.86]). We also observed that non-Hispanic Black respondents were also less likely than non-Hispanic White respondents to report a lack of technological resources as a barrier to telehealth care (aOR = 0.50, 95% CI: [0.30, 0.84]), and less likely to prefer in-person care (aOR = 0.55, 95% CI: [0.41, 0.74]). Additionally, incarceration exposure (aOR = 1.93, 95% CI: [1.06, 3.51]) and job loss (aOR = 1.35, 95% CI: [1.02, 1.78]) were associated with increased reports of no available telehealth appointments, and both incarceration exposure (aOR = 4.12, 95% CI: [1.51, 11.28]) and difficulty paying bills (aOR = 3.83, 95% CI: [1.76, 8.33]) were associated with a greater likelihood of reporting a lack of private or confidential space for telehealth.
Discussion: In our study of PRAMS respondents in 2020-2021, we found that incarceration exposure, difficulty paying bills, and job loss were associated with an increased experience of barriers to prenatal telehealth care—specifically a lack of available prenatal telehealth appointments and a lack of a private or confidential space to use. Future research should investigate the causal mechanisms of these associations. Additionally, health care providers seeking to expand prenatal care access through telehealth should consider assessing the experience of stressful life events and pursue solutions to address these barriers for patients.
Virtual Doula Support After COVID-19: Strengths, Limitations, and Adaptations in a Changing Care Landscape
Lori Uscher-Pines PhD, MSc, Kortney James PhD, Molly Waymouth MPH
RAND
Primary Email:luscherp@rand.org
Background: Since the COVID-19 pandemic, doula care has shifted to incorporate virtual support. Despite ongoing delivery of virtual support and growing Medicaid coverage of both virtual and hybrid (virtual and in-person) support models, little is known about doulas’ post-pandemic experiences or how they have adapted their practices to virtual settings.
Methods: We conducted semi-structured interviews with 20 certified birth doulas across the United States between November and December 2025. Participants provided both in-person and virtual doula support. Interviews incorporated the FRAME implementation science framework to characterize practice modifications and included critical incident technique questions to elicit comparisons between virtual and in-person care. Transcripts were analyzed using inductive thematic analysis
Results: Participants identified numerous advantages of virtual doula support, including convenience, scheduling flexibility, reduced travel burden, accommodation of client preferences, and increased participation of geographically distant family members. Key disadvantages included challenges with rapport-building, lack of physical touch, reduced effectiveness during birth, and inability to provide hands-on postpartum assistance. While many doulas reported maintaining a similar approach across modalities, others described modifying, dropping, or creating practices to adapt to virtual support. Views on the comparability of virtual versus in-person support varied widely and appeared related to doulas’ conceptualization of their role. Most participants viewed virtual birth support as somewhat inferior to in-person support, though exceptions were noted.
Discussion: Virtual doula support offers meaningful advantages for access and flexibility but presents certain trade-offs. The lack of consensus across doulas regarding quality underscores the need for rigorous comparative effectiveness studies to inform policy and coverage decisions as virtual doula care continues to expand.
Bridging Practice and Education: Telemedicine Providers’ Perspectives on Telemedicine Needs
Steven Crellin DO, Rachel Dumont MS, OTR/L, Al Griffin BSN, RN, Tori Miller BS
Geisinger Health System
Primary Email:rdumont@geisinger.edu
Background: Research indicates that telemedicine education can enhance health care providers' knowledge and skills with telemedicine and contribute to improved patient outcomes. However, there is a need for evidence-based curricula. A recent international study identified core competencies in telemedicine education for health care professionals, including domains of environment and technology. To advance telemedicine education within a rural health care system, a survey was conducted among telemedicine providers to identify content areas for the domains of environment and technology.
Methods: A 23-question survey was distributed to health care providers utilizing a telemedicine video platform for supporting patients in a rural health system. The survey included multiple-choice and open-ended questions that aimed to assess how often challenges occur during telemedicine video encounters and sought specific details about those challenges to help improve telemedicine education. Survey Results: were categorized into education modules by a telemedicine provider/educator, a telemedicine educator, and an education and medical simulation center.
Results: Eighteen telemedicine providers from five medical specialties participated in the survey. 72% of respondents identified specific audio challenges, 22% detailed peripheral capability issues, 17% reported specific impact to lighting during video visits, 17% documented screensharing issues, and 11% detailed challenges during remote examinations. The themes emerging from the survey Results: were organized into three modules: technology basics and troubleshooting guidance for telemedicine providers, environmental preparations and peripheral setup for health care staff who are patient-side, and physical exam and peripheral guidance for health care staff who are patient-side.
Discussion: Ensuring provider expertise and insight into content area development for telemedicine education may contribute to the successful adoption and implementation of telemedicine practices in rural communities. Further exploration of the identified telemedicine education domains, with contributions from health care staff, can enhance the training curriculum and evidence-based practice in telemedicine. Additional focuses include longitudinal evaluation of this telemedicine education curriculum on providers' knowledge and skills in telemedicine and patient outcomes.
Differences in Primary Care and Mental Health State Leader Interpretation of Audio-Only Telemental Health Policies
1University of California, Los Angeles David Geffen School of Medicine, 2OCHIN, and 3Weill Cornell Medicine
Primary Email:cdermart@gmail.com
Background: Audio-only telehealth has been critical in expanding access to care, particularly for low-income families and rural communities who may lack access to broadband internet, devices capable of supporting video visits, and transportation. States enacted different telehealth policies and laws, including reimbursement for audio-only telemental health services, aiming to close care access. Prior research found variability in interpretation of policies by state leaders, but it unknown whether variation may be driven by specialty differences, such as focus on physical versus mental health conditions. This study aimed to compare perspectives on audio-only policies, specifically for telemental health services, between primary care and mental health leaders within the same state.
Methods: This study utilized legal mapping processes (“50 state survey”) to characterize the effective dates of state-level telehealth policies including Medicaid reimbursement of audio-only telemental health visits, from January 1, 2018 to December 30, 2023. States were rank-ordered based on the number of months with telemental health-friendly policies. Using a positive deviance approach, we identified states in the top- and bottom quartiles and recruited health leaders (e.g., mental health commissioners, primary care association leaders, Medicaid officials) in those states for interviews. We employed qualitative methods to gather insights on how state telemental health policy expansion influenced mental health services delivery, with a focus on improving safety-net care. Particular attention was given to audio-only policies and their implementation. Through thematic analyses of these interviews, we identified key differences in policy understanding between primary care and mental health state leaders related to audio-only allowances, reimbursement, and policy permanence.
Results: We found differences across primary care and mental health state leaders’ interpretations of audio-only regulatory policies for mental health services. We identified three main areas of differences in interpretation of audio-only policies – services allowed, reimbursement, and policy permanence. In one state, primary care leaders reported audio-only was broadly permitted for medical and behavioral services, whereas mental health leaders indicated audio-only was limited to psychotherapy. In another state, primary care leaders noted audio-only reimbursement ceased when federal flexibilities ended, while mental health leaders reported Medicaid maintained audio-only reimbursement despite federal changes. In a third state, mental health leaders stated audio-only was no longer allowed, contrasting with primary care leaders’ view that Medicaid permanently permits audio-only services in that state. Both primary care and mental health leaders highlighted that payment parity reduces provider incentive to use modifiers to report audio-only service delivery.
Discussion: This study revealed differences across primary care and mental health leaders’ interpretations of state-level audio-only telemental health policies, i.e., whether audio-only was broadly permitted or limited to certain services, the permanence of audio-only allowances post-public health emergency, and reimbursement/payment parity. Confusion may stem from difficulty tracking temporary policy changes, conflation of state and federal policies, uneven access to information, and differing relevance of audio-only policies based on specialty care. Leaders also noted that audio-only payment parity may have reduced incentives to code audio-only visits distinctly from video or in-person care. Future efforts should strengthen communication between policymakers, mental health leaders, and primary care partners to ensure consistent understanding and policy implementation and better support audio-only coding.
Telehealth Use and Perceived Quality of Health care among Cancer Patients: A National Cross-Sectional Survey Study
James Kimani1, Elijah Onsomu2, Dakysha Moore1, Ali Salman1, Yi-Hui Lee3
1North Carolina Agricultural and Technical State University, 2Winston-Salem State University, and 3Wright State University
Primary Email:jkkimani@ncat.edu
Background: Telehealth shows promise for improving access to health care, especially for people living in non-urban areas. Using different information and communication technologies, telehealth enables patients to access care provided remotely by health care professionals. However, while the potential of telehealth is widely recognized, research studies indicate mixed Results: on the impact and effectiveness of telehealth in chronic disease management. This inconsistency could be attributed to a range of factors that may influence the design, use and quality of telehealth programs. The objective of this study is to examine the association between telehealth use and perceived quality of health care among cancer patients. The study will also examine relationship between the use of telehealth and other patient-centered factors (e.g., technology infrastructure, digital literacy, trust in the health care system). The study findings will provide insights for policymakers and health care providers on how to improve the design and utilization of telehealth for medical consultations and services among cancer patients.
Methods: The study uses cross-sectional, nationally representative data from the Health Information National Trends Survey (HINTS) (fielded March-July 2024), adjusting for weights and strata to account for its complex design. HINTS collects data on the US public’s need for, access to, and use of health- and cancer-related knowledge, attitudes, and behaviors. Descriptive statistics describe the characteristics of the sample and multivariate multinomial logistic regression models assess the effect of telehealth use on the perceived quality of health care among cancer patients.
Results: The study sample included 5,919 non-institutionalized U.S. adults aged 18 years and older, of whom 17% reported having been diagnosed with cancer and 83% reported no history of cancer. A multivariate multinomial logistic regression analysis was conducted to examine the association between quality of health care and use of telehealth services. Overall, individuals who received care from a health care provider via telehealth were more likely to report their health care quality as very good (adjusted relative risk ratio [aRRR] = 1.69, p = 0.0001), good (aRRR = 1.66, p = 0.015), or fair/poor (aRRR = 1.73, p = 0.091) compared with those who did not use telehealth. Among participants who reported a cancer diagnosis, telehealth users were more likely to rate their health care quality as very good (aRRR = 2.23, p = 0.093), good (aRRR = 3.57, p = 0.022), or fair/poor (aRRR = 4.39, p = 0.022) relative to non-users. Similarly, among participants without a history of cancer, those who received telehealth care were more likely to report very good (aRRR = 1.69, p = 0.0001), good (aRRR = 1.63, p = 0.029), or fair/poor (aRRR = 1.78, p = 0.091) health care quality compared with those who did not use telehealth.
Discussion: This study sought to examine the relationship between telehealth use and perceived quality of health care among cancer patients. Access to health care through telehealth is influenced by a range of factors at individual and system level. The study findings highlight the need to examine closely issues such as reliable internet infrastructure and consideration of Social Determinants of Health and health equity in the formulation of policies that are aimed at expanding telehealth coverage and use among patients with cancer and other chronic conditions. This study also demonstrates the need to strengthen public trust in the health care system to enhance telehealth service quality. These findings suggest that adopting comprehensive strategies and policies is important to better support the adoption and utilization of telehealth for accessing health services among cancer patients.
Advancing FNP Curriculum Through Simulation-Driven Telehealth Innovations
1University Of North Carolina Wilmington and 2SP-ed
Primary Email:conder@uncw.edu
Background: Nurse practitioner students must be prepared for telehealth encounters as future providers. Although the National Organization for Nurse Practitioner Faculties (NONPF) supports integrating telehealth into APRN programs, no standardized protocol exists. NONPF outlines essential competencies such as etiquette, privacy and security, program development, practice integration, and documentation. It further emphasizes telehealth education as a means to expand care to underserved populations. Embedding simulation-based telehealth training with Standardized Patients (SPs) into nurse practitioner curricula equips students with practical experience, enabling them to master these competencies. This approach also supports Doctor of Nursing Practice (DNP) goals, including demonstrating leadership to improve quality and safety, and applying information and technology to transform care at both individual and population levels.
Methods: Two clinical faculty members earned telehealth certification and co-developed scenarios and scorecards with an SP educator to align objectives, scoring criteria, and feedback expectations. Course faculty were trained on assignment objectives to ensure students gained skills in telehealth etiquette, clinical decision-making, and state-specific laws, all while applying standards of best practice. Preparation included a telehealth education module in every course. Pre-clinical students received an hour of on-campus instruction on etiquette, while final-semester students accessed recorded content within their modules. Supplemental resources—videos, handouts, and webpages—were provided for review. Students participated in one-on-one SP virtual visits, practicing interviewing, etiquette, and decision-making in a safe environment. SPs offered immediate feedback on communication and professionalism, reinforcing essential skills. Each course concluded with a faculty-led debrief and short written reflection, allowing students to evaluate comfort, etiquette, and clinical judgment while refining differential diagnoses, decision-making, and care planning.
Results: During the first implementation of this initiative, faculty and pre-clinical students were surveyed before and after implementation to evaluate changes in comfort with telehealth. At baseline, 71% of students and 66% of faculty reported minimal or no prior telehealth experience. Following comprehensive educational modules, structured assignments, and simulation debriefings, 93% agreed the SP encounter was valuable and feedback-rich, and student comfort with telehealth components increased by approximately 36%. Content was updated to reflect current guidelines and implemented to a new cohort of pre-clinical students. Overall, the survey Results: indicate clear growth in students’ competency with telehealth training. An average of 27 students completed the pre-survey compared to 21 on the post-survey, providing a strong basis for comparison. Correct response rates on the pre-survey ranged widely—from 14.3% to 100%—while the post-survey showed a noticeable shift upward, with scores ranging from 30% to 100%. This improvement is reflected in the overall 13.6% increase in competency-based questions, suggesting that students not only engaged with the material but also strengthened their understanding in meaningful ways.
Discussion: Grounded in Jeffries’ framework and aligned with best practice standards, telehealth simulation has proven to be an effective pedagogical strategy for modernizing FNP education. Beyond improving comfort and knowledge, SP-based telehealth encounters generated actionable performance data (scorecard trends) that faculty can use to refine instruction and target high-impact gaps such as safety screening, empathy, and patient-directed remote exam maneuvers. Embedding telehealth into the curriculum prepares future nurse practitioners to deliver high-quality, patient-centered care across traditional and digital platforms, advancing accessibility and innovation. Additional data from the current semester is under analysis to further validate outcomes and guide ongoing refinement of telehealth integration.
Assessing the Impact of State Telehealth Policy Expansion on 988 Suicide & Crisis Calls Nationally
Jasmeen Santos MPH1, Tyler Cordero2, Susan Ettner PhD1, Lucia Chen MS1, Jose Escarce MD, PhD1, Lucinda Leung MD, PhD, MPH1
1University of California, Los Angeles David Geffen School of Medicine and 2Georgetown University School of Medicine Washington, District of Columbia
Primary Email:JJSantos@mednet.ucla.edu
Background: Suicide is one of the leading causes of death in the U.S., with rates rising over time. The 988 Suicide & Crisis Lifeline launched nationally in July 2022 to improve access to behavioral health crisis care. State telehealth policies—such as participation in the Psychology Interjurisdictional Compact (PSYPACT)—may influence 988 call routing by expanding the reach of licensed psychologists and behavioral health providers across state lines. Little is known about the downstream effects of telehealth policies on crisis service engagement. This study examined the adjusted association between PSYPACT adoption and 988 calls volumes within states.
Methods: We conducted a retrospective observational analysis using 988 call data from Vibrant Emotional Health from January 2022 through December 2024. The study sample included all 50 states and D.C., aggregated at the state-month level. The unit of observation was state-month and the outcome was the count of 988 calls routed. The key predictor was state participation in PSYPACT. We ran negative binomial regression models, including a state population size offset, fixed year effects, and state random effects. Models adjusted for state-level factors associated with clinical need and/or access to non-crisis behavioral health services obtained from public datasets (e.g., demographics, median income, broadband [=100/20 Mbps] availability, mental health professional shortage areas, unemployment rates, Medicaid and uninsured rates, rurality).
Results: Across all state-months (Nf1836), 988 call volumes varied widely, with a mean of 4,916 calls (SD= 5824.7), median of 3,171 (IQR=1280-6246.5), and range of 225-40,772 calls per month. Rapid adoption of PSYPACT within states occurred, rising from 67% in 2022 to 80% in 2024. PSYPACT adoption was significantly associated with higher 988 call routing rates (IRR = 1.12, 95% CI 1.03–1.23, p < 0.012), indicating ∼12% greater call volume in states participating in PSYPACT. There was a clear year effect (IRR= 1.25, 95% CI 1.12–1.39, p < 0.001) indicating significantly steadily rising 988 calls nationwide over time. No other state-level factor, including rurality, was associated with 988 call volume.
Discussion: PSYPACT participation was independently associated with increased 988 call routing, suggesting that policies expanding telemental health provider reach may strengthen crisis service engagement. Future research can incorporate direct measures of underlying need to ensure findings are sufficiently robust to ongoing policy Discussion:s on sustaining pandemic-era telehealth flexibilities.
Remote patient monitoring for type 2 diabetes in pregnancy: device usability and maternal-neonatal outcomes
Crystal Jones MHD, RDCS, Cheng Peng PhD, MPA, MS, Rebecca Jones MPH, Karina Leal BSN, RNC-MNN, Amalie Gunn BS, Nafisa Dajani MD, Hari Eswaran PhD
University of Arkansas for Medical Sciences
Primary Email:cdjones@uams.edu
Background: Type 2 Diabetes Mellitus (T2DM) during pregnancy is associated with adverse maternal and neonatal health outcomes. Pregnant women with T2DM record glucose readings 4-6 times daily using a paper log. This study assessed the feasibility of using a Remote Patient Monitoring (RPM) iGlucose glucometer to manage T2DM during pregnancy among a cohort of Medicaid women and compared clinical outcomes among RPM users and women using a standard glucometer with paper log.
Methods: Thirty-three pregnant women utilizing Medicaid with T2DM were provided an RPM iGlucose device. Participants completed a pre-post survey and semi-structured interview. To assess clinical outcomes, we created a Connected Device Use Group of participants who used the iGlucose device or a continuous glucose monitoring device (CGM), and Standard Paper Log group of individuals who used a standard glucometer.
Results: A significant decrease between pre-post scores was seen for Appraisal of Diabetes (p=0.0046) and Perceived Stress (p=0.0296). Treatment Self-Efficacy (p=0.0030) and General Self-Efficacy (p=0.0129) significantly increased with iGlucose device use. Overall, perceptions of the iGlucose device were positive with advantages including automatic upload of glucose readings, ease of use, increased self-efficacy, perceived better care, and decreased stress and anxiety. No significant difference in clinical outcomes was seen.
Discussion: By automatically uploading glucose readings through a remote patient monitoring glucometer, remote patient monitoring significantly lightens the burden for people with chronic conditions like diabetes. Integrating this technology provides a comprehensive view of glycemic control throughout pregnancy, enabling clinicians to identify glucose patters early and shift from reactive management to proactive, data-driven decision-making.
Telehealth Experiences and Preferences Among Patients with Cardiovascular Disease Risk Factors
Allison Tep MPH, Olivia Jones MPH, Sruthi Cherkur MPH, Meg Yuan MPH, Cristin Mathew MPA
American Heart Association
Primary Email:Allison.Tep@heart.org
Background: The American Heart Association Center for Telehealth aims to address gaps in the telehealth landscape by guiding telehealth integration into outpatient settings for cardiovascular disease risk factor management. The use of telehealth in the management of cardiovascular conditions has the potential to increase the type and quality of care that patients can access. The Heart Association’s Patient Solutions and Support Team supports this mission by developing patient resources that reflect patient experiences with telehealth. The Heart Association’s Evaluation Team conducted a cross-sectional survey at health systems participating in the Center for Telehealth’s Learning Collaborative. The survey goal was to understand patients’ experience, knowledge, and attitudes about telehealth, to inform the development of patient resources that aim to prepare patients for telehealth visits and to inspire informed decision-making between patients and health care professionals (HCPs).
Methods: Twelve participating health systems, located across 9 states, invited their patients to complete a 30-question survey hosted online in the Qualtrics system. The survey was available in English and Spanish, and participants who completed the survey were provided a $20 gift card. Participants were eligible to complete the survey if they were the age of majority in their state and had been previously diagnosed with hypertension, hyperlipidemia, and/or diabetes. For the analysis, descriptive statistics of all survey question responses were calculated in Excel. Data was further stratified by 7 demographic variables to assess differences in descriptive statistics by demographic characteristics. The Pearson Chi-Square and Fischer’s Exact Test were performed to determine statistical significance of the stratified data. Lastly, the 8-item eHealth Literacy Scale was used to measure participants’ eHealth literacy. A score of 1 to 25 denoted low eHealth literacy, and a score of 26 to 40 denoted high eHealth literacy.
Results: A total of 571 responses were collected and analyzed. Most participants were female (68.9%) and represented various races including Black/African American (32.9%), White (26.3%) and Hispanic/Latino (20.1%) (n=547). Most participants were below 65 years old (81.9%, n=571). Of those who indicated they had health insurance (n=465), almost half (43.9%) had Medicare or Medicaid. Participants’ top three facilitators to easier telehealth access were lower telehealth costs/copays than in-person visits, having HCPs directly call in prescriptions after visits, and access to reliable internet connection. Black/African American participants were statistically significantly more likely to report that accessible video features and using more images/handouts during visits would make telehealth easier to access than non-Black/African American participants (p< 0.05). Hispanic/Latino participants were statistically significantly more likely to report that access to a private space to have telehealth in and access to language interpreter services would make telehealth easier to access than non-Hispanic/Latino participants (p< 0.05). Most participants were confident they could use telehealth to help manage their condition in the future (61.1%, n=553).
Discussion: The survey Results: informed the development of four patient resources: 1) “How to Get Ready for a Telehealth Appointment” flyer, 2) “Get Ready with Me for a Virtual Doctor’s Visit” video, 3) “What to Expect During Your Telehealth Visit” flyer, and 4) “Common Concerns & Facts on Telehealth” flyer. These resources are available on the Heart Association website. A follow-up survey will be conducted from January to February 2026 to understand the effectiveness of the resources in preparing participants for future telehealth appointments, as well as their perceived utility of the developed resources.
Mobile Broadband Access as a Foundation for Telehealth Engagement in an FQHC Feasibility Study
Chrissy Kuahine MPH
Waianae Comprehensive Health Center
Primary Email:mkuahine@wcchc.com
Background: Telehealth has expanded rapidly across health care settings, yet access to reliable broadband, connected devices, and digital readiness remains uneven, particularly in underserved and rural communities. Within a Federally Qualified Health Center (FQHC) setting, these gaps are often driven by affordability related mobile broadband access barriers, including inability to maintain cellular data plans or access camera enabled devices, which restrict participation in video-based care and result in reliance on audio only visits. While telehealth research frequently focuses on platforms, workflows, or digital literacy interventions, fewer studies examine whether removing mobile broadband access barriers alone can support telehealth engagement. This study examines the feasibility of addressing mobile broadband access as a foundational step toward improving participation in connected care within a safety net clinical setting.
Methods: This feasibility study employed a single arm design to evaluate implementation, engagement, and participant reported telehealth use over a 6-month period. Up to 10 adult patients receiving care at an FQHC and experiencing identified mobile broadband access barriers were enrolled. Clinical operations staff were limited to identifying eligible patients during routine care and submitting a simple referral to the Principal Investigator, with no additional clinical tasks required. All study explanation, consent, participant engagement, and follow up were conducted by the Principal Investigator outside of routine clinical workflows. Participants received a study issued mobile device with an unlimited data plan and brief orientation focused on device use and telehealth navigation. No clinical care was delivered as part of the intervention. Data collection relied exclusively on participant reported measures, including baseline and post participation surveys assessing digital literacy, health literacy, and telehealth readiness. Monthly structured check ins documented participant contact and self-reported telehealth use with providers or care teams. Analysis focused on descriptive feasibility indicators, including enrollment, retention, engagement frequency, and survey completion.
Results: The feasibility approach proved workable within routine clinical operations. Participants were successfully recruited and retained over the 6-month study period, with most completing scheduled monthly check ins. Participants primarily represented underserved populations receiving care at an FQHC, with most identifying as Native Hawaiian and experiencing socioeconomic barriers to maintaining reliable mobile broadband access. All participants met affordability related criteria that would have qualified them for subsidized connectivity programs during the study period. Participants reported increased confidence using mobile devices for health care related activities and greater readiness to engage in telehealth. Participant reported telehealth use with providers occurred during the study period, with several participants reporting multiple completed encounters. Survey completion rates met predefined feasibility targets. Implementation insights highlighted the importance of flexible engagement strategies, ongoing technical support, and a referral-based workflow that minimized impact on clinical operations while separating mobile broadband access support from clinical care delivery.
Discussion: This feasibility study demonstrates that addressing mobile broadband access barriers is both practical and acceptable within an FQHC setting. By treating connectivity as a prerequisite rather than an add on to telehealth, participants were better positioned to engage in connected care without increasing clinical workload. The referral-based design, which required minimal involvement from clinical operations staff, further supports the feasibility of this model in safety net settings where clinical teams are already overextended. These findings provide early, real world evidence that mobile broadband access interventions can serve as a critical foundation for broader telehealth strategies in underserved communities. Results: will inform refinement of study protocols and support future research examining how improvements in mobile broadband access influence telehealth utilization and patient engagement in safety net health care settings.
A Telehealth-Enhanced Integrated Rural Care Model Enabling Safe Buprenorphine-Benzodiazepine Co-Prescribing
Amir Batrice BS,1 Mohammad Al-sheikh BS,1 Milcah Poothakary BA,1 Edwin Paul MPH,1 Roger Mason, MD,2 Ariel Santos MD, MPH, FACS, FCCM1
1Texas Tech University Health Science Center School of Medicine and 2Healing Hands Addiction Centers
Primary Email:amir.batrice@ttuhsc.edu
Background: Opioid Use Disorder (OUD) treatment retention suffers from numerous barriers, including fragmented care delivery, limited psychiatric integration, specialist shortages, and inadequate management of psychiatric comorbidities. These barriers to retention have become increasingly consequential, as mortality risk after discontinuing OUD treatment skyrocketed compared to the pre-fentanyl era. While evidence supports combining various behavioral interventions, interdisciplinary care, and pharmacological therapies, one particularly misunderstood treatment is co-prescribing buprenorphine (BUP) with benzodiazepines (BZD) for anxiety stabilization. The mortality risk of treatment dropout due to inadequate psychiatric care exceeds the perceived pharmacologic risks of supervised co-prescribing, yet clinicians lack structured models to implement holistic treatment. This study describes how a vertically integrated care model in rural Arkansas uses telehealth-enhanced interdisciplinary coordination to deliver comprehensive OUD treatment, including BUP-BZD co-prescription.
Methods: We conducted a literature review examining buprenorphine-benzodiazepine co-prescribing in patients with opioid use disorder, identifying inconsistencies in previous literature and highlighting more recent studies and federal guidelines that challenge historical restrictive practices. We searched PubMed, Google Scholar, and Cochrane Library for peer-reviewed articles, clinical practice guidelines, and observational studies examining concurrent BUP-BZD use in OUD treatment populations. We examined confounding factors (psychiatric illness severity, polysubstance misuse, lack of clinical oversight) that may explain these inconsistencies. Additionally, we provide a detailed program description of a vertically integrated medication-assisted treatment clinical model in rural Arkansas, discussing team composition, care coordination mechanisms, telehealth modalities (synchronous psychiatric monitoring, asynchronous peer support), behavioral health integration strategies, and transitions across levels of care.
Results: Previous literature associates co-prescription with an increased mortality risk, which are confounded by psychiatric illness severity, polysubstance misuse, and lack of clinical oversight. Studies in supervised clinical settings with structured monitoring reported different safety profiles. Current literature emphasizes that comprehensive care for OUD benefits from behavioral interventions and interdisciplinary coordination alongside pharmacological therapies, yet implementation of a holistic approach, especially in rural areas, remains a challenge. This model addresses this challenge through vertical integration across the treatment continuum. Key structural elements include 24/7 peer support specialists in emergency departments to facilitate warm handoffs, telehealth-enabled psychiatric monitoring, behavioral health counselors providing anxiety-focused therapy combining cognitive behavioral therapy and Mindfulness-Oriented Recovery Enhancement intervention delivered both in-person and via telehealth, and interdisciplinary team communication through shared electronic health records allowing real-time coordination between psychiatrists, therapists, and peer support specialists to prevent siloed care.
Discussion: Increasing treatment retention for OUD treatment requires coordinated delivery of behavioral interventions, interdisciplinary care coordination, and pharmacological therapies. This holistic model demonstrates how connected health infrastructure can address barriers: vertical integration eliminates fragmented care; shared EHRs allows for better interdisciplinary treatment; telehealth-enabled monitoring extends specialist coverage where workforce shortages exist; and telehealth empowered behavioral health counselors allow for continuous management of patients with psychiatric comorbidities. Within this model, BUP-BZD co-prescribing represents how holistic care models can safely implement evidence-based treatments that fragmented systems struggle to deliver. Structural components and telehealth workflows implemented in this model can also be adapted in similar settings. Future research should establish validated telehealth-based sedation monitoring protocols and evaluate retention outcomes comparing telehealth integrated vs fragmented care models.
Measuring Telehealth Integration for Chronic Cardiac Disease Management: Pilot Metric Development & Testing
Sruthi Cherkur MPH, Cayla Hadley BS, Gary Myers MS
American Heart Association
Primary Email:Sruthi.Cherkur@heart.org
Background: Following accelerated growth in response to COVID-19, telehealth is increasingly utilized to care for diseases not traditionally managed virtually. This rapid expansion, while increasing access to care, has resulted in significant variation in care delivery in part due to lack of clinical guidance on appropriate integration of telehealth. This demonstrates a need for better measurement and evaluation of telehealth models of care to better understand impact on patients’ diseases management and ensure consistent delivery of high-quality telehealth care. The American Heart Association aims to address this through an initiative to pilot quality metrics across a diverse cohort of 12 participating health systems across the United States, serving urban, suburban, and rural populations, and spanning various care settings from large multi-site and academic health centers to small and freestanding community health centers. A variety of virtual care models are utilized at these sites from text and phone call management to hybrid telehealth and video consults and remote patient monitoring.
Methods: Pilot metrics were developed based on the Four Domain Model of Virtual Care and Value framework, spanning Equity, Economic, Experiential, and Functional domains, as this framework is critical for measuring quality and standardization (Demaerschalk et al, 2022). Additionally, existing measures such as HEDIS and CMS MIPS measures were leveraged in metric design to enhance feasibility of data capture. The cohort provided feedback on proposed metrics based on data gathering capabilities and applicability before metrics were finalized and data reporting began in Q1 2025. The following four metrics were required of participating sites: % of completed telehealth visits, % of patients provided with preparation to access telehealth appointments, % of telehealth satisfaction questionnaires completed, and % of patients reporting satisfaction with telehealth visits. Additionally, sites choose two clinical quality-focused metrics out of five options: blood pressure (systolic/diastolic), HbA1c %, LDL-C levels, statin adherence, and beta blocker adherence. These metric pairs compared in-person only data to those that had at least one hybrid/telehealth visit over a given quarter.
Results: Across three quarters from Q1-Q3 2025, completed telehealth visits averaged 73% and remained stable from Q1 (72%) to Q3 (73%). Patient-reported satisfaction was consistently high (>83%), though satisfaction questionnaire completion declined from 46% in Q1 to 41% in Q3. Clinical quality-focused metrics showed modest improvement for telehealth users: blood pressure control increased from 72% to 73%, and blood glucose control from 66% to 68%, very slightly outperforming in-person visits, but not significantly so. Medication adherence for statins and beta blockers remained >90% throughout. Community Health Centers reported the highest telehealth volumes, but had lower completed telehealth visits and completed satisfaction surveys compared to primary care clinics.
Discussion: Clinical quality metrics for in-person and hybrid/telehealth visits were largely comparable, and in some cases slightly higher for telehealth, indicating that virtual care supports consistent disease management. This suggests telehealth can extend high-quality care to patients unable to attend in-person visits, improving access for management of chronic cardiac conditions. Telehealth visit completion remained stable, and satisfaction rates were high, reflecting strong patient acceptance. However, data collection posed challenges due to varied EHR systems and infrastructure gaps, and satisfaction survey volumes were lowest given process and engagement barriers. These pilot metrics enable sites to evaluate telehealth-integrated care models, drive continuous improvement, and support sustainability. Several sites reported gaining new insights into telehealth populations, creating opportunities to refine virtual care strategies and enhance patient support.
Population Health and Social Needs Associated with Medicare Telehealth Use: An Elastic Net Approach
Zhaoqiang Zhou, Sara Al-Ajlouny, Saif Khairat PhD, MPH, FACMI
University of North Carolina at Chapel Hill
Primary Email:zhzhou@unc.edu
Background: Telehealth expanded rapidly for Medicare beneficiaries during the COVID-19 era and remains widely used, yet substantial state-level variation persists. This heterogeneity raises questions about whether telehealth utilization is aligning with underlying population health burden and health-related social needs, which may influence both demand for and access to virtual care. U.S. Centers for Disease Control Prevention (CDC) Population Level Analysis and Community Estimates (PLACES) provides standardized, nationwide indicators spanning chronic disease outcomes, preventive service use, risk behaviors, disability, health status, and social needs, enabling comparable state-level profiling of health and social vulnerability. Linking Centers for Medicare & Medicaid Services (CMS) Medicare Telehealth Trends with PLACES offers an opportunity to assess how state-level telehealth use corresponds to these population health characteristics using publicly available data.
Methods: We performed a cross-sectional analysis at the state level using publicly available CMS Medicare Telehealth Trends data and CDC PLACES indicators. Telehealth use was operationalized as an annual state-level utilization ratio, defined as the number of unique Medicare Part B beneficiaries with ≥1 telehealth service divided by the number of unique beneficiaries with ≥1 telehealth-eligible service. Quarterly observations within 2023 were aggregated to annual estimates using denominator-weighted aggregation. PLACES measures were drawn from the 2025 release (BRFSS 2023 based estimates) and included domains spanning health outcomes, preventive service use, health risk behaviors, disability, health status, and health-related social needs. All predictors were standardized prior to modeling. We evaluated associations using Elastic Net regression with cross-validated hyperparameter tuning to identify a parsimonious set of correlates and reported non-zero coefficients as selected features. Model stability and fit were assessed using coefficient-path diagnostics and observed-versus-predicted plots.
Results: Health condition data from 3,143 counties was aggregated to 50 states and the DC. Higher telehealth use was most strongly linked to asthma (β=0.956) and psychosocial burden (lack of social/emotional support β=0.754; social isolation β=0.742; depression β=0.510; short sleep β=0.406; frequent physical β=0.289; mental distress β=0.252), with smaller positive associations for high cholesterol (β=0.274) and vision disability (β=0.230). Lower telehealth use was associated with binge drinking (β=−0.161), certain disabilities (hearing β=−1.177; self-care β=−0.280; cognitive β=−0.165), and several chronic conditions (coronary heart disease β=−0.335; diabetes β=−0.464; COPD β=−0.617; stroke β=−0.636; high blood pressure β=−0.743; cancer/melanoma β=−1.018; arthritis β=−1.163). Overall, telehealth use is aligned more with respiratory and psychosocial vulnerability than with cardiometabolic disease and disability burden. Diagnostics suggested stable selection and good fit, with coefficients remaining non-zero across α and observed vs predicted values closely aligning with the line of equality with no prominent outliers.
Discussion: Stronger associations were observed for respiratory and psychosocial measures, suggesting telehealth may be particularly well positioned to support access for conditions and needs that benefit from frequent, low-barrier contact. At the same time, several chronic disease and disability measures showed different patterns of association, underscoring that telehealth uptake likely reflects heterogeneous clinical needs and care pathways across conditions. Overall, these findings illuminate where telehealth is likely to be most effective and provide actionable insight to support more targeted and need-responsive telehealth planning.
Use and perceptions regarding a telementoring program for physicians in rural settings: a mixed-methods study
Stefan Escobar-Agreda MD1, Kelly De la Cruz-Torralva BSc2, Nicole Villagaray-Paheco MD2, Leonardo Rojas-Mezarina MD2, Saif Khairat PhD, MPH, FACMI1
1University of North Carolina at Chapel Hill, Chapel Hill and 2Unidad de Telesalud, Universidad Nacional Mayor de San Marcos
Primary Email:escobara@unc.edu
Background: In low- and middle-income countries (LMICs), mandatory rural service programs often deploy newly graduated physicians to remote areas. While this strategy expands service coverage, it is commonly implemented in settings with limited specialist availability, variable connectivity, and a high clinical and administrative workload. In this context, remote mentoring can provide support that facilitates physicians’ work. In Peru, a specialist-led Telementoring Program was implemented and subsequently optimized after limitations identified during initial deployment. We evaluated this program between 2019 and 2024, focusing on its characteristics, user perceptions, and recommendations to strengthen implementation.
Methods: We conducted a mixed-methods study using three data sources: (1) a survey of physicians participating in the program to describe their characteristics and consultation patterns; (2) a descriptive analysis of program consultation records to characterize response time, communication channel, consultation status, and consultation area and specialty; and (3) a qualitative analysis of interviews with rural service physicians (SERUMS) conducted in 2019, 2021, and 2024, identifying themes related to facilitators, barriers, and improvement proposals. Findings were integrated through triangulation, contrasting quantitative patterns of use and performance with participants’ perceptions and recommendations.
Results: Among surveyed physicians (n=352), mean age was 27.9 ± 3.3 years and 50.6% were women. Most worked in Ministry of Health facilities (71.6%), and 44.9% reported having used the telementoring program. Prior to the program, 58.0% reported never seeking clinical/technical consultation, 36.3% consulted 1–3 times per month, and 5.7% consulted at least once per week. Among consultations (n=662), WhatsApp was the predominant response channel (84.2%), followed by WhatsApp plus phone call (8.5%) and an academic forum (6.0%). Median response time was 0.7 hours, and 98.7% of consultations were completed. Most consultations were clinical (60.5%), followed by administrative (21.2%) and medico-legal (18.2%) topics. Qualitative findings indicated that the program was perceived as accessible and easy to use and as supportive for clinical and administrative decision-making, contributing to reduced stress. Reported barriers included insufficient training, limited dissemination, unstable connectivity, and occasional delays, as well as perceptions of “passive” management and lack of feedback on case status.
Discussion: The telementoring program was primarily used through instant messaging and was valued as clinical, administrative, and emotional support. To increase its impact and uptake, participants recommended operational and training improvements, including stronger dissemination and onboarding, triage criteria based on urgency and expanded specialist availability, visible case-status feedback, and proactive training strategies. Finally, participants highlighted the need for training in digital tools and AI (prompting skills and source verification) to support safe and appropriate use.
Student-Led Implementation of a Virtual Self-Inquiry and Peer Leadership Model: The H2H Connected Health Framework
1Heart-2-Heart, Rock Bridge High School, 2Vandalia Health-CAMC, 3Bolles High School, 4Sathyabama Dental College & Hospital, and 5Omandurar Medical College
Primary Email:trevor.lovell@vandaliahealth.org
Background: Rising levels of stress, burnout, and loss of confidence among adolescents and young adults represent a growing global public health challenge, particularly within academic and professional training environments. Access to traditional mental health services remains limited by stigma, workforce constraints, and scalability barriers. H2H (Heart-to-Heart) is a student-founded, self-inquiry-based resilience and leadership framework designed to support youth mental wellbeing through awareness-building, peer connection, creative self-authorship, and purpose development. Unlike clinical or therapeutic models, H2H emphasizes non-pathologizing language, peer leadership, and empowerment. This abstract describes the evolving implementation of H2H as a connected health model, with recent expansion into international academic settings and student-led delivery.
Methods: H2H was implemented as an 8-week virtual program for adolescents and young adults (ages 13-30) across academic and community contexts. Participants enrolled digitally and completed baseline self-reported measures assessing perceived stress, confidence, resilience, and sense of purpose. The intervention consisted of brief weekly digital modules, guided self-inquiry prompts, reflective micro-practices, and optional group discussions. Delivery evolved from mentor-supported facilitation to a peer-led model, with trained H2H student ambassadors facilitating sessions independently. Implementation feasibility was evaluated through enrollment, completion rates, and participant feedback. Program adoption was further assessed through formal inclusion in international academic conferences and institutional partnerships, including a newly formalized student wellness collaboration in Malaysia. Descriptive analyses were used to assess changes in wellbeing indicators and implementation acceptability.
Results: H2H demonstrated high feasibility and sustained engagement across multiple cohorts. Participants reported reductions in perceived stress and improvements in confidence, self-awareness, and clarity of purpose. Qualitative reflections emphasized increased emotional regulation, self-belief, and readiness to support peers. Importantly, implementation maturity advanced beyond pilot delivery. H2H was formally evaluated and adopted as a resilience and leadership training model at an international medical education conference. For a January 2026 academic conference, five trained H2H student ambassadors independently delivered formal peer-to-peer training sessions without faculty facilitation, indicating successful leadership transfer and capacity building. Additionally, an international student wellness collaboration in Malaysia was formalized, supporting cross-cultural scalability of the model.
Discussion: H2H demonstrates the feasibility of a scalable, student-led connected health framework for youth resilience and leadership development. The transition from facilitated delivery to independent peer-led implementation, coupled with international adoption in academic settings, suggests that H2H functions not only as a wellbeing intervention but as a capacity-building leadership model. These findings support further evaluation of student-led, non-clinical connected health approaches as complements to traditional mental health services across global educational environments.
Efficiency and Care Patterns in an Academic Telepsychiatry Service Using Synchronous and Asynchronous Modalities
Nathaniel Sowa MD, PhD, Marcelo Garibaldi BSPH, Jennifer Morelli MPS, RN, Saif Khairat PhD, MPH, FACMI
University of North Carolina at Chapel Hill
Primary Email:nate_sowa@med.unc.edu
Background: Rates of mental health conditions continue to rise, while access to care is challenging for many populations. As a result, rural hospitals face increasing numbers of patients presenting to emergency departments in crisis or being admitted to their medical units for treatment. Many hospitals do not have psychiatrists on staff, which can lead to delays in psychiatric evaluation. Telepsychiatry has proven effective in reducing wait times and lengths of stay, particularly in rural hospitals. The literature describing the use of psychiatric faculty at academic medical centers to provide telepsychiatry consultation to community hospitals is limited but shows that it is feasible, reduces the time to psychiatric consultation, and is well-received. However, descriptions of telepsychiatry services that incorporate asynchronous consultations (E-consults) are lacking. Here we present quantitative and qualitative data from a large telepsychiatry consultation service staffed by faculty from an academic medical center to support rural hospitals that use both synchronous (video) consults and E-consults.
Methods: A convergent mixed-methods design integrated quantitative analysis of all telepsychiatry encounters from July 2022 to March 2025 with qualitative interviews of psychiatry faculty (n = 5). Quantitative measures included patient demographics, social vulnerability indicators, consult duration, consult turnaround time, emergency department (ED) length of stay, and disposition outcomes. Qualitative data were collected through semi-structured interviews and analyzed using thematic analysis. Findings were integrated to identify convergent and divergent patterns across modalities and clinical contexts.
Results: Across 6,757 encounters, 6,586 (97%) were synchronous teleconsultations and 171 (3%) were E-consults . Live video consults had a median duration of 93 minutes (range 1–4,545), compared with 20 minutes for - consults. Median turnaround time was longer for synchronous consults than E-consults (175 vs 82.5 minutes). In contrast, average ED length of stay was shorter for synchronous encounters than E-consults (102 vs 270 hours). E-consults accounted for a larger share of consultations on inpatient medical and surgical units (31.0%) than in emergency departments (8.4%). Social vulnerability and digital readiness were similar between groups (median SVI 0.485 vs 0.455; median Digital Health Index (DHI) 0.570 in both). In interviews, psychiatrists generally preferred synchronous assessments but viewed E-consults as a more efficient option for lower acuity cases.
Discussion: This mixed-methods evaluation demonstrates that an academic medical center–based telepsychiatry service can effectively support rural hospitals using both synchronous and asynchronous modalities. Synchronous video consults remain the preferred approach for comprehensive assessment, while E-consults offer faster turnaround and greater efficiency for lower acuity inpatient cases. Together, these modalities expand access to psychiatric expertise, streamline clinical workflows, and provide a flexible model for meeting the growing behavioral health needs of rural communities.
Remote Neurology Consults to a Rural Mississippi Hospital: Addressing Specialist Shortages
Neil Maneck MS,1 Akshaya Vijayasankar,1 Poojah Keriwala,1 Brigham Walker PhD,2 Lindsey Kuiper PhD,1 Melody Narmour,1 Vinayak Nahar MD,1 Hao Mei PhD,1 Saurabh Chandra MD, PhD, MBA,1 Shreyas Gangadhara MD1
1University of Mississippi Medical Center and 2Tulane University
Primary Email:nmaneck@umc.edu
Background: Rural hospitals face severe neurologist shortages, limiting timely access to inpatient neurologic care. Teleneurology may offer a scalable solution, yet evidence comparing inpatient teleneurology rounding with in-person neurologist coverage in real-world rural settings is limited. The objective of the present study was to determine whether a part-time inpatient teleneurology service provides non-inferior clinical outcomes compared with in-person neurologist rounding in a rural community hospital.
Methods: This retrospective cohort study included all adult patients at a rural Mississippi community hospital who received at least one teleneurology consult between January 1 and December 31, 2023 (281 patients; 291 hospitalizations). A quasi-random assignment occurred because local neurology coverage rotated during the first half of each month, while teleneurology coverage occurred during the second half. Excess Days of Teleneurology represents how many more days teleneurology compared with in-person neurologist coverage was available for each patient. This measure captures the effect of substituting an additional day of teleneurology for a day of in-person coverage. Primary outcomes were hospital length of stay (LOS) and discharge to home. Bayesian generalized linear models assessed the association between Excess Days of Teleneurology and each outcome. Covariate balance testing evaluated whether exposure was quasi-random.
Results: No covariate demonstrated statistically significant association with Excess Days of Teleneurology, supporting quasi-random treatment exposure. In LOS models, the best-fitting non-linear specification showed a statistically significant negative association between teleneurology exposure and LOS (expβ = 0.76; 95% CI, 0.57–1.01; p = .0303*), while a linear model demonstrated a similar direction of effect (expβ = 0.99; 95% CI, 0.97–1.01). For discharge disposition, each additional teleneurology day increased the odds of home discharge by 6% (OR = 1.06; 95% CI, 0.98–1.15; p = .0711**), indicating a potentially significant positive effect. (*, **: p is posterior probability of telehealth inferiority, *: probability of positive association with LOS, **: probability of negative association with odds of home discharge)
Discussion: A rotating teleneurology rounding model produced hospital utilization outcomes comparable to in-person neurologist coverage, with trends toward shorter LOS and higher rates of discharge home. These findings demonstrate that teleneurology is a viable and effective strategy for addressing neurologist workforce shortages and maintaining high-quality inpatient neurologic care in rural settings.
Funding and Disclaimer (If abstract is accepted, this will appear in any published version of the abstract if word limits allow)
This abstract was made possible by the Health Resources and Services Administration (HRSA) of the US Department of Health and Human Services (HHS) as part of the National Telehealth Centers of Excellence Award (U66RH31459). The contents are those of the author(s) do not necessarily represent the official views of nor an endorsement by the HRSA, HHS or the US Government.
Advanced Care at Home: A Virtual Health Model for Pediatric Acute Home Care
Cynthia Zettler-Greeley PhD, Collin Miller RN, Jennifer Leidel MD, Sarah Wawrzynski PhD, CCRN, Kelsey Higgins, Abel Abraham
Nemours Children's Health
Primary Email:czettler@nemours.org
Background: Hospital at Home (HaH)– an inpatient health care model whereby patients recover from low acuity conditions at home while remaining under clinical care– offers many benefits, including reduced ED visits, cost savings, and high patient satisfaction. Patients report more personalized care and value receipt of care at home. HaH has been available for decades in Europe but has had limited adoption in the United States (U.S.). Whereas the COVID-19 pandemic inspired the launch of many U.S. adult HaH programs through application of CMS waivers, pediatric HaH models remain constrained by reimbursement challenges. Consequently, their implementation has lagged, depriving children of the many benefits inherent in home recovery and care. To overcome this barrier, we leveraged virtual technology to deliver clinician visits to pediatric patients eligible for home care. In this study, we describe the development and implementation of “Advanced Care at Home” (ACaH), a novel, tech-enabled, enhanced outpatient model of care.
Methods: ACaH is an enterprise-wide, quality improvement initiative enabling pediatric patients to meet clinical milestones while recovering at home. Following keen support from our health care system’s nursing and executive leadership, nurse leaders partnered with primary and specialty care providers to identify suitable cases based on clinical needs and capabilities. ACaH launched in the first of our two hospitals in April 2025 with the second following in December 2025. Enrolled patients meet outpatient eligibility criteria and are monitored 24/7 via a dedicated Virtual Command Center. Five clinicians, including two physicians, oversee patient care. Current in-home capabilities include telemedicine-administered virtual nurse visits customized based on levels of patient complexity, ranging from daily, to once a week, to on demand; clinical triage and escalation support; remote monitoring, including blood pressure, heart rate, pulse oximetry, weight, and end tidal CO2; enteral support; post-surgical monitoring; wound care; oxygen/ventilator weaning; and eating disorder support. Families receive medical devices as needed for monitoring in the home setting prior to discharge or via courier and may upload patient data to Epic MyChart.
Results: An abundance of performance KPIs and other metrics are being tracked to assess the success of the ACaH program, including operational and patient outcome metrics such as average daily census, length of stay, 30-day readmission rate, ED visits avoided, inpatient days saved, and patients graduated; clinical metrics such as nurse visit completion and provider visit completion; cost and revenue metrics; and satisfaction scores. To date, the average daily census is 87 patients, with 51 having graduated from the program. Since April 2025, the average number of admissions per month is 20 patients. Over 113 ED visits have been avoided, with associated cost savings from 30-day readmission avoidance estimated at $530,000. Likewise, 32 inpatient admissions have been avoided, resulting in an estimated cost savings (inpatient days saved) exceeding $592,000, yielding a total cost savings estimated at 1.1 million YTD. Length of stay in the hospital has been reduced by an average of 1.4 days. Over 2,690 nurse/provider visits have been administered to enrolled patients. Patient satisfaction, captured by Net Promotor Score (NPS) has held steady at 100% since the program’s inception.
Discussion: Leveraging our existing telemedicine infrastructure, in fewer than nine months of operation, ACaH has evidenced a profound impact on how our pediatric patients recover; reduced ED visits; saved over one million dollars in unnecessary health care costs; and consistently achieved high satisfaction scores among our patient-families enrolled in the program. The advanced care techs operating our centralized 24/7 Virtual Command Center monitor patients representing a breadth of medical complexity and a variety of diagnostic conditions, ranging from complex cardiac care to remote weight monitoring of “feeders and growers.” New services are being planned as capability allows, including home phototherapy treatment for newborns with hyperbilirubinemia. Future directions include staffing the Command Center with RNs 24/7 and continued enterprise expansion to support more children. These efforts demonstrate how the ACaH model may be leveraged to benefit children in other pediatric health care systems across the U.S.
Enterprise wide cost reduction and rural patient outreach through national tele-specialty program
Broderick Flynn RN/BSN/MSN, Bernard Ng MBBS, MSc
Veterans Affairs
Primary Email:broderick.flynn@va.gov
Background: The National TeleRheumatology Program (NTRP) launched in 2024 as an Office of Rural Health (ORH) Enterprise Wide Initiative (EWI) to address persistent rheumatology workforce shortages within Veterans Affairs (VA), particularly in rural areas. Many VA facilities lack onsite rheumatology care and rely on outsourcing to private providers. This outsourcing creates fragmented care, delay and has a high cost to the VA. NTRP leverages the VA's national telehealth infrastructure to improve access and decrease cost.
Methods: NTRP functions through utilizing the VA's telehealth infrastructure and provides care through clinic to clinic video and video to home modalities. NTRP has also created a hub and spoke model of care where documentation and workload are captured in a way that optimizes billing. NTRP has also utilized nationally implemented technology to gain access across the national electronic medical record to keep charting within patient side charts. The workflows that are in place allow for providers located across the country to maximize access and streamline care to rural areas. The process has also expedited access to veterans who previously did not have access to quality rheumatology care. Quality and charting compliance are monitored through national databases and specially tailored Power BI dashboards that NTRP service has created to monitor care. Protocols and specific criteria have been identified to assist in consult referral and have translated to high acceptance rate to program.
Results: NTRP has had great success in its deployment. Patient satisfaction is over 90% positive. Facilities that have adopted NTRP are satisfied with the program and have been identifying ways to better utilize the service. NTRP has been able to stay agile and is preparing to expand clinical teams in the next year. Sites that have adopted NTRP have also seen a decrease in wait time for rheumatology care for rural patients. NTRP's host site has seen increase in reimbursement through clinical visits captured.
NTRP by the numbers:
Number of patients served-2,045
Number of clinical visits-7,837
Number of medical facilities serviced-21
Top referring site savings-$350,435
Discussion: How can telehealth access rural patients in need of specialty care? What kind of technical infrastructure is needed to meet the needs of rural patients? Is there potential for telehealth expansion with advances in remote patient monitoring for other specialty care initiatives?
Pediatric dermatology for the Upper Midwest ECHO program evaluation: impact of a longitudinal multistate ECHO
1University of North Dakota School of Medicine & Health Sciences, 2University of Mississippi Medical Center, and 3Hometown Dermatology
Primary Email:mckenzie.burian@und.edu
Background: Less than 4% of pediatric dermatologists practice within a rural community, creating barriers to care for those not located in a metropolitan area. Project ECHO: Pediatric Dermatology for the Upper Midwest serves to improve dermatologic care for children living in rural areas. Each month virtual, synchronous ECHO sessions are held, offering health care professionals education on selected pediatric dermatologic conditions. Each session consists of a didactic portion and dedicated time for questions or case presentations. Following each session, participants receive a post-session survey. A prior retention of knowledge QI pilot with pre/post quiz format had limited response rates. This project continues our work to address the unique challenge of determining the true impact of a longitudinal (starting March 2024), open attendance (non-cohort based) subspecialty ECHO that reaches across multiple states and multiple health care touchpoints - including schools, clinics, and hospitals.
Methods: Descriptive statistics were used to analyze ECHO session attendance and survey data from March 2024 to December 2025, for a total of 21 sessions. Specific endpoints of interest included attendee location, attendee profession, and longitudinal attendance (i.e., the number of repeat attendances). After each session, participants were surveyed to evaluate each session for self-efficacy, clinical impact, and perceived utility of each session. An additional five sessions of attendance and survey data are anticipated by June 2026.
Results: This Project ECHO serves a target audience in the Upper Midwest, with 62% of participants living in rural or urban cities in Minnesota, North Dakota, Wisconsin, and Nebraska. Additional participants join from across the United States and several different countries, including India, Ecuador, Tanzania, and Mexico. Pediatricians and other physicians account for 45% of the participant population. School nurses account for 24% of participants. Other attendees include advanced practitioners, clinical nurses, and ECHO team members. Of the attendees who completed the post-session survey, 63% were found to be repeat participants. Pending the acquisition of further survey Results:, our final presentation will include a new analysis of perceived utility, self-efficacy and estimates of clinical impact - including estimates of students or patients helped.
Discussion: This revised program evaluation will present the impact and reach of a Pediatric Dermatology ECHO aimed at rural areas in the Upper Midwest. Further, this analysis lays the groundwork for examining the impact of longitudinal, open-attendance, subspecialty ECHO programs that reach across multiple states or health systems with a changing group of attendees. With this format, data capture Methods: within single-state metrics or health systems are not possible, presenting unique challenges in assessing efficacy. With a participant group comprised of physicians, school nurses, and other health care professionals throughout the Upper Midwest and across the United States, our evaluation will utilize participants' perceived value of attending. Through our project ECHO, we hope to help our attendees build upon core fundamentals within pediatric dermatology, ultimately helping them improve health care outcomes for their patients.
Evaluating Patient Activation Between In-person and Voice-enabled LLM Encounters
John Geracitano CISSP, CISM, CCNA, Zhaoqiang Zhou, Saif Khairat PhD, MPH, FACMI
University of North Carolina at Chapel Hill
Primary Email:johngera@unc.edu
Background: Patient activation, which encompasses knowledge, skills, and confidence in managing one's health, directly influences outcomes, health care utilization, and treatment adherence. Yet traditional patient-provider interactions face persistent barriers (e.g., limited access, time constraints, and asymmetric health literacy). Large language models (LLMs) with voice capabilities offer a potentially transformative solution, enabling scalable patient education and engagement. This pilot study directly compared patient activation and engagement following standardized consultations with a licensed physician and a voice-enabled LLM, using a within-subject design to control for individual variability. We hypothesized that while physician consultations would be rated highly, an appropriately designed voice-enabled LLM might achieve comparable patient-reported outcomes in measures of health management confidence and engagement.
Methods: A mixed-methods within-subject pilot study compared patient activation after consultations with a licensed physician and a voice-enabled LLM. Participants served as simulated patients in identical standardized scenarios, with consultation order randomized between participants. Immediately after each encounter, participants completed the 13-item Patient Activation Measure (PAM) survey, which uses five-point Likert scales to assess health self-management confidence across multiple domains: health responsibility, disease prevention, medication understanding, knowing when to seek care, communicating concerns, treatment adherence, understanding medical conditions and their causes, knowledge of treatment options, and maintaining lifestyle changes. Demographic data collected included sex, age, weekly LLM use, and prior experience with LLM voice features. Following the LLM consultation, participants answered open-ended questions about its strengths and weaknesses. We summarized quantitative responses using medians and interquartile ranges (IQR) and compared physician and LLM encounters using paired Wilcoxon signed-rank tests.
Results: Six participants (ages 22–40; 4 female) completed the study. Most reported moderate LLM use (66% used 0–10 hours weekly), while 50% had never used AI voice features, and 50% used them occasionally. Both consultation modalities received consistently high ratings across all 13 PAM items (median scores 4–5 out of 5), with similar variability (median IQR = 0.75 for both). Paired Wilcoxon signed-rank tests revealed no statistically significant differences between physician and LLM consultations on any measure (W = 0–1.5; all P ≥ 0.50). Descriptively, the LLM showed slightly higher median scores for items assessing the ability to raise health concerns, adhere to home treatments, understand medical conditions and their causes, and identify treatment options (differences of +0.5 to +1.0 points). Qualitative feedback highlighted the LLM's strengths in speed, structured delivery, clinical precision, clarity, and perceived empathy.
Discussion: This study shows that voice-enabled LLMs can achieve patient activation comparable to in-person physician consultations in standardized scenarios. Our findings extend existing research on LLM medical competence by examining patient-centered outcomes rather than clinical accuracy alone. Unlike prior text-based chatbot studies, we directly measured activation across self-management domains and found no significant differences between modalities. Slightly higher LLM ratings for communicating concerns and understanding treatments suggest advantages in consistent information delivery, addressing known variability in patient-provider communication. Perceived empathy challenges assumptions about irreplaceable human connection in health care. Limitations include a small and young sample and a lack of long-term outcome data. Future research should examine diverse populations, real patients, and sustained behavioral change to assess the appropriate integration of LLM tools as scalable adjuncts to patient education when physician access is limited.
Expanding and Sustaining Video Visit Utilization in Primary Care
Britney Malone MHA
University of North Carolina Health
Primary Email:Britney.Malone@unchealth.unc.edu
Background: To increase utilization of video visits across primary care clinics and support a hybrid (in-person and virtual) model of care, our virtual care center revamped its Video Visit Education curriculum in FY24. The goal was to expand access to care, optimize in-person clinic capacity, and standardize virtual care workflows across practices. A pilot was launched at five health care system primary care clinics to test the effectiveness of a structured, practice-level education and adoption strategy.
Methods: The center implemented a comprehensive education and engagement approach designed to support providers and clinic staff in adopting video visits as a routine care modality. The approach focused on role-based education and practice-level data to ensure relevance and sustainability.
Key components included:
In-person and virtual education sessions for practice managers, providers, clinical staff, scheduling teams, and front desk staff.
Clinic site visits to engage stakeholders, reinforce workflows, and provide hands-on training.
Patient Risk Assessment Score education, enabling schedulers and providers to identify patients most appropriate for video visits.
Direct patient advertising, developed in collaboration with Marketing, including flyers and posters placed in exam rooms, waiting areas, and restrooms to encourage patients to ask about video visit options.
Front desk and nursing engagement, encouraging staff to proactively inform patients that eligible visits may be conducted via video.
The objective of the education was for end users to demonstrate correct video visit workflows specific to their role and understand the value of video visits in improving access and care delivery.
Results: FY24 Pilot Results (5 Clinics):
212% increase in video visit volume, rising from 34 to 107 visits per month.
6% decrease in telephone visit volume, indicating a shift toward more appropriate virtual care modalities.
FY25 Expansion Results:
Building on the success of the initial FY24 pilot, the Video Visit Education curriculum was expanded to two additional regions in FY25.
Initial Pilot Region 1 (5 clinics)
Sustained growth through monthly dedicated virtual care days for each provider.
Continued use of the Video Visit Education curriculum across all five clinics.
Year-over-year video visit volume increased by 114% to 2,696 visits in FY25 from 1257 visits in FY24.
Second Pilot Region (3 clinics)
Adopted the Video Visit Education curriculum in FY25.
Implemented integrated care strategies to increase virtual visit utilization.
Year-over-year video visit volume increased by 113% to 991 visits in FY25 from 465 visits in FY24.
Third Pilot Region (3 clinics)
Implemented monthly virtual care half-days for providers in FY25.
Improved access while reducing strain on in-person clinic operations.
Year-over-year video visit volume increased by 700% to 200 visits in FY25 from 25 visits in FY24.
Discussion: The initial pilot demonstrates that structured, role-based education combined with operational and patient-facing strategies can significantly increase video visit utilization in primary care settings. Sustained growth in the initial pilot region and rapid adoption in the subsequent pilot regions highlight the scalability of this model. Key drivers of success included provider engagement, staff empowerment at the front desk and nursing level, data-informed patient selection, and direct patient education within clinic settings. Together, these elements supported a cultural shift toward viewing video visits as a standard and effective care modality. This initiative supports the health care system’s broader goal of delivering hybrid care by improving access, optimizing in-person clinic capacity, and embedding virtual care into routine primary care workflows.
Mining UDS Data for Telehealth Program Performance Metrics
Jonathan Neufeld PhD
University of Minnesota
Primary Email:jneufeld@umn.edu
Background: Community health centers deliver comprehensive primary care to 10–14% of the population of the United States annually, making them the single largest organized primary care “system” in the country. In 2020, community health centers first began reporting their telehealth encounters to federal funders on an annual basis, along with other data submitted via the Uniform Data System (UDS). There is a great deal of public information available on the clinical and administrative functioning of CHCs, including detailed information on their use of telehealth technologies. It is of great interest to see what CHC characteristics are associated with virtual visit volume and overall program success, and to see how health centers can more effectively evaluate the performance of their virtual care programs through comparisons with their peers.
Methods: Uniform Data Set tables were downloaded from the CMS website (data.cms.gov) for 2024 and analyzed using standard data management software libraries (R, Python/pandas). The total number of patients served across the health center was used to develop size cohorts, and health centers were compared to both the total group and to their similar-size cohorts. Variables derived from volume and cost tables were computed to reflect telehealth program efficiency, primary care vs behavioral health volume, and costs associated with virtual service delivery. Links to external data sources for detail on claims were added as available. Site-to-site comparisons were done using z-scores for a variety of variables of interest, calculated in comparison with both the total set of health centers and only those in the similar-size cohort. A web-based browsing tool was developed to allow for simple querying.
Results: A great deal of variability was found among health centers of all sizes. Presenting overall statistics, including histograms of total health center size, was found to be informative. Calculating z-scores within similar-size cohorts, however, allowed for more precise comparison of program performance versus relevant peers than overall averages and z-scores. Tables and figures showing distributions of critical derived variables and how the scores can be used in program evaluation will be presented and discussed. Results: suggest that health centers can gain extensive insights into the performance and effectiveness of their virtual care programs by using z-score comparisons of specific variables with reference to similar-size cohorts.
Discussion: Telehealth and virtual care services research is moving beyond visit counts and beginning to explore better ways to measure effectiveness, efficiency, and program performance. Using a rich data set like the UDS, we were able to derive measures that allow meaningful comparisons among health centers of comparable size and resource bases. It is hoped that these comparison tools can support more effective evaluation of telehealth programs.
Leveraging Tele-Critical Care to Support Rural Hospitals: Insights from a Mississippi Implementation
Md Rokibul Hasan MSc, Farhana Lima MSc, Rhea Arora, MS, Lindsey Kuiper PhD, Hao Mei, PhD, Saurabh Chandra MD, PhD, MBA
University of Mississippi Medical Center
Primary Email:mrhasan@umc.edu
Background: Rural hospitals often lack access to intensivists, leading to delays in critical care decision-making, higher transfer rates, and increased strain on limited resources. Tele–critical care (TCC) provides a mechanism for real-time specialty support, but implementation in rural Southern hospitals remains limited. To address these gaps, a Tele-critical Care Program (TCCP) was established to provide 24/7 remote intensivist consultation to a rural Mississippi hospital, aiming to enhance clinical decision support, manage complex patients locally, and improve operational outcomes.
Methods: Retrospective chart review (November 2023 – July 2024) examined TCCP utilization and clinical patterns at two rural Mississippi hospitals. Intensivists provided remote consultation via EMR access and an audiovisual cart system integrated into Emergency Department and inpatient workflows. Data included patient demographics, consultation timing, reason for admission, reason for TCC consult, number of follow-up encounters, discharge disposition, and provider order entry. Descriptive analyses characterized utilization patterns across clinical conditions. Analyses also included one-way ANOVA to test differences between discharge disposition and time-to-TCC (defined as time from hospital admission to first TCC consultation) and correlation analysis evaluated the association between time-to-TCC and hospital length of stay (LOS).
Results: Data from 145 patients were included in the analysis. TCC encounters were primarily used for severe conditions such as respiratory, cardiac, neurologic, and infectious/sepsis diagnoses, reflecting selective deployment when local clinical capacity was insufficient. While most patients required one TCC encounter, repeated follow-ups were more frequently seen among patients with complex conditions, especially those with respiratory failure, sepsis, and renal/metabolic disorders. Time-to-TCC varied significantly across discharge outcomes (ANOVA F = 4.55, p < 0.001). Moreover, a statistically significant moderate positive correlation was identified between time-to-TCC and hospital length of stay (r = 0.48, p < 0.000001). Patients receiving three or more TCC consultation were more often transferred to inter-facility transfer, reflecting greater illness severity.
Discussion: At these rural Mississippi hospitals, implementing TCC provided timely access to intensivist expertise and revealed meaningful associations between consultation timing, need for follow-up, and patient outcomes. The variation in time-to-TCC and frequency of TCC engagement was associated with differences in discharge disposition and hospital length of stay, supporting the program’s role in improving clinical decision support and stabilizing local care delivery. These findings highlight the value of TCC as a scalable model for rural hospitals seeking to enhance complex patient management despite limited on-site critical care resources.
Improving access to telehealth services in a charitable pharmacy
Matthew Chong PharmD, Treston Warren PharmD, Madison Luck PharmD, Lydia Bailey PharmD, BCACP
St. Vincent de Paul Charitable Pharmacy - Cincinnati
Primary Email:pharmacyresident@svdpcincinnati.org
Background: Serving over 12,000 underserved patients of diverse Background: s, a Southwest Ohio charitable pharmacy has dispensed over 1 million free prescriptions and provides no-cost clinical and primary care services valued at $5 million per year. These services include periodic follow-up with patients by phone and text message. Using a multi-round quality improvement process over the course of a year, pharmacy text communication was transitioned to an updated platform. Previous studies have largely used clinical outcomes as endpoints, yet few have investigated telehealth’s impact on organizational workflow.
Methods: This study will assess the effect of the charitable pharmacy’s updated telehealth texting platform on patient follow-up efficiency. As the primary endpoint, the study will compare the number of successful interventions made during three consecutive 3-month periods: pre-implementation of the new platform, post-implementation, and post-implementation with the addition of standardized training. During the final 3 months, 4th year pharmacy students were also asked to log the length of time to patient response with telephone calls versus texting, which will serve as the secondary endpoint. Both endpoints will be assessed using paired t-tests.
Results: Preliminary data has shown that out of over 1000 follow-ups completed in the 3 months prior to the implementation of the new texting platform, over 70% were successful. The success rate increased to 75% after the platform was implemented. Third trimester data with the inclusion of standardized training began in the first quarter of 2026 and is still in progress.
Discussion: Telehealth can allow providers to reach more patients quickly and frequently. More patients are also likely to use telehealth to communicate, highlighting the importance of incorporating digital communication into existing workflows in all areas of practice. The results of this study will also help direct best practice for telehealth workflow.
Validating Telehealth Competence Through Standardized Patient Encounters in Graduate Nursing Education
Renee Wadsworth BSBA1, Tina Gustin DNP, APRN, CNS, FAAN2
1SP-ed and 2Old Dominion Univerrsity
Primary Email:rwadsworth@sp-ed.com
Background: As telehealth becomes integral to health care delivery, graduate nursing programs require reliable Methods: to assess learner competence in virtual care. Many programs rely on peer-to-peer role-play for telehealth assessment due to logistical convenience; however, peer evaluation can introduce inconsistent scoring, variable feedback quality, scheduling challenges across time zones, and reduced confidence in competency validation. This project addressed a gap in telehealth competency validation by replacing peer-evaluated role-plays with structured, graded standardized patient (SP) telehealth encounters embedded into a required graduate nursing course. The initiative aimed to improve assessment reliability, feedback quality, learner confidence, and faculty assurance while establishing a repeatable quality measure for telehealth competency within connected health education.
Methods: A structured SP telehealth encounter was embedded into a required graduate nursing course as a graded competency assessment. Prior to implementation, a telehealth evaluation rubric was developed and reviewed for clarity and reliability. SP cases were designed by content experts to ensure relevance across graduate nursing roles, and SPs were trained using experienced SP educators. Each learner completed a 20-minute synchronous telehealth encounter conducted via a digital simulation environment. Three case options were offered to align with varied clinical interests: a primary care abdominal pain visit, a behavioral health consultation, and a pre-operative anesthesia evaluation. Scenarios and rubrics will be made available to support replication. Learners received a standardized pre-brief outlining expectations and encounter logistics. SPs assessed performance using the validated rubric and provided immediate verbal feedback. Learners then submitted a one-page reflective integration plan describing how telehealth competencies would be applied in current or future practice. Centralized scheduling was used to reduce logistical barriers, missed sessions, and time zone conflicts, supporting consistent implementation across cohorts.
Results: The transition to structured SP telehealth encounters resulted in improved logistical efficiency and more reliable competency validation compared to peer-evaluated role-plays. Assessment outcomes demonstrated greater rubric consistency, fewer contested grades, and decreased instances of missed or late sessions. Standardized scoring and feedback supported earlier identification of learners requiring remediation. In the Telehealth Interpersonal Skills Checklist (TIPS-CH), SPs marked highest scores (“very good”) to environment/privacy (95–97%) and eye contact (90–100%), while empathy showed greater variability (48–79%), highlighting empathy as a high-impact coaching target. Across 100 post-encounter surveys, 97% agreed or strongly agreed the experience was educationally valuable. Learners reported increased confidence in telehealth communication, clinical reasoning, professionalism, and etiquette. Notably, 95% rated the digital SP encounter as helpful or more helpful than face-to-face SP sessions. These findings support structured SP encounters as both a valid competency assessment and a learner-accepted modality for telehealth education.
Discussion: Embedding standardized patient encounters into graduate nursing curricula offers a consistent, equitable, and sustainable approach to telehealth competency validation compared to peer-based assessment models. This approach ensures uniform rigor across learners, improves feedback quality, and supports timely identification of remediation needs. Centralized scheduling and standardized evaluation processes reduce logistical burden while enhancing reliability. Structured post-encounter reflection reinforces the transfer of telehealth competencies into clinical practice. SP-based telehealth assessments represent an effective quality initiative for graduate nursing education and provide a scalable, replicable model for validating telehealth competence within connected health training programs.
Evaluating a Direct-to-Consumer Maternal Health Remote Patient Monitoring Program for Rural Mississippi
Tearsanee Davis DNP, FNP-BC, PMHNP-BC, FAANP, Tiffany Regan RN
University of Mississippi Medical Center
Primary Email:tcDavis2@umc.edu
Background: Rural Mississippians face profound maternal health disparities, driven by a confluence of barriers: limited access to prenatal, high-risk pregnancy management, and postpartum care, a critical shortage of mental health services, and significant socioeconomic challenges. Traditional clinic-based models alone cannot meet the complex needs of this population. This comprehensive Remote Patient Monitoring (RPM) program is designed to supplement traditional maternal health care and address multifactorial gaps in care by providing innovative monitoring, timely interventions, and enhanced access to essential maternal health services. The objectgive of this study was to evaluate the feasibility, clinical outcomes, and impact of a direct-to-consumer (DTC) maternal health RPM program designed for rural pregnant individuals in Mississippi. To improve health outcomes, reduce disparities, and empower patients by integrating remote monitoring with traditional care models.
Methods: We conducted a prospective cohort study to evaluate the impact a comprehensive maternal remote patient monitoring program that supplements traditional maternal care could have on maternal and infant outcomes. Participants in the program received:
Biometric Monitoring: Blood pressure and glucose monitoring with Bluetooth-enabled devices, enabling timely nurse-led intervention and care coordination.
Structured Patient Education: Trimester-specific educational content to improve health literacy and empower informed decision-making.
Mental Health Support: Systematic mental health screenings with immediate pathways to free, virtual counseling and psychiatric services.
Care coordination: Social determinants of health (SDOH) screenings, paired with personalized assistance from a dedicated maternal RN to connect patients with community resources.
Results: At the time of this submission, data analysis is underway. Preliminary findings have shown that there is a positive impact on maternal and infant birth outcomes when mothers received needed support via telehealth. Preliminary data and reviewed literature confirm that such integrated models:
Improve Mental Health Access: Embedding mental health screening and virtual treatment into routine maternity care bypasses stigma and geographic isolation.
Address Resource Scarcity: The dedicated RN care coordinator actively identifies social needs (e.g., food, housing) and facilitates resource linkage, filling a critical gap left by overburdened clinic staff.
Overcome Systemic Barriers: Home-based monitoring reduces transportation barriers to effective and quality care. The program's proactive, structured support between appointments provides a supplemental safety net unavailable in traditional, appointment-only models.
Discussion: This study will provide critical evidence on the implementation of a comprehensive maternal health RPM program in a high-need, rural setting. Findings will inform best practices for using telehealth/RPM to improve access, equity, and outcomes for mothers and infants, with potential implications for sustainable, scalable care models.
National Trends in Telehealth Utilization Among Individuals With at Least One Prescription Past Year (2020-2023)
Background: The study aims to assess the trends of telehealth utilization among individuals with at least one prescription from 2020 to 2023.
Methods: A cross-sectional study was conducted using merged data from the National Health Interview Survey (NHIS) from 2020 to 2023. This sub analysis included individuals with at least one prescription (Nf83,721) in the past year. The primary outcome was telehealth utilization determined by whether a participant had a virtual medical appointment in the past 12 months. Descriptive analysis was conducted and stratified by year. Both unweighted and weighted multiple logistic regression were conducted and used to predict the study outcome adjusting for sociodemographic factors, health status, and health access-related variables. The statistical analysis was conducted using SPSS and SAS at an alpha of 0.05.
Results: A total of 83,721 individuals with at least one prescription were included in the study. Overall, telehealth utilization was estimated at 41.3% with the highest use observed in 2021 (49.1%).Weighted logistic regression showed that females, those with at least a 12th-grade education, individuals of other races, and Hispanic ethnicity had higher odds of using telehealth at a significance level of p<.05 adjusting for other factors. Having health insurance, income above the poverty level, a recent doctor visit, and receiving home health care were also significantly associated with increased telehealth use at a significance level of p<.05 adjusting for other factors.
Discussion: Telehealth utilization was high with the highest levels observed in 2021 likely due to COVID-19. Education, insurance, income, recent health care visits, and home care were key predictors of telehealth. These important factors can help inform policy decisions on telehealth extensions in the future.
Telehealth Integration in Regional Neonatal Care: A Children’s Hospital’s Experience Using a Hub-and-Spoke Model
Michelle Mejia MD, Rachel Umoren MBBCh, MS, Megan Gray MD, Mark Lo, MD, MS
Seattle Children's Hospital
Primary Email:michelle.mejia@seattlechildrens.org
Background: While regionalized care has improved survival for high-risk neonates, it has also created gaps in specialized newborn care in rural areas. Telehealth helps fill this void, extending neonatal expertise beyond tertiary centers into special care nurseries (SCN) in community facilities providing lower levels of neonatal intensive care. Despite growing adoption of telehealth for neonatology, there are few reports on post-implementation processes and quality improvement (QI) measures, curbing our understanding how telehealth programs evolve and stabilize over time. The objectgive of this study was to assess telehealth adoption and engagement trends across three regional Level II SCNs within a hub-and-spoke framework using Statistical Process Control (SPC) c-chart analysis.
Methods: Seattle Children’s Level IV NICU implemented a hub-and-spoke telehealth service that supports regional NICUs through real-time consults and virtual rounds. We conducted a retrospective review of telehealth engagements—including all interactions via consults and multidisciplinary rounds—from Q3 2020 to Q2 2025. SPC c-charts were generated for individual and overall telehealth utilization: Site 1 (go-live: 2021), Site 2 (2021), and Site 3 (2022). Control limits were calculated to identify special cause variation and assess process stability.
Results: Total engagement showed minimal activity during the first five quarters, followed by a sharp rise and sustained use. After the initial ramp-up, most data points remained within control limits (CL = 75.6; UCL = 101.6; LCL = 49.5). A brief decline occurred in Q3 2024, after which engagement stabilized (CL = 60.5; UCL = 83.8; LCL = 37.2). Two instances of positive special-cause variation were identified, and overall performance remained stable within control limits, indicating consistent utilization and program maturity.
Site 1 demonstrated low early engagement, peaking at 68 sessions in Q4 2023, followed by a gradual decline to an average of 19.3 sessions/quarter from Q3 2024–Q2 2025. Two stable phases are evident, with a downward shift in Q3 2024 suggesting potential process drift or external influences.
Site 2 showed steady early growth, peaking at 27 sessions in Q2 2023, then declining to a stable average of 11.7 sessions/quarter from Q1 2024–Q2 2025. Two stable phases are present, with a downward shift beginning in Q1 2024 indicating operational or contextual factors affecting use.
Site 3 exhibited gradual growth after its 2022 go-live, peaking at 33 sessions in Q4 2024. Continued upward but unstable trends through Q1 2025 suggest ongoing adoption and potential process changes requiring further review.
Discussion: SPC analysis across three Level II SCNs demonstrates successful but heterogeneous telehealth adoption, with early ramp-up followed by site-specific stabilization or decline. A centralized hub-and-spoke framework enabled scalable implementation, standardized workflows, and sustained utilization, supporting diffusion beyond initial champions. SPC charts proved useful for ongoing operational surveillance, allowing timely detection of shifts and trends. Notably, observed special-cause variation warrants targeted investigation to identify drivers of negative utilization (e.g., staffing changes, scheduling friction, competing priorities) and to amplify facilitators of ongoing adoption (e.g., streamlined triage, reliable technology, feedback loops, and local clinical leadership). Programs should pair SPC monitoring with structured rapid-cycle improvement to mitigate drift, reinforce stability, and adapt to evolving community needs, ensuring durable access and equity in regional neonatal care.
The Case for National Standards and Integrated Metrics in Virtual Care Reporting
Tazeen Farooque MHA, Madeleine Williams
UNC Health Virtual Care Center
Primary Email:Tazeen.Farooque@unchealth.unc.edu
Background: Virtual care utilization has expanded across health systems, yet the field lacks standardized definitions, consistent terminology, and national benchmarks for reporting. As a result, organizations often rely on locally developed metrics that vary widely in scope, inclusion criteria, and interpretation. This inconsistency limits the ability to compare performance, assess quality, track outcomes, or evaluate equity across institutions. It also reinforces the idea that virtual care is separate from traditional care delivery, when in fact it should be measured alongside and integrated into the same operational and clinical frameworks used for in-person care. Establishing standardized definitions and embedding virtual care metrics within existing health system measures are essential steps toward improving comparability, accountability, and long-term research on the quality and effectiveness of virtual care.
Methods: We conducted a comprehensive review of all business terms and measures (“assets”) documented within six UNC Health Virtual Care Enterprise Dashboards using Collibra, a data catalog platform. For each asset, we captured the name, type (business term or measure), definition, calculation logic, inclusion/exclusion criteria, data location, and responsible domain. We then audited each asset to determine whether it was specific to a virtual care workflow or represented a community metric also used in other care settings. To understand the origin and consistency of definitions, we assessed which stakeholders, analysts, operational leaders, or clinical teams developed each metric and whether any aligned with external or national standards. Finally, we evaluated the extent to which virtual care metrics could be integrated into standard enterprise reporting structures.
Results: Across six enterprise dashboards, we identified 39 total assets. Twenty-eight assets (72%) were specific to virtual care use cases, while 11 (28%) were community assets already used in emergency services, hospital operations, or quality reporting. None of the virtual-care–specific assets were designed to align with national definitions or external standards; all were internally developed by UNC Health analysts in partnership with operational teams. Several virtual care measures, such as Advanced Care at Home operational and quality metrics, closely mirrored metrics routinely used in in-person care but were reported separately due to the absence of shared definitions. This separation reinforced siloed reporting structures and limited opportunities for integrated dashboards that could assess virtual and traditional care side-by-side using consistent logic.
Discussion: Our analysis highlights significant variation in how virtual care metrics are defined and reported, even within a single health system. The absence of national standards leads to fragmented reporting and prevents meaningful comparisons across organizations. Equally important, many virtual care metrics mirror traditional operational and clinical measures, suggesting that virtual care should be incorporated into established enterprise metric frameworks rather than treated as an isolated modality. Developing standardized definitions and national benchmarks while also embedding virtual care within systemwide reporting would improve data quality, comparability, and accountability. These steps are essential for evaluating virtual care performance, guiding policy, and supporting the integration of virtual care as a core component of modern care delivery.
Evaluating AI-enabled fall prevention in Virtual Nursing
Svara Narain MS, Hao Mei PhD, Lindsey Kuiper PhD, Briana S. Petty MSN, RN, Saurabh Chandra MD, PhD, MBA
University of Mississippi Medical Center
Primary Email:svaranarain1994@gmail.com
Background: Inpatient falls remain a persistent patient safety concern associated with preventable harm and increased health care utilization. As connected health systems integrate artificial intelligence into virtual nursing workflows, rigorous evaluation Methods: are required to assess their impact on safety outcomes. In February 2025, an AI-enhanced fall prevention feature within Artisight was implemented in two inpatient pilot units (4N and 6W) at the University of Mississippi Medical Center (UMMC). This evaluation prioritizes inferential Methods: to estimate changes in falls outcomes attributable to implementation, while minimizing reliance on descriptive monitoring alone. The objective of this study was to assess whether AI-enabled virtual nursing was associated with changes in inpatient falls using a quasi-experimental design, supported by visualization tools to aid interpretation.
Methods: Difference-in-Differences (DiD) regression models were applied to monthly inpatient falls data from UMMC to evaluate changes associated with AI-enabled virtual nursing implementation. Pilot units (4N and 6W) were compared against non-pilot like units that did not implement the AI-enabled feature during the study period, serving as control groups. Falls outcomes were normalized by patient-days to account for differences in patient volume. Primary outcomes included total falls, falls with harm, and falls without harm. To support interpretation and communication of statistical findings, two unit-specific dashboards were developed for 4N and 6W. Dashboards included a line chart of monthly raw fall counts, a slope chart comparing total falls during the nine months before and nine months after implementation, and KPI indicators summarizing percentage changes. Dashboards were designed as supportive tools to contextualize DiD Results: rather than to generate inferential conclusions.
Results: DiD analyses demonstrated heterogeneous effects across pilot units relative to controls. In 4N, total falls decreased significantly following implementation (−1.30 falls per 1,000 patient-days, p = 0.02), driven in part by a significant reduction in harmful falls (−0.44 falls per 1,000 patient-days, p = 0.01). Changes in non-harmful falls were smaller and did not reach statistical significance. In 6W, no statistically significant differences in total, harmful, or non-harmful falls were observed relative to controls, consistent with low baseline fall incidence prior to implementation. Dashboard visualizations aligned with statistical findings by illustrating temporal trends, pre-intervention stability, and post-implementation variability. The integration of DiD modeling with visual summaries supported distinction between intervention-associated changes and routine fluctuation without overstating results.
Discussion: This evaluation demonstrates the value of Difference-in-Differences analysis for assessing AI-enabled fall prevention initiatives within connected health systems. Applying a quasi-experimental framework with appropriate control units strengthens causal interpretation, while dashboards support transparent communication of findings. Together, these methods provide a rigorous and practical approach for evaluating virtual nursing interventions. Future work will extend follow-up periods and incorporate stratification to further strengthen evaluation of AI-enabled virtual nursing interventions.
Monitoring AI-enabled fall prevention in Virtual Nursing
Svara Narain, MS, Lindsey Kuiper PhD, Briana S. Petty MSN, RN, Saurabh Chandra MD, PhD, MBA
University of Mississippi Medical Center
Primary Email:svaranarain1994@gmail.com
Background: Patient falls remain a critical inpatient safety concern, often resulting in preventable harm, increased length of stay, and added health care costs. As hospitals adopt virtual nursing (VRN) and AI-enabled fall prevention technologies as connected health interventions, there is a growing need for transparent and interpretable tools to evaluate safety outcomes. In February 2025, an AI-enhanced fall prevention feature within Artisight was implemented in two inpatient pilot units at the University of Mississippi Medical Center (UMMC), 4N and 6W. While falls data are routinely collected, they are often presented in static reports that limit longitudinal interpretation and operational use. To address this gap, two unit-specific, interactive falls dashboards were developed to support evaluation of fall patterns before and after VRN implementation. The purpose of these dashboards is to translate routinely collected safety data into actionable insights for clinical, quality, and telehealth stakeholders.
Methods: Separate dashboards for inpatient units 4N and 6W were developed using a consistent, unit-specific analytic approach that prioritized longitudinal comparability around the February 2025 implementation of AI-enabled fall prevention within the VRN program. Institutionally reported falls data were structured into aligned pre- and post-implementation windows, enabling within-unit comparisons without cross-unit aggregation. Visual encodings were deliberately chosen to balance interpretability and analytic rigor: monthly line charts were used to preserve temporal continuity and highlight underlying trends, while slope charts were employed to clearly communicate directional change between matched nine-month pre- and post-implementation periods. KPI cards were calculated to summarize relative percentage change, reinforcing the key comparison while minimizing cognitive load for non-technical stakeholders. Overall, the dashboards apply a standardized yet flexible framework that emphasizes transparent pre/post evaluation, reproducibility, and accessibility for decision-makers.
Results: The dashboards offer a consolidated view of falls data for both pilot units that was previously unavailable in a single analytic tool. In 4N, visualizations demonstrated a reduction in fall counts during the post-implementation period, reflected in both longitudinal trends and slope chart summaries. In 6W, fall counts increased from a low baseline following implementation, largely due to non-harmful events, with no corresponding increase in harmful falls. Presenting raw monthly trends alongside aggregated pre/post comparisons improved interpretability and helped contextualize observed changes. Stakeholders reported improved clarity in understanding unit-level fall patterns and increased confidence when discussing the impact of AI-enabled virtual nursing on fall prevention.
Discussion: These unit-level dashboards demonstrate how applied analytics can support the evaluation of AI-enabled virtual nursing interventions using routinely collected patient safety data. By combining intuitive visualizations with clear pre/post comparisons, the dashboards facilitate transparent, data-informed Discussion:s at the unit level without overstating outcomes. Future directions include extending post-implementation observation periods and incorporating stratification to further strengthen evidence-based evaluation of connected health technologies.
Scaling virtual nursing across inpatient units: Early experience
Bethany Smith BSN, RN, Lindsey Kuiper PhD, Saurabh Chandra MD, PhD, MBA, Briana S. Petty MSN, RN
University of Mississippi Medical Center
Primary Email:bhsmith2@umc.edu
Background: Health systems face increasing strain from nursing workforce shortages, high turnover, and growing clinical complexity, particularly in acute care settings. Virtual nursing has emerged as a promising care delivery model to support bedside nurses, enhance patient throughput, and improve staff satisfaction without replacing in-person care. This abstract describes the phased implementation and early outcomes of a virtual nursing program designed to augment bedside nursing practice through remote admission, discharge, and supportive clinical workflows across adult inpatient units.
Methods: A virtual nursing program was implemented in a large academic medical center using a phased expansion model. The program initially supported one adult inpatient unit and later expanded to a second unit, increasing total bed coverage from 14 to 46 beds. Virtual nurses collaborated with bedside teams to complete standardized admission and discharge workflows, provide real-time clinical support, and assist with documentation and patient education. Program impact was evaluated using operational metrics (volume of virtual admissions and discharges), nursing workforce measures (bedside nurse retention and turnover), and staff satisfaction surveys collected on the newly added unit at baseline, pre implementation, 3 months, and 6 months after implementation.
Results: Between March 2023-February 2025 (Phase One), virtual nurses completed 641 admissions and 971 discharges. Admissions and discharges increased in February 2025 due to expanding to an additional 32 bed unit. During Phase Two (February 2025-December 2025), the virtual nurses completed 2,580 admissions and 2,578 discharges. Overall, saving the bedside nurses a total of 3,351 hours (279 12-hour shifts). Staff satisfaction on the newly added unit improved steadily with time particularly in domains related to workload and perceived support. Early concerns largely resolved by 3 months, and by 6 months all respondents report satisfaction. Bedside registered nurse retention, improved, and turnover decreased following implementation, with the first unit having zero nursing turnover in the first 18 months. After expansion to the additional unit, retention trends remained, supporting the sustainability of the virtual nursing model. Bedside registered nurse retention improved, and turnover decreased following implementation, with 36% turnover (February 2024-February 2025) compared to14% turnover (February 2025-October 2025).
Discussion: Early findings suggest that virtual nursing can effectively augment inpatient nursing care by supporting high-burden workflows, improving staff experience, and contributing to improved nurse retention. The phased expansion model demonstrates scalability across units while maintaining positive workforce and operational outcomes. Virtual nursing represents a viable strategy for health systems seeking innovative, non-commercial approaches to strengthen nursing practice and care delivery in acute care environments.
Improving Hypertension Outcomes Through a Structured Remote Patient Monitoring Program: A 12-Month Case Study
Xiaoxu Kang PhD,1 Ergi Gumeseneli MD2
1KangarooHealth, Inc. and 2Grand Junction Psychiatry
Primary Email:hello@kangaroohealth.com
Background: Remote Patient Monitoring (RPM) integrated with Chronic Care Management (CCM) programs supports chronic hypertension management by enabling continuous physiologic data collection outside clinical settings. Structured RPM-CCM programs can improve blood pressure control, patient engagement, and timely clinical interventions. Outcomes, however, depend on program design, patient education, adherence tracking, and escalation protocols. This abstract presents a case study of a 2,500-patient RPM-CCM program, highlighting implementation best practices and demonstrating measurable improvements in patient outcomes over a 12-month period.
Methods: This case study included 2,500 patients with hypertension enrolled in an RPM-CCM program. Patients received home blood pressure monitors and followed individualized monitoring schedules. Data were transmitted to a centralized platform, reviewed by trained care coordinators, and escalated to clinicians based on pre-defined thresholds. Program best practices included standardized onboarding, patient education, adherence tracking, and structured escalation workflows. Outcomes over 12 months included blood pressure trends, patient adherence, clinical interventions triggered by alerts, and urgent care utilization. Care team feedback assessed workflow efficiency and patient engagement.
Results: Over 12 months, adherence to daily blood pressure monitoring exceeded 85%. Mean systolic blood pressure decreased by 6 mmHg and diastolic by 4 mmHg. Structured escalation enabled timely clinical interventions, reducing non-urgent emergency department visits by 20% compared with baseline. Patients reported increased confidence in self-management, and care teams reported improved workflow efficiency and clinical decision-making. These findings indicate that outcomes were driven primarily by program design, standardized workflows, and patient and clinician education rather than device technology alone.
Discussion: This RPM-CCM case study demonstrates that structured monitoring programs can improve hypertension management, enhance patient engagement, and reduce unnecessary health care utilization. Success depends on standardized workflows, dedicated clinical review, patient education, and clear escalation protocols. Integrating RPM with CCM into routine care enables multidisciplinary teams to leverage telehealth to achieve measurable improvements in chronic disease outcomes and provides a scalable, quality-driven model for connected health programs.
Telehealth use, barriers, and user experience among adults in Mississippi: A population-based survey
1University of Mississippi Medical Center, 2Mississippi State University, and 3Delta Community Solutions, LLC
Primary Email:ccompretta@umc.edu
Background: Telehealth can reduce geographic and socioeconomic barriers to care and became a routine component of health care delivery following its rapid expansion during the COVID-19 pandemic. However, use remains uneven, and population-representative evidence on current utilization and experience is limited. Mississippi exhibits substantial variation in health care access and digital readiness across communities, making it a relevant setting to examine contemporary telehealth use. Beyond uptake alone, understanding patient experience is essential for assessing the value and sustainability of telehealth in routine care.
Methods: We analyzed the Mississippi Telehealth Survey, a statewide dual-frame random-digit-dial telephone survey of household adults aged ≥18 years conducted from September 2024 to May 2025. The probability-based design produced a representative sample with 1,250 completed interviews. Survey weights were applied to produce population-level estimates aligned with Mississippi demographic benchmark. Weighted descriptive analyses were conducted to examine telehealth utilization patterns across demographic, socioeconomic, insurance, and internet access characteristics. Multivariable logistic regression models were then used to identify factors independently associated with telehealth use while adjusting for potential confounders. Additional weighted descriptive analyses assessed reasons for telehealth use and non-use, recency of telehealth utilization, and patient-reported experience and satisfaction with telehealth services.
Results: Approximately one-third of adults reported ever using telehealth. In multivariable analysis, women had higher odds of telehealth use than men (aOR = 2.02, 95% CI: 1.38–2.96; p = 0.0003). Adults aged 35–49 were more likely to use telehealth compared with those aged 18–34 (aOR = 1.72, 95% CI: 1.05–2.84; p = 0.0328). Being uninsured was associated with lower odds of telehealth use (aOR = 0.43, 95% CI: 0.20–0.93; p = 0.0309). Higher education (Bachelor’s degree or above: aOR = 1.58, 95% CI: 0.98–2.54; p = 0.0589) and lack of internet access (aOR = 0.46, 95% CI: 0.21–1.01; p = 0.0542) showed borderline associations with telehealth use. Race and income were not significantly associated with use. Among telehealth users, convenience—limited time for in-person visits (42.7%) and difficulty traveling (29.8%)—was the most frequently reported reason for use. Among non-users, preference for face-to-face care was the dominant barrier (88.4%), followed by limited awareness or difficulty using telehealth technology. Primary care providers were the most common source of telehealth information (47.3%). User experience was highly favorable: over 90% of users reported satisfaction, trust in privacy and security, and confidence that their concerns were addressed, and more than 80% indicated intention to continue using telehealth.
Discussion: These Results: describe a baseline of substantial yet uneven telehealth use in Mississippi. Variation linked to gender, age, and insurance status and signals for education and internet access—frames disparities relevant to appropriate access to care. Strong user experience and stated intention to continue can inform future tracking of whether gaps narrow over time.
Enhancing Neonatal Care Closer to Home: Impact of Telehealth Consults on Triage and Transports in a Regional Network
Michelle Mejia MD, Rachel Umoren MBBCh, MS, Megan Gray MD, Mark Lo MD, MS
Seattle Children's Hospital
Primary Email:michelle.mejia@seattlechildrens.org
Background: Telehealth is an essential strategy for improving access to high-quality neonatal care in semi-urban and rural NICUs, where on-site neonatology coverage is often limited. Prior studies demonstrate its value in supporting transport triage and enhancing pre-transport stabilization by enabling real-time assessment and collaboration across sites. The objectgive of this study was to evaluate whether telehealth consults influence the frequency and variability of neonatal transports across a regional NICU network. Secondarily, we assessed whether telehealth affected the likelihood of infants remaining at their birth hospital or being transferred to a community Level III NICU versus a tertiary Level IV NICU.
Methods: Seattle Children’s Level IV NICU implemented a telehealth service to support regional Level II NICUs, including real-time consults at the point of transport center contact to enhance shared decision-making, provide procedural guidance, and ensure continuity of care. Transfer-center encounters from Q4 2020 to Q2 2025 were analyzed using statistical process control (SPC). XmR charts assessed changes in transport volume and variability, and p-charts evaluated quarterly proportions of transfers from Level II to Level III versus Level IV NICUs. Encounters were stratified by the presence or absence of a telehealth consult. Chi-square tests and odds ratios were used for comparative analyses.
Results: We analyzed 313 transfer-center encounters from three Level II NICUs. Mean quarterly transports remained stable before and after telehealth implementation (13.8 vs. 15.1; NS), indicating that the intervention did not increase overall transfer volume. Quarter-to-quarter variability increased (mR centerline 3.3 to 5.5), demonstrating a shift toward more deliberate, case-specific triage rather than routine transfer. Post-implementation, the proportion of infants transferred to regional Level III NICUs increased (CL 37.6%, UCL 71.9%; NS), while Level IV transfers decreased (CL 55.8%, LCL 20.6%; NS), reflecting improved alignment of patient acuity with receiving-facility capability. Patients engaged in a telehealth consult were more likely to remain at their birth hospital or transfer to a Level III NICU (31.9%) than those without a consult (11.9%), exceeding the pre-implementation average of 19.6%. Telehealth consults were associated with higher odds of remaining local (OR 3.2, 95% CI 1.03–9.96; p=0.035) and regional Level III transfer (OR 1.88, 95% CI 1.16–3.05; p=0.01), supporting a sustained improvement in refining neonatal transport.
Discussion: Telehealth implementation did not change overall transport volume but altered the pattern of decision-making. Increased quarter-to-quarter variability reflects a shift from routine transfer to individualized, case-specific triage supported by real-time consultation. Post-implementation, more infants were directed to Level III NICUs and fewer to the Level IV NICU, indicating improved alignment of patient acuity with receiving-facility capability. Importantly, increased local retention was driven by active engagement in telehealth consults rather than the presence of the service alone. With a consult, local retention or Level III transfer occurred more frequently (31.9% vs. 11.9% without consults) and exceeded pre-implementation levels (19.6%). Consults were also associated with higher odds of remaining at the birth hospital (OR 3.2, 95% CI 1.03–9.96) and regional Level III transfer (OR 1.88, 95% CI 1.16–3.05). Overall, telehealth supported more deliberate triage, appropriate local care, and optimized regional resource use.
A Mixed-Methods: Study of U.S. Children's Hospitals' Preparedness to use Telehealth in Disaster and Surge Response
Rachel Umoren MBBCh, MS,1 Shireen Atabaki MD, MPH,2 Lauren Robinson MD,3 Tehnaz Boyle MD, PhD,4 John Chuo MD, MSBI, IA,5 Michelle Mejia MD,1 Alejandro Lopez-Magallon MD,2 Marie Lozon MD,8 Shivaprasad Bhuvanendran DEng,2 Mark Batshaw MD2
1Seattle Children's Hospital 2Children's National Hospital 3University of Alabama at Birmingham 4Boston Medical Center 5University of Pennsylvania Perelman School of Medicine and 6University of Michigan
Primary Email:rumoren@uw.edu
Background: Telehealth has the potential to improve emergency care in disasters through remote expert teleconsultation and education. However, there are still gaps in the utilization of telehealth for pediatric patients. The Pediatric Pandemic Network (PPN) is a national collaborative initiative aimed at enhancing pediatric care during emergencies by empowering children's hospitals and health care systems, specifically as it relates to telehealth, to increase the capacity and capability of telehealth to address children’s unique needs during a disaster. The scope of this work involves supporting hub sites to assess telehealth capacities, expand telehealth capabilities, leveraging current telehealth programs to develop disaster responses. Limited data exists regarding the readiness of health care facilities that care for children to utilize telehealth capabilities during disasters for expert consultation and education to support clinicians and patients in community hospital settings.
Methods: The objective of this study was to evaluate pediatric telehealth capabilities for disaster and surge response in children's hospitals participating in the Pediatric Pandemic Network (PPN). Cross-sectional surveys and interviews on children’s hospitals’ telehealth capabilities were conducted from 2023-2025. The 15-item web-based survey [Qualtrics] developed by the PPN Telehealth working group was completed by telehealth operations leaders. Survey items focused on pediatric telehealth availability, cross-state use, system integration, surge planning, and key barriers to effective use. Following IRB approval, the survey was distributed electronically to all participating facilities. Descriptive statistics were used to summarize survey Results:. Key informant semi-structured interviews were conducted with participating hospitals to identify supports and barriers to telehealth. Thematic analysis of the transcripts organized using the World Health Organization (WHO) Six Health System Building Blocks of service delivery, health workforce, health information systems, access to essential technologies, health financing, leadership and governance, identified themes around best practices and barriers to pediatric telehealth in the context of disasters.
Results: All 14 PPN children’s hospitals completed the survey and qualitative interviews (RR = 100%). Participating facilities were geographically distributed across all 10 HRSA regions, in urban areas (13, 93%), academic pediatric or free-standing children’s hospitals (10, 79%), with a range of bed capacities. While a majority of facilities offered telehealth consultations to community health care facilities outside of their health care system (12, 86%); and routinely served pediatric patients at critical access (10, 71%) and rural health facilities (11, 79%); fewer had experience with remote patient screening sites (6, 43%); schools, daycare centers or other pediatric, non-medical facilities (5, 36%); emergency medical services (4, 29%); or temporary field hospitals (1, 7%). While it was common for the telehealth systems to be integrated with patient appointment, patient portal, electronic medical records and medical billing software (12, 86%), fewer reported integration of telehealth with their emergency operations center (3, 21%). Analysis of interview data revealed substantial maturity in pediatric telehealth service delivery and workforce capacity across hubs. Participants consistently described telehealth as an integral component of routine clinical operations. However, gaps persist in infrastructure resilience, financing sustainability, interoperability, and governance—particularly outside periods of declared emergency.
Discussion: Children's hospitals must be able to accommodate disaster and surge needs, within hours, across multiple health specialties for a range of pediatric populations in urban and rural settings, often across state lines. Telehealth can play a pivotal role in supporting this care. Our effort to determine PPN children's hospitals' current readiness to provide this support has identified many strengths and opportunities which may have applications to other health facilities that serve children nationally. Integration of pediatric telehealth into hospital infrastructure and emergency operations centers will support infrastructure resilience and enhance children’s hospital’s preparedness to leverage telehealth in disasters and surge events, as will guidance on best practices, and the development of policies around financing sustainability, interoperability and governance.
Telehealth Consent Explanations by Large Language Model-Powered Chatbot: A Text Quality Analysis
Hiral Soni PhD, MS,1 Hattie Wilczewski BS,1 Julia Ivanova PhD, MA,1 Triton Ong PhD,1 Akanksha Bagam,2 Brandon Welch PhD, MS1
1Doxy.me Inc. and 2Jack C Hays High School
Primary Email:hiral.soni@doxy.me
Background: Informed consent is critical for clinical care and research. The conventional approaches such as pen and paper or online forms are often long and verbose, commonly filled with medical and legal jargon, leaving patients with limited opportunities for questions about aspects of the form they may not understand. Large language models (LLMs) have shown potential in generating and summarizing complex consent forms. We are developing a consent assistant (CA) to explain consent forms to patients in plain language, ensure consent comprehension, and facilitate the signing process using targeted prompts with OpenAI GPT-4-0613 model, OpenAI Chat Completion API, and nutrient.io PDF SDK. Research suggests the need for evaluation of generic LLM-generated text quality as LLMs can provide incorrect, non-factual information. Poorly worded, inconsistent, or incorrect information may lead to patient confusion, misinterpretation, or potential ethical or legal concerns with the consent process. The goal of the study is to assess the text quality of CA generated consent form explanations including accuracy, reliability, validity, consistency, bias, and readability.
Methods: This quality improvement study evaluated the text quality of assistant-generated explanations using a Telehealth Appointment Consent Form. Clinicians with experience obtaining telehealth consent participated in remote, moderated sessions with screen recording and think-aloud feedback. Pre-study questionnaires collected demographics, professional experience, and AI use. Clinicians generated and evaluated explanations using predefined measures rated on five-point Likert scale including: accuracy (correct retention of consent information), reliability (consistency across repeated generations of the same statement), information validity (alignment with the intent and key messages of the original consent), consistency (formatting, length, tone, and writing errors), and bias (presence of linguistic bias). Readability of original consent text and generated explanations was assessed using Flesch Reading Ease, Flesch-Kincaid Grade Level, and Simple Measure of Gobbledygook (SMOG) indices. Post-study surveys assessed overall experience and likelihood to recommend. Quantitative data were analyzed using descriptive statistics and percentage agreement for quality measures. Qualitative data from think-aloud sessions and open-ended responses were analyzed using thematic analysis. This study was designated Non-Human Subjects Research by the Medical University of South Carolina IRB.
Results: Of eight clinicians, most were mental health providers (87.5%), reported current use of AI in practice (62.5%) and moderate-to-high willingness to use AI in health care.
Accuracy: CA explanations were rated highly accurate overall (M = 4.76 ± 0.43/5). Percent agreement ranged from 75–100% (mean 84.72%). Qualitative feedback noted clear, concise explanations, with suggestions to reduce repetition and adjust wording that could be confusing or overly casual.
Reliability: Reliability ratings were high (M = 4.93 ± 0.20/5). Mean percent agreement was 93.06%. Participants described explanations as consistent and stable across repeated generations, with minor recommendations to vary word choice and improve transparency language.
Validity, Consistency, and Bias: Validity and consistency were both rated 4.63 ± 0.52. Average bias rating was 0.25 ± 0.46, indicating minimal perceived linguistic bias. Overall quality was rated as Excellent or Good by all participants. Net Promoter Score was 75.
Readability: CA-generated explanations were significantly more readable than the original consent form across all indices (FRE, FKGL, SMOG; p < .001), corresponding to approximately sixth–eighth grade reading levels versus college-level readability for the original form.
Qualitative feedback highlighted ease of use, clarity, and patient empowerment, with recommendations to improve clinical nuance, reduce repetition, and clarify limits of confidentiality.
Discussion: This quality improvement study evaluated the text quality of consent explanations generated by a consent assistant (CA). Clinicians rated the CA explanations highly across quality measures and expressed strong willingness to use the tool in practice, indicating potential to enhance telehealth consent workflows. The CA produced accurate and reliable explanations that preserved the intent of the original consent text and remained consistent across repeated prompts. Slightly lower scores in certain sections reflected clinician preferences for nuanced and affirming language, underscoring the importance of careful wording. CA explanations were written at sixth–eighth grade level compared to college-level readability of the original consent form, which may improve patient comprehension and support informed decision-making. Although minor wording issues lacking clinical nuance were identified, no inaccurate information was observed. Limitations include a small clinician sample and evaluation of a single consent form. Overall, LLM-powered consent assistants show promise in improving the clarity and accessibility of telehealth informed consent.
Bidirectional Tele-Mentoring via Project ECHO to Strengthen Rural Internal Medicine Education
Edwin Paul MPH, Christian Bell BS, Yaizeth Gurrola-Mares MS, James Nichols BS, Timothy Brooks BS, Milcah Poothakary BA, Mathew Geroge MS, Lekha George MD, Ariel Santos MD, MPH, FACS, FCCM
Texas Tech University Health Sciences Center School of Medicine
Primary Email:Edwin.paul@ttuhsc.edu
Background: Rural West Texas continues to face a significant shortage of Internal Medicine (IM) physicians and limited access to specialty-driven continuing medical education. Projections by Texas Department of Health and Human Services indicate that demand for primary care specialties, especially general IM, will continue to outpace supply in West Texas through 2030, exacerbating access challenges. To address this shortage gap, Project ECHO utilizes the hub-and-spoke model to participate in a tele-mentoring program connecting University Medical Centers (academics) with primary care providers (PCP) through a monthly case-based virtual session series focused on selected cases related to metabolic health disparities. We implemented a student–specialist co-teaching structure, a novel teaching model within the Project ECHO system, during IM grand rounds to expand educational access while enhancing medical student training in telehealth practice. This study evaluates the feasibility, educational value, and bidirectional learning dynamics of integrating medical students into a tele-mentoring network serving rural clinicians.
Methods: During the Project ECHO sessions, medical students collaborated with IM specialists to present a de-identified clinical case, which was followed by faculty-led didactics and an interactive Discussion: in which students assisted with provider questions and synthesis of key take-home points, all of which was broadcast to PCPs across West Texas through the Project ECHO platform. A mixed-methods evaluation was conducted to evaluate the study. Medical student outcomes were assessed using a pre/post-participation survey measuring confidence across domains related to virtual case presentation. Responses were recorded on a 5-point Likert scale, and pre- and post-participation scores were compared using a one-tailed Wilcoxon signed-rank test. Clinician outcomes were evaluated through the use of post-session cross-sectional surveys. Surveys were utilized to assess clinician perceptions of engagement, clinical relevance, and overall educational value of the student-specialist teaching format. Provider responses were analyzed using descriptive Statistics, including mean Likert scores and distribution of agreement. Additional qualitative data were collected from student reflection logs, and qualitative analysis guided by the Consolidated Framework for Implementation Research (CFIR) was used to identify themes related to feasibility, engagement, and bidirectional learning within the tele-mentoring model.
Results: Medical student pre- and post-participation survey Results: demonstrated substantial improvement across six confidence and skills domains. Pre-session mean scores ranged from 2.1 to 2.9, with the lowest confidence in facilitating question-and-answer Discussion:s and the highest in clinical synthesis. Post-session mean scores increased to 4.4–5.0, with the highest confidence reported for telehealth communication. All domains showed positive mean changes, with the greatest improvement in preparedness for future roles (+2.5), followed by clinical synthesis (+2.0). One-tailed Wilcoxon signed-rank testing indicated significant increases across all domains (p < 0.01). The post-session survey Results: for providers were also assessed. On average, providers indicated a high levels of satisfaction scores ranged from 4.25 to 4.75 on a five-point scale. The three areas where providers had the highest level of agreement were: clinical application of case to rural health, the student-specialist model, and delivery of practical strategies for rural settings (4.75 mean score with 100% of respondents either agreeing or strongly agreeing with these three statements). Qualitative analysis of the student reflection logs utilized CFIR indicated that they were more comfortable medical presenting cases, synthesizing clinical facts, and had a better understanding of the challenges associated with practicing in rural communities.
Discussion: This evaluation highlights a mechanism to enhance educational flow and engagement in virtual learning environments. Actively involving medical students in case presentation and Discussion: facilitated structured, learner-centered sessions while maintaining high educational value for rural clinicians. Student participation supported clear case framing and continuity between case-based learning and faculty-led instruction, contributing to interactive dialogue and shared problem-solving. Improvements in student confidence across telehealth-related domains suggest that repeated, guided participation in ECHO sessions may strengthen early telemedicine competencies. In addition, provider feedback supports that student involvement complemented the tele-mentoring learning experience rather than a limitation. Incorporating trainees into an already established tele-mentoring infrastructure allows for reciprocal learning opportunities, sustains workforce development for scalability, and aligns with health system paradigms toward connected health and sustainability of telemedicine delivery models to rural areas.
Remote Patient Monitoring: Using Implementation Science to Promote Adoption and Sustainability in Pregnancy Care
Mary Allison PhD, MPH, Hannah McCoy MPH, Sylvia Wise, Cari Bogulski PhD
University of Arkansas for Medical Sciences
Primary Email:kallison@uams.edu
Background: Health conditions like hypertension and diabetes can increase risk during pregnancy and necessitate additional monitoring by a health care provider. Digital technologies, like remote patient monitoring (RPM), can assist with this monitoring and reduce the need for frequent in-person clinic visits. RPM uses digital devices to capture vital signs and directly transmit readings to health care providers in real-time, enabling immediate assessment and management of certain health conditions. With improved uptake and efficiency, RPM has the potential to address gaps in health care access for rural and underserved populations, including those with high-risk pregnancies. Implementation Science offers tools and methods to study the uptake of evidence-based practices into routine care. This study aimed to use Implementation Science frameworks and approaches to (1) assess facilitators and barriers of RPM implementation in pregnancy care and (2) identify optimized implementation strategies to support uptake and sustained use of RPM.
Methods: Informed by the Consolidated Framework for Implementation Research (CFIR), we conducted qualitative interviews with 16 key obstetric stakeholders, including obstetricians, nurses, researchers, IT staff, and call center staff. Using a rapid analysis approach, we analyzed interviewer notes and summarized reported facilitators and barriers to RPM implementation by CFIR domains. Then, using an Evidence-based Quality Improvement (EBQI) approach, we formed a workgroup of RPM stakeholders and implementation scientists and conducted a series of group Discussion:s to review and prioritize the facilitators and barriers identified in Aim 1 interviews, map these determinants to implementation strategies using the CFIR-ERIC Implementation Strategy Matching Tool, and prioritize and describe recommended strategies to optimize RPM adoption, implementation, and sustained use in pregnancy care.
Results: Aim 1 revealed facilitators and barriers across the CFIR domains. Inner setting barriers included clinic workflow issues, like using a data platform separate from the EHR, while facilitators included implementation support from RPM project teams, IT, and a 24/7 nurse call center. Outer setting barriers included reimbursement challenges, and facilitators included motivation to reduce rural patients’ travel burden. Innovation characteristic facilitators included using cellular-enabled devices to address broadband access inequity. Facilitators related to individuals included providers’ familiarity with digital technology and virtual communication. The Aim 2 stakeholder workgroup identified implementation strategies needed to address key barriers and leverage facilitators. These strategies included: organizing interdisciplinary implementation team meetings to optimize workflow and facilitate logistical decision-making; developing resource sharing agreements or contracting with nurse call centers; promoting adaptability of data aggregator platforms and monitoring devices; tailoring implementation strategies to account for patient needs (e.g., broadband and phone access); staging implementation scale-up; purposely reexamining the implementation through real-time continuous quality improvement; and providing ongoing consultation in the sustainment phase.
Discussion: Findings from this study informs optimization of future RPM programs in pregnancy care by addressing known barriers to uptake and sustainment. While prior implementation research on remote monitoring in pregnancy care has focused on disease-specific implementation barriers, this study identifies context-specific barriers to RPM for disease management broadly in pregnancy care. Future research should assess the effectiveness of implementation strategies identified in this study.
A Care Model to Support Caregivers of Children with Medical Complexity in Using Telehealth
Josh Brown PhD, Savithri Nageswaran MD, Doug Easterling, Cara Janusz, Sabina Gesell, Erica Hale
Atrium Health Wake Forest Baptist
Primary Email:josh.brown@advocatehealth.org
Background: Children with medical complexity (CMC) require frequent outpatient care from multiple providers, yet in-person visits pose significant logistical challenges for parents/caregivers. Telehealth offers a promising alternative, but models to support caregivers in effectively using telehealth remain underdeveloped. As part of an ongoing comparative effectiveness trial, we are testing a three-component intervention to facilitate telehealth and improve care coordination for CMC in primary care. One component, Caregiver Telehealth Support (CTS), aims to identify and proactively address barriers caregivers face when engaging in telehealth. This abstract describes the (1) CTS model and (2) early Results: regarding the extent of caregiver telehealth-related needs.
Methods: In this ongoing trial, 191 children have been enrolled to date in four study blocks. The CTS model uses dedicated personnel (“Telesupporters”) to address caregivers’ telehealth needs remotely using standardized procedures (“CTS curriculum”). The Telesupport team consists of a 0.5 FTE Telesupporter and 0.23 FTE Telesupport Manager. Telesupporters provided structured support around device issues, internet issues, accessing the patient EHR portal, telehealth visit login, test telehealth visits, scheduling, and other free-texted needs. The model’s two steps are: (1) systematic assessment of caregiver/patient needs related to telehealth access and use, and (2) provision of assistance to facilitate successful telehealth engagement. Assessment occurs via caregivers completing study-specific surveys that evaluate known telehealth barriers (e.g., technology access, connectivity, scheduling). Telesupporters then reviewed caregiver-specific dashboards in a REDCap database that showed the caregiver-reported barriers and provided needed Telesupport to caregivers over the phone. During those calls, Telesupporters worked through identified barriers and other issues that emerged. A bilingual Telesupporter supported Spanish-speaking caregivers.
Results: Preliminary process/implementation data from 101 caregivers who were enrolled in the first two study blocks and completed their needs assessment surveys were examined. Among those, 49 (48.5%) reported having at least one initial telehealth-related support need. Of those with at least one identified telehealth-related need, the average number of needs was 1.49 (SD = 0.85). However, when telehealth-related support needs were examined by the caregiver’s primary language (English vs. Spanish), Spanish-speaking caregivers were more likely to report having at least one telehealth-related support need than English-speaking caregivers, 93.8% (15/16) vs. 40% (34/85), respectively. Further, Spanish-speaking caregivers reported having a greater number of initial needs (n = 16; M = 2.2; SD = 1.2) compared to English-speaking caregivers (n = 85; M = 1.2; SD = 0.4). The table below shows the frequency with which each barrier/need was reported based on caregiver language.
Language
N
Device Support
Internet Support
Patient Portal Support
Login Support
Test Visit Support
Scheduling Support
Other Support
English
85
1 (1.18%)
1 (1.18%)
7 (8.24%)
28 (32.94%)
0 (0.00%)
3 (3.53%)
0 (0.00%)
Spanish
16
4 (25.00%)
3 (18.75%)
9 (56.25%)
12 (75.00%)
2 (12.50%)
3 (18.75%)
0 (0.00%)
Discussion: A structured Caregiver Telehealth Support (CTS) model for caregivers of CMC can be designed and successfully implemented within a clinical trial. Though we do not yet have complete data on caregiver engagement with or outcomes of the Telesupport provided, telehealth-related needs of caregivers varied widely, underscoring the importance of conducting individualized assessments and providing individualized support – even after increased national use during the COVID-19 pandemic. Bilingual Telesupport also emerged as a critical facilitator of equitable access, particularly given the higher barriers/needs endorsed by Spanish-speaking caregivers. Future work should examine sustainability and scalability of this model beyond grant-funded settings.
Providing Telehealth Support to Pediatric Primary Care Providers
Josh Brown PhD, Savithri Nageswaran MD, Doug Easterling, Cara Janusz, Sabina Gesell, Erica Hale
Atrium Health Wake Forest Baptist
Primary Email:josh.brown@advocatehealth.org
Background: Children with medical complexity (CMC) need easily accessible primary care to facilitate coordination of their highly specialized care needs, yet primary care providers (PCPs) do not consistently use telehealth with this population, which may prove to be a barrier to access. Existing models offering structured, individualized telehealth support to PCPs and their practices are limited. As part of an ongoing comparative effectiveness trial testing a three-component intervention to facilitate telehealth for CMC, we developed a Primary Care Provider Telehealth Support (PTS) model. PTS is designed to identify and address PCP and practice-specific barriers to utilizing telehealth. This abstract describes (1) the PTS model and (2) early findings regarding the extent and variability of PCP telehealth support needs among PCPs and their practices.
Methods: Children and their PCPs are enrolled in blocks across diverse primary care practices. The PTS model uses dedicated Telesupporters to provide structured support based on a standardized PTS curriculum. The Telesupport team consists of a 0.5 FTE Telesupporter and 0.23 FTE Telesupport Manager. Telesupporters provided structured support around a number of known telehealth barriers (e.g., device needs, accessory needs, etc.). The model’s two steps are: (1) systematic assessment of telehealth needs of PCPs and needs of the practice, and (2) provision of needed assistance to PCPs and practices to facilitate successful telehealth utilization. The assessment consists of three parts: (1a) practice managers complete a practice-level assessment, (1b) PCPs complete surveys on their attitudes and behaviors, and (1c) a practice needs-assessment site visit where findings are reviewed, tested, and refined. Practices receive support during a post-needs assessment visit and are assigned a Telesupporter who provides ongoing telehealth assistance as needed. PCP support is delivered through individualized PCP-specific webpages built in REDCap that provide tailored guidance (e.g., tip sheets, videos) and a link to request additional Telesupport.
Results: Implementation data from the first two blocks included 117 children and 59 PCPs representing 9 practices. Leaders from 8 practices (88.9%) completed practice-level needs assessments, and 43 PCPs (72.9%) completed baseline needs assessment surveys. Practice leaders most commonly reported that their PCPs lacked private space for telehealth (50%), needed scheduling support (50%), and needed resource support (37.5%). PCPs most frequently reported not knowing how to incorporate interpreter services into telehealth visits (67.4%), followed by needing instructions on how to conduct telehealth visits (30.2%), and lack of resource/equipment (27.9%). Interviews revealed substantial variability in needs and engagement by practice and by provider, with additional barriers routinely emerging during follow-up Discussion:s with practices and PCPs. Table 1 summarizes practice and PCP needs.
Telehealth Support Needs Reported by Practice Leaders and PCPs
Device Support
Accessory Support
Space Support
Internet Support
Conduct Visits Support
Platform Support
Interpreter Support
Billing Support
Scheduling Support
Resident Provider Support
Resources Support
Other Support
Practices (n=8)
1 (12.5%)
1 (12.5%)
4 (50%)
2 (25%)
2 (25%)
2 (25%)
N/A (included in Login Support)
1 (12.5%)
4 (50%)
N/A
3 (37.5%)
2 (25%)
PCPs (n=43)
4 (9.3%)
10 (23.3%)
9 (20.9%)
1 (2.3%)
13 (30.2%)
5 (11.6%)
29 (67.4%)
11 (25.6%)
5 (11.6%)
6 (14%)
12 (27.9%)
2 (4.7%)
Discussion: A structured PTS model supporting PCP telehealth use for CMC can be implemented across diverse primary care settings. Early findings show wide variation in PCP needs, emphasizing the importance of individualized assessment and proactive outreach. Often, PCP and practice needs emerged during continued engagement, suggesting that routine follow-up may be essential. Future work will assess the role that PCP preferences towards telehealth play in their willingness to utilize telehealth, their support needs, and the effect of Telesupport on their telehealth adoption and equitable care access for CMC. Long-term sustainability of PTS outside grant-funded contexts will also need to be examined.
Advancing Telehealth Concussion Assessment Through Novel Virtual Technology Development
Jennifer Reneker PT, PhD,1 William Pruett PhD, Ryan Babl PT2, Michael Brown PT, DPT, PhD, SCS,4 Jacob Daniels PT, DPT, EdD,3 William Pannell PT, DPT, SCS, UDN-C,3 Heather Shirley PhD4
1Northeast Ohio Medical University, 2Auburn University, 3University of Mississippi Medical Center, and 4Ole Miss
Primary Email:jreneker@neomed.edu
Background: Concussion commonly occurs in sports and military venues and is difficult to diagnose and manage. Clinical (non-instrumented) tests continue to be relied upon as standard practice to identify impairments after a concussion and, together with patient self-reporting, allow a qualified practitioner to arrive at a diagnosis. Clinicians using these tests are only able to detect what they can perceive (i.e., gross abnormality); or what patients report as provocative of familiar symptoms, however, impairments associated with concussion can be subtle and elusive to the naked eye and symptoms are often under-reported. Diagnosis becomes much more difficult when done through telehealth. A medical device is needed to perform an assessment for concussion and identify functional deficits in-person or through remote technology. This report presents the developmental methodology, including user experience and human factors Results:, for a new virtual reality (VR)-based technology.
Methods: During software development, the unique capabilities of VR were harnessed to objectively assess oculomotor control, visual perception, positional awareness, and the vestibular system. These tests were re-imagined from traditional clinical tests, informed by research evidence, and translated by a multi-disciplinary team into the virtual environment. This included a clinical expert, a data scientist, a computer engineer, and a software developer. An iterative process was used to meet the technical and clinical aspects desired by the collaborative team. Data collection with human participants occurred between 2020 and 2024, amassing 1008 participants between the ages of 18 and 40 years. A written log was implemented with 815 participants, to collect data related to human factors, including each participant’s interaction and difficulty with the test completion. Symptom provocation on a 0 – 10 scale for the user’s experience of headache, dizziness, nausea, and fogginess were collected at the beginning of the test set and after each individual test, yielding nine measures of symptom report. The initial software was modified, informed by human factors and user experience data, including symptom report and need for examiner assistance, leading to a modified second version.
Results: Of participants enrolled, 49.2% were female (n=496) and 25% (n=252) were non-White. The mean age of the participants was 21.9 years of age (SD 4 years; range 18 – 40 years). Symptom provocation during the VR tests demonstrated less than 5% had a > 2-point increase in headache, nausea, and mental fogginess across; 9.2% had > 2-point increase in dizziness. This is in line with reports from similar clinical tests, demonstrating that the VR environment does not pose an additional risk. Regarding human factors, for the first version of the software, participants required additional instructions at the beginning of the tests (i.e., additional to the software-generated audio and visual instructions) from the examiner for the symptom report 49.4% of the time (n=211); this decreased to close to 0% (n=2) with the second version of the software. The most difficult tests for the participants to understand, in both versions of the software, were tests of pro- and anti-saccades, peripheral vision, and cervical neuromotor control, which continued to require examiner support in up to 11.1% of cases.
Discussion: Clinical tests of functional neurology were translated into a virtual environment and multidimensional sensor-based data was collected on a sample of participants, who did not experience unexpected symptom provocation during test completion. This developmental work was completed with the goal of addressing technological gaps in concussion management, including both in-person and remote examination and identification of specific neurological deficits indicative of a concussion. The eventual outcome is the enablement of targeted treatment strategies and the provision of decision support for optimal medical management. The approach described here regarding the translation of real-world clinical tests into the VR environment, towards the development of a medical device, may be useful to many other health care disciplines and fields, especially with consideration of telehealth patient management. Pending Results: of the machine learning classification (which remains ongoing), this device may prove useful in decision support for concussion diagnostics and determination of recovery.
A Systematic Review of Governance Frameworks for Secure Global Telehealth
Suguna Kotte, Saif Khairat PhD, MPH, FACMI
University of North Carolina Chapel Hill
Primary Email:sugunak@unc.edu
Background: The rapid global adoption of telehealth highlights the need for secure, interoperable repositories capable of multi-national data exchange without compromising regulatory compliance. Despite growing deployment, few systems balance encryption, semantic interoperability, and research readiness. Emerging technologies including blockchain, AES/RSA encryption, and ontology-based models offer potential, but their scalability and regulatory alignment across countries remain largely untested. Understanding these patterns is critical to inform repositories that support cross-border research, real-time monitoring, and AI-driven analytics. Furthermore, a central tension persists between the clinical need for large-scale data analytics and the strict requirements for patient privacy. This systematic review addresses the urgent need to align global interoperability standards with robust governance frameworks to enable secure, scalable, and equitable multi-national health data exchange.
Methods: This study employed a systematic review approach following PRISMA guidelines. A comprehensive search was conducted across PubMed, Scopus, and Embase databases, initially identifying 37 potentially relevant records. After a rigorous screening process based on title, abstract, and full-text relevance to multi-national telehealth governance and interoperability, 8 articles were selected for detailed evaluation. Due to full-text availability constraints for one record, 7 high-impact articles published between 2022 and 2025 were finalized for synthesis. The methodology involved a thematic analysis of technical standards, such as Health Level Seven International (HL7) FHIR, and data management philosophies like the Findable, Accessible, Interoperable, and Reusable (FAIR) principles. A multi-layered framework was derived by mapping technical requirements against the legal and social interoperability needs identified across the finalized literature.
Results: Three critical pillars for scalable multi-national exchange were identified. First, HL7 FHIR is the dominant technical standard, cited as the essential enabler for modular, real-time data integration and Artificial Intelligence (AI) readiness. Second, “Semantic Harmonization” remains a major barrier; while data formats are standard, clinical meaning often requires localized terminology mapping using Systematized Nomenclature of Medicine Clinical Terms (SNOMED CT). Third, a profound governance maturity gap exists; in regions like Jordan and Palestine, technical infrastructure is advanced, while legislative readiness remains initial. Quantitative findings from Uganda highlight that while District Health Information Software 2 (DHIS2) reporting coverage reached 90%, institutional readiness for ethical data reuse remains low (∼10%). Effective enablers identified include stakeholder co-design and privacy-preserving techniques, such as blockchain-enabled audit trails and Federated Learning (FL), which mitigate the tension between data utility and confidentiality.
Discussion: For connected health to achieve global scale, the strategic focus must shift from a technology-centric to a governance-first approach. This review demonstrates that while technical barriers are being lowered by standards like FHIR, the disparity in policy maturity remains the primary inhibitor of cross-border exchange. Scalability requires a foundation of trust built on transparent data rights, harmonized international regulations, and patient-centered Dynamic Consent (DC) models. Implementation of the proposed multi-layered framework offers a roadmap to bridge these gaps, ensuring that sensitive information can securely cross borders without compromising the Right to Privacy. Future efforts should prioritize longitudinal investments in digital capacity and the alignment of national policies with international standards like the FAIR principles to foster an equitable global health ecosystem. Achieving this balance is essential for realizing the full potential of global health surveillance and Precision Medicine (PM).