
Abstract
Background:
Access to high-quality mental health (MH) care in rural communities remains a persistent challenge. In 2019, the Veterans Health Administration (VA) developed 18 regional Clinical Resource Hubs (CRH) to increase Veteran access to clinical services, mainly through telemedicine and telemental health. This study evaluates trends in CRH MH services among Veterans residing in rural areas for the first 5 years of the program.
Methods:
This retrospective cohort study utilized CRH MH encounter data (i.e., clinical visits or patient contacts) from the VA Corporate Data Warehouse for the first 5 years of the CRH program (Fiscal years [FY] 2020–2024) with a focus on rural and highly rural Veterans. Veteran demographics and clinic characteristics were collected, and measures were aggregated for each FY. Descriptive statistics were calculated using independent t-tests for continuous variables and Fisher’s exact or Chi-square tests for categorical variables.
Results:
Using primarily telemental health services, CRH MH teams completed 627,436 encounters, with 81.9% delivered via telemedicine among Veterans residing in rural or highly rural areas. Care delivery shifted substantially over 5 years, with video visits to a patient’s homes increasing from 9.2% to 64.3% while clinic-based video visits declined from 77.5% to 7.1%. Racial and ethnic diversity increased steadily over time, especially among Black and Hispanic Veterans. Between FY20 and FY24, encounters for depressive disorders decreased slightly while encounters for anxiety disorders, posttraumatic stress disorder, and attention-deficit/hyperactivity disorder diagnoses increased.
Conclusions:
Veterans in rural and highly rural communities often struggle to access MH care, and the CRH MH program was designed to utilize primarily telemental health to fill in these gaps to improve Veteran access. During the first 5 years of the CRH MH program, the amount of MH care provided to rural Veterans more than doubled with expanded site participation and an increasingly diverse patient population over time.
Introduction
Veterans residing in rural areas have higher rates of physical health conditions, comorbidity, and mental health (MH) disorders, in addition to less utilization of MH care compared with Veterans living in urban areas.1,2 Further, suicide rates among rural Veterans are 20–22% higher than those among Veterans living in urban areas. 3 Although rural and urban Veterans are similar in their prevalence of MH comorbid conditions, rural Veterans are substantially less likely to receive MH services compared with their urban counterparts.4,5 Previously identified factors contributing to this disparity include long distances to medical centers, staff shortages, insufficient MH expertise among non-Veterans Affairs (VA) clinicians, and cultural factors such as MH stigma and an emphasis on self-reliance.6,7 The lower likelihood of rural Veterans receiving care may also be due to the digital divide, including limited or costly internet access, underdeveloped infrastructure, and issues related to digital literacy and trust. Older adults, who make up a growing proportion of rural Veterans, may face additional obstacles including less familiarity with technology, lower confidence in using digital tools, and heightened concerns about privacy or trust in virtual care.8–11
To address persistent access barriers to high-quality MH care for rural Veterans, including challenges related to the digital divide, the VA has prioritized the development and implementation of telehealth programs designed to expand access while accommodating varying levels of technology access and literacy. VA’s national network is divided into 18 administrative regions called Veterans Integrated Service Networks (VISNs). The Maintaining Internal Systems and Strengthening Integrated Outside Networks (MISSION) Act of 2018 included support for the creation of the VA Clinical Resource Hubs (CRHs) to develop regional telehealth services.12,13 CRHs are VISN-level resources that primarily use approved VA telehealth technologies to provide primary care, MH, surgical, rehabilitation and extended care, and specialty care services to Veterans in areas experiencing gaps in access to care. Importantly, CRH-supported care is delivered through multiple modalities, including telephone-based services, video visits, and in-person support, and is complemented by VA initiatives that provide devices, internet access, and technical assistance, helping to mitigate barriers related to the digital divide.8–11,13 Together, these features position CRH as more than a traditional telehealth model, offering a flexible and supported approach to care delivery that directly addresses key barriers associated with the digital divide.
For rural Veterans, telehealth frequently functions as a primary treatment modality, helping offset the lack of health care resources and other barriers to obtaining care.14,15 Multiple studies have reported that telehealth services are comparable to in-person care, demonstrating that telemental health can be effective in making accurate diagnoses and providing effective treatment for common MH disorders.16–19 Moreover, use of TMH has been associated with increased access and utilization among rural Veteran populations.16–19
Previous evaluations of the CRH program found that MH conditions highly prevalent in VA primary care—such as depressive disorders, posttraumatic stress disorder (PTSD), and anxiety disorders—were frequently diagnosed and treated in CRH, demonstrating that telemental health care can be delivered effectively. 20 Additionally, we found that although these services were more frequently provided to Veterans in urban areas, they were also being routinely delivered to Veterans residing in rural and highly rural areas. 20 The current evaluation will describe the predominantly telemental health delivered by CRH MH teams to Veterans residing in rural and highly rural areas over the first 5 years of the CRH program. We will focus on the type of MH care delivered, the Veterans receiving this care, and the modalities of care utilized. Understanding these components will be critical to identify gaps in care delivery, inform ongoing monitoring of access and quality, and address persistent inequalities in MH care among rural Veterans who face distinct risks and structural barriers compared with their urban counterparts.8–11
Methods
This retrospective cohort study utilized CRH MH encounter data from the Corporate Data Warehouse (CDW) for the first 5 years of the CRH program (October 1, 2019–September 30, 2024). Data from the VHA Support Service Center (VSSC) Planning Systems Support Group (PSSG) were used to identify rurality of Veteran residence (derived from Rural-Urban Commuting Area codes), and clinics were considered rural or highly rural if >50% of their patient population had an address in a rural area. 21 The cohort was then limited to clinics considered rural or highly rural. Primary and secondary stop codes were used to determine the modality of each encounter. Stop codes are used to categorize and track different types of clinical encounters and services provided to Veterans (Supplementary Appendix S1). The primary stop code is the main identifier for the service being provided (e.g., primary care, MH), while the secondary stop code provides additional context, including modality of the visit. Using these codes, encounters were categorized as in-person or telehealth encounters. Telehealth encounters included home-based video visits (VVC, Veterans connected with providers from their homes using a VA-approved platform), clinic-based video visits (CVT, Veterans presented to clinic and connected via video with a remote provider), telephone encounters, and secure messaging. Encounter data were aggregated for each month of the study to examine trends among rural/highly rural Veterans, and trends were compared with the VA overall.
Veteran demographics were pulled from the CDW for each fiscal year (FY) of the study, and included age (years), gender (self-identified), race/ethnicity (Non-Hispanic White, Non-Hispanic Black, Hispanic, Asian/Pacific Islander/Native Hawaiian, and Multi-Race/Other), marital status (married or not married), homelessness (yes or no), and priority group. 22 Socioeconomic status was measured using a census tract-based index and categorized into deciles (0–10), with lower values indicating a greater socioeconomic disadvantage. 23 Comorbidity burden was assessed using the Gagne comorbidity score (range of −3 to 25, with scores of 6 or less indicating lower short-term mortality risk. 24 MH diagnosis codes were extracted, and patients were flagged if they had a positive diagnosis of select MH conditions (attention-deficit/hyperactivity disorder [ADHD], alcohol, anxiety disorders (PTSD and anxiety disorder were reviewed separately), bipolar disorder, cognitive disorders (including dementia, depressive disorders, substance use disorder, psychoses, PTSD, and schizophrenia) for each FY (Supplementary Appendix S2).
Clinics were designated as community or hospital affiliated (community-based outpatient clinics [CBOC] or VA medical centers [VAMC]), and clinic covariates were collected including clinic size (count of total unique patients per year), primary care staffing ratio (a measure obtained from the Patient Aligned Care Team Compass Module within the CDW of the clinic-level support staff per primary care clinicians), the MH underserved score (a composite measure of unreservedness in MH that ranks workforce capacity and access at VAMCs, with higher scores indicating greater unmet need), medically underserved area (MUA) scores (federal designation of areas that lack adequate access to primary care), and measures of MH population coverage (Supplementary Appendix S3) and MH staffing (Supplementary Appendix S4, and S5).25,26
All demographic and clinical covariates were aggregated to the facility level for each FY. Descriptive statistics were calculated using independent t-tests for continuous variables and Fisher’s exact or Chi-square tests for categorical variables. The p-values of <0.05 were considered statistically significant. All analyses were completed in SAS EG V8.3. This project met the criteria for quality improvement/nonhuman subject’s research and therefore did not require Institutional Review Board approval or informed consent.
Results
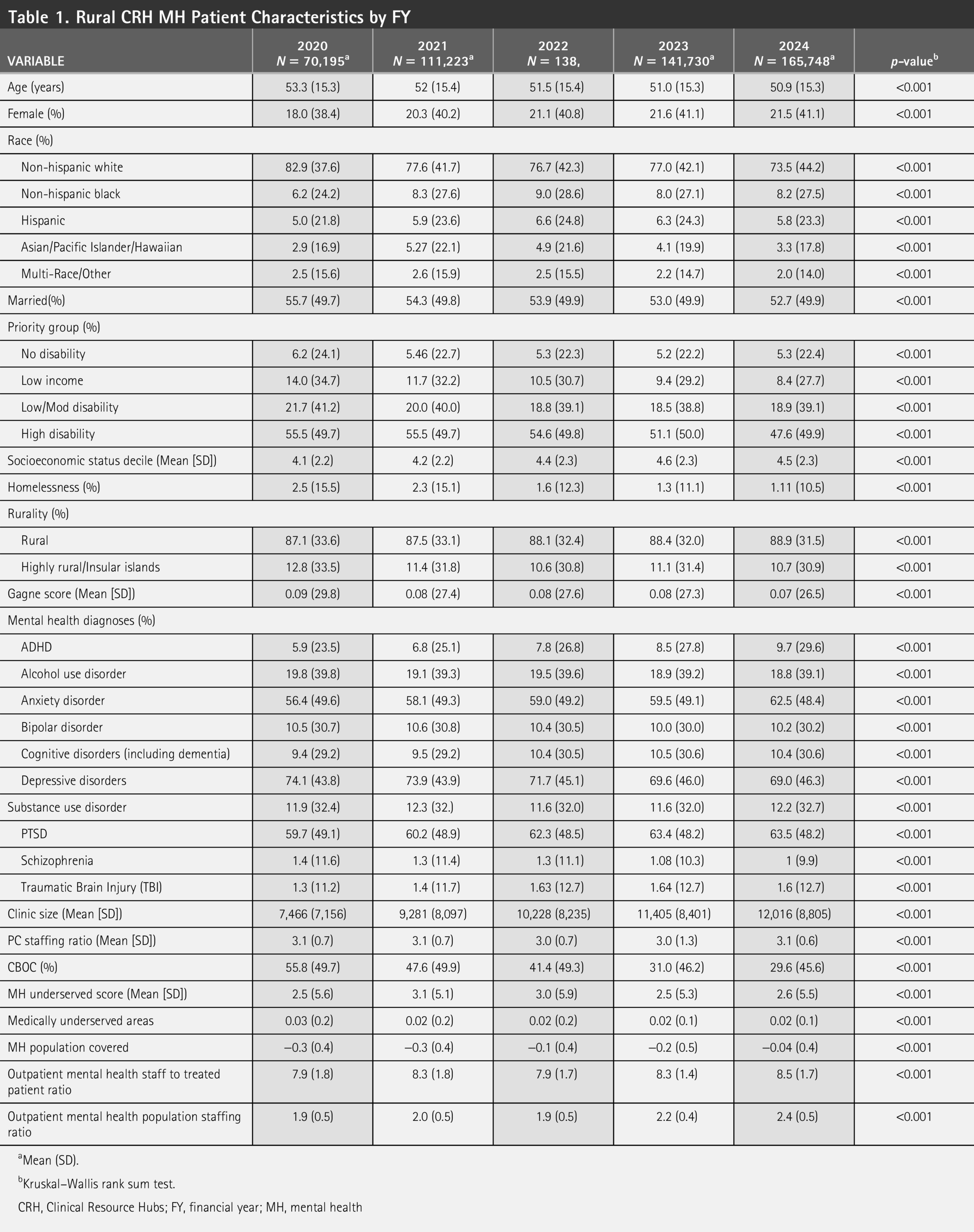
CRH MH teams completed 627,436 encounters with Veterans residing in rural or highly rural areas, 81.9% of which were telehealth visits. Encounters to these areas increased steadily over time, from 70,195 encounters in FY20 to 165,748 encounters in FY24 ( Table 1 ). Telehealth encounters (including phone, secure messaging, and video) increased from 76.7% of all CRH encounters in FY20 to 86.7% of all encounters in FY24. During the study period, monthly encounters delivered to Veterans in rural or highly rural areas increased threefold (5,058 MH encounters in October 2019 to 14,152 encounters in September 2024), while monthly overall CRH MH encounters increased fourfold (9,044 CRH MH encounters in October 2019 to 40,654 CRH MH encounters in September 2024) ( Fig. 1 ). The number of unique clinics that had at least one CRH MH encounter steadily increased at both urban and rural/highly rural sites over time (239 unique rural and 203 unique urban sites providing care in October 2019 to 440 unique rural and 455 unique urban sites in September 2024) ( Fig. 1 ). Between FY20 and FY24, the primary modality of care utilized at rural and highly rural sites shifted from video visits by a CRH clinician into a spoke clinic (77.5% of all encounters in FY20 to 7.1% in FY24) to video visits in the patient’s home (9.2% in FY20 to 64.3% in FY24) ( Fig. 2 ).

Growth of CRH MH Encounters and CRH MH Sites among Veterans Living in Rural and Highly Rural Areas, FY20-24. CRH, Clinical Resource Hubs; MH, mental health.
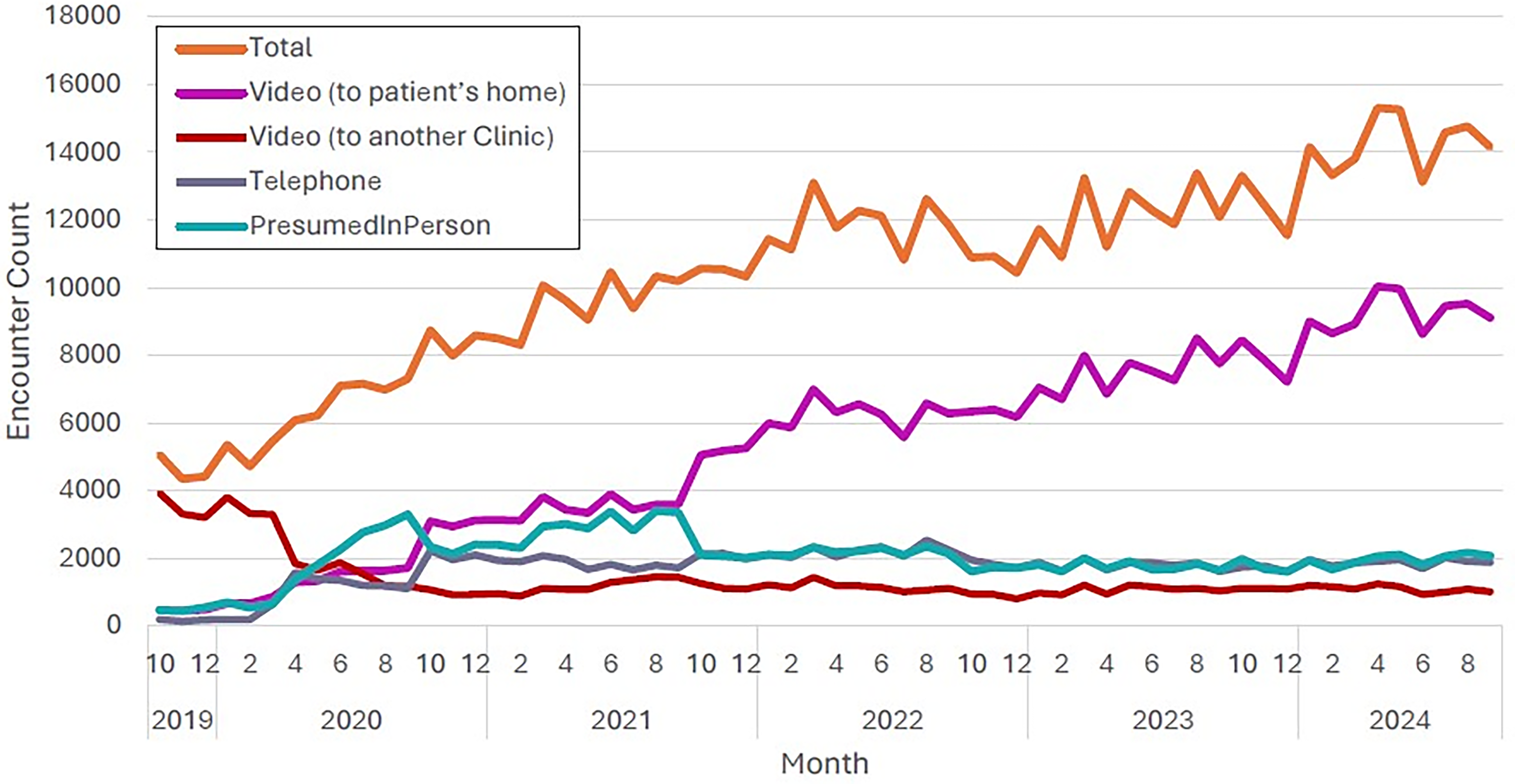
CRH MH Encounters by Modality Type, FY20–24.
Rural CRH MH Patient Characteristics by FY
Mean (SD).
Kruskal–Wallis rank sum test.
CRH, Clinical Resource Hubs; FY, financial year; MH, mental health
Analysis of rural patient demographics revealed an increase in racial and ethnic diversity over time, especially among Black (6.2% in FY20 and 8.2% in FY24) and Hispanic (5.0% in FY20 and 5.8% in FY24) Veterans. During this same period, telehealth modality use was similar across demographic groups with video visits increasingly becoming the predominant mode of care. Among Black rural Veterans, video visits increased from 51.1% of encounters in FY20 to 61.7% in FY24, while in-person visits declined from 38.2% to 27.7% during that same period. Among Hispanic rural Veterans, video visits remained the predominant modality throughout the study period, accounting for 68.7% of encounters in FY24. Between FY20 and FY24, the percent of rural Veterans cared for with depressive disorders saw a slight decrease (74.1% in FY20 to 69% in FY24, p < 0.001), while there was a slight increase in Veterans diagnosed with anxiety disorder (56.4% in FY20 to 62.5% in FY24), PTSD (59.7% in FY20 to 63.5% in FY24), and ADHD (5.9% in FY20 to 9.7% in FY24) ( Fig. 3 ).

Unique CRH MH Rural/Highly Rural Patients with Diagnosed Mental Health Conditions, FY20–24.
Discussion
Rural and highly rural communities are often moderately or severely understaffed with MH care clinicians, which continues to pose challenges for Veterans living in these regions.6,7,27 These challenges are complicated and multifactorial including factors related to distance, culture, access to providers, as well as digital divide challenges (i.e., barriers related to limited broadband access, device availability, and digital literacy).9,10 As a national health care system serving all Veterans, the VA is mandated to provide equitable access to MH care to those living in rural communities. 11 However, recruiting MH clinicians to serve in rural areas is challenging for many reasons including professional and geographic isolation, limited resources, stigma, infrastructure issues, burnout, and high turnover.9,28–32 Veterans residing in these areas may present for care with complex and severe MH conditions related to military trauma that exceed the expertise and resources of non-VA clinicians. Consequently, the lack of local MH support and infrastructure within rural VA sites can compound burnout risk and impede access to timely, specialized care.9,33
Analysis of encounter data from the first 5 years of the CRH MH program found that the availability of CRH regional telemental health support for rural VA community-based clinics was associated with rapid growth in use of virtual MH services by rural and highly rural Veterans. Telemental health accounted for 76.7% of encounters in FY20 and increased to 86.7% by FY24. The increase among Black and Hispanic Veterans suggests that regionally delivered virtual care may help mitigate traditional barriers to care that disproportionately affect minority Veterans in rural communities, including limited broadband access, provider shortages, and lower availability of culturally competent clinicians.34–37 Between FY20 and FY24, the proportion of video visits delivered directly to patients’ homes (VVC visits) rose from 9.2% to 64.3%. This trend parallels broader VA telehealth trajectories during and after the COVID pandemic with a twelvefold increase in system-wide video encounters between 2019 and 2020. 38 Comparable national evaluations of CRH MH have found that regional telehealth hubs provided care with significantly higher Veteran satisfaction when compared with community care, 6 suggesting the expansion of accessible, flexible care modalities, particularly increased use of home-based video and virtual services, may improve patient experience by reducing logistical barriers and increasing convenience for rural Veterans.
Our findings align with other evaluations of large-scale VA telehealth interventions targeting rural and underserved populations. These findings are consistent with prior evaluation of telemental health services, which demonstrate enhanced access to MH services through elimination of geographic barriers and improved utilization through increased convenience and reduced travel requirements. 39 For example, the VA TeleSleep and primary-care telehealth initiatives reported millions of Veteran travel miles avoided through virtual encounters. 40 Beyond improved access, TMH has been associated with high patient and provider satisfaction, reduced wait times, and positive clinical outcomes.39,41 These efficiencies enable better resource allocation and cost saving for both Veterans and the health care system, particularly in regions with limited local MH expertise. 42 Furthermore, expansion of telemental health may address stigma and privacy concerns that often discourage care-seeking among rural Veterans by allowing treatment to occur in private home environments.42,43
Despite these gains, persistent challenges remain. Rural veterans continue to face digital barriers related to broadband availability, device access, and technological literacy. 43 Continued monitoring of equity, connectivity, and staffing adequacy will be essential to ensure that telemental health services translate into sustained improvements in access and outcomes for rural populations.
Limitations
This study has several limitations. As a retrospective analysis using electronic health record data, results may be affected by documentation inaccuracies or missing data. Because of its observational design, findings demonstrate associations rather than causal relationships. To mitigate data quality concerns, we implemented stringent quality checks where possible, relied on standardized variables, and used aggregated data to minimize the influence of individual-level anomalies that could distort overall trends and to smooth out inconsistencies in data. Focusing on long-term trends rather than isolated time points also helped to reduce the impact of any short-term fluctuations or reporting variability. While the cohort included a diverse range of Veterans to enhance the representativeness of the rural veteran population, results may still not generalize to all geographic regions of VA facilities. Finally, the study period overlapped with the COVID-19 pandemic, during which telehealth utilization expanded rapidly across the VA. The early implementation of the CRH program during this period may have been influenced by pandemic-related changes in care delivery, and findings should be interpreted within this contextual period.
Conclusions
We found that the amount of predominantly telemental health services provided by the CRH program to rural Veterans more than doubled over a 5-year period, with expanded site participation and an increasingly diverse patient population over time. CRH MH encounters delivered to Veterans in rural areas experienced threefold growth over the first 5 years of CRH implementation, and the number of rural sites providing CRH MH care doubled across VA during this 5-year period. These services reached a progressively more diverse Veteran population, addressing a wide range of MH needs, including increasing numbers of Veterans diagnosed with PTSD, anxiety disorders, and ADHD. Together, these findings show that CRHs have reduced historic gaps in rural MH access, though additional research is necessary to identify predictors of CRH MH use among rural Veterans as well as the quality of MH care delivered.
Authors’ Contributions
E.J.: Methodology, data curation, software, formal analysis, visualization, writing—original draft preparation, writing—review and editing. C.L.W.: Conceptualization, methodology, data curation, writing—original draft preparation, writing—review and editing. K.N.: Supervision, writing—review and editing. I.C.: Writing—review and editing. L.W.: Writing—review and editing. B.F.: Conceptualization, methodology, supervision, writing—original draft preparation, writing—review and editing.
Footnotes
Acknowledgments
This work was undertaken as part of the Clinical Resource Hub (CRH) under the Veterans Administration’s Primary Care Analytics Team (PCAT).
Author Disclosure Statement
The views expressed are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs.
The authors have no conflicts of interest or financial disclosures to report. The views expressed are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs.
Funding Information
No funding was received for this article.
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.