
Abstract
Background:
Approximately 50,000 neonates weighing under 1,500 grams are born annually in the United States, with 15–20% delivered in smaller community hospitals without a neonatal intensive care unit. These “outborn” infants face higher risks of adverse outcomes due to limited resources. Implementing tele-resuscitation services with targeted training workshops may enhance providers’ technical skills, confidence, and perceptions of feasibility and acceptability.
Methods:
In January 2023, Oklahoma Children’s Hospital launched a tele-resuscitation program offering real-time, audio-video support to community hospital staff. This service targeted neonates ≤32 weeks’ gestation, <1,500 g, and those >32 weeks requiring advanced resuscitation. Workshops were hosted to give community hospital providers a first hand experience with the technology, and it included background on tele-resuscitation, technical skills training, and neonatal resuscitation simulations incorporating telemedicine. Pre- and postworkshop surveys with Likert scale questions assessed attendees’ confidence in advanced resuscitation and feasibility of integrating tele-resuscitation into practice.
Results:
Briefly, 20 community providers attended two interprofessional workshops, including 5 physicians (25%), 11 nurses (55%), and 4 respiratory therapists (20%). One-quarter of attendees reported prior experience with telemedicine, and one attendee reported prior experience with tele-resuscitation. Following the workshops, participant confidence in performing tasks such as intubation, umbilical line placement, needle thoracentesis, and debriefing increased significantly (p < 0.001 for all procedures). While ratings for the appeal and applicability of telemedicine to their practice showed no significant changes (p = 0.267 and p = 0.056, respectively), the perceived feasibility of tele-resuscitation significantly improved after the workshop (p = 0.029).
Conclusions:
Neonatal tele-resuscitation workshops improved providers’ perceptions of this service and increased their acceptance of such a program. Additionally, the skill sessions and simulated resuscitations increased their confidence with procedures commonly performed during advanced neonatal resuscitation.
Introduction
Approximately 10% of all newborns require assistance with breathing at birth, and less than 1% require extensive cardiopulmonary resuscitation in the delivery room (DR). 1 Smaller community hospitals, particularly those in rural areas, tend to have fewer deliveries and infrequent neonatal emergencies, which makes it challenging for pediatricians and family physicians to stay proficient in DR resuscitation. Studies have shown a rapid decline in provider skill and knowledge as early as 4–6 months after their training.2–5 Through a real-time, audio-video telemedicine connection, tele-resuscitation allows neonatologists to provide on-demand bedside support to staff at these community hospitals. The remote neonatologist can assist the community hospital care team during high-acuity resuscitations and postnatal stabilization, thereby enhancing the quality of care. 6 Tele-resuscitation has the potential to narrow the gap in care between infants born in community hospitals without a neonatal intensive care unit (NICU) and those delivered in referral hospitals with a NICU.
Numerous studies have demonstrated the effectiveness and feasibility of tele-resuscitation.6–10 Video-assisted resuscitation has been found to shorten the time to achieve effective ventilation, enhance the application of corrective measures for ineffective ventilation, reduce the need for intubation, and improve compliance with the Neonatal Resuscitation Program (NRP) guidelines during simulated resuscitations. 7 A retrospective study comparing neonates who received telemedicine support during resuscitation with those who did not found that the telemedicine group had higher resuscitation quality ratings. This improvement was especially notable in the preterm subgroup, which was also more likely to receive critical interventions. 6 Video-assisted resuscitation reduced the necessity for transfers to a NICU, shortened the length of stay at the birth facility, and decreased the number of days newborns required supplemental oxygen at the birth hospital.10,11 Preventing unnecessary neonatal transfers supports family-centered care, boosts revenue for community hospitals, and eliminates the cost and risks associated with a patient transport.
Telemedicine is also being utilized successfully to train and guide health care providers in performing urgent procedures during neonatal resuscitation, including airway management, needle thoracentesis, and placement of umbilical lines.12–14 In addition to offering virtual assistance during resuscitations and procedures, telemedicine can also be utilized to deliver regular neonatal resuscitation training sessions. Multiple studies have shown that tele-education is a viable alternative to traditional neonatal resuscitation training, offering health care providers similar gains in knowledge and skill proficiency.15–17 It can be utilized to evaluate resuscitation skills among providers at remote centers and strengthen neonatal resuscitation training in regions with limited access to experienced instructors. 18
Neonatal tele-resuscitation workshops were conducted with an intention to expose newborn delivery providers from community hospitals to this technology and demonstrate its effectiveness and feasibility in their clinical practice. These workshops included both educational lectures and hands-on technical skill training focused on procedures and competencies essential to advanced neonatal resuscitation. The study aimed to determine whether participation in tele-resuscitation workshops could increase the perceived feasibility and applicability of tele-resuscitation programs in community hospital settings and improve technical skills while boosting self-confidence amongst community health care providers by providing procedural tele-guidance.
Methods
In 2023, Oklahoma Children’s Hospital (OCH) launched a neonatal tele-resuscitation program to support community hospitals with level I nurseries in rural areas of the state with annual delivery volumes ranging between 300 and 1,000. Health care professionals, including labor and delivery nurses, respiratory therapists, family medicine physicians, and pediatricians, from these hospitals were invited to attend tele-resuscitation training workshops held at OCH. Two interprofessional workshops were conducted in May 2023 and March 2024, featuring lectures, telemedicine-guided technical skills training, neonatal resuscitation simulations that included tele-resuscitation, and instructional debriefing sessions. Attendance at these workshops was completely free for everyone.
The workshop spanned 8 h and was divided into instructional lectures and practical skill-based sessions. The didactic session included an introduction to tele-resuscitation, a review of telemedicine-specific skills, guidance on effective communication and teamwork through telemedicine, and a walkthrough of the steps needed to implement the service. In the tele-simulation sessions, participants were organized into small groups of three to five individuals. Additionally, one OCH neonatologist or a neonatology fellow with no prior tele-resuscitation experience was paired with each of the groups and served the role of a tele-consultant for the simulations.
Using three simulated neonatal resuscitation scenarios, the neonatologist or fellow used telemedicine to guide community hospital staff through key NRP procedures. The learning objectives of the first scenario were to deliver effective positive pressure ventilation, which included using the corrective steps for ineffective ventilation. The second session focused on establishing an alternative airway (either endotracheal intubation or supraglottic airway insertion) and performing thoracentesis. The objectives of the third scenario were to deliver effective chest compressions and successfully place a low-lying umbilical venous catheter for epinephrine administration. For the first two scenarios, the neonatologist or fellow used a telemedicine cart device (Teladoc®) to complete the telemedicine consult, while consultation during the third scenario was performed over a video conference (Zoom®) application on a mobile device (iPhone®) placed on a tripod stand.
During these sessions, the session leader first reviewed the equipment and setup with the participants, allowing time to familiarize and practice before commencing the tele-simulation. Then the neonatologist or fellow led the scenario remotely from a different room under the guidance of the session leader. Upon conclusion of each scenario, the team engaged in a debriefing session utilizing the audio and video recordings from the simulation center.
Finally, all participants observed a mock tele-resuscitation consult led by a neonatologist in the room, providing virtual support to a community hospital neonatal team. The program concluded with a demonstration showcasing an effective debriefing process with the community hospital neonatal team using telemedicine. At the start of the workshop, all participants received anonymous paper surveys featuring Likert scale questions created by the study team, aimed at evaluating the practicality of implementing a tele-resuscitation program in their practice and assessing their level of confidence in performing advanced resuscitation procedures (Supplementary Data).19,20 The surveys gathered information about providers’ roles and the length of time they had served in those roles. No data were collected regarding the institutions with which they were affiliated. Completion of the survey was considered their consent to participate. The first portion of the survey was completed before the workshop began, while the second portion, containing the same questions, was completed at the end of the workshop to reassess their readiness to adopt the program and the change in their procedural confidence when offered tele-guidance. The surveys were returned in a bin as attendees concluded the workshop. Additionally, after establishing contracts with community hospitals, the OCH telehealth team organized quarterly tele-simulation sessions with these sites to support the ongoing development and retention of health care providers’ resuscitation skills.
Survey response data were reported using descriptive statistics. Changes in Likert ratings from pre- to postworkshop were analyzed using paired t-tests. Analysis was performed using R. This study was considered exempt by the Institutional Review Board (IRB) of the University of Oklahoma, IRB#15881.
Results
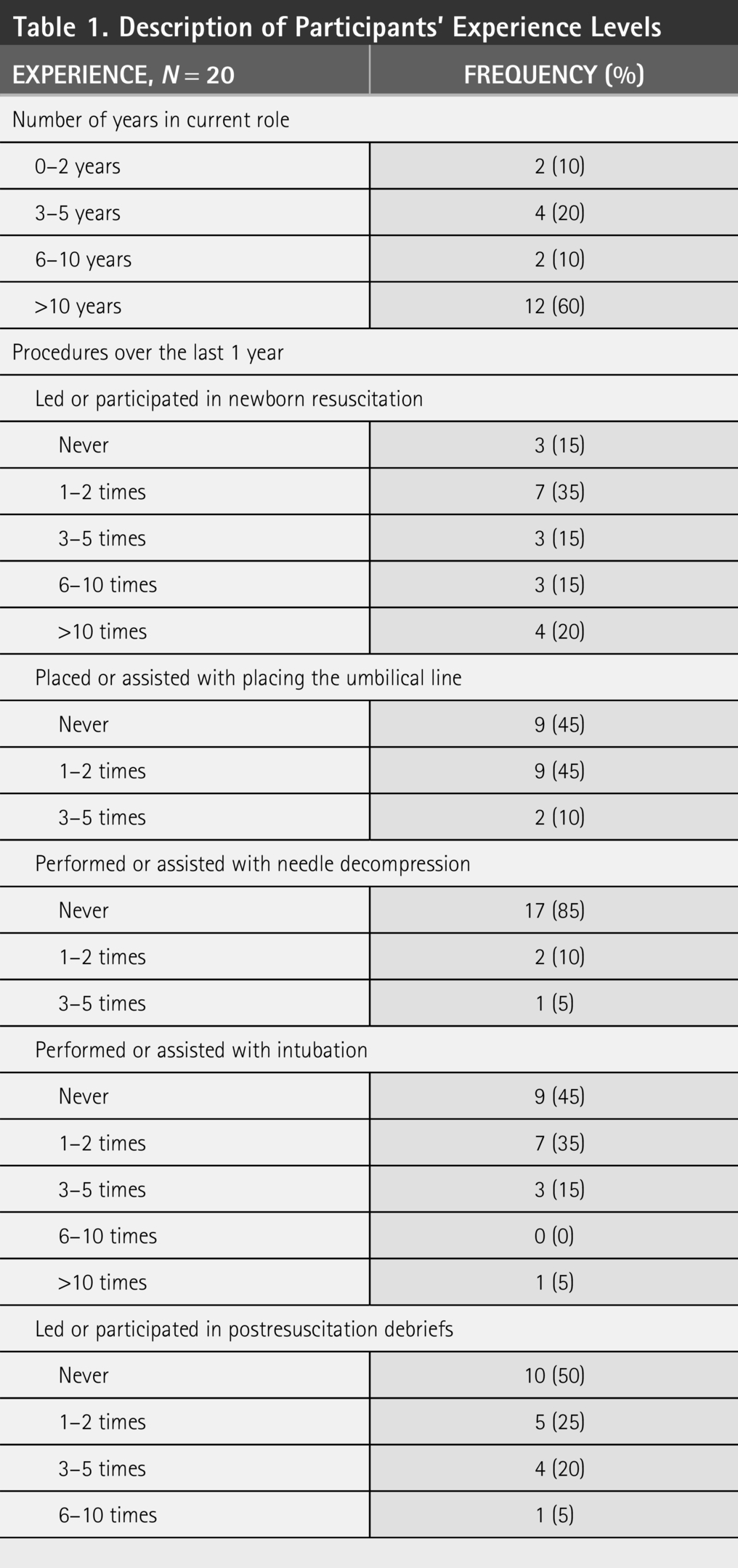
The two workshops were attended by 5 physicians (20%), 11 nurses (55%), and 4 respiratory therapists (20%) from 5 different community hospitals. Table 1 describes participants’ levels of experience with newborn resuscitation, procedures, and debriefing. The majority of participants (n = 12, 60%) had been in their role more than 10 years, and half of participants had led or participated in no more than 2 newborn resuscitations in the last year.
Description of Participants’ Experience Levels
Confidence significantly increased for the following activities: Leading or participating in a newborn DR resuscitation; placing or assisting with placing an umbilical line; performing or assisting with a needle decompression; performing or assisting in an intubation; and leading or participating in a postresuscitation debrief with telemedicine support ( Fig. 1 and Table 2 ).
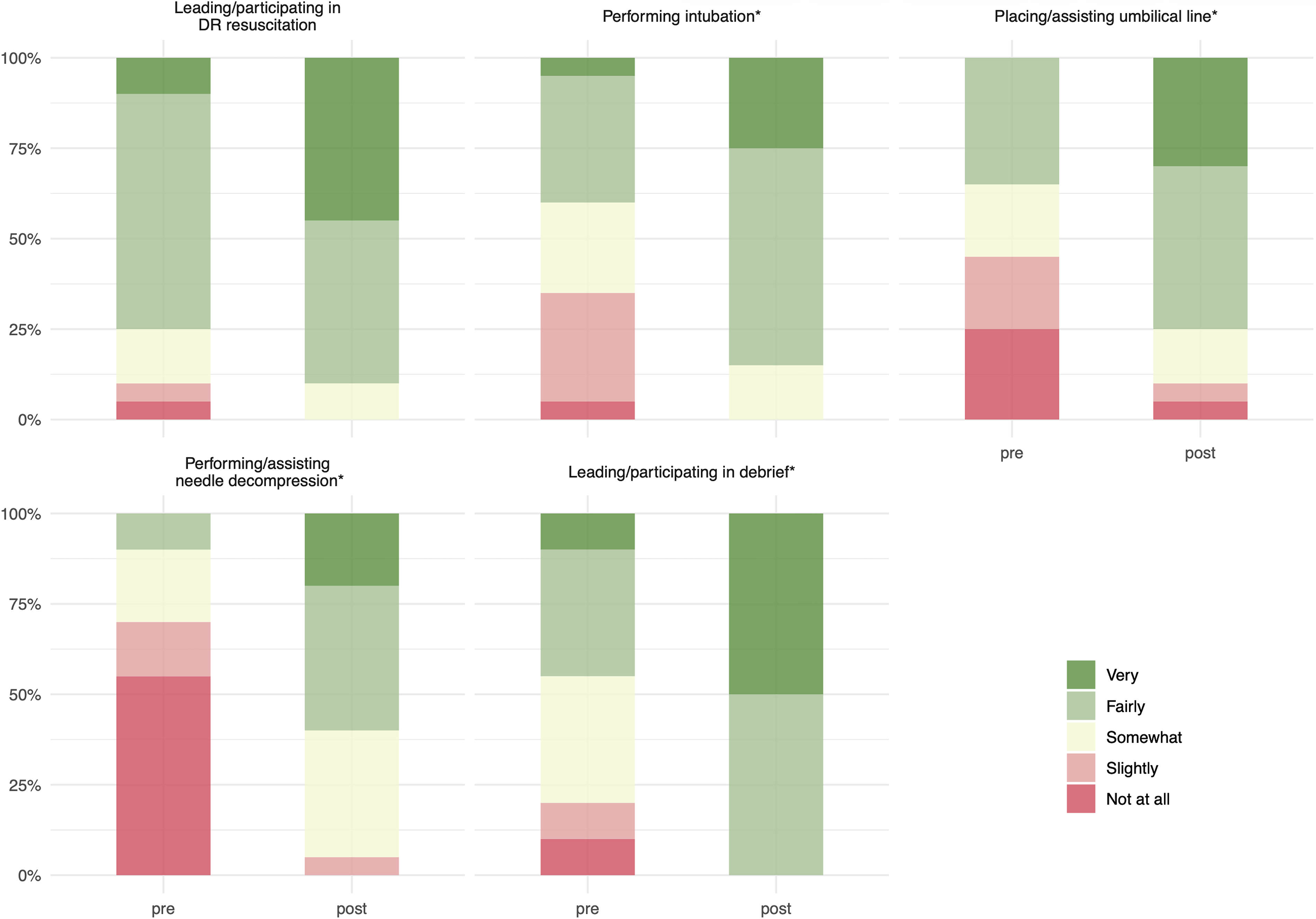
Provider confidence scores with neonatal procedures before and after the workshop Significant increase in confidence scores from pre- to postworkshop in performing tasks including intubation, umbilical line placement, needle thoracentesis, and debriefing, all with p < 0.001. Significant change in leading or participating in newborn resuscitation (p = 0.015).
Comparison of Pre- and Post-Workshop Survey Responses
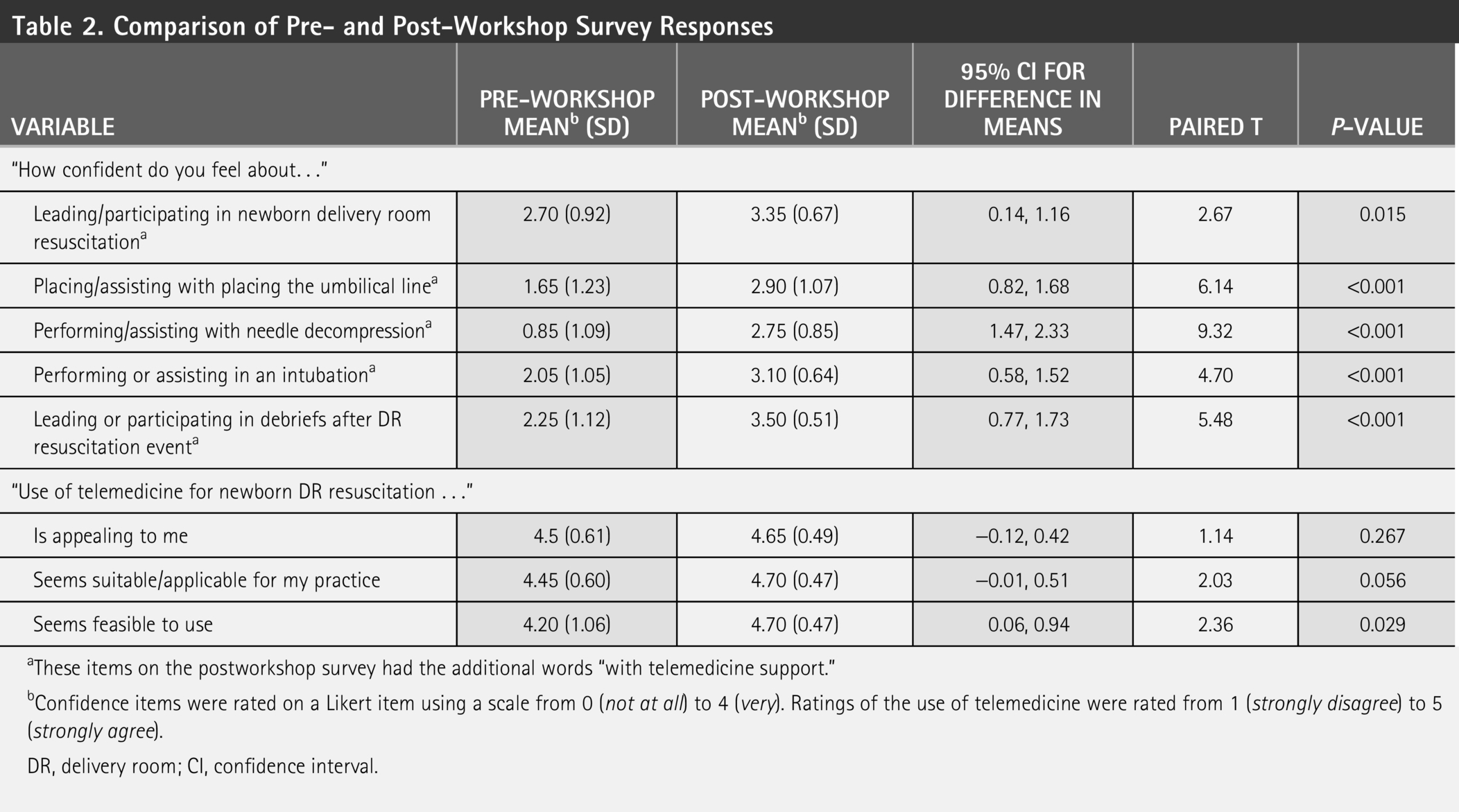
These items on the postworkshop survey had the additional words “with telemedicine support.”
Confidence items were rated on a Likert item using a scale from 0 (not at all) to 4 (very). Ratings of the use of telemedicine were rated from 1 (strongly disagree) to 5 (strongly agree).
DR, delivery room; CI, confidence interval.
Participants also had significantly higher mean ratings endorsing tele-resuscitation as feasible to use. Ratings on suitability or applicability to their practice showed an upward trend (p = 0.056) from pre to postworkshop.
Discussion
These workshops were designed to expose community health care providers to tele-resuscitation technology, provide them with an opportunity to experience it in real-time, and evaluate its applicability and feasibility in their clinical practice. To the best of our knowledge, this is the first study to evaluate the effectiveness of a workshop in delivering essential knowledge and practical exposure to tele-resuscitation technology, enabling providers to gain a better firsthand understanding of the service and assess its applicability to their own clinical practice. In this study involving health care professionals from five community hospitals, we demonstrated that neonatal tele-resuscitation workshops increased perceptions of tele-resuscitation feasibility and improved provider confidence in performing neonatal resuscitation skills with tele-guidance. Participants represented a multidisciplinary group with varying levels of clinical experience. Following the workshop, there was a significant increase in the perceived feasibility of using tele-resuscitation in their local practice, with a positive trend toward greater perceived suitability for clinical practice. Additionally, participants reported significant improvements in confidence across all procedural areas when guided via telemedicine.
The participating hospitals represented a range of community-level NICUs with variable levels of neonatal acuity, staffing models and provider experience. This heterogeneity mirrors the broader national landscape, where many outlying hospitals face challenges in maintaining resuscitation competencies due to infrequent exposure and limited specialist support. 5 The consistency in improved confidence across diverse roles and institutions suggests the workshop model could be effectively scaled to other similar settings, particularly in rural or underserved regions where telemedicine is increasingly vital to care delivery. 21
Telemedicine workshops have utility for training participants from community hospitals in telemedicine practice and resuscitative procedures. Notably, despite the fact that many participants had been in their roles for over a decade, a substantial proportion had limited hands-on exposure to key resuscitative procedures, including DR resuscitation, umbilical line placement, needle decompression, intubation, and postresuscitation debriefing—half had participated in no more than two newborn resuscitations, and most had never assisted with intubation or needle decompression in the last year. Notably, confidence gains were substantial in this cohort, where half of the participants had limited exposure to newborn resuscitation. Incorporating tele-resuscitation elements into the scenarios allowed participants to gain comfort not only with technical tasks but also with the dynamics of remote collaboration, a critical aspect of successful tele-resuscitation consults. 6 As telemedicine becomes more embedded in neonatal care models, training efforts that build familiarity and acceptance among bedside providers will be essential to sustained implementation success. 22
The structure of the telemedicine workshop itself may contribute to its effectiveness. Preparatory skills sessions, followed by standardized simulated scenarios—ensured that all participants had equal exposure to content and procedural practice. Although session leaders varied slightly between sessions, core teaching content and simulation structure were standardized, helping to reduce instructional variability. 23 These preparatory sessions were intentionally excluded from performance evaluation, allowing participants to build procedural familiarity and confidence. Participants were able to experience both high- and low-fidelity technologies for tele-resuscitation, and no notable difference was observed in their postworkshop confidence with the procedure between the two technologies.
LIMITATIONS
The study had several limitations. The small sample size restricted statistical power and prevented subgroup analyses. The prepost design, while appropriate for a training intervention, limits causal interpretation. Its reliance on immediate postworkshop confidence measures may not adequately capture lasting skill retention or the real-world effectiveness of the training. Additionally, wording differences between the pre and postworkshop surveys—specifically, the addition of “with telemedicine support” in postworkshop confidence items—may have contributed to inflated postintervention scores. The absence of a significant change in perceived appeal of tele-resuscitation is likely explained by a ceiling effect, as preworkshop ratings were already high. Variability in the bedside team experience was another consideration, as tele-simulation sessions were led by physicians with no prior tele-resuscitation experience, potentially impacting the consistency of feedback and guidance.
Furthermore, the workshops were conducted at a simulation center within a tertiary hospital setting, geographically removed from the rural community sites where participants typically practice. This disconnect may have limited real-time contextual learning. In the first workshop, participants were assigned to mixed-institution teams, which reduced opportunities to reflect on site-specific workflows or equipment gaps—such as the absence of laryngeal mask airways in some hospitals’ emergency kits. However, there were positive responses observed across all measured domains of provider confidence and perceptions of telemedicine feasibility. The use of pre- and postworkshop surveys allowed for direct within-subject comparisons, minimizing interindividual variability. While self-reported confidence is a subjective measure, the magnitude and consistency of improvement across multiple domains strengthen the credibility of the findings and suggest a true educational effect.
Conclusion
Neonatal tele-resuscitation workshops enhanced providers’ views on the feasibility of implementing such a program in their practice. The hands-on skill sessions and tele-resuscitation simulations improved participants’ confidence in performing commonly conducted procedures during advanced neonatal resuscitation when supported through tele-guidance. However, ongoing assessment of participant performance over time is necessary to determine the durability of knowledge retention, procedural competency, and the long-term impact of the training received during the workshop. In addition, future studies involving larger sample sizes are needed to improve the generalizability of these findings and to further evaluate the effectiveness and scalability of tele-resuscitation training programs across diverse health care settings.
Footnotes
Acknowledgments
The authors are thankful for their commitment to advancing health care education and supporting initiatives aimed at improving health outcomes across Oklahoma.
Author Disclosure Statement
Dr. Fang has licensed intellectual property and earns royalties from Teladoc Health. The remaining authors declare no competing financial interests.
Funding Information
This project was funded by the Tobacco Settlement Endowment Trust (Agreement # DG23-02).
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.