
Abstract
Objective:
To evaluate the association between implementation of a personalized, postdischarge telehealth support program and 30-day hospital readmission among patients hospitalized with stroke.
Methods:
This observational pre–post implementation study was conducted within an acute care hospital system and included adult patients (≥18 years) admitted with ischemic stroke, intracerebral hemorrhage, or subarachnoid hemorrhage. Following discharge, eligible patients were offered enrollment in a person-centered telehealth support program. The primary outcome was all-cause 30-day readmission. Multivariable regression models were used to adjust for baseline clinical characteristics.
Results:
Among 405 patients, 258 were admitted before telehealth implementation, 31 were enrolled in the telehealth program after implementation, and 116 were postimplementation nonenrollees. Thirty-day readmission occurred in 23 of 258 patients (8.9%) before implementation, in 0 of 31 telehealth enrollees (0%), and in 3 of 116 nonenrollees (2.6%). After adjustment for clinical covariates, postimplementation patients demonstrated a lower estimated risk of 30-day readmission compared with preimplementation patients, with the lowest risk observed among telehealth enrollees. Based on a 6.3% absolute reduction in readmissions and published cost estimates, telehealth implementation corresponded to an annual savings of approximately $112,000–$124,000 in avoided uncompensated care for uninsured patients and $545,000–$602,000 in reduced exposure to denied claims for insured patients per 1,000 strokes. Anticoagulant use was associated with a higher estimated probability of readmission.
Conclusion:
Implementation of a person-centered postdischarge telehealth service was associated with substantially lower 30-day readmissions among patients hospitalized with stroke and may provide meaningful economic benefits by reducing costly readmissions and financial burden on hospitals.
Introduction
Stroke is a leading global cause of death and long-term disability. It ranked as the second-leading cause of death and the third-leading cause of death and disability combined in 2019, accounting for approximately 7 million deaths worldwide in 2021. Each year, around 5.5–7 million people die from stroke, and among survivors, nearly one-third to one-half experience lasting functional limitations that significantly impair independence and quality of life.1,2 In the United States, more than 795,000 new or recurrent strokes occur annually, making stroke a primary cause of serious morbidity and the fifth leading cause of death nationally.3,4 In addition to its huge negative personal impact, stroke also imposes a significant clinical and economic burden on patients, families, and health care systems. Across the United States, 30-day hospital readmission rates after stroke are considerable, commonly ranging from 6% to over 12%.5–7
These early readmissions highlight potential gaps in postdischarge care and contribute significantly to increased health care utilization and costs, particularly among vulnerable populations and institutions serving under-resourced communities.8,9 Hospital readmissions after stroke also impose a significant economic challenge for hospitals and health systems. 9 Each unplanned readmission is associated with considerable costs, often exceeding tens of thousands of dollars per patient per year, due to extended hospital stays, additional diagnostic evaluations, and increased rehabilitation needs. 10
Digital health and telehealth platforms, particularly those providing personalized support and guidance after hospital discharge, may offer a helpful yet underutilized approach to enhancing stroke recovery. Kandu Health’s Principal Illness Navigation (PIN) model is a good example of this approach. Early pilot data suggest the PIN model may improve postdischarge outcomes, including reduced readmissions and improved follow-up care. 11 As a result, personalized telehealth support has gained attention because it can be easily expanded and fits well with modern value-based care practices and recovery recommendations.
Despite promising early results, the theoretical pathways through which person-centered telehealth may reduce readmissions remain underexplored in the literature. Conceptually, several frameworks help explain these mechanisms. The Chronic Care Model emphasizes self-management support, care coordination, and proactive follow-up, elements associated with improved chronic disease outcomes and reduced acute care utilization. 12 The Transitional Care Model highlights structured discharge planning, early postdischarge engagement, symptom monitoring, and caregiver involvement as critical determinants of 30-day outcomes. 13 Similarly, the Reach, Effectiveness, Adoption, Implementation, and Maintenance framework provides a structure for evaluating the real-world impact and scalability of telehealth interventions. 14 However, few stroke studies explicitly integrate these models into their design, limiting the field’s understanding of how telehealth components, such as navigation, symptom monitoring, or care coordination, mechanistically influence readmissions.
Another critical gap in the literature involves feasibility and real-world implementation. While controlled studies show benefits in functional recovery, quality of life, and other patient-centered outcomes, 15 few investigations have evaluated the impact of personalized telehealth programs on hospital-wide 30-day readmissions, health care utilization, or economic outcomes. Understanding how a standardized, person-centered telehealth program performs in routine practice, including its effect on readmissions, follow-up engagement, symptom escalation pathways, and associated costs, is essential to determine its practicality, scalability, and value for health care systems.
The present study aims to address these gaps by evaluating stroke patient readmission rates and early recovery outcomes before and after the hospital-wide implementation of a personalized telehealth navigation system at a single center. Specifically, we examine the relationship between this intervention and 30-day readmissions, an established quality and performance indicator, while also assessing feasibility, patient engagement, and early recovery within everyday clinical practice.
Methods
This study adheres to the Strengthening the Reporting of Observational Studies in Epidemiology guidelines for reporting observational research. This study was conducted in two parts at a single comprehensive stroke center within a large regional health system. The regional health system spans 3 metropolitan regions and includes 14 acute care hospitals. Among these, there are five Comprehensive Stroke Centers; eight Primary Stroke Centers, of which three are currently pursuing Thrombectomy-Capable or Comprehensive Stroke Center designation; and one is a nonstroke center. While patient enrollment and data collection occurred at our institution, readmission outcomes were evaluated across the entire regional system to ensure readmissions to any affiliated hospital were captured. First, we retrospectively collected data over the 6 months preceding the introduction of Kandu Health’s telehealth program and compared readmission rates with those from the 6 months following implementation, regardless of patient participation. In the second part, we analyzed a prospectively collected cohort by comparing readmission rates between patients enrolled in the telehealth program and those who were not. Overall, this comparative study evaluated the impact of Kandu Health’s 30-day virtual stroke recovery program on patient outcomes and hospital readmissions.
This research activity was determined to be exempt from Institutional Review Board (IRB) oversight in accordance with current regulations and institutional policy (internal reference number: 2024-909).
PARTICIPANTS
Adult patients (≥18 years) admitted with ischemic stroke, intracerebral hemorrhage, or subarachnoid hemorrhage were included. Stroke confirmation requires both clinical evaluation by a neurologist and neuroimaging (Magnetic Resonance Imaging of the brain).
In the retrospective cohort, stroke diagnoses were identified using International Classification of Diseases, Tenth Revision codes. For the prospective cohort, all consecutive patients presenting with neurological symptoms were assigned stroke codes as part of standard practice at our comprehensive stroke center. Eligible patients were discharged either directly home or to an acute rehabilitation unit. Patients with transient ischemic attack, unconfirmed stroke, discharge to hospice, transfer to a skilled nursing facility or other nonoutpatient location, or with planned readmission were excluded.
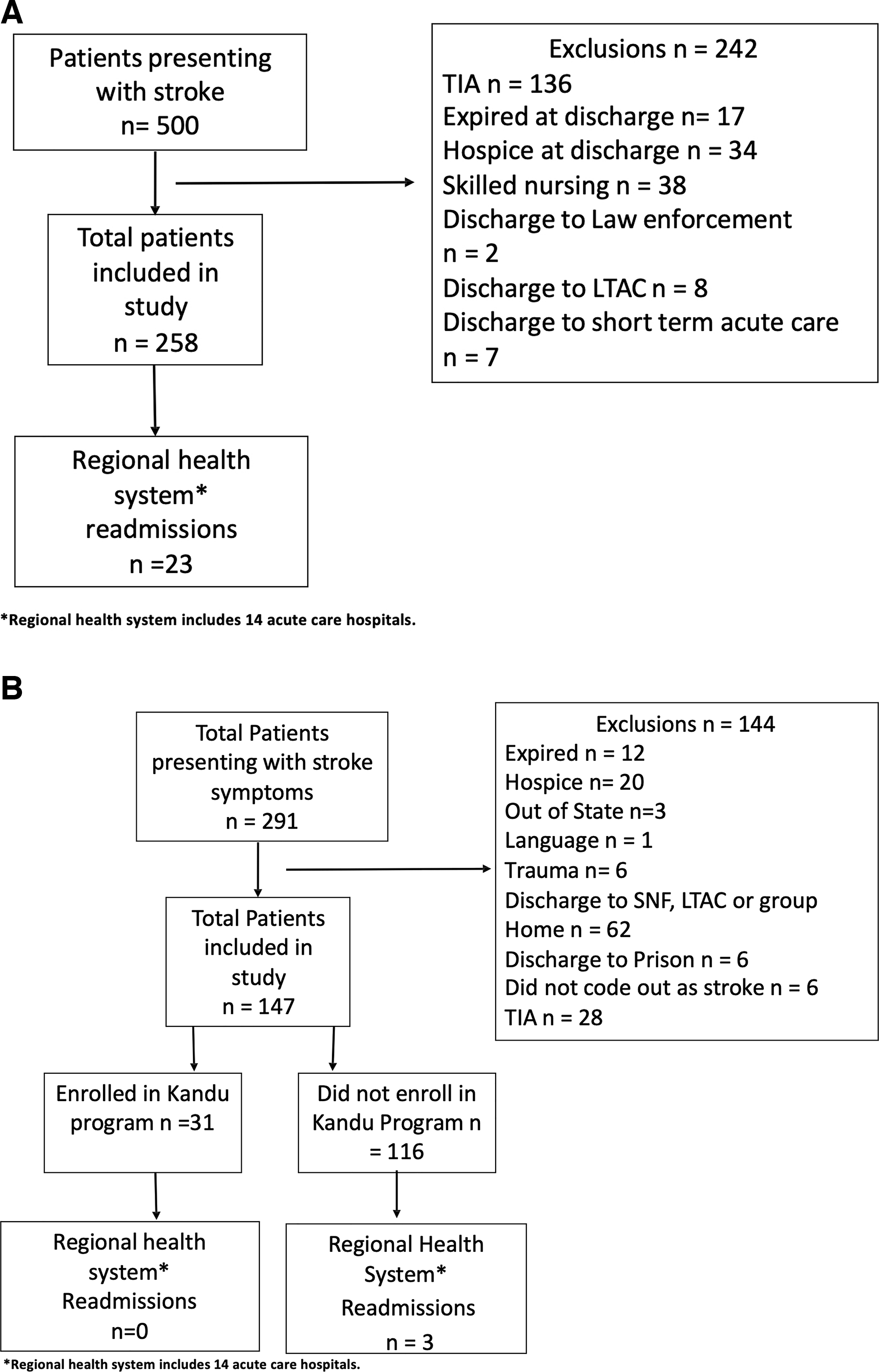
Flow diagrams summarizing patient screening, eligibility, and allocation are presented in Fig. 1 . Fig. 1A shows patient selection for the retrospective pretelehealth implementation cohort, and Fig. 1B illustrates patient selection for the prospective postimplementation cohort.
INTERVENTION
All patients in the prospective cohort were offered participation in Kandu Health’s virtual recovery program (telehealth program). Those who agreed began with an initial virtual evaluation and management visit with a Kandu physician. 16 Subsequently, each patient was paired with a dedicated Kandu Navigator through an app-enabled platform. Navigators are licensed occupational therapists or licensed clinical social workers in the states where patients reside and provide care incident to the prescribing clinician. Navigator training consists of a structured 2–4 week onboarding period with a gradually increasing caseload under the oversight of a lead clinician at Kandu Medical Services. Training includes completing 31 standardized modules and Standard Operating Procedures across 9 Centers for Medicare & Medicaid Services-aligned competency domains, supplemented by stroke-specific content developed by Kandu, with competency assessments conducted before independent patient engagement.
These Navigators, who are clinicians or licensed specialists, provided structured support for postdischarge care, including medication adherence, blood pressure monitoring, scheduling and reminders for follow-up visits, rehabilitation referrals, risk factor management, addressing social determinants of health, and caregiver support.11,17 Telehealth sessions were delivered primarily via video visits, with phone, email, and in-app messaging as adjuncts. Sessions were conducted weekly initially and biweekly thereafter, targeting at least 60 cumulative min/month. Early sessions lasted approximately 60 min to cover transition to home, safety planning, risk mitigation, medication adherence, chronic condition management, and follow-up coordination. Follow-up sessions averaged 30 min, with additional time for patients with aphasia or complex needs. Asynchronous communication was available throughout. Each session included review of the care plan, health education, secondary prevention counseling, functional status and Activities of Daily Living assessment, evaluation of follow-up appointment completion, monitoring of Social Determinants of Health, and caregiver support.
This program was designed to optimize both clinical and psychosocial aspects of recovery. In contrast, patients in the retrospective cohort received standard postdischarge care without Kandu support.
DATA COLLECTION
Data were obtained from patient medical records and, for the prospective cohort, supplemented with information from Kandu Health. Extracted variables included patient demographics and clinical characteristics such as age, sex, race/ethnicity, insurance status, and chronic conditions. The primary outcome of interest was unplanned inpatient readmissions at 30 days. The 30-day readmission period was selected over 90 days because reimbursement policies and quality metrics primarily base their assessments on 30-day readmission rates, making it the most clinically and administratively relevant timeframe for outcome evaluation. Secondary outcomes included modified Rankin Scale (mRS) scores and National Institutes of Health Stroke Scale (NIHSS) scores at discharge and length of hospital stay. All data were securely stored on the local hospital’s secure network, with access restricted to the primary site principal investigator, and no patient identifiers were shared outside the study team.
STATISTICAL ANALYSIS
Continuous variables were assessed for normality using the Shapiro–Wilk test. Variables with a normal distribution are presented as mean ± standard deviation, and nonnormally distributed continuous variables are reported as median with interquartile range. Categorical variables are reported as counts and percentages (n [%]).
Baseline characteristics and clinical outcomes were compared across the three study groups: pretelehealth implementation, postimplementation enrollment and completion of the telehealth program, and postimplementation nonenrollment. For continuous variables, one-way ANOVA was used for normally distributed data, and the Kruskal–Wallis test was used for nonnormally distributed data. Categorical variables were compared using Pearson’s chi-square test or Fisher’s exact test, as appropriate.
Results
BASELINE DEMOGRAPHICS AND CLINICAL CHARACTERISTICS
A total of 405 patients were included in this study: 258 in the pretelehealth implementation cohort, 31 who enrolled in the postimplementation telehealth program with follow-up through 30 days, and 116 who did not enroll during the postimplementation period. Baseline demographic and clinical characteristics are summarized in Table 1 .
Baseline Demographic Characteristics of Pre- and Post-Telehealth Implementation Cohorts
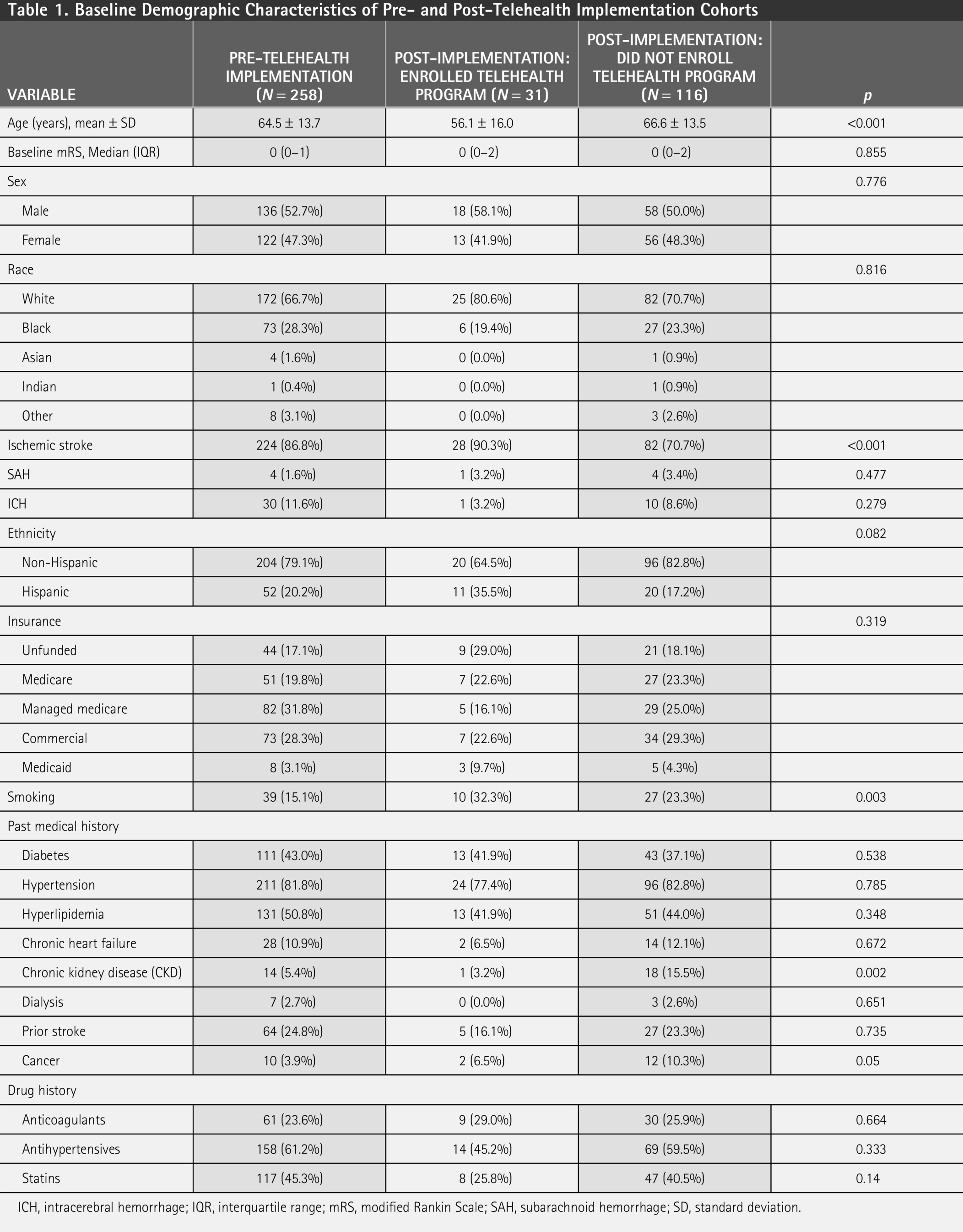
ICH, intracerebral hemorrhage; IQR, interquartile range; mRS, modified Rankin Scale; SAH, subarachnoid hemorrhage; SD, standard deviation.
The mean age was significantly lower in the telehealth-enrolled group (56.1 ± 16.0 years) compared with the preimplementation group (64.5 ± 13.7 years) and the postimplementation nonenrolled group (66.6 ± 13.5 years; p < 0.001). There were no significant differences in sex, race, or insurance status across the groups. Rates of smoking were higher in the telehealth-enrolled group (32.3%) compared with the preimplementation (15.1%) and nonenrolled (23.3%) groups (p = 0.003). Most other comorbidities, including diabetes, hypertension, hyperlipidemia, and chronic heart failure, were comparable across groups. However, chronic kidney disease (CKD) was less frequent in the telehealth-enrolled group (3.2%) compared with the preimplementation group (5.4%) and the nonenrolled group (15.5%; p = 0.002).
CLINICAL OUTCOMES
Compared with the pretelehealth implementation group, both postimplementation groups, patients enrolled in the telehealth program and those not enrolled, had higher mRS scores at discharge (p < 0.001), indicating greater disability. NIHSS scores did not differ significantly among the three groups (p = 0.265). Hospital length of stay was longer in both postimplementation groups than in the preimplementation group (p = 0.005). Notably, 30-day readmission rates were significantly lower postimplementation, with no readmissions among telehealth-enrolled patients and only 2.6% among nonenrolled patients, compared with 8.9% before implementation (p = 0.04). Clinical outcomes are presented in Table 2 .
Clinical Outcomes and 30-Day Readmission by Study Group
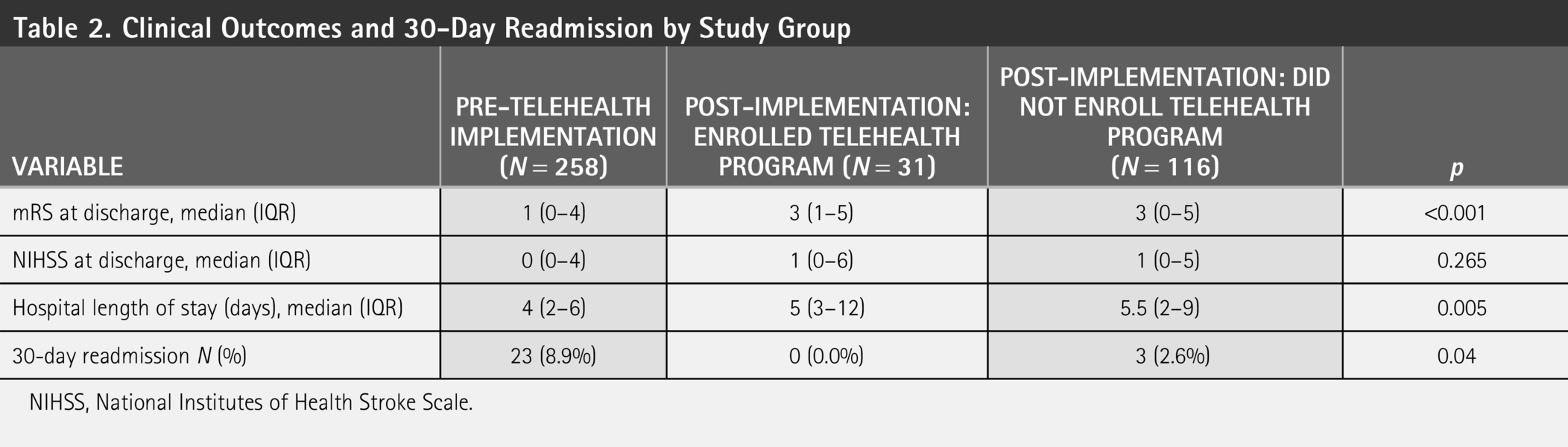
NIHSS, National Institutes of Health Stroke Scale.
30-DAY READMISSIONS
There were no 30-day readmissions among patients who enrolled in the telehealth program (0%, 95% confidence interval [CI]: 0–11.1%), compared with 8.9% (95% CI: 5.2–13.6%) in the preimplementation group and 2.6% (95% CI: 0.3–9.1%) in the postimplementation nonenrolled group (p = 0.04). Figure 2 illustrates the proportion of patients with 30-day readmissions across the study arms.
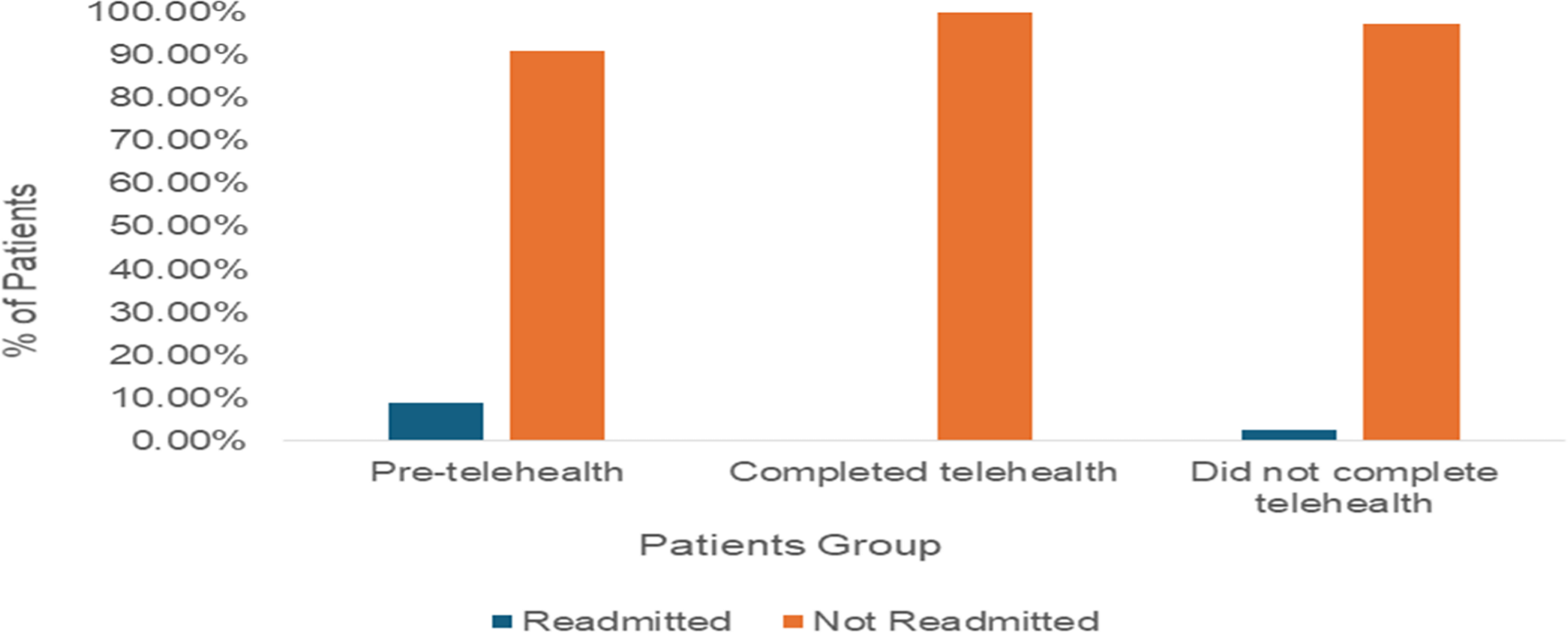
Proportion of patients with 30-day readmission across study arms. Telehealth completion was associated with zero readmissions.
LOGISTIC REGRESSION ANALYSIS
Multivariable logistic regression was performed to evaluate predictors of 30-day readmission. Due to zero readmissions in the telehealth-enrolled group, the odds ratio could not be reliably estimated for this group. Patients who did not enroll in the telehealth program showed a trend toward lower readmission rates than before implementation (odds ratio [OR]: 0.25, 95% CI: 0.04–1.62, p = 0.145
Discussion
The present study evaluates the impact of person-centered telehealth services on 30-day hospital readmission rates among stroke survivors. Our findings show a significant reduction in readmission rates following the implementation of the telehealth program. Notably, readmissions decreased from 8.9% in the retrospective preimplementation cohort to 2.6% in the overall postimplementation cohort, including 0% among patients actively enrolled in the telehealth program and 2.6% among patients who were not enrolled. This suggests that even patients who did not directly engage with the program had a lower readmission rate than the preimplementation cohort.
The observed reduction in readmissions, even among patients who did not enroll in the program, may reflect the broader effect of structured patient engagement during hospitalization. Extensive discussions emphasized the importance of follow-up care, timely medication adherence, and early recognition of warning signs, which likely contributed to improved postdischarge outcomes.
Our results are consistent with previous studies, which have shown the effectiveness of telehealth in reducing hospital readmissions among stroke patients. For instance, a survey by Hermosura et al. reported a 6.25% reduction in readmission rates among stroke patients using telehealth services, highlighting the potential of telehealth in poststroke care. 18 Similarly, a systematic review by Bilicki et al. found that outpatient follow-up visits, including telehealth, were associated with a 21% reduction in 30-day all-cause readmissions among stroke patients. 8
The experience at Emory Healthcare during the Coronavirus Disease 2019 pandemic provides complementary evidence. In that system, the implementation of telemedicine significantly increased 90-day poststroke follow-up rates from 19% before implementation to 41% afterward. 19 Although that study did not specifically measure readmission, it highlighted improved continuity of care, an outcome that may explain our observed reduction in readmissions.
While our study observed a significant reduction in readmission rates, some literature reports different outcomes. For example, Kolesnick et al. evaluated the impact of in-person and telemedicine transitions-of-care (TOC) stroke clinics at Thomas Jefferson University Hospital. The study reported a 30-day all-cause readmission rate of 5.8% overall, with a higher rate among patients followed via telemedicine (8.8%) than among those followed in person (2.1%; p = 0.038). Although their study demonstrated the overall value of TOC clinics for patients’ self-efficacy and confidence, it suggests that telemedicine follow-up alone may not always reduce readmissions. 20
These findings highlight the potential influence of program structure, patient engagement, and the specific telehealth intervention on outcomes. Our results suggest that the person-centered design of Kandu Health’s telehealth program, combined with structured inpatient education and proactive discharge planning, may have contributed to a reduction in readmissions even among patients who did not enroll in the program. The regression analysis reinforces that this association is statistically robust, independent of baseline demographics and clinical risk factors.
Beyond clinical outcomes, our findings also have significant financial implications for hospitals and health systems. Readmissions within 30 days incur substantial costs, including uncompensated care for uninsured patients and denied claims for insured patients. Although stroke is not currently included in the Hospital Readmissions Reduction Program, Medicare does reserve the right to deny claims for readmissions within 30 days of discharge (Medicare QIO Manual, Chapter 4, section 4240—Readmission Review, State Operations Manual Appendix A). This policy is broadly adopted by Medicare Advantage plans, 21 which cover slightly more than half of the Medicare population. Uninsured patients similarly generate uncollectable costs when readmitted. A statistical brief from Healthcare Cost and Utilization Project estimates the average cost of 30-day all-cause readmissions after circulatory system diseases to be $17,700 per readmission, 22 while published meta-analyses and Monte Carlo simulations estimate the mean cost of 30-day readmissions across all conditions at $16,037.08. 23 Applying these estimates to our observed 6.3% reduction in same-center 30-day readmissions suggests a potential annual savings of $112,259–$123,900 in avoided uncollectable costs for uninsured patients and $545,261–$601,800 in reduced exposure to denied claims for insured patients in a 1,000-patient stroke service line. These findings highlight that postdischarge telehealth programs not only decrease readmissions but may also alleviate the substantial economic burden associated with poststroke readmissions.
This study has several strengths. It is one of the first to evaluate the real-world impact of a structured telehealth program specifically designed for stroke survivors on readmission outcomes. Unlike many prior studies, our design included both a retrospective preintervention cohort and a prospective postintervention cohort. The inclusion of patients who did not enroll in the telehealth program but still demonstrated reduced readmissions provides insight into the effect of structured discharge education and follow-up discussions. The prospective data collection enhances the validity of our findings for the postimplementation group by reducing recall bias and enabling more accurate outcome capture. In addition, the sample included both ischemic and hemorrhagic stroke patients, enhancing the relevance of the results to diverse clinical populations. Ultimately, the significant reduction in readmissions is clinically meaningful for both patients and health systems, given the financial penalties and resource strain associated with unplanned readmissions.
LIMITATIONS
Several limitations should be considered when interpreting these findings. The study was not randomized, and although all patients were offered enrollment after telehealth program implementation, patients were not directed to participate, limiting assessment of barriers to adoption and the maximum achievable uptake. Outcomes were not stratified by engagement level, which limited our ability to isolate the independent effect of telehealth participation from potential cointerventions. As with any observational study, selection bias may be present, as patients at lower risk of readmission may have been more likely to enroll in the virtual telehealth program. Importantly, direct patient-level cost data were not collected; therefore, the estimated economic impact reflects modeled cost savings derived from published literature rather than observed financial outcomes within our health system. The single-center design may limit generalizability to other health care settings, particularly those with different payer structures or patient demographics. Finally, although sufficient to detect statistically significant differences, the sample size was modest compared with national stroke registries. Future studies should incorporate randomized designs and larger multicenter cohorts to confirm these findings and to evaluate long-term clinical and economic outcomes.
Conclusion
The implementation of a person-centered telehealth service was associated with lower 30-day readmission rates among stroke survivors. These findings highlight the importance of integrating structured discharge education with personalized telehealth to enhance poststroke outcomes, improve care continuity, and reduce hospital burden.
Authors’ Contributions
M.E.: Conceptualized and designed the study, supervised data collection, and critically revised the article; A.A.M.: Contributed to the statistical analysis, interpretation of results, and drafting of the article; E.A. and L.M.: Contributed to data collection. R.E., Z.A., R.W., L.G., M.E.-G., and Y.J.A.: Contributed to article drafting and revision. All authors reviewed and approved the final article and agreed to be accountable for all aspects of the work.
Ethical Considerations
This research activity was determined to be exempt or excluded from IRB oversight in accordance with current regulations and institutional policy. Our internal reference number for this determination is 2024-909. All research materials provided herein, in whole or in part, are subject to copyright protection by HCA Healthcare and/or one of its subsidiaries. All rights reserved.
Consent to Participate
Informed consent was waived because the study involved analysis of fully anonymized data. No identifiable patient information was accessed, and individual participants could not be identified at any stage of the study. In accordance with institutional and ethical guidelines, the use of anonymized data did not require informed consent.
Data Availability
Data will be available upon request and approval from the primary institution.
Disclaimer
This research was supported (in whole or in part) by HCA Healthcare and/or an HCA Healthcare-affiliated entity. The views expressed in this publication represent those of the authors and do not necessarily represent the official views of HCA Healthcare or any of its affiliated entities.
Footnotes
Acknowledgments
The authors gratefully acknowledge Kirsten Carroll and Seth Wilk (Kandu Health, Los Angeles, CA) and Gregory E. Wilding, PhD (University at Buffalo, The State University of New York), for their assistance in coordinating the logistics of providing our hospital with the Kandu service and for supplying valuable references regarding patient reimbursement and statistical considerations relevant to our independent study.
Disclosure Statement
Kandu Health provided its services to our hospital at no charge but was not involved in the study design, patient screening, data analysis, or the interpretation of results. M.E. has a small investment in Galaxy Therapeutics and serves as a consultant and/or speaker for Stryker, Viz.ai, and Imperative Care. The remaining authors declare that they have no conflicts of interest.
Funding Information
This research received no external funding.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.