
Abstract
Background:
Evidence assessing rural older cancer survivors’ patient portal use is limited. To this end, we analyzed My Chart messages among this group to reveal key insights into their patient portal use.
Methods:
We conducted a retrospective qualitative chart review of MyChart messages from cancer patients aged at least 65 years and from rural ZIP codes receiving care at an urban hospital from March 1, 2020, to May 25, 2023.
Results:
The resulting sample consisted of 860 coded messages from 411 patients. The qualitative analysis yielded 1,295 coded occurrences, from which nine themes emerged. The most frequent coded messages were identified as Ongoing Clinical Care Concerns (n = 464) and Supportive Care (n = 128). The least frequently coded theme was Requesting telehealth (n = 35).
Conclusion:
Our analysis of MyChart messages of rural older cancer survivors demonstrates high engagement with MyChart messaging and has implications for the use of tailored patient portal designs for this uniquely vulnerable patient population.
INTRODUCTION
Despite an inverse relationship between telehealth adoption and age, cancer care teams are increasingly integrating telehealth into cancer care.1–5 This is particularly important because aging is a major risk factor for many types of cancers. 4 Older cancer survivors (aged at least 65 years old) with complex care plans and barriers to using telehealth are uniquely vulnerable to poor care coordination, worse cancer outcomes, and reduced quality of life. 6 These risks intensify for rural older cancer survivors, with limited broadband infrastructure and technology usability challenges.
Rural older cancer survivors often reside in health professional shortage areas and face financial and travel burdens accessing care in distant urban centers. While COVID-19 policies increased rural clinics’ telehealth uptake by 70% from 2019 to 2022; 7 rural older cancer survivors still reported a lower probability of telehealth availability than their urban counterparts (53% vs. 63%). 8 Consequently, rural older cancer survivors constitute a clinically significant population facing a convergence of vulnerabilities, including rural residence, older age, an increasingly digitized health care landscape, and complex care plans.
Patient portal use—a measurable outcome of telehealth engagement—is positively associated with increased cancer screening and patient engagement.9–12 MyChart, an Epic System’s patient portal, enables patients to view medical records, pay bills, and exchange secure messages with their health care providers. 13 Messaging is its most used feature, with 60% of the portal’s users engaging with this feature. 14 Relating to the clinical significance of patient portal utilization, patient portal messaging is positively associated with breast cancer outcomes, improved breast screening behaviors, and increased reporting of previsit patient-reported outcomes.11,12 While younger and more urban adults are more likely to use MyChart Messaging, older adults consider this feature helpful in communicating their clinical care, billing needs, and appointment scheduling. 15
While portal engagement is used to measure telehealth engagement among clinically significant populations, 15 little is known about rural older cancer survivors’ engagement with these platforms. Given that telehealth is embedded in the rural health care tapestry and that patient portals are an effective measure of telehealth engagement, we aim to assess rural older cancer survivors’ utilization by analyzing MyChart Messages of rural cancer survivors who receive care from a large, urban, academic health center. These data may reveal key insights into their technological and cancer survivorship care needs, important to develop interventions and programs to increase patient portal usability among this population. To achieve this, we applied a systematic review methodology to sort the messages and then applied a qualitative thematic approach to assign themes for each message.
METHODS
This cross-sectional retrospective chart review was approved by the Northwestern University Institutional Review Board (IRB# STU00218312). A team of researchers reviewed MyChart messages from patients at least 65 years old, from a rural zip code defined by the rural-urban commuting area codes, 16 written from March 1, 2020, to May 29, 2023, and a patient of a large, urban, academic health center. A block group of ICD codes was used that included all cancer types in this data analysis. All MyChart messages were electronic communications initiated by the patient or their proxy from MyChart tethered to the Epic Systems Corporation’s Electronic Health Records.
Using an Excel database, trained pairs of reviewers screened MyChart messages, aggregated redundant or broken threads, and removed duplicate messages. Protected health information was redacted, including patient or caregiver names, local addresses, and other personal identifiers, to ensure patient confidentiality. Caregivers were identified as individuals other than the patient or provider who either self-identifies or are referenced within the MyChart message.
Another team of paired reviewers screened and double-coded deidentified MyChart messages using a thematic analysis approach (L.B., A.H., K.F., and B.P.). Messages were double-coded to improve the findings’ reliability. 17 Each message was assigned codes or subcodes inductively—developing codes as the messages were read— to identify salient content. 18 The coding team conducted regular consensus meetings to compare and discuss emergent codes, develop the codebook, and monitor thematic saturation–a qualitative review process in which text is coded until no new information is found. 19 Discrepancies were reviewed by a qualitative expert (M.W.L.).
RESULTS
Between March 1, 2020, and May 29, 2023, 2055 individual messages were submitted by rural older cancer survivors and/or their caregivers to a provider. The average number of communicated messages per patient was 88.8 ± 123.2 messages over an average of 53.5 ± 57.6 days ( Table 1 ). The resulting coded sample included 860 coded messages from 411 patients, with a mean age of 73.3 ± 6.2 years. Of this sample, 54.3% self-identified as female; 87.6% identified as Non-Hispanic White; and 73.2% were married. Most patients’ primary health insurance was Medicare (68.4%) or Medicare Advantage (22.9%). The mean Charlson score was 3.2 ± 2.9.
Participant Demographic Characteristics (N = 411)

*p ≤ 0.05.
Our qualitative analysis resulted in 1,295 coded occurrences. Relevant coded messages were grouped into nine themes ( Fig. 1 ). A single message could be coded multiple times. Table 2 displays the themes, subthemes, exemplar quotes, and frequency of occurrence for each subtheme. Of the nine themes, the most frequently coded themes were Ongoing Clinical Care Concerns (n = 464); Tangential content (n = 268); Supportive Care Concerns (n = 128), and Scheduling (n = 98).
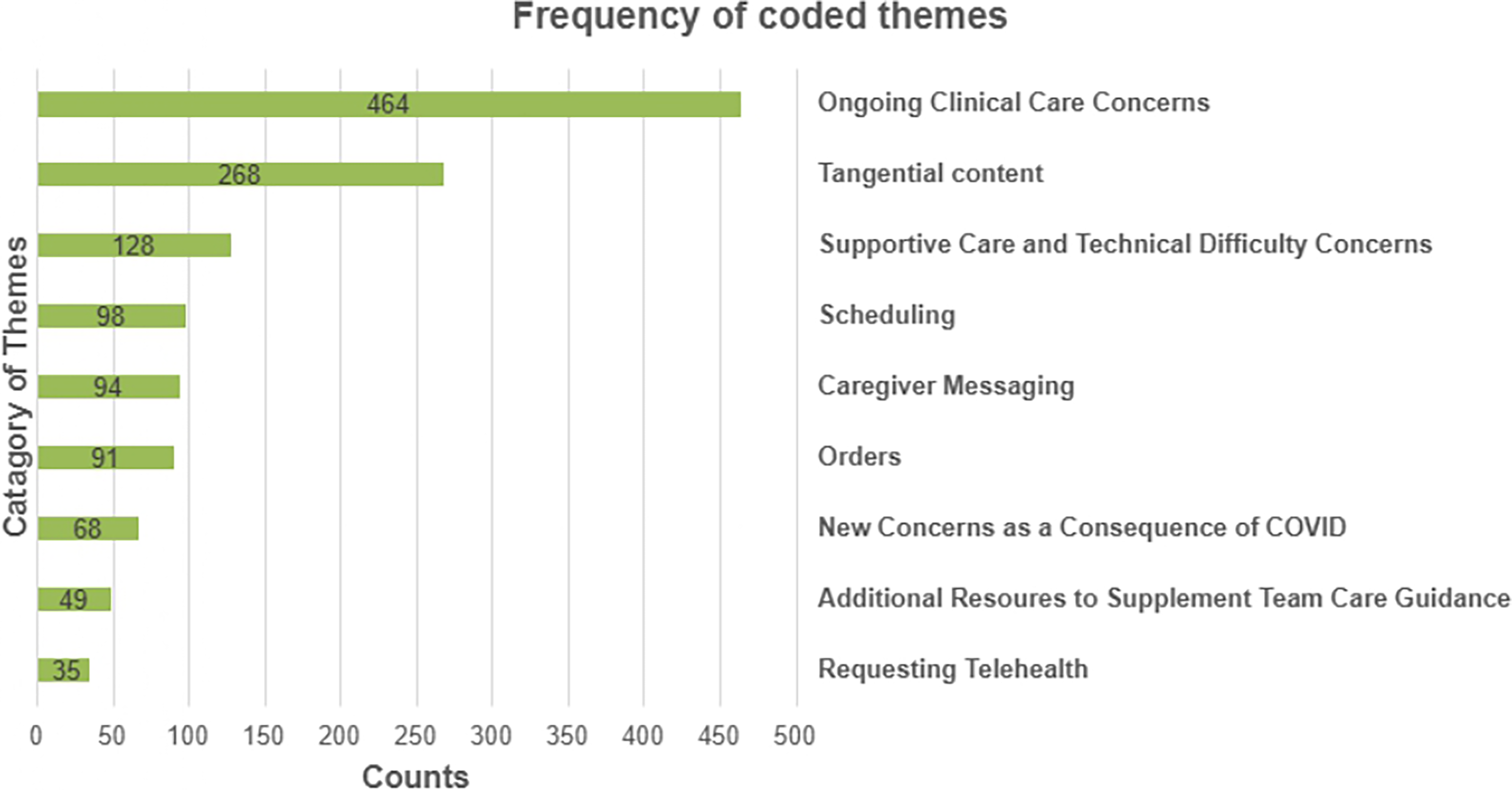
MyChart Message Counts for each category of codes.
Codes, Subcodes, Frequency, and Corresponding Exemplar MyChart Messages (N = 1,295)

The theme Ongoing Clinical Care Concerns (n = 464) described messages that generally require some interpretation or action from the clinical care team. The six subthemes populating this theme are symptom management, medication changes and symptoms, communicating a need for personal health information, discussion of test results, treatment follow-up, and acute pain needs. For example, a patient questioned, “Will you call me and advise follow-up when you have the results?
Notably, the second most common theme was identified as Tangential content (n = 268), composed of messages that are tangential to the study aim and include exclamations (e.g., thanks), pre-clinic visit test results, and billing updates (e.g., I will be paying this bill by April 8th).
Messages coded as Supportive Care included emotional, technical, and financial needs (n = 128). These messages focused on the quality of life and technical support needs and concerns of patients. The eight subthemes are logistics and access, acquiring medications, insurance coverage, identifying emotional concerns, technical navigation, patient portal technical difficulties, financial burden of health care, and miscommunication with telehealth/digital. Examples of these messages might describe the patient as “nervous”, “overwhelmed”, or unable to “financially afford” their care. One patient wrote, “At our upcoming appointment, I’d like to discuss the impact of work-related stress on my diabetes and emotional health.”
Messages pertaining to establishing, changing, or canceling appointments were coded to the Scheduling theme (n = 98). For example, a patient commented that, “Dr. [name] states okay to schedule MRI lumbar spine.”
In brief, less frequently reported message themes include messages written by a patient supporter, identified as Caregiver Messaging (n = 94), which included two subthemes: caregiver communicates with the health care team and patient requests to include caregivers. The Orders theme (n = 91) also included two subthemes: lab orders and ordering test results. Messages concerning health care needs associated with Covid-19 were identified as New Concerns as a Consequence of Covid-19 (n = 68). This theme included three subthemes: recommendations about vaccines, requesting a telehealth visit related to COVID-19, and requesting an alternative to an in-person visit due to COVID-19. The theme Additional Resources to Supplement Care Team Guidance (n = 49) describes messages that emphasize the need to connect patients with appropriate resources, providers, and services based on their geographic location and social needs. This theme is comprised of three subthemes: new care team providers, geographically appropriate referrals, and requesting navigation of social needs. The least frequent theme was Requesting Telehealth (n = 35), which included messages overcoming travel and technology (e.g., desktop rather than smartphone) burdens and requesting a telehealth appointment with a provider. Subthemes for this theme were unspecified reasons for telehealth, related to distance, provider requested. Additional exemplar quotes for themes and subthemes are detailed in Table 2 .
DISCUSSION
Our findings provide deeper insights into the content discussed between rural older cancer survivors and their providers via MyChart messaging. This study identified that rural older cancer survivors primarily use MyChart messaging for ongoing clinical and supportive care concerns. Our findings align with a pre-pandemic MyChart Message analysis of older adults, which reported clinical issues and scheduling as the most frequent concerns. Unlike that study, our data reveals an emerging emphasis on supportive care concerns (e.g., quality of life) as the third most frequent coding theme. 15 This focus on supportive care needs punctuates an increased focus on psychosocial aspects of cancer care by providers and hospital systems. For rural residents, this is particularly important given the dearth of specialized and supportive care resources in rural areas. A study using 2017–2018 data reported that rural cancer patients were less likely than urban patients at the same hospital to use and value supportive care services. 20 These disparities, in part, contribute to persistent gaps in rural-urban survivorship outcomes and reduced survivorship rates for rural cancer patients. Although an examination of disparities was beyond the scope of this study, our evidence signals a potentially growing awareness and use of supportive care services among rural cancer patients.
Notably, our findings have implications for the broader discussion of billing for patient-provider electronic communication. While billing for electronic messages may incentivize concise messaging and reduce provider burnout, it could disproportionately burden rural residents in medically underserved areas. Findings from this study revealed that, on average, rural older cancer survivors had nearly 89 communicated messages between their providers; these data illuminate the usefulness of MyChart messaging for rural older adults. Given that most rural counties are designated health professional shortage areas, this study underscores the need for policies that keep MyChart free and accessible to improve access to care for rural residents. It is, however, important to understand that m-health technology utilization is strongly associated with healthier outcomes. In an analysis of 2019 HINTS data, older adults who used online patient-provider communication were also associated with having higher health literacy and health self-efficacy, as well as improved quality of life indicators. 21 To this end, continued investment for extending high-speed internet should be complemented by clinical and community-based programming that strengthens telehealth usability, which is critical to impact health outcomes for the most vulnerable rural and remote communities.
LIMITATIONS
This research has several notable strengths. Our sample size and thematic analytic approach yielded a robust sample of messages, enabling the research team to draw thematic conclusions of a uniquely vulnerable population. Additionally, the data were double-coded by pairs of medical students in a rural medicine program. Their perspectives strengthened credibility and enhanced the reliability of our findings—a qualitative strategy known as reflexivity. 22 However, findings may not generalize beyond a majority Non-Hispanic White rural older population receiving care from an urban hospital. Future studies should analyze MyChart messages of racial and ethnic minoritized rural older adults. Additionally, this chart review did not include income, education, and employment data, as it was not collected within the health records. Insurance was gathered as a proxy for these variables. Future studies will need to prioritize data sets that include these important social determinants of health. Lastly, prior research reports that most older adults have caregiver assistance using patient portals, raising the possibility that caregiver messages were underreported in the current study. 23 We identified caregiver messages if the messenger self-identified as other than the patient, and caregiver messages that were written assuming the patient’s identity could not be distinguished. A future prospective longitudinal study would reveal nuances in caregiver and older adult patient portal practices.
CONCLUSIONS
In this retrospective chart review of MyChart patient portal messages initiated by rural older cancer survivors, patients most discussed clinical and supportive care concerns. The findings reveal real-time health concerns experienced while living in a medically underserved area and relying on patient portals as a readily used health care resource, as well as limited access to broadband internet.
Authors’ Contributions
A.H., L.B., K.F., B.P., and P.D. contributed to the analysis and interpretation of the data and preparation of the article. M.L. developed the study concept and design, acquired subjects’ data, contributed to the analysis and interpretation, and helped prepare the article.
Footnotes
Ethical Considerations
This retrospective chart review was approved by the institutional review board at Northwestern University (STU00218312). In accordance with federal regulations (45 CFR 46.116), the Institutional Review Board granted a waiver/alteration of the informed consent process, as the study involved minimal risk to participants, the waiver did not adversely affect participants’ rights or welfare, and the research could not be practicably carried out using the standard consent procedures.
Data Availability
Data are available on request.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Dr. Lewis was supported by a grant from the National Cancer Institute (PI: Lewis,