
Abstract
Marshall Medoff and Christopher Dennis identify some errors in National Abortion Rights Action League’s (NARAL) data on the effective start dates of various state-level antiabortion laws. However, they misunderstand the purpose of my 2011 State Politics and Policy Quarterly article which was to measure the impact of a range of antiabortion laws—not analyze competing theories as to why the abortion rate has fallen in the United States. Furthermore, their analysis contains a number of critical measurement, and methodological and estimation errors. When these errors are corrected, the empirical results add to the substantial body of peer-reviewed research which finds that public funding restrictions, parental involvement laws, and properly designed informed consent laws all reduce the incidence of abortion.
Keywords
Marshall Medoff and Christopher Dennis identify some errors in the data set of antiabortion laws that I used in my 2011 State Politics and Policy Quarterly article “Analyzing the Effect of Anti-Abortion U.S. State Legislation in the Post-Casey Era.” Nearly all of the errors that Medoff and Dennis identify came from NARAL’s (various years) Who Decides? publication. Data from NARAL are frequently used by political scientists who are interested in researching state-level variation in abortion policy (Arceneaux 2002; Bowler and Donovan 2004; Burden 2005; Gerber 1996; 1999). Unfortunately, it is apparent that NARAL did not always draw proper distinctions between laws that were passed and laws that were actually being enforced. In particular, many antiabortion laws were periodically not in effect due to various legal challenges. NARAL’s reporting, particularly on state-level informed consent laws, often failed to reflect this.
That having been said, my data set of state-level public funding restrictions and parental involvement laws was fairly accurate. Most of the errors identified by Medoff and Dennis in my data set of public funding restrictions and parental involvement laws were due to relatively small differences in the specific enforcement dates of these laws. A few errors occurred because in some cases, scholars, antiabortion groups, and abortion rights groups disagree about whether a relatively weak law actually constitutes an antiabortion law. Overall, these errors fail to substantively affect my findings on the impact of either parental involvement laws or public funding restrictions.
Furthermore, the data set of antiabortion laws used by Medoff and Dennis also contains a substantial number of errors. In particular, many antiabortion laws do not go into effect the day judicial decisions are issued. Often, there are additional legal appeals. Other times, there is a grace period to give abortion providers and state health department administrators time to prepare for the implementation of the law. An examination of local media coverage provided accurate enforcement dates for many state-level antiabortion laws. Overall, when these errors in the data set used by Medoff and Dennis are corrected, the empirical results add to the substantial body of peer-reviewed research which finds that public funding restrictions, parental involvement laws, and properly designed informed consent laws all reduce abortion rates.
This article proceeds as follows. The first section will provide a review of the academic literature, which analyzes the impact of abortion restrictions. The second section will provide a correction of the errors in the Medoff–Dennis data set of state-level antiabortion laws. In the third section, I will discuss the methodological concerns put forth by Medoff and Dennis and analyze the corrected data set of state-level antiabortion laws. The fourth section will analyze factors that might be responsible for the long-term abortion decline in the United States. The fifth section will conclude the article.
Literature Review
Medoff and Dennis are correct that various antiabortion groups have used my research to argue for the effectiveness of antiabortion laws. However, these groups have also drawn upon a very broad body of economic and public health research that also documents the effectiveness of various abortion restrictions. Interestingly, Medoff and Dennis only cite a small fraction of the studies that have looked at the issue. In reality, there is a substantial body of research that has analyzed the impact of both public funding restrictions and parental involvement laws. There is also a small but growing body of research analyzing the impact of antiabortion informed consent laws. A summary of the relevant literature is below.
Public Funding Restrictions
A 2009 Guttmacher Institute literature review identified 18 peer-reviewed studies that analyzed the impact of state Medicaid funding restrictions on the incidence of abortion (Henshaw et al. 2009). These methodologically diverse studies used abortion data from a variety of sources. Overall, of the 18 studies they considered, 15 found statistically significant evidence that abortion rates fell after Medicaid funding was reduced. 1
This finding held for studies using time-series cross-sectional data to analyze overall abortion rates (Blank, George, and London 1996; Haas-Wilson 1993; 1997; Hansen 1980; Levine, Trainor, and Zimmerman 1996; Matthews, Ribar, and Wilhelm 1997; Medoff 2007; Meier et al. 1996; Meier and McFarlane 1994). It also held for studies using time-series cross-sectional data to specifically analyze teen abortion rates (Haas-Wilson 1996; Lundberg and Plotnick 1990; Medoff 1999; 2007). This held as well for studies that analyzed abortion rates in smaller groups of states (Korenbrot, Brindis, and Priddy 1990; Trussell et al. 1980) and for two studies that specifically analyzed the impact of public funding restrictions on pregnancy outcomes in North Carolina (Cook et al. 1999; Morgan and Parnell 2002).
The studies that analyzed data from North Carolina were especially interesting. From 1980 to 1995, North Carolina publicly funded abortion for low-income women—not through Medicaid but through a state abortion fund that periodically ran out of money. Whenever funds were depleted, the researchers found there were statistically significant decreases in the abortion rate, and months later, statistically significant increases in the birthrate (Cook et al. 1999; Morgan and Parnell 2002). These findings were statistically stronger when the pregnancy outcomes for African American women were considered. Overall, Cook et al. concluded that 37% of the women who would have otherwise had an abortion carried their child to term when funding was not available.
Overall, the authors of the Guttmacher literature review acknowledge that the best research indicates that Medicaid funding restrictions reduce the incidence of abortion. In the discussion that follows the literature review, they state that the best studies . . . used detailed data from individual states and compared the ratio of abortions to births both before and after the Medicaid restrictions took effect. These found that 18-37 percent of pregnancies that would have ended in Medicaid funded abortions were carried to term when funding was no longer available. (Henshaw et al. 2009, 27)
They state that the Cook and Parnell study that analyzed data from North Carolina had the “best design.” They conclude by stating that “considering the case studies collectively, reasonable estimate is that a lack of funding influences a quarter of Medicaid eligible women to continue unwanted pregnancies” (Henshaw et al. 2009, 27).
Parental Involvement Laws
A 2009 Guttmacher Institute literature review identified 16 peer-reviewed studies that analyzed the impact of parental involvement laws on minor abortion rates (Dennis et al. 2009). I was able to identify three additional peer-reviewed studies for a total of 19 studies. 2 Each of these 19 studies finds that parental involvement laws result in a statistically significant decline in the in-state abortion rate for minors. 3
This is true of studies that analyze time-series cross-sectional data on minor abortion rates (Haas-Wilson 1993; 1996; Levine 2003; Medoff 2007; New 2007; 2009; 2011; Ohsfeldt and Gohman 1994; Tomal 1999). It is also true of studies that focus on the impact of individual state-level parental involvement laws. There have been separate studies analyzing the laws in eight states, including Indiana (Ellertson 1997), Massachusetts (Cartoof and Klerman 1986; Donovan 1983), Minnesota (Donovan 1983; Ellertson 1997; Rogers et al. 1991), Mississippi (Henshaw 1995; Joyce and Kaestner 2001), Missouri (Ellertson 1997; Pierson 1995), South Carolina (Joyce and Kaestner 1996; 2001), Tennessee (Joyce and Kaestner 1996), and Texas (Colman, Joyce, and Kaestner 2008; Joyce, Kaestner, and Colman 2006).
The findings are very similar. After the passage of a parental involvement law, the research shows that there is a statistically significant reduction in the in-state minor abortion rate anywhere from 13% (Henshaw 1995) to 42% (Cartoof and Klerman 1986). Most studies found a decline in the in-state minors’ abortion rate ranging from 15% to 20% (Colman, Joyce, and Kaestner 2008; Ellertson 1997; Haas-Wilson 1996; Joyce, Kaestner, and Colman 2006; Levine 2003; New 2011; Ohsfeldt and Gohman 1994; Tomal 1999).
There is an ongoing debate about to what extent these in-state minor abortion declines are offset by out-of-state increases. Some studies find that these laws result in a significant increase in the number of minor girls seeking abortions in adjacent states where the laws are more permissive (Cartoof and Klerman 1986; Ellertson 1997; Henshaw 1995; Joyce and Kaestner 2001). Other studies find little evidence that a significant number of minor girls circumvent these laws by obtaining abortions in nearby states (Blum, Resnick, and Stark 1987; Joyce, Kaestner, and Colman 2006; Rogers et al. 1991).
However, the two best studies on parental involvement laws that track, and compare, both in-state and out-of-state minor abortions, each show that the in-state abortion decline significantly exceeds the out-of-state increase. The first is “Parental Consent for Abortion: Impact of the Massachusetts Law.” This study appeared in the American Journal of Public Health in 1986 and analyzed the Massachusetts parental involvement law that took effect in 1981 (Cartoof and Klerman 1986). The second is “Changes in Abortions and Births and the Texas Parental Involvement Law.” This study appeared in The New England Journal of Medicine in 2006 and analyzed the Texas parental involvement law that took effect in 2000 (Joyce, Kaestner, and Colman 2006). Both studies were unique because they were able to analyze monthly data on in-state minor abortions, out-of-state minor abortions, and births to minors.
These studies found that after the enactment of both the Massachusetts law and the Texas law, the in-state abortion decline clearly exceeded the out-of-state of increase. Furthermore, both studies found evidence of short-term increases in the minor birthrate. The Texas study found statistically significant increases in the birthrate of minors who were above 17 and half years old when they conceived (Joyce, Kaestner, and Colman 2006). Another Texas study that analyzed similar data found that the birthrate for 17-year-olds increased by 2% after the parental involvement law took effect (Colman, Joyce, and Kaestner 2008). The Massachusetts study suggests that in the year after the parental involvement law took effect, anywhere from 50 to 100 minors gave birth—instead of having abortions—as a result of the law (Cartoof and Klerman 1986).
Additional evidence pointing to the effectiveness of parental involvement laws comes from research indicating that the presence of a parental involvement law improves health outcomes for teen girls. A 2003 study in the Journal of Health Economics (Levine 2003) found that parental involvement laws reduce the pregnancy rate of 15- to 17-year-olds by 4% to 9%. A 2008 study in the Journal of Law Economics & Organization shows that parental involvement laws reduce the gonorrhea rate anywhere from 12% to 20% for females under 20 (Klick and Stratmann 2008). Finally, the journal Economic Inquiry published a study which shows that the enactment of parental involvement laws is associated with an 11% to 21% reduction in the number of 15- to 17-year-old females who commit suicide (Sabia and Rees 2013).
Informed Consent Laws
Medoff and Dennis consistently misinterpret the Joyce et al. (2009) literature review on the impact of informed consent laws. Of the 12 studies that Joyce et al. analyze, only six examine the impact of informed consent laws on the incidence of abortion. The other six studies look at the impact of informed consent laws on suicide rates and other public health outcomes.
Of those six studies, three studies specifically analyze the impact of Mississippi’s informed consent law that took effect in 1993 (Althaus and Henshaw 1994; Joyce, Henshaw, and Skatrud 1997; Joyce and Kaestner 2000). This law was unique because it was the first that required women seeking an abortion to make two separate trips to the abortion clinic. Each of the three studies found that this informed consent law resulted in a statistically significant abortion rate reduction (Althaus and Henshaw 1994; Joyce, Henshaw, and Skatrud 1997; Joyce and Kaestner 2000).
The three other studies included in this literature review use a time-series cross-sectional approach. They all find that informed consent laws only had a marginal impact on the incidence of abortion. However, these three studies all have methodological shortcomings. They include one study that analyzed only three years of data (Medoff 2007), one study whose data set ended in 1992—before many of the stronger Casey-style informed consent laws took effect (Meier et al. 1996)—and one that analyzed only the subset of informed consent laws that contained waiting periods (Bitler and Zavodny 2001). A fourth study, not included in the Guttmacher literature review, is limited because it only analyzes one year of abortion data (Medoff 2009).
Overall, the existing research on informed consent laws provides solid empirical evidence that Mississippi’s informed consent law—which requires that women seeking abortions make two separate trips to the abortion provider—has reduced abortion rates. The current research provides very little information on the impact of other types of informed consent laws.
Other Research
There exists other research which finds that the incidence of abortion is affected by its legal status. For instance, a study analyzing changes in abortion policy in Eastern Europe after the fall of communism found abortion restrictions reduced abortion rates by around 25% (Levine and Staiger 2004). A recent National Bureau of Economic Research study found that in 1971 and 1972, state abortion rates were significantly affected by both the legal status of abortion in their own state and their distance to New York which in 1970 became one of the first states to legalize abortion (Joyce, Tan, and Zhang 2012). Finally, a recent study analyzed a Texas law which required that all abortions taking place at or after 16 weeks of gestation be performed in either a hospital or an ambulatory surgical center. It found that this law reduced the number of abortions performed in Texas at or after 16 weeks of gestation by 88%. While there was an increase in the number of Texas residents seeking late-term abortions in other states, the out-of-state increase failed to offset the in-state decline (Colman and Joyce 2011).
Correcting Medoff and Dennis’ Data Set of State-Level Antiabortion Laws
Medoff and Dennis go through my data set of state-level antiabortion laws and cite several errors. Most of the errors they find are due to the fact that NARAL did not track state-level antiabortion informed consent laws prior to 1992 and the fact that NARAL often did not draw appropriate distinctions between laws that were passed and laws that were being enforced. Other errors they find involve situations where researchers, antiabortion groups, and abortion rights groups disagree about the presence or absence of an antiabortion law. Still other errors reflect relatively small discrepancies in the precise enforcement dates of the various antiabortion laws.
Furthermore, Medoff and Dennis make a substantial number of mistakes on their own. Although they fail to acknowledge it in their article, their enforcement dates for one parental involvement law (Arizona), two public funding restrictions (Connecticut, 4 Minnesota), and three informed consent laws (Pennsylvania, Ohio, Indiana) are correct only because I provided them with this information during the review process. In addition, their enforcement dates for a very high percentage of informed consent laws are also incorrect. Very often, antiabortion laws do not go into effect the day judicial decisions are issued. Often, there are additional legal appeals. Other times, there is a grace period to give abortion providers and the state health department time to prepare for the implementation of the law. A listing of the errors found by Medoff and Dennis with my comments is shown below.
Parental Involvement Laws
1. Arizona
In my 2011 State Politics & Policy Quarterly (SPPQ) article, I originally listed a March 2003 enforcement date for Arizona’s parental involvement law and coded its enforcement date as March 2, 2003. Medoff and Dennis’ original SPPQ submission listed the start date for Arizona’s law as October 9, 2002. They only were able to obtain the correct March 4 start date (Associated Press 2003b) because I provided them this information during the review process. Overall, a two-day difference in the enforcement date is a trivial error.
2. Idaho
Medoff and Dennis are incorrect that Idaho never had a parental involvement law in place. A parental involvement law was signed into law by Idaho Governor Dirk Kempthorne on February 22, 2000 (Fick 2000; Spokesman Review 2000). After some legal challenges, on September 1, 2000, a judge blocked enforcement of what he said were overly restrictive portions of the law but allowed the law to take effect (Warbis 2000). This law remained in effect until July 16, 2004, when the 9th Circuit Court of Appeals struck it down (Fick 2004; Spokesman Review 2004). Overall, Idaho had a parental involvement law in place from September 1, 2000, to July 16, 2004. Idaho’s Parental Involvement Law value should have been .33424 in 2000; 1 in 2001, 2002, and 2003; and .54098 in 2004. 5
3. Connecticut
In 1990, Connecticut enacted a law which requires that a physician or a counselor give minors objective information about abortion and its alternatives and discuss the “possibility” of involving her parents or other adult family members in her decision making. NARAL listed Connecticut as a state with a parental involvement law every year from 1990 to 1997 in their annual Who Decides? publication. Then starting in 1998, Who Decides? quit listing Connecticut as a state with a parental involvement law. Some academic studies have considered Connecticut as a state with a parental involvement law (Blank, George, and London 1996; Levine 2003; Ohsfeldt and Gohman 1994). However, considering that the Connecticut statute does not explicitly require that a minor seeking an abortion involve her parents—it is probably best to consider Connecticut as a state without a parental involvement law.
Summary
My 2011 SPPQ study analyzed 36 states with parental involvement laws. Only two, nontrivial errors were found in the data set—and these were in states where there exists disagreement among scholars, antiabortion groups, and abortion rights groups about the presence or absence of these parental involvement laws. Overall, my 2011 SPPQ article coded 98.5% of state years correctly.
Public Funding Restrictions
1. Arizona
Medoff and Dennis are correct that in 2002, the Arizona Supreme Court ruled that Arizona must fund medically necessary Medicaid abortions. However, in practice, Arizona funds very few abortions through Medicaid. In FY 2006 Arizona only paid for seven abortions through Medicaid (Sonfield, Alrich, and Gold 2008). In FY 2010, Arizona only paid for 13 abortions through Medicaid (Sonfield and Gold 2012). In both of these years, less than 0.2 percent of abortions performed in Arizona were paid for by Medicaid. As Table 1 indicates, Arizona pays for a much smaller percentage of abortions than do other states which fund medically necessary abortions through Medicaid. As such, it seems appropriate to code Arizona as a state where public funding of abortions is restricted. My 2011 SPPQ article was correct. Arizona’s Medicaid funding restrictions variable should be scored a 1 from 1985 to 2005.
Percentage of Abortions Funded through Medicaid.
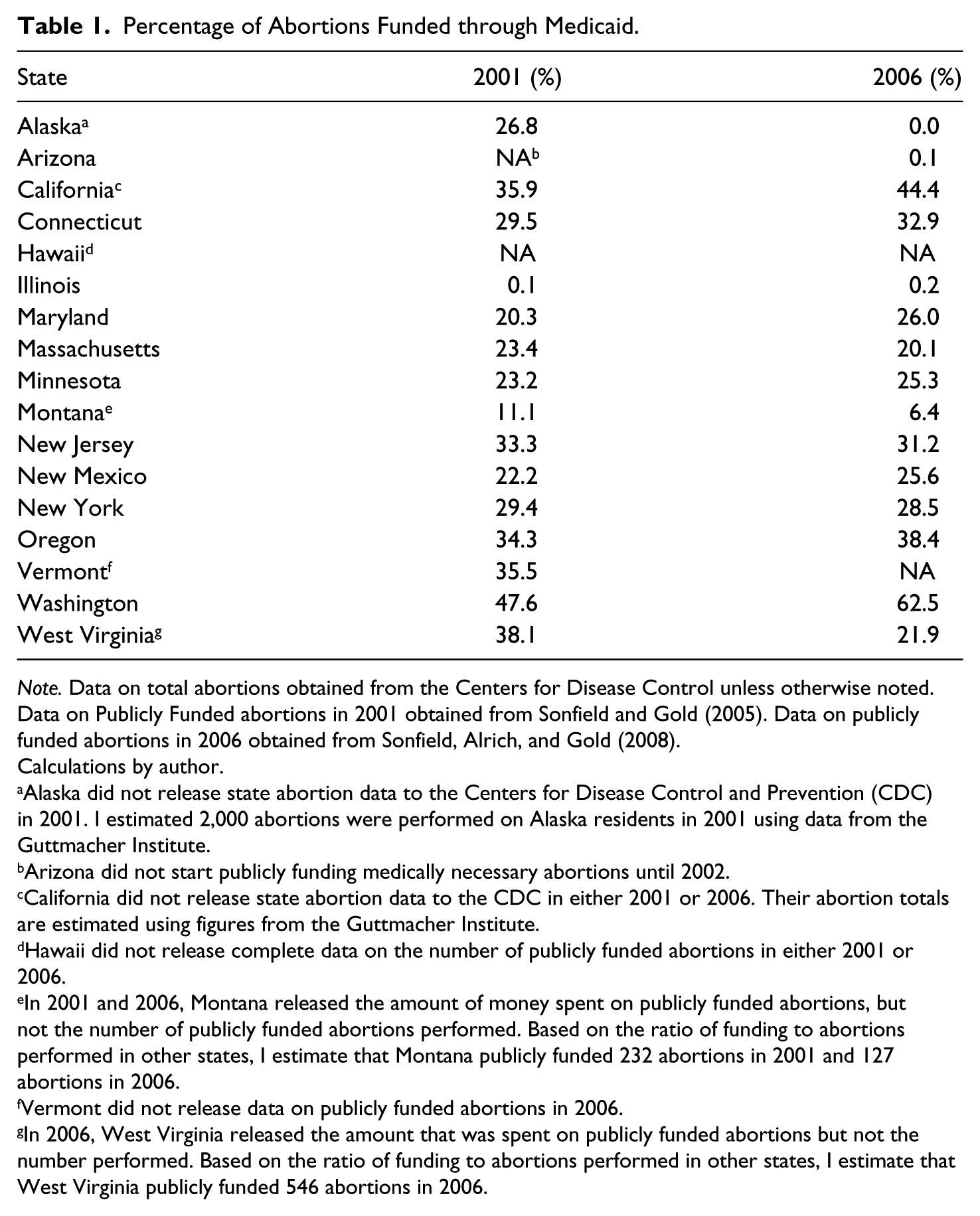
Note. Data on total abortions obtained from the Centers for Disease Control unless otherwise noted. Data on Publicly Funded abortions in 2001 obtained from Sonfield and Gold (2005). Data on publicly funded abortions in 2006 obtained from Sonfield, Alrich, and Gold (2008).
Calculations by author.
Alaska did not release state abortion data to the Centers for Disease Control and Prevention (CDC) in 2001. I estimated 2,000 abortions were performed on Alaska residents in 2001 using data from the Guttmacher Institute.
Arizona did not start publicly funding medically necessary abortions until 2002.
California did not release state abortion data to the CDC in either 2001 or 2006. Their abortion totals are estimated using figures from the Guttmacher Institute.
Hawaii did not release complete data on the number of publicly funded abortions in either 2001 or 2006.
In 2001 and 2006, Montana released the amount of money spent on publicly funded abortions, but not the number of publicly funded abortions performed. Based on the ratio of funding to abortions performed in other states, I estimate that Montana publicly funded 232 abortions in 2001 and 127 abortions in 2006.
Vermont did not release data on publicly funded abortions in 2006.
In 2006, West Virginia released the amount that was spent on publicly funded abortions but not the number performed. Based on the ratio of funding to abortions performed in other states, I estimate that West Virginia publicly funded 546 abortions in 2006.
2. Maryland
In my 2011 SPPQ article, I reported that Maryland did not fund therapeutic abortions through Medicaid for six months in 1998. Medoff and Dennis are correct that “Maryland has voluntarily funded Medicaid abortions uninterrupted.” My mistake was based on a misreading of a table in NARAL’s 1998 Who Decides? publication. I regret the error. Maryland’s Medicaid funding restrictions variable should be scored a 0 for every year from 1985 to 2005.
3. Minnesota
My 2011 SPPQ article indicated that Minnesota funded therapeutic abortions through Medicaid starting in 1995. Medoff and Dennis correctly identify June 16, 1994, as the correct start date for this policy (Merz, Jackson, and Klerman 1995). However, Medoff and Dennis’ original SPPQ submission listed the start date for Minnesota’s law as December 15, 1995. They only were able to obtain the correct start date for this law because I provided them this information during the review process. Minnesota’s Medicaid funding restrictions variable should be scored a .455 for 1994 and a 0 for every subsequent year.
4. Montana
Medoff and Dennis are correct that in 1995, the Montana District Court ruled that Montana must fund medically necessary Medicaid abortions. However, Montana is something of a unique situation because it funds a relatively small percentage of abortions through Medicaid. In 2001, only 11.1% of abortions performed on Montana residents were funded by Medicaid. That figure was 6.4% in 2006. Medicaid consistently pays for over 20% of the abortions in nearly every other state where it funds medically necessary abortions (Table 2). Still, since Montana, unlike Arizona, funds a non-trivial number of abortions through Medicaid, it is reasonable to score Montana’s funding restrictions variable a 0 from 1995 to 2005.
North Carolina Abortions 1985–95.

Note. Data on State Funded Abortions come from Cook et al. (1999). Data on total abortions come from the CDC. Cook et al. report state funded abortions by fiscal year rather than calendar year, but this table still provides a good approximation of the percentage of abortions annually paid for by the state abortion fund. CDC = Centers for Disease Control and Prevention.
5. New Mexico
Here Medoff and Dennis are correct that New Mexico has funded medically necessary abortions through Medicaid since December 1, 1994. My error was caused by the fact that NARAL’s Who Decides? fails to list New Mexico as a state funding medically necessary abortions in 1996, 1997, or 1998. What likely caused the discrepancy was that on April 19, 1995, New Mexico State Human Services Secretary Dorothy Danfelser announced she would limit public payment for abortions to only cases of rape, incest, and life of the mother (Peterson 1995). However, on June 5, 1995, New Mexico District Court Judge Steve Herrera issued a permanent injunction blocking these limits (Abortion Report 1995a; American Health Line 1995). On December 1, 1998, the New Mexico Supreme Court ruled these proposed limits on Medicaid-funded abortions unconstitutional (Oswald 1998). New Mexico has continued to fund medically necessary abortions through Medicaid since December 1, 1994. New Mexico’s Medicaid funding restrictions variable should be scored a .915 in 1994 and a 0 for every subsequent year.
6. North Carolina
North Carolina presents a unique situation. Medoff and Dennis are correct that until 1995, North Carolina funded abortions not through Medicaid but rather through a separate state abortion fund. Two aspects of the state abortion fund render it appropriate to treat North Carolina differently than states that fund abortion through Medicaid. First, only those women with incomes less than 50% of the poverty line were eligible for a publicly funded abortion (Cook et al. 1999). In states that fund abortions through Medicaid, the income threshold for eligibility is much higher. Second, starting in 1985, North Carolina restricted publicly funded abortions to cases of rape, incest, fetal deformity, documented maternal health risk, or situations where the mother was mentally retarded (Cook et al. 1999).
As such, relatively few abortions in North Carolina were publicly funded. Table 2 shows that between 1985 and 1993, North Carolina never funded more than 12% of its abortions through its state abortion fund. Overall, North Carolina’s state abortion fund paid for a considerably smaller percentage of state abortions than state Medicaid plans that covered therapeutic abortions. As such, a separate variable will be added to the regression models to specifically capture the impact of North Carolina’s state abortion fund. It will be scored a 1 in 1985 through 1988 .033 in 1989, .5 in 1990, .277 in 1991, .422 in 1992, .378 in 1993, 1 in 1994, .50 in 1995, and 1 in every subsequent year.
7. Vermont
Medoff and Dennis use an incorrect start date. On September 28, 1985, a state court in Vermont enjoined the state, which was only paying for Medicaid abortions in accordance with the federal Hyde Amendment standard. As such, Vermont was required to fund medically necessary abortions (Merz, Jackson, and Klerman 1995). This was prior to the Vermont Superior Court’s 1986 Doe v. Celani decision that Medoff and Dennis cite. Unfortunately, in my 2011 SPPQ article, I listed the start date for Vermont’s public funding as September 28, 1984, instead of the correct date of September 28, 1985. I regret the error. Vermont’s Medicaid funding restrictions variable should be scored a .740 in 1985 and a 0 for every subsequent year.
Summary
Medoff and Dennis state that they found seven errors in my data set of public funding restrictions. One error (Maryland) was due to the fact I misread a table in a 1998 NARAL publication. Another error was due to the fact that NARAL for a few years misclassified a state (New Mexico) that was funding medically necessary abortions through Medicaid. Another state (North Carolina) is a unique situation because it funded abortions not through Medicaid but through a state abortion fund, which periodically ran out of money. In one state (Minnesota) our time frame is similar, but Medoff and Dennis only obtained the correct start date because I provided them this information during the review process. In another state (Vermont), we both ended up using slightly incorrect start dates. Finally, one state is unique (Montana) because it funds relatively few abortions through Medicaid.
However, I coded Arizona correctly because it funds a tiny percentage of abortions through its Medicaid program. In future research, Illinois should also be excluded from the data set of states that fund medically necessary abortions through Medicaid. On December 2, 1994, the Circuit Court of Cook County ordered the state to provide reimbursement “for abortions necessary to protect a woman’s health” (Merz, Jackson, and Klerman 1995). Since 1995, NARAL has listed Illinois as a state that publicly funds medically necessary abortions through Medicaid.
However, according to data from the Guttmacher Institute, in 2001 and 2006, less than 0.2% of all abortions performed on Illinois residents were funded by Medicaid (Table 1). Similarly, according to data from the Illinois Department of Public Aid, every year from 1994 to 2002, less than 1% of abortions performed on Illinois residents were paid for by Medicaid. 6 As such, it would be appropriate to consider Illinois a state that does not fund abortions through Medicaid.
Errors identified by Medoff and Dennis in my Dataset of Informed Consent Laws
1. Alabama
Medoff and Dennis use an incorrect start date for Alabama’s informed consent law. Alabama’s informed consent law took effect on October 14, 2002 (Associated Press 2002; Otts 2002). As such, Alabama’s informed consent variable should be scored a .216 in 2002 and a 1 in every subsequent year.
2. Delaware
Medoff and Dennis are correct that Delaware had an informed consent law as of 1985. However, there is evidence that Delaware’s informed consent provisions date back to 1979 (Associated Press 1979c; NARAL 2012b). Delaware’s informed consent variable should be scored a 1 for every year from 1985 to 2005.
3. Indiana
Medoff and Dennis are correct. Legal challenges over Indiana’s informed consent law continued until November 2005 (Browning 2005). However, the law took effect on May 1, 2003 (Associated Press 2003a; Penner 2003). I should note, however, that Medoff and Dennis’ original SPPQ submission stated that Indiana never had an informed consent law between 1985 and 2005. They only were able to obtain the correct May 1, 2003, start date because I provided them this information during the review process. Indiana’s informed consent variable should be scored a .671 in 2003 and a 1 in every subsequent year.
4. Kentucky
Medoff and Dennis use an incorrect start date for Kentucky’s informed consent law. On April 15, 1998, the Kentucky House and Senate overrode the veto of Governor Paul Patton (American Health Line 1998). The law was to take effect on January 1, 1999 (Wolfe 1998). However, an Associated Press story indicated that the American Civil Liberties Union (ACLU) was suing over the constitutionality of the law and that the law had not yet gone into effect (Greuter 1999). On December 20, 2000, a Federal District Court upheld the constitutionality of the law (Schreiner 2000). The informed consent law took effect sometime in March 2001 (Wolfe 2002). As such, Kentucky’s informed consent variable should be scored a .797 in 2001 and a 1 in every subsequent year.
5. Louisiana
Medoff and Dennis likely use a correct start date for a recent version of Louisiana’s informed consent law. However, Louisiana first enacted an informed consent law in 1978 (Crider 1978). On March 3, 1980, the U.S. District Court in Margaret S. v. Edwards struck down most of the law (Crider 1980). However, the court upheld certain provisions. For instance, it found that “providing information to patients concerning social services available to a pregnant woman or a recent mother is rationally related to the giving of an informed consent” and sustained this section. As such, Louisiana’s informed consent variable should be scored a 1 from 1985 to 2005.
6. Maine
Medoff and Dennis use an incorrect start date for Maine’s informed consent law. Maine’s first informed consent law was enacted in 1979 (Weeks 1980). In Women’s Community Health Center, Inc. v. Cohen, the U.S. District Court struck down the 48-hour waiting period, but did not strike down the informed consent provision. As such, Maine’s informed consent variable should be scored a 1 from 1985 to 2005.
7. Massachusetts
Here Medoff and Dennis are incorrect. Massachusetts passed an informed consent law in 1980 (Avila 2005). In 1981, in Planned Parenthood League of Massachusetts v. Bellotti, the First Circuit Court of Appeals struck down the 24-hour reflection period and the requirement that forms be produced describing the stages of fetal development. However, the requirement that the Department of Public Health produce forms describing possible medical complications and alternatives to abortion was upheld (Avila 2005). As such, Massachusetts’ informed consent variable should be scored a 1 from 1985 to 2005.
8. Mississippi
Medoff and Dennis use an incorrect start date for Mississippi’s informed consent law. Mississippi’s informed consent law took effect on August 8, 1992 (Althaus and Henshaw 1994; The San Francisco Chronicle 1992; The Washington Post 1992). As such, Mississippi’s informed consent variable should be scored a .397 in 1992 and a 1 in every subsequent year.
9. Montana
Montana enacted an Abortion Control Act in 1974 (The Hotline 1991; NARAL 2014a) that included an informed consent law. It does not appear that this informed consent law was enforced (Abortion Report 1991). However, the fact that an informed consent law was on the books explains why NARAL considered Montana a state with an informed consent law in each Who Decides? booklet that was published between 1992 and 2005. Medoff and Dennis are correct that Montana’s informed consent variable should be scored a 0 for every year from 1985 to 2005.
10. Nebraska
Medoff and Dennis have Nebraska enforcing an informed consent law for all of 1993. However, Nebraska’s informed consent law took effect on September 9, 1993 (Abortion Report 1993a). As such, Nebraska’s informed consent variable should be scored a .312 in 1993 and a 1 in every subsequent year.
11. Nevada
Medoff and Dennis are incorrect. On July 17, 1985, in Glick v. McKay, the U.S. District Court in Nevada upheld parts of Nevada’s abortion statute that included having the “Attending physician . . . explain the physical and emotional implications of having the abortion.” NARAL (2012c) also cites a 1985 start date for Nevada’s informed consent law. As such, Nevada’s informed consent variable should be scored a .458 in 1985 and a 1 in every subsequent year.
12. North Dakota
Medoff and Dennis use an incorrect start date for North Dakota’s informed consent law. North Dakota enacted an informed consent law in 1975 and amended the law in 1979 (Associated Press 1980). In 1980, a U.S. District Judge upheld parts of the law while declaring parts of the law unconstitutional (Associated Press 1980). As such, North Dakota’s informed consent variable should be scored a 1 from 1985 to 2005.
13. Ohio
My 2011 SPPQ article correctly lists March 14, 1994, as the enforcement date for Ohio’s informed consent law. There was no error to be corrected. I should add that Medoff and Dennis’ original SPPQ submission listed the start date for Ohio’s law as July 27, 1993. They were only able to obtain the correct start date for this law because I provided them this information during the review process. Ohio’s informed consent variable should be scored a .803 in 1994 and a 1 in every subsequent year.
14. Pennsylvania
My 2011 SPPQ article correctly lists March 21, 1994, as the enforcement date for Pennsylvania’s informed consent law. There was no error to be corrected. I should add that Medoff and Dennis’ original SPPQ submission listed the start date for Pennsylvania’s law as June 29, 1992. They were only able to obtain the correct start date for this law because I provided them this information during the review process. Pennsylvania’s informed consent variable should be scored a .784 in 1994 and a 1 in every subsequent year.
15. Rhode Island
Medoff and Dennis are correct. Rhode Island’s informed consent law dates back to 1982 (Davis 2003). Rhode Island’s informed consent variable should be scored a 1 from 1985 to 2005.
16. South Carolina
Medoff and Dennis use an incorrect start date. South Carolina’s informed consent law took effect on January 3, 1995 (Abortion Report 1995b). As such, South Carolina’s informed consent variable should be scored a .994 in 1995 and a 1 in every subsequent year.
17. South Dakota
Medoff and Dennis may be correct that a recent version of South Dakota’s informed consent law was upheld in 1993. However, news reports indicate South Dakota’s informed consent law dates back to 1980 (Brokaw 2005). NARAL also cites a 1980 start date for South Dakota’s informed consent law (NARAL 2012d). As such, South Dakota’s informed consent score should be a 1 in 1985 and every subsequent year.
18. Tennessee
Medoff and Dennis are incorrect. Tennessee’s first informed consent law was enacted in 1978 (Abortion Report 1994; Tenn Code. Ann. Sec. 39-302: 1978; The Family Action Council of Tennessee 2011; NARAL 2014b). Tennessee passed another informed consent law in 1992. Parts of the law were upheld by a Davidson County Circuit Court judge in 1992 (Abortion Report 1993b) and 1994 (Abortion Report 1994). In Planned Parenthood of Middle Tennessee v. Sundquist, the Tennessee Supreme Court ruled that this later informed consent law was unconstitutional, but allowed the state to continue the informed consent requirements of appropriate information about abortion. As such, Tennessee’s informed consent score should be a 1 in 1985 and every subsequent year.
19. Texas
Medoff and Dennis use an incorrect start date. Texas’ informed consent law was passed in 2003 but did not take effect until January 1, 2004 (Colman and Joyce 2011; Pasztor 2004). Texas’ informed consent variable should be scored a 0 in 2003 and a 1 in 2004 and every subsequent year.
20. Utah
Medoff and Dennis may be correct that a recent version of Utah’s informed consent law was upheld in 1994. However, Utah’s informed consent statute dates back to 1974 (Utah Law Review 1994). NARAL also cites a 1974 start date for Utah’s informed consent law (NARAL 2012e). As such, Utah’s informed consent score should be a 1 in 1985 and every subsequent year.
21. Virginia
Medoff and Dennis use an incorrect start date. Virginia enacted a parental consent bill in 1997 (Nakashima 1997). However, Virginia’s informed consent law took effect on October 1, 2001 (Misjewski 2001; Szabo 2001). Virginia’s informed consent variable should be scored a .252 in 2001 and a 1 in every subsequent year.
22. Wisconsin
Medoff and Dennis use a series of incorrect start dates. Wisconsin’s original informed consent law was enacted in 1985 (NARAL 2012f; Wis. Stat. Ann. § 253.10: 2011). Governor Tommy Thompson signed a subsequent informed consent law on April 30, 1996 (Telegraph Herald 1996b) which was to take effect on July 1, 1996 (Telegraph Herald 1996a). After a series of legal challenges, U.S. District Judge Barbara Crabb approved the state-produced materials on February 5, 1998 (McLaughlin 1998) and the law took effect on June 1, 1998 (Segall 1998). As such, Wisconsin’s informed consent variable should be scored a .586 in 1985 and a 1 in every subsequent year.
Correcting My Own Dataset of Informed Consent Laws
The data set of informed consent laws used in my 2011 SPPQ article and Medoff and Dennis in their SPPQ article includes some additional errors that should be corrected.
1. California
California’s informed consent law took effect around February 17, 1982 (California Code of Regulations, tit. 22 § 75001: 2012; California Code of Regulations, tit. 22 § 75040: 2012). As such, California’s informed consent variable should be scored a 1 for 1985 and every subsequent year.
2. Connecticut
Connecticut’s informed consent law took effect on August 1, 1983 (Conn. Gen. Stat. Ann. §§ 19a-116, 19a-116-1(c): 2011; NARAL 2012a). As such, Connecticut’s informed consent variable should be scored a 1 for 1985 and every subsequent year.
3. Delaware
Delaware’s informed consent law took effect on July 13, 1979 (Del. Code Ann. Tit. 24 § 1794: 2012; Esenberg 2007). As such, Delaware’s informed consent variable should be scored a 1 for 1985 and every subsequent year.
4. Florida
In 1979, Florida passed a group of abortion restrictions that included an informed consent bill. They took effect on June 29, 1979 (Associated Press 1979b). On December 13, 1979, a U.S. District Judge struck down most of the law, including the parental consent and spousal notification provisions. However, parts of the informed consent provision were upheld (Sewell 1979). As such, Florida’s informed consent variable should be scored a 1 for 1985 and every subsequent year.
5. Georgia
Georgia Governor Sonny Perdue signed the Woman’s Right to Know Act on May 10, 2005 (Hart 2005; Market Wire 2005; Georgia Department of Public Health 2014). The text of the law indicates the “act shall become effective upon its approval by the Governor” (Ga. Code Ann. §§ 31-9A-1, -2, -5, -7, -8: 2010). As such, Georgia’s informed consent variable should be scored a .644 in 2005 and a 1 in every subsequent year.
6. Idaho
Idaho’s informed consent bill law dates back to 1973 (Idaho Code §§ 18-604: 2011). As such, Idaho’s informed consent variable should be scored a 1 for 1985 and every subsequent year.
7. Illinois
My 2011 SPPQ article listed Illinois as having an informed consent law in 1993 and 1994. This was because NARAL’s 1993 Who Decides? lists Illinois as a state with an informed consent law. However, no subsequent NARAL publication or any National Right to Life Committee (NRLC) publication lists Illinois as ever having an informed consent law. Similarly, there are no media reports that indicate Illinois as having an informed consent law in place. As such, Illinois’ informed consent variable should be scored a 0 for every year.
8. Kansas
Kansas Governor Joan Finney signed an informed consent bill on April 23, 1992 (Truell 1992). As such, Kansas’ informed consent variable should be scored a .689 in 1992 and a 1 in every subsequent year.
9. Minnesota
On March 21, 1974, Minnesota Governor Wendell A. Anderson signed a group of abortion restrictions that included an informed consent bill (Minn. Stat. Ann. §§ 145.412: 2013; The New York Times 1974b). A U.S. District Court overturned the law on June 28, 1974 (The New York Times 1974a). On October 6, 1976, in Hodgson v. Lawson, the U.S. Eighth Circuit Court of Appeals upheld the informed consent provisions of the law. Specifically, “no abortion may be provided unless the woman consents after a full explanation of the procedure and its effect.” As such, Minnesota’s informed consent variable should be scored a 1 for 1985 and every subsequent year.
10. Missouri
On June 29, 1979, a group of abortion restrictions including an informed consent bill was signed by Missouri Governor Joseph Teasdale (Associated Press 1979a). U.S. District Court Judge Elmo Hunter struck down much of the legislation (The Washington Post 1980), but parts of the informed consent law were upheld (United Press International 1981). A later court ruling also upheld portions of the informed consent law including provisions requiring physicians to inform women about medical risks with the abortion technique to be used (United Press International 1981). As such, Missouri’s informed consent variable should be scored a 1 for 1985 and every subsequent year.
11. Oklahoma
Oklahoma Governor Brad Henry signed informed consent legislation on May 20, 2005 (Associated Press 2005a). The law took effect immediately with Henry’s signature (Associated Press 2005b). As such, Oklahoma’s informed consent variable should be scored a .616 for 2005.
12. West Virginia
West Virginia’s informed consent law took effect in March 2003 without Governor Robert Wise’s signature (Saxton 2003). As of September 2003, abortion providers were waiting for the state to produce materials with fetal development information and a directory of community resources that provide information on alternatives to abortion. However, other parts of the informed consent law were being enforced as of this time (Saxton 2003). As such, West Virginia’s informed consent variable should be scored a .797 for 2003 and a 1 for every subsequent year.
Summary
Medoff and Dennis criticize me for using a data set of state-level antiabortion laws that contains a number of errors. However, their revised data set contains a substantial number of errors as well. In their current article, 27 of the 33 informed consent laws they analyze have incorrect start dates. 7 Their original submission to SPPQ in the summer of 2011 used an incorrect start date for 30 of the 33 state-level informed consent laws. 8
A New Approach to Analyzing Informed Consent Laws
As I mentioned earlier, there is relatively little academic research analyzing the impact of state-level antiabortion informed consent laws. Part of the reason for this is that there is no commonly accepted data set of these laws. Another potential reason is that there exists great variation in these types of laws. Some informed consent laws simply require that the abortion provider give the gestational age of the child. Other informed consent laws represent more aggressive attempts to dissuade women from obtaining an abortion.
For instance, some informed consent laws require that women view color photos of fetal development, make multiple visits to the abortion clinic, and have the opportunity to view an ultrasound prior to the abortion procedure. In addition, some informed consent laws require that women receive information about the potential health risks involved with an abortion. In their article, Medoff and Dennis consider this information “blatantly false” or “misleading.” However, there is a substantial body of peer-reviewed research linking abortion to a higher risk of breast cancer and a range of mental health problems. 9
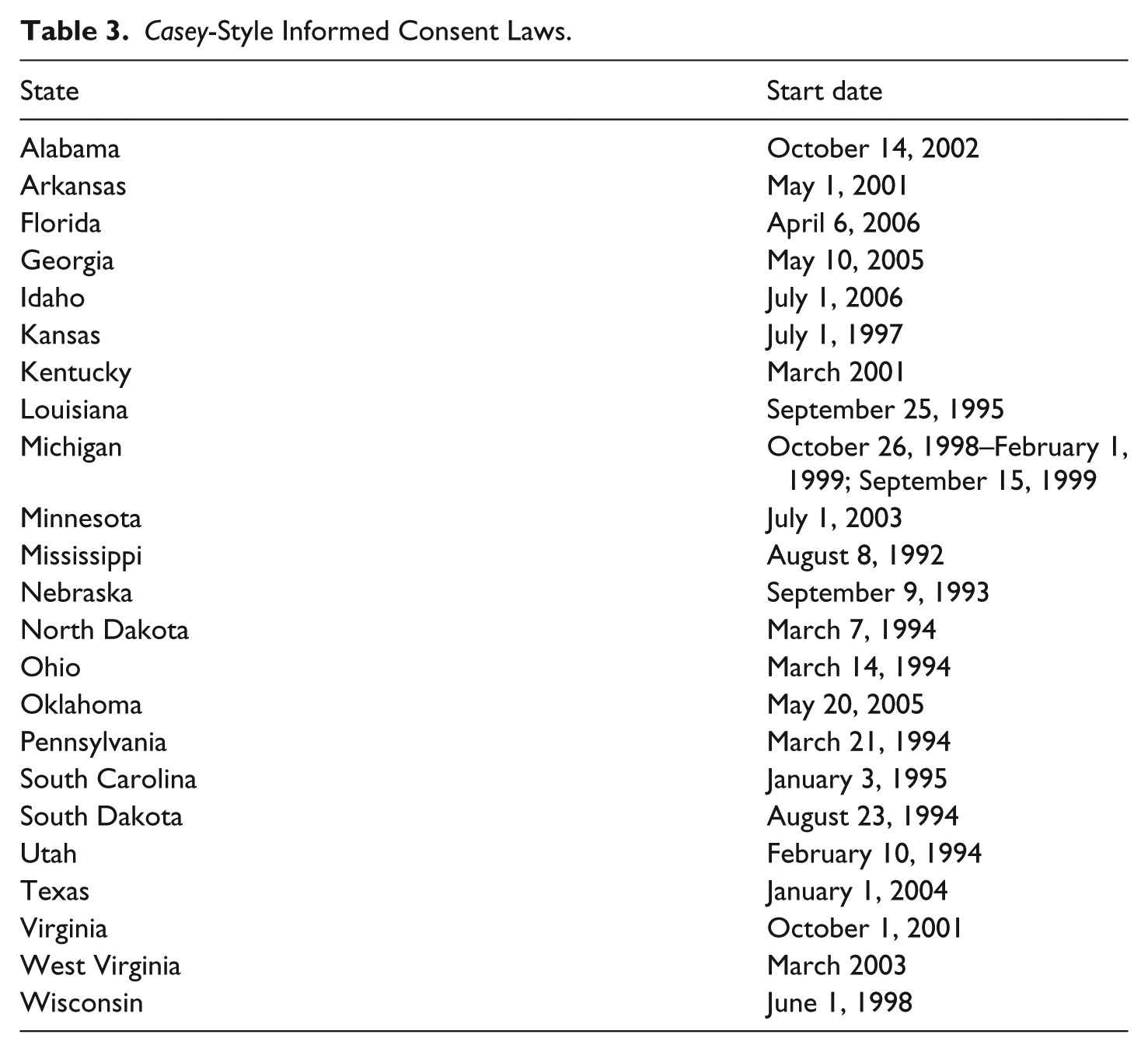
In 1996, the NRLC started tracking states that had passed “Casey-style” informed consent laws. These laws are modeled after Pennsylvania’s informed consent law, parts of which were upheld in the Supreme Court’s 1992 Planned Parenthood v. Casey decision. They all require that women seeking an abortion have the opportunity to view state-produced materials that include color photos of fetal development. Separately analyzing this category of informed consent laws might be a way to analyze a more recent group of informed consent laws that were specifically designed to dissuade women from obtaining abortions. A list of states that have enacted Casey-style informed consent laws can be found in Table 3.
Casey-Style Informed Consent Laws.
Analyzing the Methodology of My 2011 SPPQ Article
Medoff and Dennis identify five methodological errors with my 2011 SPPQ article. However, their concerns are overstated. First, in Footnote 3, they criticize me for excluding data from Alaska. The sales of oil and minerals are important components of Alaska’s economy, and shifts in the prices of these commodities can cause very substantial fluctuations in Alaska’s economic indicators. Because a number of economic variables are included in the regression model, I exclude data from Alaska. Medoff and Dennis argue that a case could be made to exclude data from other “unique” states as well. However, they fail to realize that many studies exclude Alaska when state fiscal data are being analyzed or held constant (Besley and Case 2003; Matsusaka 1995; 2004; Merrifield 2000; New 2010; Owings and Borck 2000; Primo 2006).
Second, Medoff and Dennis wrongly claim that my regression results are “implausible.” In my 2011 SPPQ article, I argue that antiabortion informed consent laws would have a larger impact on adult abortion rates than minor abortion rates. The regression results I present in Table 5 of my 2011 SPPQ article demonstrate this. However, Medoff and Dennis claim these results are “implausible.” They claim that if my theory is correct, the value of the informed consent variable should be the largest when the adult abortion rate is the dependent variable. Instead, the informed consent coefficient is the largest when the overall abortion rate is being analyzed.
What Medoff and Dennis fail to understand is that I am running regressions on two separate data sets. Not all states provide separate abortion data for minors and adults. As Table 4 indicates, when I restrict the data set to only those states that provide abortion data for minors and adults, the results indicate that informed consent laws had the largest impact on the adult abortion rate, a smaller impact on the overall rate, and the smallest impact on the minor abortion rate. This is consistent with my expectations and certainly indicates that my regression results in my 2011 SPPQ article were plausible.
New’s Plausible Empirical Results from His 2011 SPPQ Article.

Note. When adult abortion rate is the dependent variable, the coefficient for the informed consent variable is significant at the .11 level. SPPQ = State Politics & Policy Quarterly; CDC = Centers for Disease Control and Prevention.
Significant at 10% level. **Significant at 5% level. ***Significant at 1% level.
Third, Medoff and Dennis criticize me for not fully considering endogeneity issues with my independent variable that measures abortion providers per capita. They are correct that there are issues with causality. Fewer abortion providers may make it more difficult for women to obtain abortions. Conversely, fewer providers may be evidence of a lower demand for abortion. However, their own analysis shows that when they use instrumental variables to predict the number of abortion providers “the two-stage least-squares coefficients were not significantly different from the coefficients using New’s generalized least-squares estimation.” Overall, they state that “any endogeneity bias using generalized least squares is small.”
Fourth, they criticize me for giving each state a constant weight throughout the data set, and not considering population fluctuations across time. My reason for using constant rather than variable weights was to give recently passed antiabortion laws the same relative weight as antiabortion laws that were enacted earlier. From an econometric perspective, it is probably more accurate to allow the variable weights to change over time. However, it should be noted from Medoff and Dennis’ regression results that replacing the constant weights with variable weights does little to change either the magnitude or the significance of the regression coefficients.
Finally, Medoff and Dennis criticize me for failing to include variables that measure border state abortion policy. They argue that if a state passes an antiabortion law, it may increase the number of women who seek abortions in neighboring states. This is certainly a valid argument. However, Medoff and Dennis use an odd measure for border state policy. The variables used by Medoff and Dennis measure the number of adjacent states that are not enforcing various antiabortion laws. They state this measure was suggested by Blank et al. (1996) and Haas-Wilson (1996).
However, the variables used by Blank et al. (1996) and Haas-Wilson (1996) measure the presence of adjacent states with parental involvement laws. 10 This is a better measure. This makes it easier to determine if stringent border state policies result in more women obtaining abortions in adjacent states. Another problem with the Medoff–Dennis border policy variables is that they do not change after a state enacts various antiabortion laws. If a state’s abortion policy is more permissive than that of neighboring states, one might expect a significant number of women would travel to obtain abortions in the state. However, if a state’s policy suddenly becomes more restrictive than neighboring states, it is unlikely that women from adjacent states would continue to travel to that state to obtain abortions.
In their SPPQ article, Medoff and Dennis run a series of regressions similar to the ones I ran in my 2011 SPPQ article. The only differences are as follows: (1) their data set of antiabortion laws includes the corrections they made to the start dates; (2) in some of their regressions, they vary their weighting variable across time; (3) they include two independent variables that, respectively, measure the number of adjacent states that do not have parental involvement laws and informed consent laws; and (4) they include an indicator variable that is scored a 1 if a state enacted an informed consent law that requires two separate visits to the abortion clinic.
The inclusion of this final variable makes sense as there are studies that indicate that Mississippi’s informed consent law, which mandates two separate visits, was effective in reducing the abortion rate in Mississippi (Althaus and Henshaw 1994; Joyce, Henshaw, and Skatrud 1997; Joyce and Kaestner 2000). However, the data sets used by Medoff and Dennis contain incorrect start dates for each of the five informed consent laws that mandate two separate trips to the abortion clinic. Table 5 provides a list of these informed consent laws, the start date in the Medoff–Dennis data set, and the actual start date for these laws.
Informed Consent Laws Requiring Two Trips to the Abortion Provider.

I reran my regressions from my 2011 SPPQ article with the following changes. First, I corrected my data set of antiabortion laws as described in the “Correcting Medoff and Dennis’ Data Set of State-Level Antiabortion Laws” section. Second, I created three separate indicator variables to measure the respective presence of an informed consent law, a Casey-style informed consent law, and an informed consent law requiring two visits to the abortion provider. Third, I created four separate variables, one that measured the number of adjacent states with parental involvement laws and three that, respectively, measured the number of adjacent states with (1) an informed consent law, (2) a Casey-style informed consent law, and (3) an informed consent law requiring two visits to the abortion provider. Each of these four adjacent state variables would be scored a 0 once a state passed that corresponding type of antiabortion law. Fourth, I weight the data using an annual measure of state population that changes across time. The results for the variables measuring the presence of antiabortion laws are presented in Tables 6 and 7. The full regression results can be found in Appendices A and B.
The Impact of Abortion Restrictions on the Incidence of Abortion (CDC Data).

Note. Absolute value of t-statistics in parentheses. The full regression results can be found in Appendix A. CDC = Centers for Disease Control and Prevention.
p < .10. **p < .05. ***p < .01.
The Impact of Abortion Restrictions on the Incidence of Abortion (GI Data).

Note. Absolute value of t-statistics in parentheses. The full regression results can be found in Appendix A. GI = Guttmacher Institute
p < .10. **p < .05. ***p < .01.
The results are fairly consistent across data sets. The regression findings clearly indicate Medicaid funding restrictions result in statistically significant reductions in both the abortion rate and the abortion ratio. This is consistent with a substantial body of previous academic research that analyzes the impact of Medicaid funding restrictions. The results also indicate that parental involvement laws have relatively little impact on overall abortion rates and ratios. This is also consistent with previous research.
The most interesting findings involve the impact of the various types of informed consent laws. The passage of an informed consent law, by itself, does not appear to have a statistically significant impact on the incidence of abortion. This is unsurprising considering informed consent laws vary greatly across states. Some informed consent laws, more than others, represent serious efforts to dissuade women from obtaining abortions.
The regression results do provide some evidence that these stronger informed consent laws reduce the incidence of abortion. Casey-style informed consent laws result in statistically significant reductions to both the abortion rate and ratio whenever Centers for Disease Control and Prevention (CDC) abortion data are analyzed. Furthermore, the coefficient for informed consent laws requiring two visits to the abortion provider approaches statistical significance when CDC data are analyzed and reaches conventional levels of statistical significance when Guttmacher abortion data are analyzed.
However, analyzing the effect of these laws on overall abortion rates and ratios may not be the best way to gauge their impact. Several of the states that enacted informed consent laws requiring two visits to the abortion provider, such as Mississippi and Utah, had low abortion rates prior to the enactment of the informed consent law. Similarly, several of the states that enacted Casey-style informed consent laws, such as North Dakota and South Dakota, have also historically had a low incidence of abortion. As such, it might be better to analyze the impact of these laws on the percentage decline in the incidence of abortion. For the next set of regressions, the dependent variables will be the weighted natural log of the abortion rate and the weighted natural log of the abortion ratio. The results for the variables measuring the presence of various antiabortion laws are presented in Tables 8 and 9. The full regression results can be found in Appendices C and D.
The Impact of Abortion Restrictions on the Incidence of Abortion (Logged CDC Data).

Note. Absolute value of t-statistics in parentheses. The full regression results can be found in Appendix B. CDC = Centers for Disease Control and Prevention.
p < .10. **p < .05. ***p < .01.
The Impact of Abortion Restrictions on the Incidence of abortion (Logged GI Data).
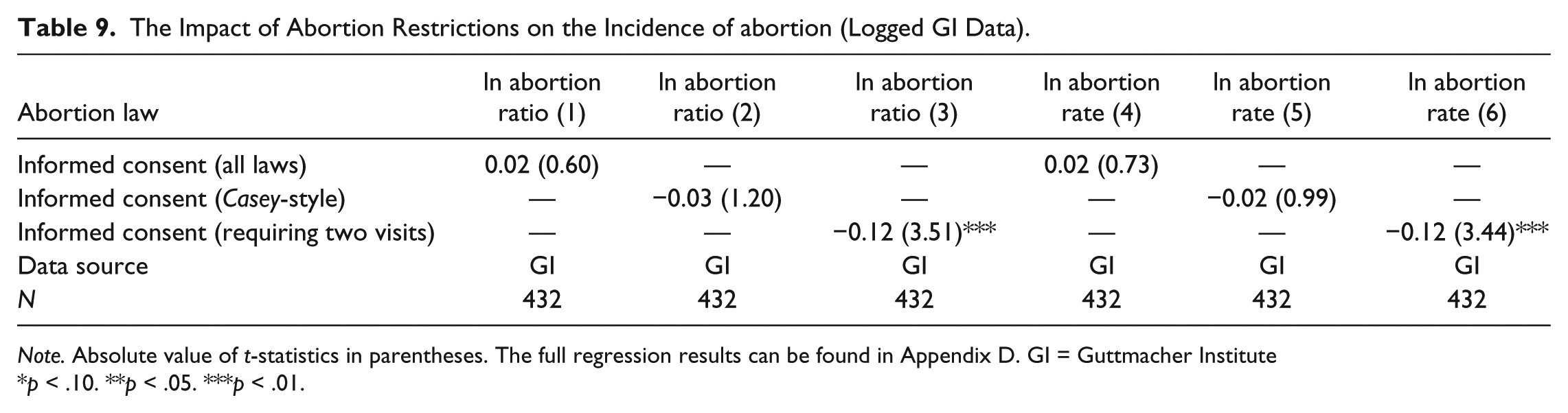
Note. Absolute value of t-statistics in parentheses. The full regression results can be found in Appendix D. GI = Guttmacher Institute
p < .10. **p < .05. ***p < .01.
The results are interesting. Once again, the passage of an informed consent law by itself does not appear to have a statistically significant impact on the incidence of abortion. The 22 Casey-style informed consent laws have an inconsistent impact across data sets. They result in statistically significant reductions in both the logged abortion rate and ratio when CDC abortion data are analyzed. However, their effect is considerably weaker when abortion data from the Guttmacher Institute is used. Overall, the most interesting finding involves informed consent laws that require women to make two trips to the abortion provider. The results indicate that these laws result in statistically significant declines in the incidence of abortion. This finding is consistent across data sets.
Previous research on abortion trends in Mississippi has documented the effectiveness of these types of informed consent laws (Althaus and Henshaw 1994; Joyce, Henshaw, and Skatrud 1997; Joyce and Kaestner 2000). However, this is the first analysis to document the effectiveness of this type of informed consent law using time-series cross-sectional data. Overall, the regression results presented in Tables 6 to 9 nicely add to the body of peer-reviewed research which shows that public funding restrictions and properly designed informed consent laws all reduce the incidence of abortion.
In their article, Medoff and Dennis find that some antiabortion laws correlate with reductions in the incidence of abortion. They run a series of statistical tests in an attempt to determine if these abortion reductions are caused by the enactment of antiabortion laws or if they are simply correlated with the passage of antiabortion legislation. It is true that the passage of antiabortion laws is not a random occurrence and it is possible that antiabortion laws could be clustered in politically conservative states where abortion rates are declining due to shifts in public opinion or other factors that cannot be easily held constant.
However, a set of natural experiments provide evidence that the abortion reductions are caused by the antiabortion laws. The results from Table 10 indicate that parental involvement laws cause statistically significant declines in minor abortion rates but fail to have a statistically significant impact on adult abortion rates. Similarly, both Casey-style informed consent laws and informed consent laws that require two visits to the provider result in statistically significant reductions to adult abortion rates. However, both types of informed consent laws have little effect on minor abortion rates. The fact that different types of antiabortion laws have disparate and predictable impact on different population subgroups provides evidence that abortion reductions are caused by antiabortion legislation and not regional shifts in public opinion or other factors.
The Impact of Abortion Restrictions on the Minor Abortion Rate and Adult Abortion Rate.
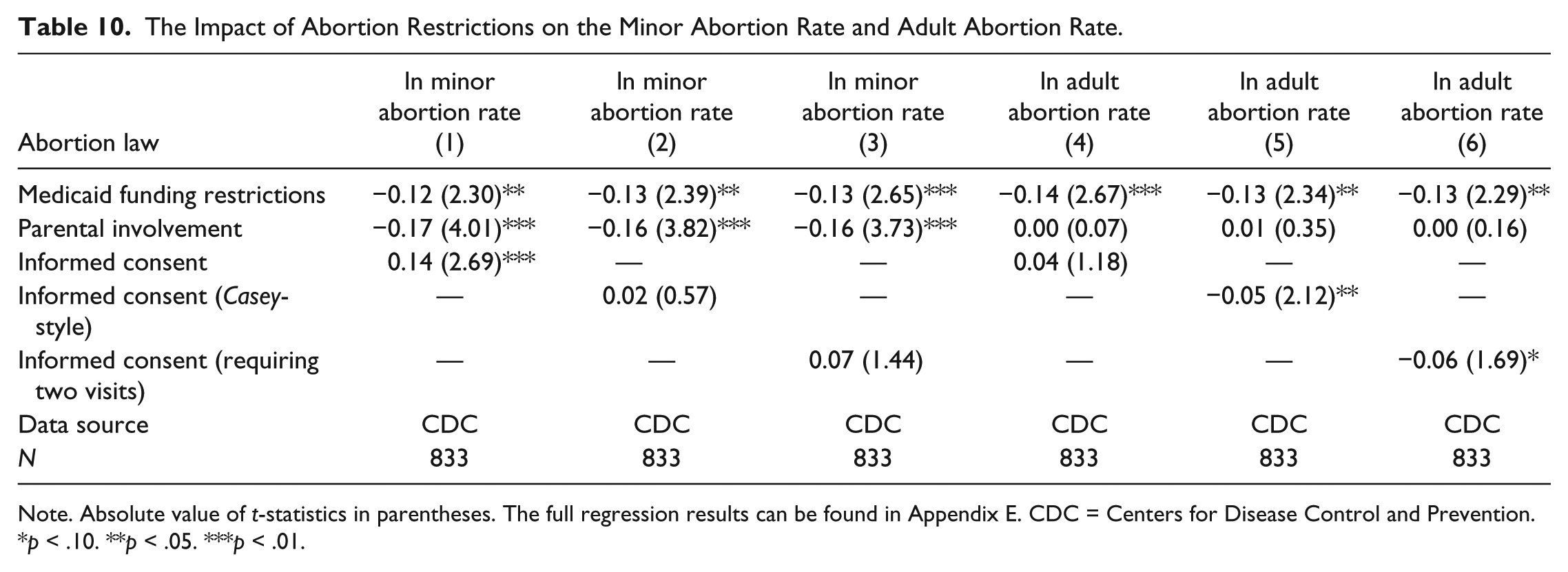
Note. Absolute value of t-statistics in parentheses. The full regression results can be found in Appendix E. CDC = Centers for Disease Control and Prevention.
p < .10. **p < .05. ***p < .01.
Similarly, Table 11 provides evidence from another set of natural experiments. On several occasions, a state has passed either an informed consent law or a parental involvement law, only to have it nullified by a judge. 11 This creates a nice set of natural experiments. A group of states decided to adopt the same type of antiabortion law. However, in some cases, the law took effect, whereas in other cases, the law was nullified due to a judicial ruling. The results indicate that nullified parental involvement laws have little impact on the incidence of abortion among minors, whereas enacted parental involvement laws result in statistically significant minor abortion rate reductions. Similarly, the coefficient for nullified informed consent laws is small and insignificant in every regression. However, both Casey-style informed consent laws and informed consent laws requiring two trips to the abortion provider again result in statistically significant reductions in both the abortion rate and ratio. These natural experiments provide solid evidence that antiabortion laws reduce the incidence of abortion.
The Impact of Nullified Abortion Restrictions.
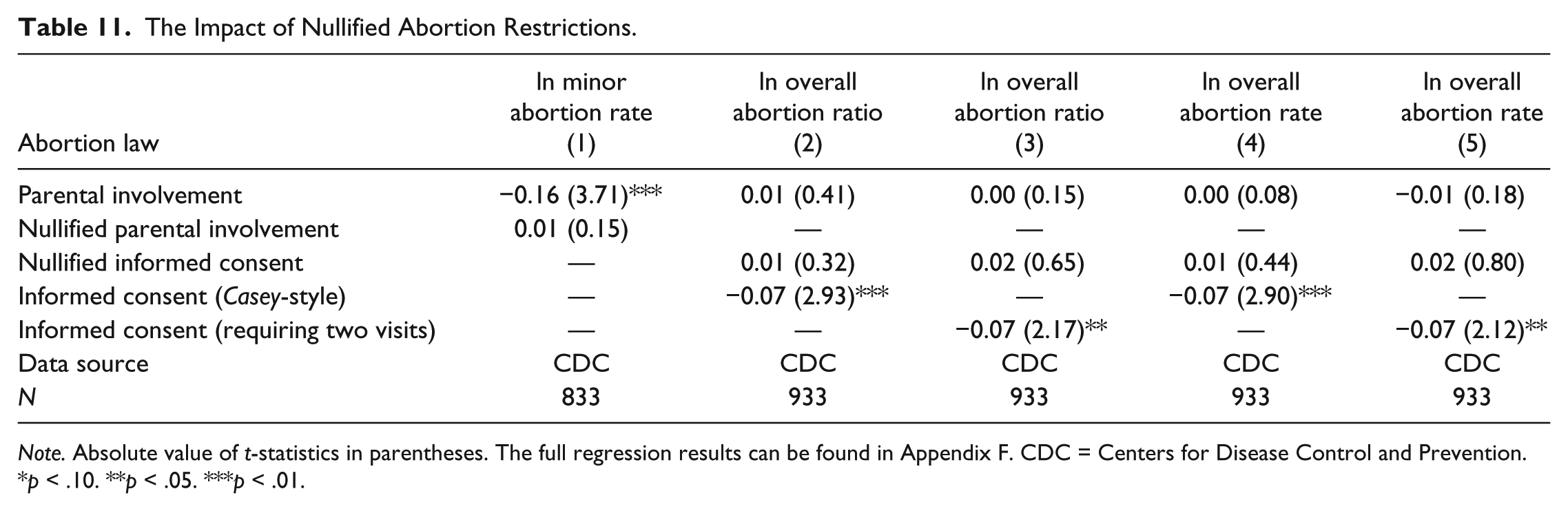
Note. Absolute value of t-statistics in parentheses. The full regression results can be found in Appendix F. CDC = Centers for Disease Control and Prevention.
p < .10. **p < .05. ***p < .01.
Analyzing the Abortion Decline in the United States since 1990
Throughout the course of their article, Medoff and Dennis criticize me for arguing that the enactment of state-level antiabortion laws is a major factor in the decline in the incidence of abortion in the United States. However, they appear to misunderstand the purpose of my 2011 SPPQ article which was to analyze the effect of state-level antiabortion laws that received greater constitutional protection after the Supreme Court’s 1992 Casey decision. The primary purpose of that article was not to explain why the abortion rate in the United States has been declining since the early 1990s. Nor was the purpose to analyze competing theories as to why America’s abortion rate was falling.
Furthermore, in the article’s introduction, I clearly cite nine other possible factors that might have led to America’s abortion decline, including (1) the strong economy, (2) declining fertility rates, (3) emphasis on lowering teen pregnancy rates, (4) changes in sex education curricula, (5) reduced sexual activity among minors, (6) greater contraceptive use among minors, (7) improvements in the reliability of contraceptives, (8) greater adult use of contraceptives, and (9) fewer physicians performing abortions. Medoff and Dennis make no mention of this.
At the end of their article, Medoff and Dennis cite some increases in contraception use in the United States and argue that increases in contraceptive use are responsible for the decline in the U.S. abortion rate. However, their arguments are unpersuasive. Increased availability of contraception may result in more sexual activity (Akerlof, Yellen, and Katz 1996; Arcidiacono, Khwaja, and Ouyang 2012; Finer 2007; Goldin and Katz 2002; Paton 2002). Increased contraception use may also be a function of increased sexual activity. Furthermore, greater contraception use may not result in fewer abortions. According to a Guttmacher Institute study, 54% of women who have abortions used a contraceptive method during the month they became pregnant (R. Jones, Darroch, and Henshaw 2002).
On a practical level, the data that Medoff and Dennis cite showing increases in contraception use since the early to mid-1980s (National Center for Health Statistics 2010) also show consistent increases in contraception use from the early 1970s to the late 1980s (Mosher and Pratt 1990). This finding was consistent among all groups of women, regardless of age, marital status, or race. However, the increase in contraception use did not reduce the number of abortions performed in the United States during either the 1970s or 1980s. In addition, research published by the National Center for Health Statistics also shows that contraception use increased between the mid-1990s and the period between 2006 and 2010. However, the same data also show that the fertility rate, the percentage of unplanned pregnancies, and the unplanned pregnancy rate have all increased since 1995 (Jones, Mosher, and Daniels 2012).
Overall, Medoff and Dennis fail to cite any research which shows that increased contraception use lowers the incidence of abortion. Indeed, the academic literature paints a very mixed picture of the relationship between contraception use and the incidence of abortion. A 2003 Guttmacher Institute study of abortion rates and contraception use in various countries finds an inconsistent relationship between contraception use and abortion rates. In fact, the Guttmacher analysis showed a simultaneous increase in both contraceptive use and abortion rates in several countries, including the United States, Cuba, Denmark, Netherlands, Singapore, and South Korea (Marston and Cleland 2003). Furthermore, a recent 10-year study in Spain saw significant increases in both contraception use and abortion rates (Dueñas et al. 2011).
Another factor in the decline in the abortion rate that Medoff and Dennis fail to consider might be shifts in public opinion about abortion. The link between abortion attitudes and abortion incidence is not well documented. However, shifts in public opinion should be considered because there is evidence of an increase in “pro-life” public sentiment since the mid-1990s. A September 1995 Gallup survey found that only 33% of Americans self-identified as “pro-life.” However, 34 of 38 Gallup surveys taken since September 1995 indicate that at least 40% of respondents self-identify as “pro-life” (Gallup 2012). The year 2009 was the first time that a majority of respondents in the Gallup survey identified as pro-life (The Washington Post 2009) and pro-life self-identification reached 50% again in May 2012 (Shellnut 2012).
Other Gallup survey questions also show an increase in opposition to abortion. Between April 1990 and June 1995, each of 14 Gallup surveys showed that at least 30% of all respondents thought abortion “should be legal in all circumstances.” However, 22 of the 23 surveys taken after June 1995 indicated less than 30% of all respondents thought abortion should be legal in all circumstances. Similarly, the 10 Gallup surveys taken between April 1990 and June 1995 found that an average of 14% of Americans thought abortion should be “illegal in all circumstances.” However, the 23 surveys taken after June 1995 indicate that an average of 20% of respondents think abortion should be banned in all circumstances. Table 12 shows statistically significant evidence of gains in antiabortion sentiment by analyzing data from Gallup surveys.
Gains in Antiabortion Sentiment.

Source. Gallup (2012).
Significant at 10% level. **Significant at 5% level. ***Significant at 1% level.
Changes in public sentiment have been documented in other ways as well. The General Social Survey (GSS) has been asking the same six questions on abortion attitudes since the early 1970s. There is evidence that starting in the mid-1990s, respondents became more willing to restrict abortion in a variety of circumstances (Wilcox and Carr 2009). Finally, there is evidence that the repeat abortion rate is only declining slightly, while the first time abortion rate has been declining more significantly over time (Franz 2011). This might be evidence that younger women are less likely to submit to an abortion when faced with an unplanned pregnancy.
Conclusion
Several times in their article, Medoff and Dennis hint that I was less than forthright about various details pertaining to my research on the impact of antiabortion laws. However, this was not the case. The set of state-level antiabortion laws that were analyzed, the data points that were excluded, and my rationale for excluding various data points were all included in the article’s appendix. The fact that I weighted the data by state population was also mentioned in the appendix. Medoff and Dennis did not have to rely on personal communication with me for any of this information. Furthermore, I also provided both the complete data sets and the STATA commands used to run each of the regressions to Professor Medoff and all other researchers who requested them.
Overall, my 2011 SPPQ article has received a considerable amount of attention from academics and journalists. It was one of the first times an article analyzing the impact of antiabortion laws appeared in a political science journal. It was also one of the few studies that used time-series cross-sectional data to analyze the impact of antiabortion informed consent laws. By scrutinizing the data set I used in my 2011 SPPQ article, Medoff and Dennis identify some circumstances where antiabortion groups, abortion rights groups, and researchers disagree about the presence or absence of a state-level antiabortion law. They also contribute to the creation of a more accurate data set of state-level antiabortion informed consent laws. All of this should be of interest to scholars of both state politics and abortion politics.
However, Medoff and Dennis fail to understand that the primary purpose of my article was not to analyze competing theories about the post-1990 abortion decline in the United States, but rather to analyze the impact of a group of antiabortion laws that received greater constitutional protection after the Supreme Court’s 1992 Casey decision. Furthermore, their analysis contains a number of critical measurement, and methodological and estimation errors. Overall, my analysis of a corrected data set of state-level antiabortion laws adds to the sizeable body of peer-reviewed research which shows that public funding restrictions, parental involvement laws, and properly designed informed consent laws all reduce the incidence of abortion.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Notes
Author Biography
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.