
Abstract
Concerns about the deservingness of policy beneficiaries appear to explain skepticism about redistributive social assistance programs. Many social insurance programs, despite requiring beneficiaries to pay in ahead of time, require discretionary evaluations of the merits of claims for benefits. Do perceptions of deservingness also affect attitudes toward these discretionary social insurance programs? Examining the politics of Social Security Disability Insurance (SSDI), a program whose size and beneficiaries have been increasingly politicized, we investigate these questions by analyzing novel survey data and two experiments conducted on national surveys. We show that people use information about a beneficiary’s eligibility-determining impairment—but not their race, which prior work argues is a key heuristic—to infer their deservingness. Moreover, support for SSDI is responsive to policy arguments emphasizing the program’s social insurance features and potential abuse. Our findings demonstrate important psychological processes relevant to the contemporary politicization of social insurance programs involving discretionary eligibility rules.
How do citizens form opinions about the merits of benefit provision under social insurance programs? In contrast to universalistic redistributive social assistance programs, most social insurance programs require potential beneficiaries to contribute ahead of time to be eligible to receive benefits in specific, defined circumstances. These programs therefore pool risk among a contributing population and are generally popular relative to redistributive programs that also serve individuals who are in need. 1 However, there is little scholarship examining whether the basis on which social insurance beneficiaries are eligible for and receive assistance affects perceptions of their deservingness. Such concerns are particularly important for understanding the contemporary politics of those social insurance programs where individuals receive benefits only after discretionary determination of the merit of their claim (as compared with programs where eligibility is determined by formal objective criteria like age, as in the case of Social Security and Medicare). As the size and cost of these “discretionary” social insurance programs (often involving case-by-case determinations of the merits of each claim for benefits) have grown over time, new efforts to scale back these programs have emerged and appear, in part, to be motivated by concerns that these programs increasingly pay benefits to those who should not receive them.
Prior work argues that support for redistributive welfare programs is governed by a “deservingness heuristic,” in which the willingness to support programs or benefits for particular beneficiaries is shaped by beliefs about whether beneficiaries demonstrated they warrant care. 2 Perceptions of the deservingness of welfare beneficiaries in general are correlated with support for welfare (i.e., cash assistance), and differences in perceptions of deservingness across individuals (e.g., across beneficiaries of different races) are correlated with differences in support for providing benefits to those individuals (e.g., Appelbaum, 2001; Gilens, 1999). This raises the question of whether, despite key differences in program design, the psychological processes explaining mass attitudes toward program beneficiaries are similar for social assistance and discretionary social insurance programs. Specifically, are beneficiaries of discretionary social insurance programs evaluated on the basis of the same “deservingness heuristic” that prior work shows is a powerful predictor of attitudes toward those receiving welfare and other social assistance programs? And do perceptions of the race of program beneficiaries, which prior work shows is a key predictor of attitudes toward support for redistributive spending (Gilens, 1999), also affect beliefs about the deservingness of Social Security Disability Insurance (SSDI) recipients? In this regard, SSDI is a useful case for study because it is not an overtly racialized policy domain, although individuals may perceive it as such.
We investigate this question using the case of support for the SSDI program. SSDI is a large and growing social insurance program in the United States that provides cash assistance to individuals who have a severe, long-term disability that interferes with work. 3 Theoretically, SSDI combines a social insurance program design with support for individuals who have been determined to have a health-driven disability that prevents work. It is therefore an ideal case for understanding the interplay of these two factors—the requirement to pay in ahead of time and discretionary determination of the merit of a claim for receiving benefits—in shaping program support. The program is funded by worker payroll taxes and provides benefits only to those who have met recent work and earnings requirements. Because of the program’s social insurance features such as prior contribution requirements and the limited basis for claiming benefits, SSDI (and SSDI recipients) may be broadly popular. In recent decades, however, the number of individuals successfully obtaining SSDI has increased substantially, accompanied by changes in who is participating (increasingly working-age men) and the basis for being declared disabled (increasingly certain musculoskeletal and mood disorders) (Autor & Duggan, 2003). To some observers, these changes show that the core function of the program has changed from being last-resort social insurance to a subsidy for individuals who choose not to work. 4 What is unknown, however, is whether these changes have had any effect on support for SSDI. Is support for SSDI beneficiaries, or for the program more generally, related to beliefs about whether those seeking benefits are in fact unable to work, or do the program’s social insurance features blunt these concerns about deservingness? Relatedly, if support for SSDI beneficiaries is partly a function of their perceived deservingness, what are relevant markers of beneficiaries that people use to form perceptions of their deservingness? Is beneficiary race a relevant factor in shaping opinions toward the program despite its social insurance features and lack of past history of racialization?
A nascent line of political science research examines support for government-provided health care benefits for sick individuals and finds that those with diseases that are less controllable (e.g., due to a pathogen or genetics rather than failure to exercise) warrant greater support (Jensen & Petersen, 2017). That research has not examined willingness to provide cash assistance to individuals with health impairments, which may differ in important respects from the provision of health care because of the greater possibility of misuse of cash. Nor has that work examined how determinations of merit are affected by different models for eligibility for government benefits (e.g., in the case of medical care, social insurance [like Medicare], means-tested redistributive programs [like Medicaid], universalistic government provision, etc.). Finally, whereas the source of an illness may be an important basis for deciding about the merits of providing government health care, SSDI is designed to compensate individuals not for lost health directly, but instead for the labor income that is lost because an impaired individual is unable to work. The critical question in adjudicating the merit of an SSDI claim, therefore, is whether the claimant is able to work, which, in addition to evaluating whether the person is sick, requires determining whether or not they could work. Thus, even if one broadly believe that sick individuals are deserving of government health care, we do not know if the basis on which one claims medical impairment affects perceptions of deservingness in the social insurance context.
In particular, building on prior theoretical work on deservingness perceptions, we expect that individuals combine cues about beneficiary-level attributes (such as the impairment they have) and group stereotypes (about beneficiaries possessing specific attributes) to form judgments about their deservingness as a function of those attributes. We focus on ease of diagnosis, by which we mean the degree to which an impairment is readily verifiable as preventing work, as a key measure of deservingness (e.g., the true merit of a claim). We expect increased perceptions of undeservingness to be associated with reduced support for a social insurance program like SSDI and its beneficiaries. The need for a discretionary evaluation of the merit of a person’s claim may therefore counteract the general popularity that accompanies social insurance programs where beneficiaries pay into those programs ahead of time. In addition, we compare the effect of beneficiary impairment with another possible marker of deservingness, beneficiary race, to understand the similarity between SSDI and more traditionally racialized policy domains such as welfare. Finally, in light of these countervailing forces and prior research on policy framing effects and historical accounts of the politicization of social insurance in the United States, we test whether public support for social insurance programs is also responsive to policy arguments emphasizing the program’s social insurance features and potential abuse.
To investigate these expectations, we analyze both observational and experimental data from a novel nationally representative survey, supplemented with additional analysis from online convenience samples. Specifically, we begin by measuring knowledge and perceptions of those receiving disability benefits. We find that, on average, individuals report being uncertain about whether those who receive disability could have worked. Thus, despite the social insurance features of the SSDI program, individuals do have beliefs about the relative merits of those receiving benefits and not all are solicitous. In addition, we find that the relative frequency with which individuals believe that those receiving disability could have worked is increasing in the social distance between an individual and the benefit recipient they are evaluating, such that individuals are more skeptical of beneficiaries who are not family members. We also investigate beliefs about the racial composition of the SSDI beneficiary pool and partisan differences in perceptions of the deservingness of program beneficiaries.
Next, we designed and fielded a vignette experiment in a nationally representative survey to investigate whether individuals with medical impairments that are more difficult to diagnose are more likely to be perceived as undeserving of disability benefits as compared with individuals with impairments that are easier to diagnose. Ease of diagnosis therefore proxies verifiability as truly impaired, a marker of deservingness, rather than merely claiming impairment to garner support. We find causal evidence that subjects are much less likely to agree with the government’s decision to grant SSDI benefits to a recipient whose impairment is having a mood disorder as compared with counterfactual recipients with either a job-related physical injury, chronic heart failure, severe arthritis of the spine, or a stroke-induced intellectual disability. This finding supports our theoretical expectation that a beneficiary’s eligibility-determining medical impairment is a relevant attribute others use to form judgments about the beneficiary’s deservingness. This result also has an important policy implication, as it suggests that the inclusion of harder-to-diagnose impairments in the set of medical impairments that determine SSDI eligibility (i.e., the impairment classes that have grown the most with increasing SSDI caseloads in the last 20 years) might explain growing skepticism about the merits of SSDI beneficiaries more generally. We do not find evidence that individuals perceive the SSDI beneficiary pool to overrepresent racial minorities (in contrast to more traditional redistributive spending programs) and the race of a specific SSDI claimant has no effect on perceptions of their deservingness, in contrast to the effects of those cues in the welfare context.
Finally, in a second experiment embedded in a nationally representative survey, we tested whether arguments emphasizing the social insurance features of SSDI or arguments about abuses of the system affect support for the program. We find causal evidence that arguments emphasizing the risk pooling features of SSDI generally increase support for the current SSDI program, whereas arguments emphasizing the program’s costliness and lax eligibility rules generally increase support for stricter eligibility requirements and a smaller program overall. These results provide evidence pushing back against monocausal claims that either a program’s social insurance features or concerns about the deservingness of beneficiaries alone shape social insurance policy attitudes. More narrowly, this is evidence that argumentative appeals about the size, design, and effects of SSDI have effects on attitudes toward the program.
Theoretical Expectations
What explains individuals’ attitudes toward social insurance programs? A large body of research has shown that a person’s attitude toward a public policy is influenced by their personal experience with that policy (e.g., Campbell, 2012; Mettler, 2007) as determined by how a program is designed and implemented and that these personal “policy feedback” effects can be consequential for the political development of public policies and useful for explaining cross-national variation in social policy attitudes (e.g., Hacker, 1998; Skocpol, 1992).
The argument that personal experience with a public policy program affects attitudes toward that program implies that the distribution of attitudes toward a program in the mass public is principally a function of the distribution of the program’s benefits and costs in the population. For many social insurance programs, individuals pay in over time to become eligible and later receive a tangible benefit conditional on meeting some objective criteria (e.g., age rules for Social Security and Medicare). Thus, all individuals who bear the cost of a social insurance program today should expect either that they will likely benefit from the program in the future or if a defined shock occurs (e.g., death of a spouse). These expectations may explain broad support for many social insurance programs, especially compared with support for redistributive welfare programs (e.g., Cook, Barabas, & Page, 2002; Page & Shapiro, 1992).
At the same time, not all social insurance programs provide benefits on the basis of these sorts of non-discretionary evaluations. In the case of SSDI, for example, individuals have to demonstrate a medical impairment that prevents work. In this case, the implementation of the social insurance program, as with many other redistributive programs (e.g., welfare), requires an evaluation of the merits of a claim. In these cases, program design therefore likely causes individuals to think about the deservingness of those who obtain benefits (i.e., granting benefits requires an evaluation of subjective merit, which raises questions about whether each program recipients should qualify). An extensive literature in public opinion and political psychology emphasizes how beliefs about the deservingness of policy beneficiaries plays a key role in shaping policy attitudes (e.g., Friedman, 2019; Gilens, 1999; Larsen, 2008; Petersen, Slothuus, Stubager, & Togeby, 2010, Petersen, Sznycer, Cosmides, & Tooby, 2012; Van Oorschot, 2000). Psychological research has shown that the use of such a “deservingness heuristic” in forming attitudes about social policies is an automatic and affective psychological process that is often more powerful than cultural stereotypes and political values (Cosmides & Tooby, 1992; Feather, 2006; Petersen et al., 2010; Weiner, 1995) and that is shaped by readily available informational cues (Petersen, 2009).
In a synthesis of psychological theories of deservingness, Van Oorschot (2000) notes that, to form perceptions of a benefit recipient’s deservingness, individuals employ informational cues about the recipient’s (1) degree of control over their condition justifying benefits, (2) level of need for benefits, (3) identity in relation to the perceiver, (4) docility and gratefulness for receiving support, and (5) level of reciprocity, operationalized as whether they have earned support. In the case of social insurance programs, unlike traditional redistributive programs, beneficiaries will have demonstrated reciprocity (criterion 5 from above) by previously contributing financially into the risk pool to become eligible. However, individuals in the mass public may still take into account any combination of the other (non-reciprocity) informational cues to form perceptions about the deservingness of beneficiaries, conditional on their beliefs about who receives benefits (Schneider & Ingram, 1993) and who should receive benefits (Wilson, 1986). In the case of SSDI, determining the merit of a claim explicitly requires such a discretionary adjudication of deservingness, deciding that someone cannot work due to a medical impairment.
Motivated by the different arguments raised in these sometimes disparate literatures, we extend prior work on the deservingness heuristic’s role in shaping policy attitudes in four ways. First, we assess whether perceptions about the deservingness of program beneficiaries are also relevant to the politics of discretionary social insurance programs, especially when a program is perceived to benefit a narrow segment of the eligible population and is potentially allocated with error (i.e., to some who are undeserving). Our work therefore departs from prior opinion research, such as work by Cook and Barrett (1992, Ch. 4), which only examines attitudes toward redistributive and non-discretionary social insurance programs (such as Social Security, where eligibility is age based). We focus specifically on the case of SSDI, a program for which the growing size and the deservingness of its beneficiaries have been politicized in recent decades in American politics. We view our focus on a specific social insurance program as an advantage of our study and an important contribution to the study of the politics of actual social insurance programs. By contrast, prior psychological research on the deservingness heuristic tends to abstract away the policy details of specific social insurance programs, which reduces its external validity for understanding actual political conflicts surrounding existing policies.
Second, we assess informational factors that affect how people form perceptions of the deservingness of disability insurance beneficiaries. Building on related work about generic support for government health care benefits for people with different ailments (Jensen & Petersen, 2017), we argue that individuals evaluate the deservingness of policy beneficiaries by making inferences about the beneficiary’s true need in light of the beneficiary’s control over their condition (criteria 1 and 2 above). 5 In this circumstance, this evaluation may apply to whether an individual is responsible for his or her illness, actually ill, and, if ill, whether their impairment prevents work. In effect, we contend that individuals engage in statistical discrimination (e.g., Arrow, 1973; Phelps, 1972) when evaluating beneficiary deservingness by making an inference about the beneficiary’s location on an underlying dimension—their deservingness—as a function of perceived observables that are salient and deemed relevant.
In our empirical analysis, we focus on a realistic and politically relevant informational cue used as a marker of deservingness: the medical impairment causing the recipient to become eligible for and receive benefits. 6 We expect beneficiaries with impairments that are more difficult to diagnose reliably (i.e., the probability that someone with a given diagnosis is not actually ill or, if they are ill, that they are still able to work is smaller) to be perceived as less deserving of receiving benefits as compared with SSDI recipients with impairments that are easier to diagnose reliably (i.e., the probability that someone with a given diagnosis is both truly ill and unable to work is larger). Our notion of ease of diagnosis is linked closely to the idea of whether an impairment is externally verifiable, that is whether it is easy for outsiders to determine whether the (claimed) disease is an actual impediment to work. (While we focus on ease of diagnoses, a related question is whether impairments also affect deservingness through different beliefs about personal responsibility for one’s impairment or other impairment-level biases, a topic we return to in the discussion section.) We expect impairments that are difficult to diagnose (as compared with those that are easy to diagnose) to reduce support for benefits because this can both decrease the mean and increase the variance of one’s belief about the beneficiary’s level of need or their degree of control over the condition justifying benefits. For example, an individual may not believe that an SSDI recipient deserves benefits if the recipient’s impairment is having an anxiety disorder (which is more difficult to reliably diagnose than, say, a spinal fracture) because that individual believes that there is a non-trivial probability that the recipient does not, in fact, have a disability or that, even if he or she has it, that he or she could still find a suitable job. 7
In light of prior research, we also examine how race may affect perceptions of SSDI beneficiaries’ deservingness in two ways. We first examine individuals’ beliefs about the racial composition of those receiving SSDI benefits (in comparison with more traditional redistributive spending programs). Second, in light of past research on how the race of a welfare recipient affects beliefs about their deservingness (e.g., Gilens, 1999), we examine whether an SSDI beneficiary’s race affects beliefs about their deservingness.
In addition, we explore partisan variation in perceptions of beneficiary deservingness and in attitudes toward SSDI. Although disability insurance has long been a non-partisan issue with strong bipartisan support, political analysts have noted that disability insurance has become increasingly polarized along partisan lines in recent years, with polarization on the issue perhaps accelerating during the 2016 presidential election (e.g., Graham, 2016). 8 We expect Democrats (as compared with Republicans) to be more likely to perceive SSDI recipients as deserving benefits. This expectation is consistent with prior psychological research by Skitka, Mullen, Griffin, Hutchinson, and Chamberlain (2002) and Skitka and Tetlock (1992) showing that perceptions of the circumstances causing the need for welfare are correlated with both perceptions of deservingness and ideology, with conservatives being more likely to view the cause of needing aid as laziness and liberals being more likely to attribute the cause of needing aid to circumstances outside of the beneficiary’s control.
Finally, we assess whether arguments about either deservingness or the social insurance features of SSDI shape attitudes toward social insurance programs and beneficiaries. We argue that although concerns about the deservingness of beneficiaries and the social insurance features of SSDI play an important role in shaping social insurance attitudes, they will not eliminate the effects of additional arguments about program design and abuse. Instead, many possible considerations can affect stated policy opinion (e.g., Chong & Druckman, 2007b; Zaller, 1992). To test this expectation, we examine how real-world policy arguments that either support or criticize aspects of the SSDI program affect attitudes about the program’s size and design. Specifically, we test whether arguments highlighting the risk pooling benefits of SSDI or the costs of the SSDI program affect attitudes about SSDI’s size or design. We also test more expansive versions of these arguments that stress the low risk of program abuse by beneficiaries (on top of highlighting the risk pooling aspect of the program’s design) or stress the problem of liberalized eligibility requirements (on top of highlighting the program’s skyrocketing costs). Thus, in addition to theoretical debates about whether one set of considerations dominate the other in shaping attitudes toward social insurance, our analysis also contributes to ongoing debates about the effect of elite discourse—that is, arguments to maintain or retrench social insurance—on social insurance policy attitudes in the mass public.
Data
Our primary data are from items we fielded on a team module of the 2016 Cooperative Congressional Election Study (CCES), a nationally representative, two-wave, stratified sample survey of adults in the United States administered by YouGov/Polimetrix. The two waves of the CCES were fielded before and after the 2016 general election in November. Our study includes 1,145 respondents from the pre-election survey and 1,231 respondents from the post-election survey (932 respondents took both surveys). Our samples from the pre- and post-election surveys are demographically similar to the nationally representative sample from the 2016 CCES Common Content file (Ansolabehere & Schaffner, 2017; see Supplemental Appendix Table A1).
We first analyze these data to make descriptive inferences about perceptions of the deservingness of SSDI beneficiaries among U.S. adults. In both the pre- and post-election surveys of our CCES team module, we included multiple survey items to measure these perceptions. We supplement these data from the CCES with additional data from a census-balanced convenience sample of 3,034 U.S. adults recruited between December 8, 2017 and January 9, 2018, using Lucid, an online survey sampling firm, 9 as well as a sample of 1,287 respondents recruited from Lucid during May 7 to 9, 2019, to understand beliefs about the demographic composition of those receiving SSDI.
We also analyze data from two experiments embedded in our CCES team module to answer our causal questions of interest. In the pre-election survey, we embedded a vignette experiment to assess the causal effect of informational cues about a hypothetical SSDI recipient’s impairment on subjects’ perceptions of the recipient’s deservingness. In the post-election survey, we embedded a second experiment to assess the causal effect of SSDI-specific policy arguments on attitudes about the program’s design and size. We supplement these experiments with a similar experiment from 2019 in which we also manipulate the beneficiary’s race to understand the causal effect of race on perceptions of their deservingness. For clarity, we describe the details of each design alongside our analysis of the data gathered using that design.
Descriptive Results: Perceptions of SSDI Beneficiaries
We begin by documenting Americans’ perceptions of SSDI beneficiaries they know and beneficiaries in general. First, in the CCES pre-election survey, we measured respondents’ perceptions of the deservingness of other SSDI recipients whom they personally know. To ensure that respondents knew what SSDI is, we first briefly described the program in the following way: The Social Security Disability Insurance (SSDI) program is a federal program paying benefits to people who cannot work because they have a medical condition that is expected to last at least one year or result in death. The program requires benefit recipients to have paid Social Security payroll taxes for a certain number of years and to earn below a monthly income threshold.
We then asked respondents to consider four groups: anyone else in your household, anyone in your extended family, any of your friends, and anyone in your community. 10 For each of these groups, respondents were asked whether they knew anyone who has received SSDI benefit payments and, if so, whether they legitimately received benefits or illegitimately received benefits (i.e., they could have worked).
Table 1 presents the distribution of respondents’ knowledge and perception of other SSDI beneficiaries across various reference groups. We describe these perceptions among all respondents (Panel I) to present the raw data, as well as among respondents who know anyone in their own household and anyone outside of their household receiving SSDI (Panel II). This restriction allows us to examine perceptions of deservingness among the subset of respondents who can evaluate multiple beneficiaries varying in social distance.
Reported Knowledge and Perception of Other SSDI Benefit Recipients, by Social Reference Group.
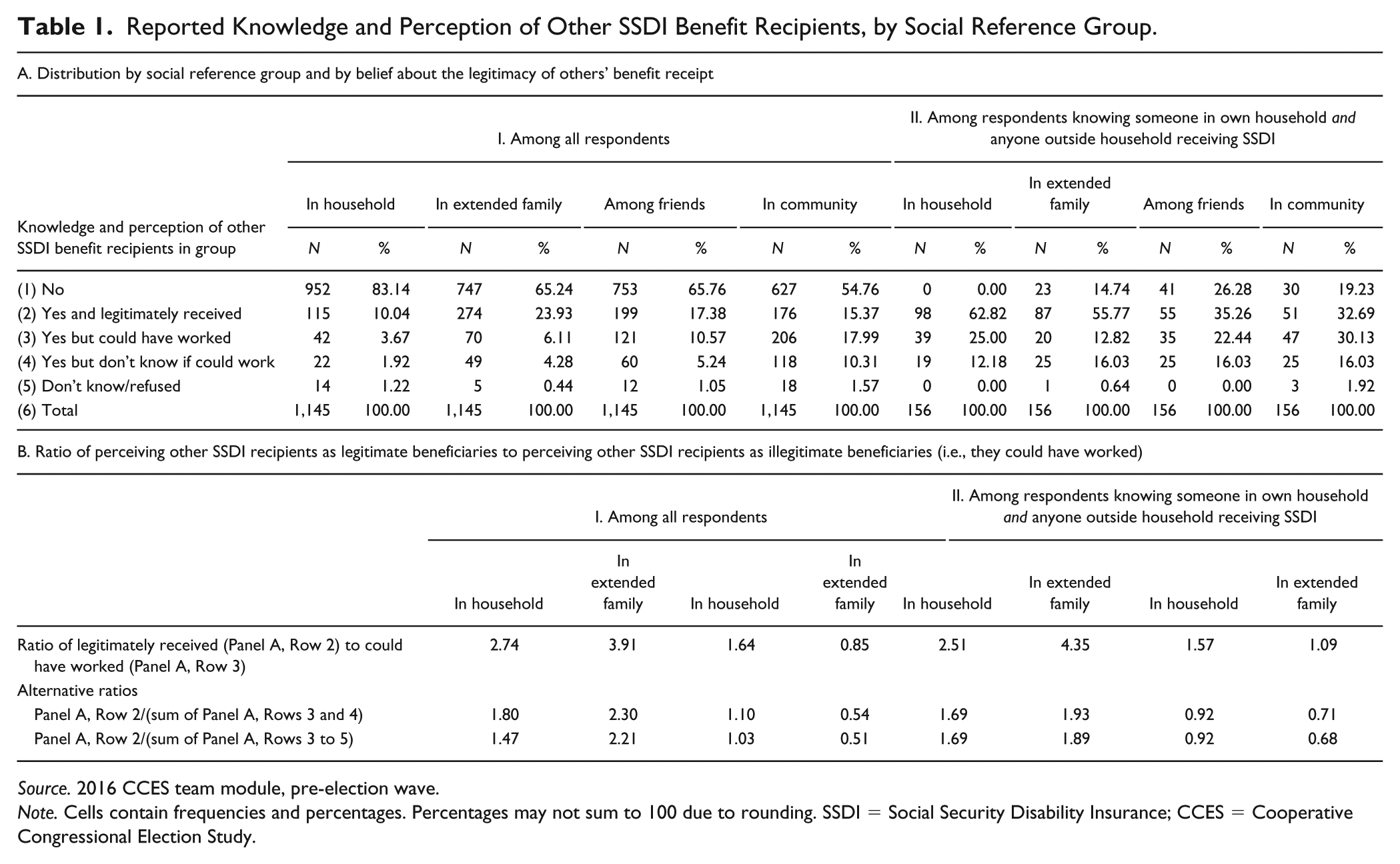
Source. 2016 CCES team module, pre-election wave.
Note. Cells contain frequencies and percentages. Percentages may not sum to 100 due to rounding. SSDI = Social Security Disability Insurance; CCES = Cooperative Congressional Election Study.
The marginals shown in the top panel of Table 1 reveal two striking patterns. First, across all social reference groups, a majority of respondents do not know of others who receive SSDI benefits. However, of those who do, perceptions that the SSDI recipient is illegitimately receiving benefits (row 3) increase in the social distance between the respondent and the benefit recipient (i.e., moving from left to right in the table). Even when focusing on the subset of respondents who know of beneficiaries both in and outside of their household (Panel A, II), we observe a similar pattern where the average respondent is more likely to view the beneficiary as legitimately receiving benefits than not as the social distance between the respondent and the beneficiary decreases.
To quantify this association, we also calculate, by social reference group, the ratio of the number of respondents who know an SSDI recipient who is perceived as legitimately receiving benefits (row 2) to the number of respondents who know an SSDI recipient who is perceived as illegitimately receiving benefits (row 3). 11 Ratios greater than (less than) 1 mean that respondents, on average, are more (less) likely to perceive SSDI recipients in a given reference group as legitimately receiving benefits. As shown in Table 1, these ratios tend to be larger when respondents think about beneficiaries in proximal groups (within one’s household or in one’s extended family) as compared with those in distal groups (among friends or the extended community). 12
Next, we examine respondents’ perceptions of SSDI beneficiaries in general. In the post-election survey, we asked respondents to estimate the share of SSDI recipients who “are in fact able to work but do not want to work”; respondents could select either “0-20% (Few),” “20-40%,” “40-60%,” “60-80%,” “80-100% (Most),” or “Don’t know.” 13 Figure 1 presents, overall and by the respondent’s partisanship, 14 the distribution of estimates of the perceived share of SSDI recipients who can but do not want to work.
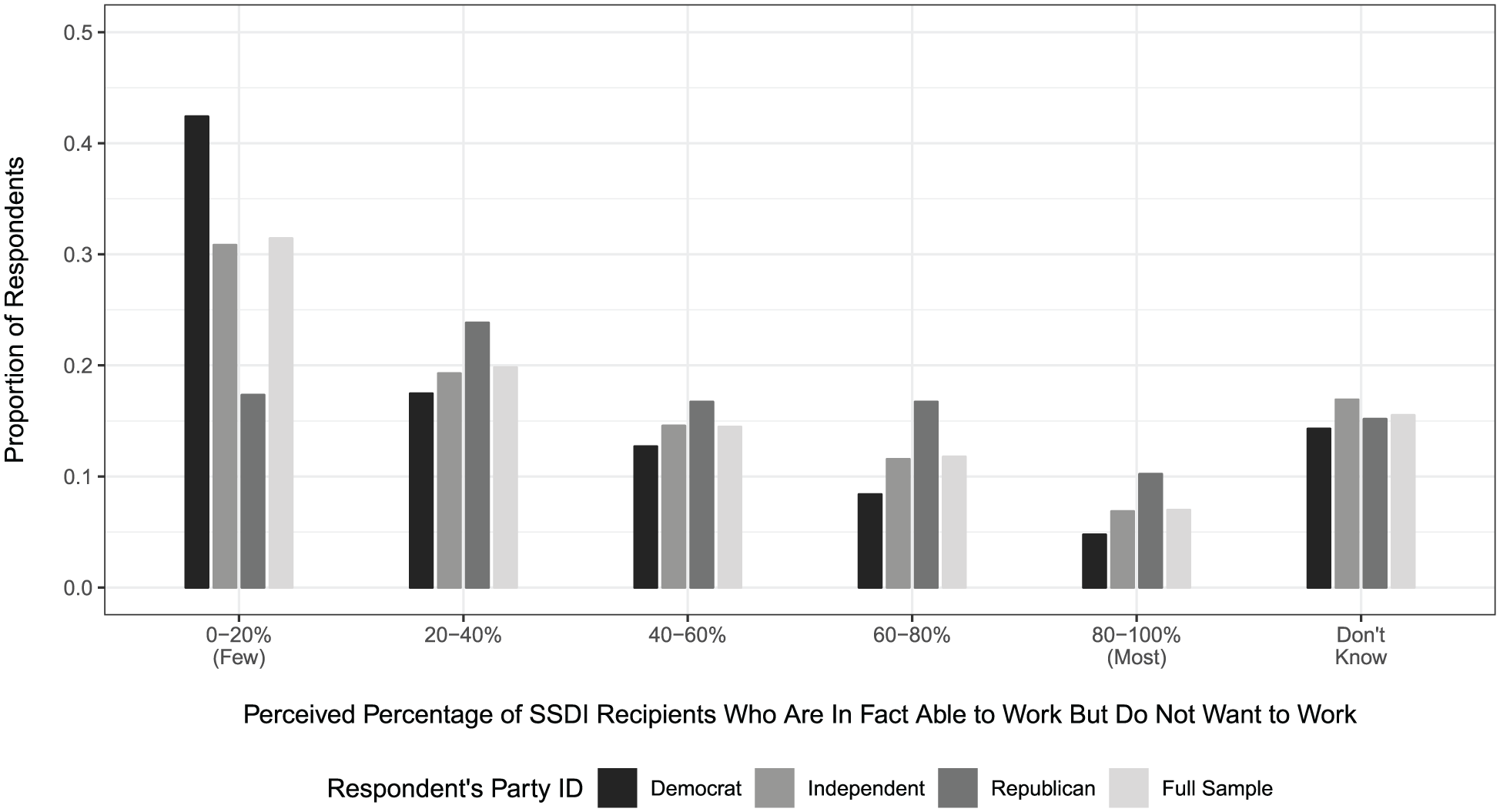
Perceptions of the Percentage of SSDI Recipients who Are Able to Work but Do Not Want to Work, by Respondent Party Identification.
Most importantly, the figure reveals that there are widespread perceptions that a substantial share of SSDI recipients are cheating the system by collecting disability insurance despite being able to work. Among the 1,040 respondents who report a perception (85.5%) of the 1,231 total respondents in the post-election survey, 653 (62.8%) perceive that at least 20% of SSDI recipients can but do not want to work, and the median respondent perceives this level to be between 20% and 40%. We find similar results in our Lucid sample, where respondents estimated that on average about 43 of every 100 SSDI beneficiaries could have worked. 15
One possible explanation for skepticism about the true need of SSDI beneficiaries, highlighted by prior research, is that individuals may perceive the SSDI program as racialized. To assess this possibility, in our 2019 Lucid survey, we asked respondents to consider SSDI and another randomly assigned social policy program—either Temporary Assistance for Needy Families (TANF) [welfare], Medicaid [welfare], or Social Security [social insurance]—and to estimate for each the share of program beneficiaries they believe are Black or African American, women, and born in the United States. 16 As shown in Supplemental Appendix Figures A4 and A5 and Supplemental Appendix Table A16, on average, respondents do not believe that Blacks and African Americans comprise a disproportionate share of SSDI beneficiaries. Focusing on partisan subgroups, Republicans (as compared with Democrats) are more likely to perceive redistributive welfare programs as serving minorities, but this partisan difference does not extend to social insurance programs. Beliefs that racial minorities are overrepresented in the SSDI recipient pool therefore do not seem likely to explain skepticism about these beneficiaries’ deservingness, particularly in contrast to those welfare programs that are perceived (especially by Republicans) as racially targeted.
At the same time, consistent with claims that SSDI has become politicized along party lines, we find that perceptions of the pervasiveness of cheating are correlated with partisanship. Among respondents reporting a perception, Republicans are more likely than Independents, who are more likely than Democrats, to perceive a larger share of SSDI recipients as being able to work but not wanting to. Among both Democrats and Independents, the median respondent perceives that between 20% and 40% of SSDI recipients are able to work but do not want to. By contrast, the median Republican respondent perceives this level to be between 40% and 60%. (Per the prior paragraph, however, it seems unlikely that these differences arise because of partisan difference in beliefs about the racial composition of the beneficiary pool.) Formal statistical analyses presented in Supplemental Appendix Table A3 and Supplemental Appendices C.2 and C.3 confirm these partisan differences for both the CCES sample and the 2018 Lucid survey.
Overall, our descriptive results document the prevalence of mass beliefs that disability insurance beneficiaries are undeserving despite the social insurance features of the program. We also show clear evidence of separation in beliefs about the deservingness of SSDI beneficiaries along partisan lines, with Republicans more likely to believe that beneficiaries are undeserving as compared with Democrats. However, average skepticism, as well as differences between the parties, seems unlikely to originate in beliefs, or differences in beliefs, about the race of SSDI recipients. Not only is SSDI not perceived in starkly racialized terms, we also do not find differences between the parties in beliefs about the racial composition of the SSDI recipient pool.
Experiment 1: How Impairment Type Affects Deservingness Perceptions
Experiment 1 is designed to allow us to assess whether informational cues about an SSDI recipient’s impairment type affects others’ evaluations of the recipient’s deservingness. This survey experiment was embedded in the pre-election wave of our CCES team module.
Design
Subjects are presented with the following brief vignette about a hypothetical SSDI recipient: Scott is a 34 year old white male who previously attended two years of college but did not graduate. He had been consistently working and making a living since he was 16, but in the last year he [DIAGNOSIS] and stopped working. Following the diagnosis, with the help of a legal aid attorney, he applied for and was approved to receive monthly disability benefits from the SSDI program.
For the [DIAGNOSIS] field in the vignette, subjects are randomly assigned with equal probability to see one of the following: (a) “was injured on the job”; (b) “suffered a stroke that led to him becoming intellectually disabled”; (c) “was diagnosed with a mood disorder”; (d) “was diagnosed with chronic heart failure”; or (e) “was diagnosed with severe arthritis of the spine.” 17
We designed the treatment conditions, which manipulate the SSDI recipient’s medical impairment, with several considerations in mind. First, the mood disorder condition is our operationalization of a difficult-to-diagnose impairment; the other conditions are intended to represent easier-to-diagnose conditions. 18 Second, we include two conditions—being injured on the job and severe arthritis of the spine—as examples of musculoskeletal disorders, because both musculoskeletal and mental disorders have been the largest growing categories of impairment designations that have been associated with growth in the disability rolls. To isolate the effect of varying the impairment on perceptions of recipient deservingness, we hold fixed all other information about the SSDI benefit recipient in the vignette across treatment arms.
Notably, the hypothetical SSDI recipient in our vignette displays potentially high markers of deservingness across all treatment conditions, having worked consistently for almost two decades. Because the types of informational cues about disability insurance beneficiaries one might encounter in the real world likely involve multiple, bundled pieces of information about their (lack of) deservingness, we argue that the estimated effects of difficult-to-diagnose impairment cues on perceptions of recipient deservingness in this setting can be interpreted as a lower bound for this class of effects.
To measure subjects’ evaluation of the deservingness of the SSDI beneficiary, subjects are then asked: “Do you agree or disagree with the government’s decision to allow Scott to collect SSDI benefit payments? (1 = Strongly disagree; 2 = Disagree; 3 = Neither disagree nor agree; 4 = Agree; 5 = Strongly agree).” For ease of interpretation, we rescale the outcome variable to range from −2 (Strongly disagree) to 2 (Strongly agree). 19
Results
How does an SSDI beneficiary’s impairment type affect others’ evaluation of their deservingness? Figure 2 presents mean agreement scores with 95% confidence intervals by impairment type for the pooled sample (Figure 2(a)) and by the subject’s party identification (Figure 2(b)). 20
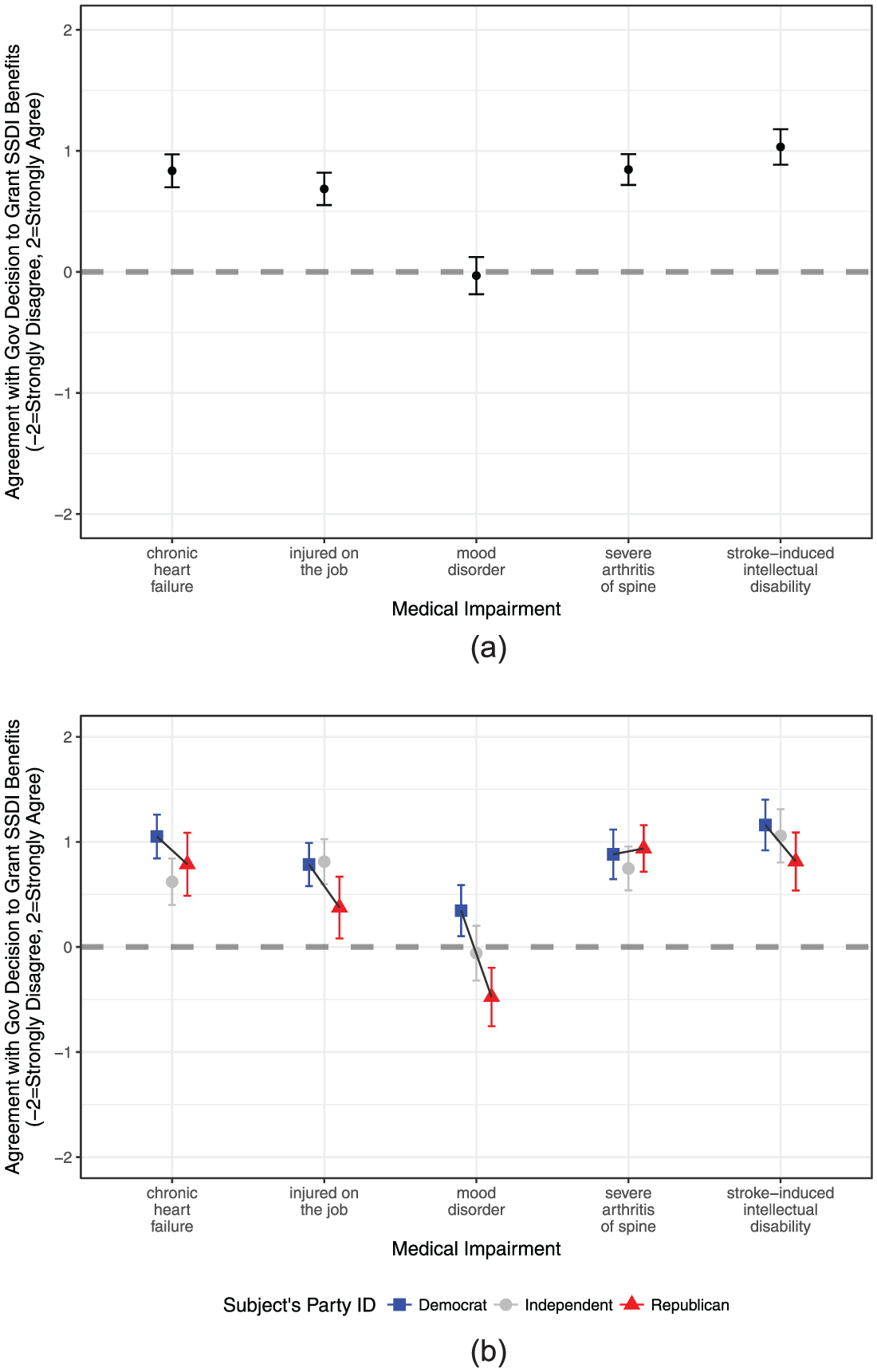
Mean levels of agreement with government decision to grant SSDI benefits to recipient by the medical impairment of the SSDI benefit recipient, among all subjects (a) and by partisanship (b), with 95% confidence intervals.
Figure 2(a) shows that subjects assigned to consider an SSDI recipient with easier-to-diagnose impairments agree with the government’s decision to grant benefits to the hypothetical recipient on average. The estimated mean agreement score is 0.686 (SE = 0.069) if the beneficiary was injured on the job, 0.835 (SE = 0.071) if the beneficiary has chronic heart failure, 0.846 (SE = 0.071) if the beneficiary has severe arthritis of the spine, and 1.032 (SE = 0.073) if the beneficiary has a stroke-induced intellectual disability. When testing the null that each of these means equals zero (i.e., a neutral evaluation), all of these means are statistically significant at the 1% level.
By contrast, considering an SSDI beneficiary with a mood disorder (i.e., a harder-to-diagnose impairment) causes a decrease in support for the government’s decision to grant them benefits as compared with considering counterfactual beneficiaries with easier-to-diagnose impairments such as a job-related injury 21 (difference = −0.72 points, SE = 0.099), chronic heart failure (difference = −0.87 points, SE = 0.10), severe arthritis of the spine (difference = −0.88 points, SE = 0.10), and a stroke-induced intellectual disability (difference = −1.06 points, SE = 0.10). 22 Each of these differences is statistically significant at the .01 level and remains significant even after applying a Bonferroni correction to account for multiple testing. 23
Importantly, these effects are also substantively significant. The mean agreement score in the mood disorder condition is −0.031 (SE = 0.071) and not statistically distinguishable from zero. Thus, on average, whereas beneficiaries with easier-to-diagnose impairments are considered deserving of receiving SSDI benefits, beneficiaries with harder-to-diagnose impairments such as a mood disorder are not considered deserving.
In our 2019 Lucid study, we expanded our experimental design to examine the influence of recipient race on perceptions of their deservingness. This allows us to understand both the relative importance of information about the impairment of disability insurance beneficiaries on perceptions of their deservingness and whether beneficiary race is itself a piece of information individuals draw on to assess deservingness (the race heuristic effect found in prior work on welfare). In this experiment, we modified the prior vignette design in three ways. First, we randomized the SSDI recipient’s race to be White or African American. Second, in the interest of preserving statistical power, we reduced the number of recipient impairment conditions from 5 to 3, such that the recipient could either be injured on the job, have a mood disorder, or have an intellectual disability due to stroke. Third, we changed the name of the SSDI recipient from Scott to Michael, as the latter (but not the former) name is one that is more plausibly held by both Whites and African Americans.
We first replicate the main finding from Experiment 1 and show in the left panel of Supplemental Appendix Figure A7 that subjects perceive SSDI recipients as being less deserving if the recipient has a mood disorder (as compared with either being injured or having an intellectual disability due to a stroke). This result is driven by both Democrats and Republicans in the sample: The effect of the recipient having a mood disorder as compared with having a job injury is −0.39 for Democrats (SE = 0.12, p < .01), −0.17 for Independents (SE = 0.19, n.s.), and −0.67 for Republicans (SE = 0.14, p < .01). Next, as shown in the right panel of Supplemental Appendix Figure A7, we assess the average effect of recipient race on perceived deservingness and find no effect of an African American beneficiary (as compared with a White beneficiary) on perceived deservingness (estimate = −0.05, SE = 0.07, p = .42). Supplemental Appendix Figure A9 shows that recipient race does not affect deservingness perceptions across partisan subgroups: The effect of the recipient being African American (as compared with White) is −0.04 for Democrats (s.e = 0.10, n.s.), 0.16 for Independents (SE = 0.15, n.s.), and −0.21 for Republicans (SE = 0.11, p < .1). Figure 3 presents mean deservingness perceptions by recipient race and recipient impairment, clearly showing that differences in deservingness perceptions are only causally attributable to differences in recipient’s impairment type, and not to differences in the recipient’s race.
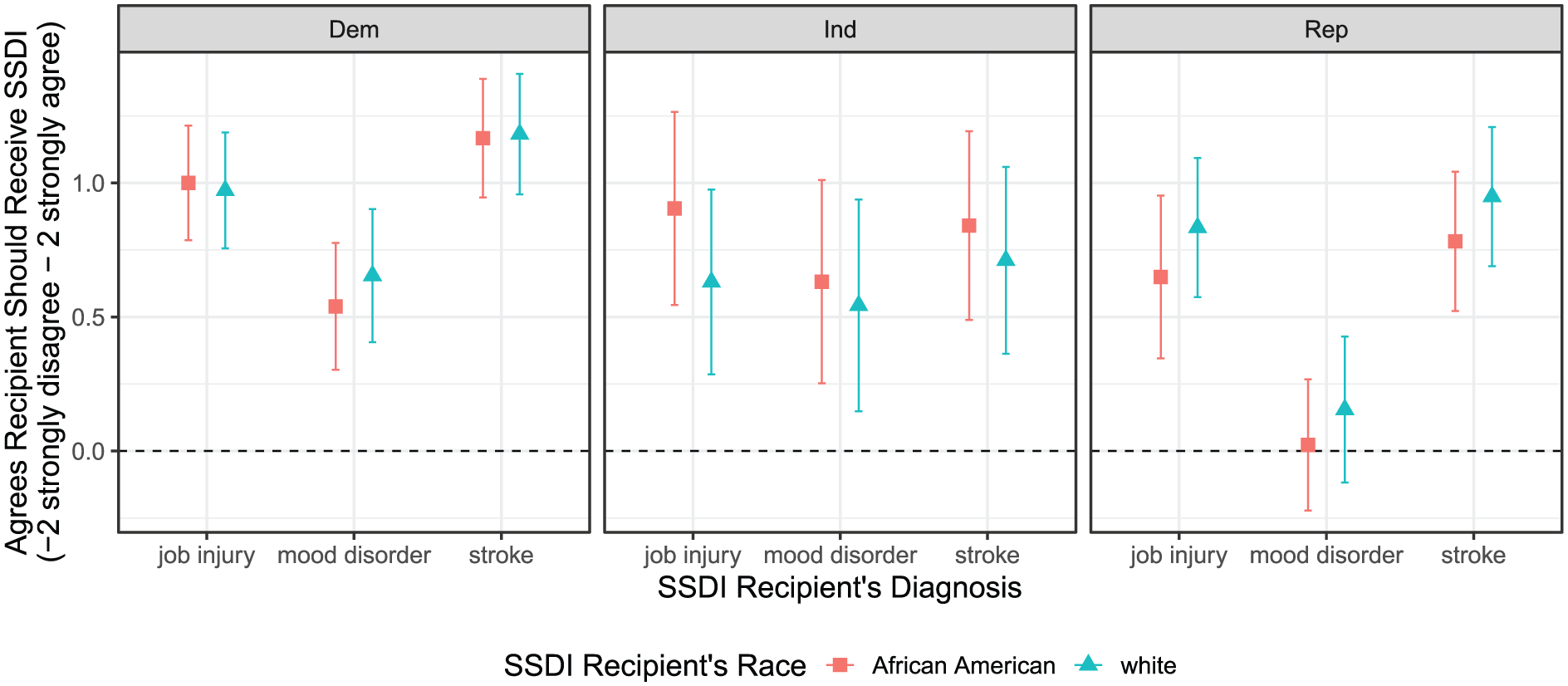
Mean deservingness perceptions by recipient race, recipient impairment, and subject’s party.
These results show that, for social insurance programs like SSDI, the beneficiary’s condition that is used in discretionary evaluations of the merits of claims for benefits (in this case the beneficiary’s impairment type) is a primary heuristic used to form deservingness perceptions, trumping a racial cue when it is available. These results also cut against the conventional wisdom in political science research that the perceived deservingness of social policy beneficiaries is primarily shaped by the beneficiary’s race for both redistributive welfare programs and social insurance programs. 24
We also explored whether there are partisan differences in how SSDI recipients with varying impairments are evaluated. 25 Figure 2(b) displays mean agreement scores by impairment type and by the subject’s partisanship. The figure shows that a partisan gap exists between Democrats and Republicans in their perceptions of the deservingness of SSDI recipients for some easier-to-diagnose impairments and for a specific class of harder-to-diagnose impairments, mood disorders. Democrats are more likely than Republicans to perceive an SSDI recipient as being deserving of benefits if the recipient has a mood disorder (difference = 0.822 points, p < .01) or is injured on the job (difference = 0.410, p = .02). We also find suggestive evidence that Democrats are more likely than Republicans to perceive an SSDI recipient as being deserving of benefits if the recipient has an intellectual disability due to stroke (difference = 0.347, p = .06) or has chronic heart failure (difference = 0.264, p = .15). 26 We find no difference between Democrats and Republicans’ evaluations of the deservingness of recipients with severe arthritis of the spine (difference = −0.056, p = .73).
These results raise the possibility that a person’s partisanship moderates the effect of an SSDI beneficiary’s impairment type (i.e., whether it is harder or easier to diagnose) on how that person evaluates the deservingness of the beneficiary. We are theoretically agnostic about whether such an interaction effect exists. On one hand, a larger partisan gap in deservingness perceptions may exist for harder-to-diagnose impairments than for easier-to-diagnose impairments if there are partisan differences in the extent to which co-partisan elite rhetoric emphasizes and makes salient the notion that an SSDI recipient with a harder-to-diagnose impairment may not deserve benefits. On the other hand, there may be no difference in partisan gaps in deservingness perceptions between harder- and easier-to-diagnose impairments if the impairment cue contains the same information, is similarly construed, and has the same average effect for all subjects regardless of party.
To test these competing expectations, we regress the agreement score on impairment type treatment indicators (excluding the mood disorder condition as the comparison group), party identification dummies for Democrats and Independents (excluding Republicans as the comparison group), and treatment-by-party interactions. We also estimate a second regression of agreement on a coarsened binary treatment indicator for any easier-to-diagnose impairment, the same party dummies for Democrats and Independents (excluding Republicans), and treatment-by-party interactions. For both estimating equations, we test the null hypothesis that the coefficients on the treatment by Democratic interactions are equal to zero using two-sided tests. 27 The estimated coefficients on the impairment-by-Democratic interactions are consistently negative. In the model containing interactions involving specific impairments, two of the interactions (workplace injury and stroke-induced intellectual disability) are statistically significant at the 10% level, the chronic heart failure by Democratic interaction is significant at the 5% level, and the spinal arthritis impairment by Democratic interaction is significant at the 1% level. In the model pooling all easier-to-diagnose treatments into a single coarsened treatment indicator, the effect of easier-to-diagnose impairments (as compared with a harder-to-diagnose mood disorder impairment) on mean perceptions of deservingness is smaller by 0.57 points (SE = 0.20, p < .01) for Democrats than for Republicans. These results provide evidence that, on average, Republicans are more likely than Democrats to view an SSDI beneficiary with a harder-to-diagnose impairment (i.e., mood disorders) as less deserving of benefits as compared with a beneficiary with an easier-to-diagnose impairment.
Taken together, the results from the first experiment show that others’ perceptions of whether an SSDI recipient deserves benefits are causally affected by the type of impairment the recipient has: SSDI recipients with harder-to-diagnose impairments (in this case a mood disorder) are perceived as less deserving of disability insurance benefits than counterfactual recipients with easier-to-diagnose impairments. Moreover, these results make clear that a person’s partisan identity is correlated with how they use information about an SSDI recipient’s impairment to form perceptions about their deservingness: The effect on an SSDI beneficiary’s perceived undeservingness of harder-to-diagnose impairments (as compared with an easier-to-diagnose impairment) is larger for Republicans than for Democrats.
Experiment 2: How Policy Arguments Affect Program Attitudes
In Experiment 2, we assess the causal effect of policy arguments about SSDI on policy attitudes toward the program’s size and design, focusing specifically on how subjects thought an individual’s impairment status and work status should affect benefit eligibility. This survey experiment was embedded in the post-election wave of our CCES team module.
Design
In this experiment, subjects first read a short paragraph providing a description of the SSDI program. Subjects were then randomly assigned with equal probability either to a pure control condition (where no additional information is provided) or to one of the following four treatment conditions presenting a different policy argument about SSDI: (a) a pro-SSDI argument highlighting the advantages of risk pooling, (b) a pro-SSDI argument that highlights the advantages of risk pooling and additionally provides assurances that the probability of program abuse is low, (c) an anti-SSDI argument highlighting the growing and high costs of the SSDI program, or (d) an anti-SSDI argument that highlights the growing and high costs of the SSDI program and additionally attributes the program’s growth to the liberalization of the program’s screening criteria. 28 The treatment arguments were modeled on real-world policy arguments about SSDI that have been articulated publicly by national think tanks. 29 Because these treatments are compound arguments inspired by real-world political arguments, treatment effects may be more difficult to detect either because subjects already know the argument (and thus their attitudes are unlikely to be moved by information they already know) or because they may be perceived as muddled (see, for example, Chong & Druckman, 2007a).
Subjects are then asked whether they strongly agree, agree, neither agree nor disagree, disagree, or strongly disagree 30 with six randomly ordered evaluative statements about the SSDI program: (a) the federal government is spending too much on SSDI benefit payments; (b) it is a major problem that people capable of working are instead opting for the disability rolls when confronted with employment challenges; (c) individuals with non-severe medical impairments, such as mood disorders and chronic fatigue or pain, should not be considered eligible for SSDI benefits; (d) individuals with less severe impairments and residual capacities to work should be encouraged to return to work at a new job compatible with their capacity to work; (e) people should be allowed to exceed the monthly income threshold (US$1,130 per month at the time the study was fielded) while still receiving SSDI benefits; and (f) SSDI, a government program, should be replaced with a policy where all employers are mandated to provide full-time employees with long-term disability insurance that is at least as generous as the SSDI program.
Our main outcome measures are the extent to which subjects agree with statements (a) through (d), because these items measure subjects’ attitudes about the size and design of the SSDI program that are theoretically expected to be affected by the treatments. Responses to statement (a) measure subjects’ general policy attitudes about the size of the SSDI program, which are plausibly affected by arguments about the risk pooling benefits of SSDI or about the total costs of the program. Responses to statements (b) and (d) are related to subjects’ attitudes about whether and how benefit receipt depends on one’s employment situation, which are plausibly affected by arguments priming considerations about who receives SSDI benefits and about their deservingness. Similarly, responses to statements (c) and (d) are related to subjects’ attitudes about how SSDI eligibility should be a function of the severity of an applicant’s impairment, which may also be affected by arguments priming considerations about who receives SSDI benefits and their deservingness. Importantly, all of these primary outcome measures implicitly prime considerations about the risk pooling features of SSDI social insurance and the deservingness of SSDI recipients, and thus offer leverage to test whether either precludes persuasion along the other dimension. Specifically, if we find that the appeals have no effect on attitudes, then that would be consistent with the claim that either set of considerations dominates. To reduce the likelihood of demand effects, we include the other two statements ((e) and (f)) as items that are seemingly unrelated to the content of the treatment appeals and for which the expected effect of the appeals on attitudes is theoretically ambiguous ex ante. 31 Outcomes are measured on a five-item scale and are rescaled to range from −2 (Strongly disagree) to 2 (Strongly agree) for ease of interpretation. On all outcome measures, positive values are coded to be directionally consistent with anti-SSDI attitudes.
Results
How do policy arguments about SSDI affect attitudes toward SSDI’s size and design? Figure 4 presents, for each primary outcome (i.e., agreement with statements about the SSDI policy), unadjusted group means with 95% confidence intervals by experimental condition. 32
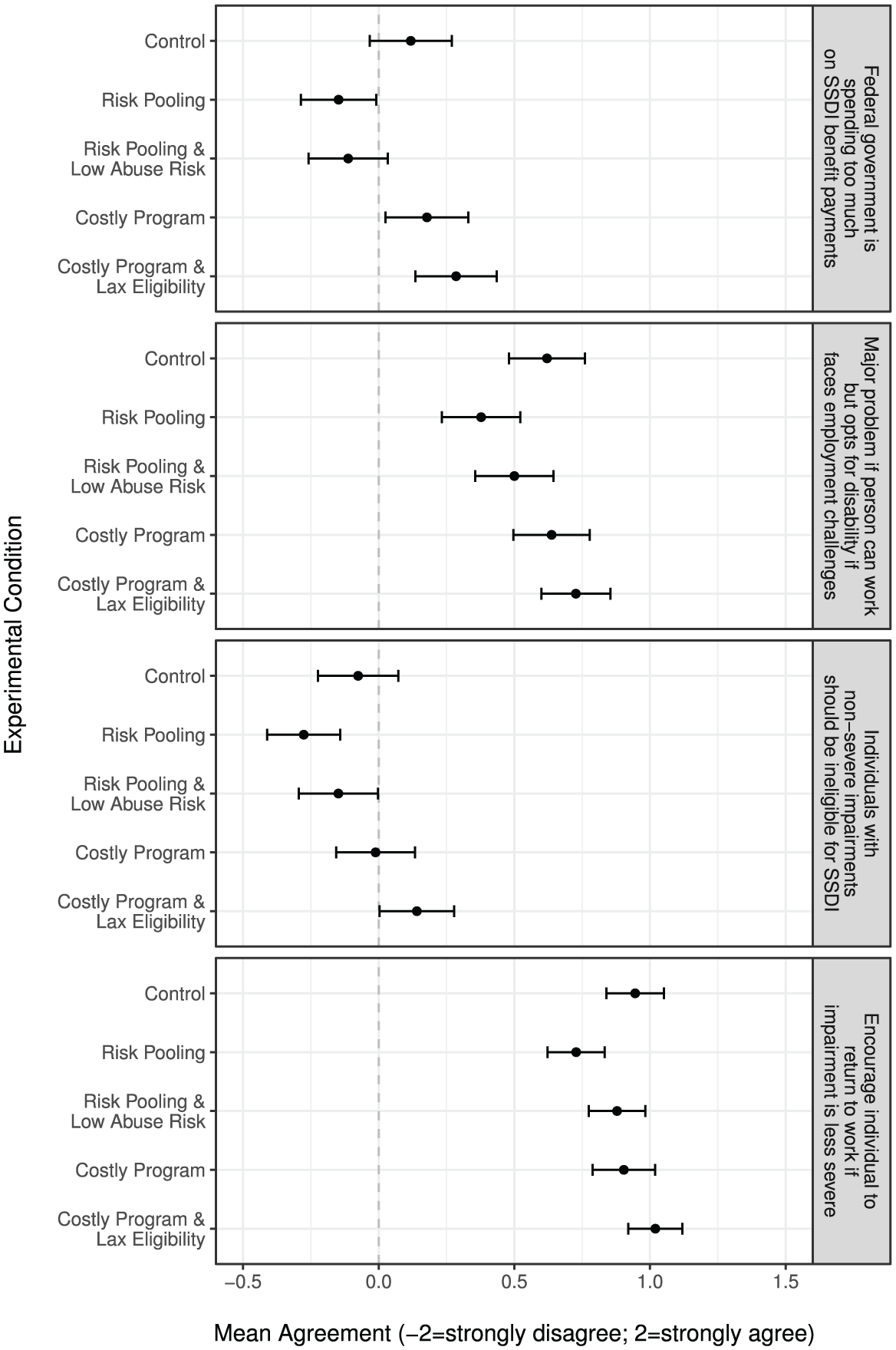
Informational appeals about the SSDI program and SSDI program attitudes.
The estimated effects of the risk pooling appeal relative to the control condition are consistently negative across all outcomes, suggesting that arguments emphasizing the risk pooling logic of SSDI increase support for SSDI. As compared with the pure control condition (no additional appeal provided), the risk pooling treatment decreases mean levels of agreement with the statement that the federal government spends too much on SSDI benefits from 0.118 to −0.148 (difference = −0.266, SE = 0.11, p = .01) and decreases mean levels of agreement with the statement that individuals with less severe impairments should be encouraged to return to work at a new job compatible with their capacity to work from 0.945 to 0.727 (difference = −0.218, SE = 0.08, p = .005).
When the risk pooling appeal includes additional information that the risk of program abuse is low, we observe similar effects only for attitudes about the size of the SSDI program: The mean agreement level decreases from 0.118 in the control condition to −0.113 in the risk pooling plus low abuse risk condition (difference = −0.231, SE = 0.11, p = .04). For the other outcomes, the estimated effects remain negative but are smaller in magnitude and not statistically distinguishable from zero. We speculate ex post that differences in effects between the risk-pooling-only arm and the risk pooling plus low program abuse arm may be due to the fact that informing subjects about the low risk of abuse could be priming those concerns, allaying those concerns, or doing both.
Next, we evaluate the effects of anti-SSDI arguments. We find that the estimated effects of appeals emphasizing both the costliness of the SSDI program and concerns about the liberalization of screening criteria are generally positive across all outcomes, suggesting that this combination of arguments moves attitudes in the anti-SSDI direction. Notably, as compared with the control condition, the costly program and lax eligibility treatment increases mean levels of agreement with the statement that non-severe impairments should not be considered eligible for SSDI benefits from −0.076 to 0.141 (difference = 0.217, SE = 0.10, p = .04). By contrast, the estimated mean effects of appeals that only emphasize the costliness of the SSDI program, while mostly positive, are smaller in magnitude and statistically indistinguishable from zero.
These results suggest that two dominant policy arguments about SSDI that exist in contemporary American political discourse have diverging effects on mass attitudes toward SSDI. Whereas arguments emphasizing the risk pooling features of SSDI tend to increase support for the program’s size and the status quo design, arguments emphasizing the costliness of the program and reasons for its growing costs tend to move attitudes in the opposite direction. 33 Overall, the results from this experiment show that informational appeals containing policy arguments about both the positive (social insurance and risk sharing) and negative (potential abuse leading to undeserving beneficiaries) implications of politicized social insurance programs like SSDI can affect the direction of public support for these programs.
Discussion
As public social insurance programs at the core of the modern American social safety net and the beneficiaries of these programs have become increasingly politicized, an important but underexamined set of questions about the politics of social insurance programs have emerged. First, to what extent do heuristics about the deservingness of program beneficiaries, which play a key role in explaining the contours of mass opinion about redistributive social assistance programs, also matter for mass opinion about social insurance programs, particularly those that require a discretionary determination of eligibility to receive benefits? Second, to what extent do informational appeals emphasizing the social insurance design and potential abuse of these programs affect support for social insurance programs?
To address these questions, we focus on the case of the SSDI program, a politically contested social insurance program in the contemporary United States. Analyzing novel survey data and two experiments conducted on the 2016 CCES as well as supplementary survey data from a large online convenience sample, we report three main sets of results.
First, we document surprisingly widespread skepticism about the deservingness of SSDI recipients. We uncover high baseline levels of concern across all citizens that cheating among SSDI beneficiaries is frequent, and find that many individuals believe that a substantial portion of SSDI recipients could, if they wanted to, work—our operationalization of illegitimately receiving benefits. This skepticism increases in the social distance between the recipient and the perceiver and by the perceiver’s partisanship. Individuals are more likely to perceive other SSDI recipients who they know as illegitimately receiving benefits as the social distance between the perceiver and the recipient increases. Republicans are about twice as likely as Democrats to perceive significant shares of SSDI recipients as receiving benefits illegitimately. In contrast to many other policy domains that have been described as racialized, however, we find little evidence that individuals believe SSDI serves minorities at disproportionate rates. These descriptive findings enrich our understanding about the content of the social imagery of SSDI beneficiaries and their deservingness and how these perceptions correlate with both political and social factors. More generally, they also reveal that, despite the social insurance features of SSDI, individuals have concerns about the deservingness of SSDI beneficiaries.
Second, we test whether realistic informational cues about the medical impairment causing an individual to receive SSDI benefits have a causal effect on others’ perceptions about the recipient’s deservingness. Using an original vignette experiment where subjects are asked to evaluate whether they agree with the government’s decision to grant SSDI benefits to a hypothetical individual, we find causal evidence that SSDI recipients with harder-to-diagnose impairments (i.e., mood disorders) are viewed as less deserving of disability benefits than otherwise identical recipients with easier-to-diagnose impairments. In addition to shedding light on how politically relevant cues about SSDI beneficiaries affect perceptions of their deservingness, these findings also have theoretical implications for our understanding of the logic of mass attitudes toward social insurance beneficiaries in programs with discretionary determinations of eligibility. Our results show that heuristics about the deservingness of social insurance beneficiaries—specifically information about their level of need and information about their control over their condition, both of which are bundled in the impairment cue—affect individual beliefs about the deservingness of beneficiaries. Accordingly, the pattern of attitudes toward social insurance beneficiaries looks strikingly similar to the pattern of attitudes toward welfare recipients when the benefit recipient is perceived as undeserving. Moreover, we show that partisanship moderates the effect of cues about recipients’ impairments on individuals’ perceptions of the deservingness of disability insurance recipients.
At the same time, we also document that beneficiary race, a factor that prior work shows affects perceptions of beneficiary-level deservingness in the case of welfare, does not affect perceptions of the deservingness of a specific SSDI beneficiary. Therefore, whereas deservingness perceptions are important for understanding the contours of support for SSDI benefits, race is not a relevant factor in this domain.
Third, we test whether common policy arguments emphasizing pro- and anti-SSDI policy considerations affect attitudes about the SSDI program’s size and aspects of the program’s design. We find causal evidence that arguments emphasizing the risk pooling features of SSDI generally increase support for the current SSDI program, whereas arguments emphasizing the program’s costliness and lax eligibility rules generally increase support for stricter eligibility requirements and a smaller program overall.
Our investigation of the role of deservingness heuristics in how people form attitudes toward SSDI contributes to ongoing social scientific debates about the psychological processes explaining mass support for social insurance programs and seeks to motivate additional scholarship to understand the politics of disability insurance in particular and the politics of social insurance programs more broadly. We note several potential avenues for future research. First, in the same way that prior scholarship on welfare politics was enriched by understanding common and focal perceptions of welfare beneficiaries, additional research on (a) the stereotypes people hold about who receives and deserves social insurance benefits and (b) how these stereotypes are both formed and revised is needed to develop a concrete understanding of the considerations and social images people have in mind when forming attitudes toward politicized social insurance policies.
Second, future work investigating the effects of cues about the deservingness of beneficiaries on perceptions about their deservingness may be advanced in several ways. In this article, we only tested the effects of two types of real-world cues: the medical impairment causing an individual to become eligible to receive SSDI benefits, which bundles two sets of informational cues about the recipient’s level of need and their level of control over their condition and their race. Future research should test the effect of other theoretically motivated real-world cues (such as individuals’ employment histories, decisions, and contexts), the effects on attitudes of unbundled informational cues, and interaction effects on attitudes of multiple cues. Doing so would provide leverage to test competing hypotheses about the channels through which cues affect attitudes and about the relative importance of competing cues. We find the strongest disease-level concerns about deservingness for a mood disorder, a type of impairment where individuals may have greater skepticism about both an individual’s claim to illness and whether it interferes with work. For other diseases, for example, chronic back pain, individuals may be much more willing to believe that an accurate diagnosis prevents work but may instead have skepticism about whether an individual can prove they have that condition. One idea would be to have individuals read simulated applications that lay bare these distinctions (verifiability of condition vs. impact if true) and assess deservingness.
In addition, future work should further investigate whether and how subjects’ partisanship moderates the effect of these cues on perceptions of beneficiary deservingness. Finally, the impairments we tested in Experiment 1 were purposely designed to be broad and potentially vague for subjects who are expected to lack specialized medical knowledge to achieve treatment realism. As an extension to this feature and limitation of our design, future work could also test whether providing additional information about the onset, diagnosis, and consequences of a given impairment (especially those considered more difficult to diagnose) affects others’ perceptions of an SSDI recipient with that impairment. At present, we have made assumptions about why individuals with certain impairments, like mood disorders, are more likely to be viewed skeptically when claiming SSDI benefits, but it would be desirable to measure the inferences individuals make about people with different medical conditions directly.
Third, additional research is needed on the effects of informational appeals on policy attitudes about the size and design of social insurance programs. Additional experimental replications with larger samples are needed to precisely identify effects. As was the case with Experiment 1, we also prioritized treatment realism in Experiment 2 and tested realistic policy arguments that contained multiple appeals to forcefully make specific arguments. Doing so allowed us to assess the causal effects of common policy arguments on policy attitudes, to document how targeting individuals with diverging appeals leads to divergence between groups in support for SSDI, and to conduct a first-order evaluation of the claim that each type of appeal can affect policy support. But this approach also limited our ability to test the effect of specific appeals and combinations of appeals on attitudes. Future experiments should therefore design treatment appeals to isolate the effect of theoretically motivated appeals on attitudes. To further investigate how people form social insurance policy attitudes in realistic information environments, future research should additionally test the effects of competing appeals on policy attitudes, how policy appeals interact with individuals’ social and political information environments to affect these attitudes, whether individuals misperceive the prevalence of impairments, and how treatment effects are moderated either by the prevalence of impairments (actual or perceived) or by the misperception of prevalence.
Finally, this article investigated the psychological processes underlying the formation of mass attitudes about a specific, politicized social insurance program in the United States involving discretionary evaluations of the merits of claims for benefits: SSDI. To better understand the role of deservingness across social insurance programs, future work should examine how deservingness matters in shaping program attitudes across different types of discretionary social insurance programs and whether the role of the deservingness heuristic in shaping program support varies between social insurance programs with discretionary versus non-discretionary eligibility rules.
Supplemental Material
anon_onlineappendix – Supplemental material for Perceptions of Deservingness and the Politicization of Social Insurance: Evidence From Disability Insurance in the United States
Supplemental material, anon_onlineappendix for Perceptions of Deservingness and the Politicization of Social Insurance: Evidence From Disability Insurance in the United States by Albert H. Fang and Gregory A. Huber in American Politics Research
Footnotes
Acknowledgements
We thank the reviewers and editor for their comments and advice, and Alex Coppock and Jacob Hacker for helpful conversations and feedback.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Institution for Social and Policy Studies and Center for the Study of American Politics at Yale Univerity. The author(s) received no other financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.