
Abstract
Introduction
The optimal neoadjuvant strategy for locally-advanced esophageal squamous cell carcinoma (ESCC) remains controversial. This study aimed to compare the efficacy and safety of neoadjuvant chemoimmunotherapy (NCIT), chemoradiotherapy (NCRT), and chemotherapy alone (NCT).
Methods
We retrospectively analyzed perioperative clinical data from ESCC patients treated with NCIT, NCRT, or NCT at the National Cancer Center in China from 2009 to 2023. The primary outcomes were pathological response, survival, recurrence pattern and surgical complications.
Results
Clinicopathological data from 462 patients (NCIT=122, NCRT=195, NCT=145) were analyzed. The pathological complete response (pCR) rate in the NCIT group (29.5%) was comparable to the NCRT group (28.7%) but significantly higher than the NCT group (3.4%). The overall postoperative complication rate in the NCIT group was higher than in the NCT group (33.6% vs. 14.5%, p<0.001) but comparable to the NCRT group (33.6% vs. 28.2%, p=0.309), with a manageable level. The overall recurrence rates were lower in NCIT (27.0%) than NCRT (48.2%) and NCT (44.1%). Notably, the distant metastasis rate in the NCIT group was significantly lower than that in the NCRT group (11.5% vs. 22.1%, p=0.017) and the NCT group (11.5% vs. 22.8%, p=0.016). As for long-term survival, the 5-year overall survival rate for NCIT was 72.5%, significantly higher than both NCRT (55.7%, p<0.001) and NCT (60.8%, p=0.004). Similarly, the 5-year recurrence-free survival rate for NCIT was 70.7%, significantly surpassing both NCRT (49.8%, p<0.001) and NCT (46.2%, p<0.001). No significant survival differences were observed between the NCRT and NCT groups.
Conclusion
NCIT provides a significant survival benefit over both NCRT and NCT in locally advanced ESCC in real-world clinical practice, achieving a comparable pCR rate to NCRT and decreased recurrence rate. It’s a favorable neoadjuvant option, with the potential to be a novel treatment strategy. Prospective randomized trials to validate our findings are warranted.
Keywords
Introduction
ESCC poses a significant global health challenge due to its highly aggressive nature and poor prognosis. 1 Although multi-modal treatment strategies have evolved, identifying the optimal neoadjuvant modalities for locally-advanced resectable ESCC (LA-ESCC) remains a central and unresolved issue in clinical practice. NCRT remains the standard of care for LA-ESCC, supported by high-level evidence.2,3 Nevertheless, long-term survival remains sub-optimal for a substantial proportion of patients due to high recurrence rate, underscoring the compelling need for more effective therapeutic strategies.
The advent of immunotherapy has transformed the therapeutic landscape. Capitalizing on the efficacy of immune checkpoint inhibitors in advanced disease,4-7 NCIT has been rapidly integrated into clinical practice. Growing clinical evidence8-10 supports the promising efficacy of this strategy, which is characterized by considerable pathological complete response (pCR) rates and improved survival outcomes.
However, the rapid integration of NCIT into clinical practice has sparked considerable debate concerning its efficacy relative to the established standard of care (NCRT and NCT). Consequently, the optimal selection of these modalities remain uncertain. While some studies, including that by Guo et al, 11 report superior survival with NCIT compared to NCRT, other study reveal no difference in efficacy and toxicity profiles. 12 To date, direct head-to-head comparisons of NCIT, NCRT, and NCT according to real-world data are scarce. The difference of the three treatment modalities in the real world is unknown. Therefore, the evidence base remains limited and requires further validation.
To address this critical evidence gap and contribute to optimizing neoadjuvant therapy for LA-ESCC, we performed a large-sample, three-arm, retrospective study. This study aimed to systematically compare the efficacy and safety profiles of NCIT, NCRT, and NCT in a real-world cohort. Our findings are expected to provide robust evidence to guide clinical decision-making and inform the design of future prospective trials.
Materials and Methods
Patient Selection
In this retrospective cohort study, we followed the STROBE guidelines.
13
We included patients with LA-ESCC who received NCIT, NCRT, or NCT at the National Cancer Center in China from 2009 to 2023. The inclusion criteria as follows: (1) age ≥18 years; (2) histopathologically confirmed ESCC with pretreatment clinical stage T1-4aN+ or T3-4aN0
14
; (3) treatment with NCIT, NCRT or NCT; (4) normal physical performance and acceptable for surgery. Exclusion criteria included (1) other malignancies, (2) other types of preoperative treatments, and (3) loss to follow-up or clinical data. The flow chart of enrolled patients is shown in Figure 1. This study was performed after approval by the Ethics Committee of Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College. Written informed consent was waived because of retrospective study. Flowchart of enrolled patients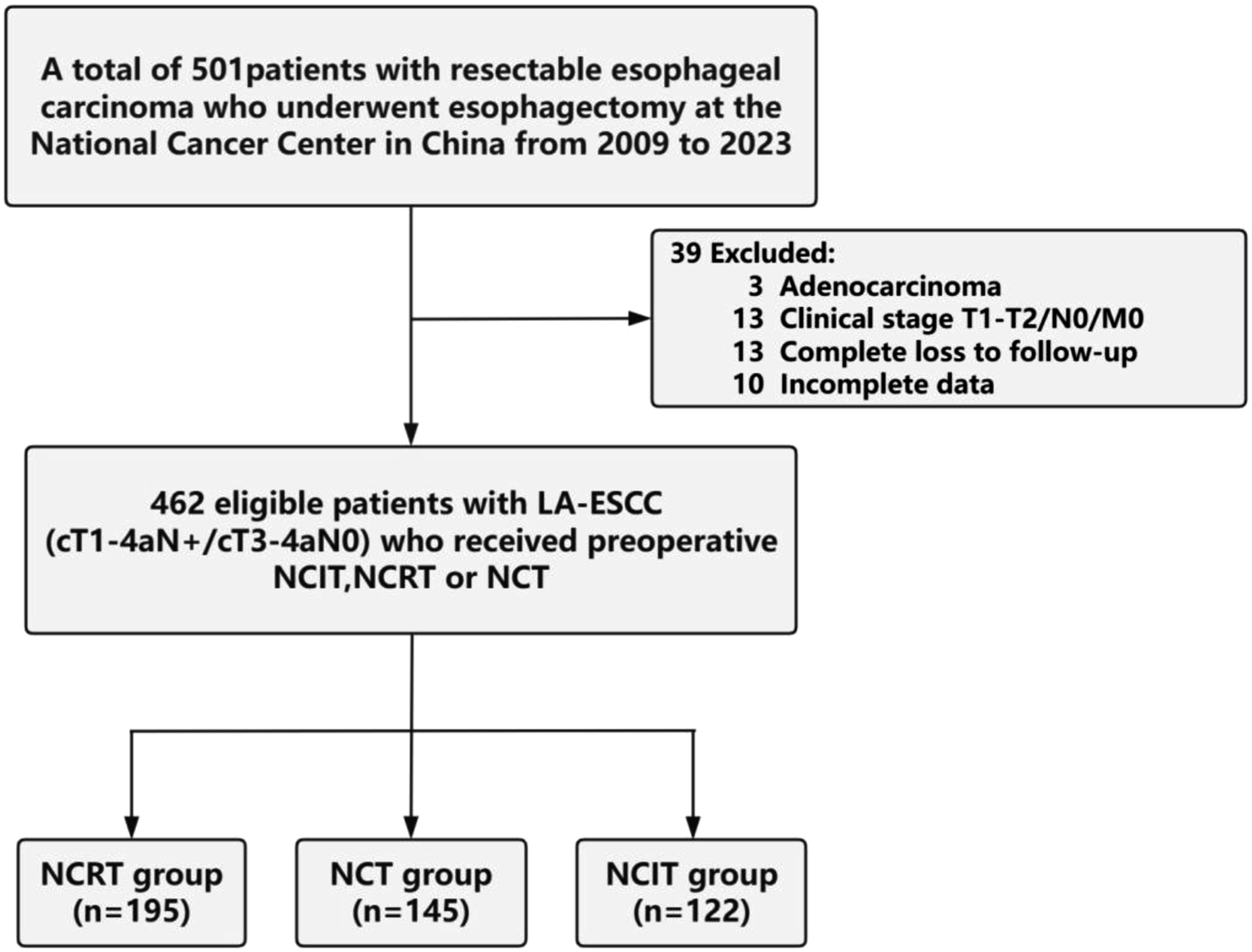
Perioperative Treatment
The neoadjuvant treatment strategy was determined by multidisciplinary team (MDT) consensus. The immune checkpoint inhibitors (ICIs) are not fully covered by health insurance. Therefore, after obtaining the informed consent, patients in the NCIT group received two cycles of platinum-based doublet chemotherapy combined with ICIs—such as pembrolizumab, camrelizumab, tislelizumab, or sintilimab—administered every three weeks. In contrast, the NCRT group received two cycles of similar platinum-based chemotherapy concurrent with radiotherapy. Usually, a total radiation dose of 40.0-41.4 Gy was given in 20-23 fractions of 1.8-2 Gy each, with 5 fractions administered per week. Adjuvant nivolumab may be considered for patients who fail to achieve pCR following NCRT. With regard to patients in NCT group, at least two cycles of platinum-based dual-drug chemotherapy was performed. In this study, the chemotherapy regimens and ICIs types of neoadjuvant therapy are shown in Table S1.
Following neoadjuvant therapy, disease reassessing and restaging was performed using positron emission tomography with integrated computed tomography (PET-CT) or contrast-enhanced CT of the chest and abdomen. Decisions regarding adjuvant therapy were based on the final pathological stage and postoperative recovery. Typically, patients in the NCIT group were recommended to receive one year of adjuvant ICIs therapy, especially for those who did not achieve pCR.
Surgical Procedures
The patients underwent radical esophagectomy following neoadjuvant therapy. The different surgical methods were performed according to the tumor location and status of mediastinal lymph-node, including minimally invasive Mckeown and Ivor-Lewis. Another small group of patients underwent open esophagectomy. First, the patients underwent thoracoscopic or open esophagectomy with mediastinal lymphadenectomy. Subsequently, proximal gastrectomy and dissection of peri-gastric lymph node was performed, and the distal stomach was made into a tube stomach. The 3-field lymphadenectomy would be performed if indicated. Afterwards, a gastric tube was pulled into the apex of the chest or left neck through esophageal bed, and an esophagogastric anastomosis was conducted.
Pathologic Evaluation, Follow-Up, and Study Outcomes
Pathological staging was assessed using the 8th edition of the American Joint Committee on Cancer (AJCC) TNM staging system. Surgical complications occurring within 30 days postoperatively were identified and defined according to the Esophagectomy Complications Consensus Group (ECCG) criteria. 15 R0 resection was defined as a microscopically margin-negative resection, with no tumor cells identified at the distal, proximal, and circumferential margins. The pCR was defined as the absence of viable tumor cells in both the primary tumor and all sampled regional lymph nodes (ypT0N0). Tumor response to neoadjuvant therapy was evaluated in the primary tumor bed using the Mandard tumor regression grade (TRG) system, categorized as follows: TRG 1, complete regression with no viable tumor cells; TRG 2, rare residual cancer cells scattered within predominant fibrosis; TRG 3, considerable residual cancer cells, but fibrosis still predominates; TRG 4, residual cancer cells outgrow fibrosis, yet evidence of treatment effect is present; TRG 5, Absence of morphological regression or only spontaneous necrosis. The RFS was calculated from the date of first neoadjuvant therapy to the date of disease recurrence or death from any cause. The OS was defined as the time from first neoadjuvant therapy to death from any cause. The location of tumor recurrence was confirmed through imaging examinations performed during patient follow-up (e.g. neck ultrasound, gastroscopy and endoscopic ultrasound, CT, or PET-CT) or through histopathological diagnosis. Recurrence patterns were primarily classified as locoregional recurrence (LR), distant metastasis (DM), and mixed recurrence. LR refers to recurrence in the primary tumor site and regional lymph nodes. DM mainly denotes distant organ metastasis and non-regional lymph node metastasis, such as lung metastasis and retroperitoneal lymph node metastasis, while mixed recurrence primarily refers to the concurrent observation of LR and DM.
Statistical Analysis
Categorical variables were summarized as frequencies and percentages, and compared using the Chi-square or Fisher’s exact test, as appropriate. For continuous variables, normality of the data was assessed using the Shapiro–Wilk test, and homogeneity of variances was evaluated with Levene’s test. Data that followed a normal distribution were expressed as mean±standard deviation, and differences between groups were analyzed using Student's t-test or one-way analysis of variance (ANOVA). For non-normally distributed data, results were presented as median and interquartile range (IQR), and group comparisons were conducted using the Kruskal–Wallis test. Survival analyses were performed using the Kaplan-Meier method, and comparisons between groups were made with the log-rank test. Univariate and multivariate Cox proportional hazards models were used to analyze the associations between clinicopathological characteristics (including clinical TNM stage, postoperative pathological stage, pCR, etc.) and long-term prognosis, with multivariate adjustment for prognostic factors. To minimize the potential influence of confounding factors and baseline imbalances among treatment groups on survival outcomes, propensity score matching (PSM) was performed with a ratio 1:1 and a caliper of 0.1. The variables included in the matching model mainly comprised sex, age, BMI, tumor location, and pretreatment clinical TNM stage. After matching, the balance of baseline characteristics between groups was visually and quantitatively assessed using propensity score. A two-sided p-value of < 0.05 was defined as statistically significant. All statistical analyses were conducted using SPSS software (version 23.0, IBM Corp.) and GraphPad Prism (version 9.5.1).
Results
Patient Characteristics
Demographic Characteristics of Enrolled Patients

Abbreviations: MIE, minimally invasive esophagectomy.
Clinicopathologic Characteristics Among Three Treatment Groups

Abbreviations: BMI, body mass index; PNI, perineural invasion; LVI, lymphovascular invasion.
Pathologic Examination
The pCR rate following NCIT was comparable to that achieved with NCRT (29.5% vs. 28.7%, p=0.880), yet significantly superior to that with NCT alone (29.5% vs. 3.4%, p<0.001). Regarding postoperative lymph node status, the ypN0 rate in the NCIT group was 63.1%, which was comparable to that in the NCRT group (73.3%, p = 0.073), but significantly higher than that in the NCT group (45.5%, p = 0.004). The pathological response to neoadjuvant therapy in the primary tumor was evaluated using the Mandard tumor regression grade (TRG) system. The proportion of patients achieving TRG 1 (complete tumor regression) was 36.1% in the NCIT group, which was comparable to that in the NCRT group (33.8%, p=0.686) and significantly superior to that in the NCT group (5.5%, p<0.001). Furthermore, the rate of ypT0 was similar between the NCRT (32.8%) and NCIT (33.6%) groups. The positivity rate for lymphovascular invasion (LVI) was 17.9% in the NCRT group, 33.1% in the NCT group, and 18.9% in the NCIT group (NCRT vs. NCT, p=0.001; NCIT vs. NCT, p=0.009; NCRT vs. NCIT, p= 0.840). The positivity rate for perineural invasion (PNI) was 24.1% in the NCRT group, 43.4% in the NCT group, and 20.5% in the NCIT group (NCRT vs. NCT, p<0.001; NCIT vs. NCT, p< 0.001; NCRT vs. NCIT, p= 0.455) (Figure 2). Pathological outcomes among three cohorts
Surgical Outcomes
Of the 462 enrolled patients, R0 resection was achieved in 458 patients, with only 4 patients having R1 resection. The R0 resection rate remained high across all groups (NCIT: 98.4%, 120/122; NCRT: 99.5%, 194/195; NCT: 99.3%, 144/145) and was comparable among the three groups, with no statistically significant difference observed (p= 0.553). The median number of lymph nodes retrieved in the overall population was 26 (IQR, 18-38). Specifically, the median number of lymph nodes dissected was 41 (IQR, 31-55) in the NCIT group, 20 (IQR, 14-25) in the NCRT group, and 28 (IQR, 20-37) in the NCT group. In the overall study population, 309 patients (66.8%) underwent MIE, while 153 patients (33.2%) underwent conventional open surgery (Table 1). Among these, the NCIT group had the highest proportion of patients undergoing MIE (99.2%, 121/122). In the NCRT group, MIE accounted for 50.8% (99/195) and open surgery for 49.2% (96/195); in the NCT group, MIE accounted for 61.4% (89/145) and conventional open surgery for 38.6% (56/145). Furthermore, the McKeown procedure via a right thoracic approach was the predominant surgical approach across all three treatment groups, while the Sweet procedure via a left thoracic approach was also frequently performed in the NCRT and NCT groups (Figure 3 for details). Of note, among the three study groups, patients in the NCRT group had the highest proportion undergoing open surgery. This might be attributed to the fact that nearly half of the patients in the NCRT group were enrolled between 2009 and 2015, when MIE techniques were far less mature than they are currently. Surgical approaches among the three study groups
Postoperative Complications
Analysis of specific complications revealed distinct safety profiles among the three groups. First, the total complications rate was markedly higher in the NCRT (28.2%) and NCIT (33.6%) groups compared to the NCT group (14.5%), with all pairwise differences reaching statistical significance (NCRT vs. NCT, p=0.003; NCIT vs. NCT, p<0.001). For anastomotic leakage, the incidence was significantly higher in the NCRT group (15.4%) than in the NCT (5.5%, p=0.004) and NCIT (3.3%, p=0.001) groups, while no significant difference was observed between the NCT and NCIT groups (p=0.379). Regarding anastomotic stenosis, the incidence rate in the NCIT group (6.6%) was slightly higher than that in the NCT group (2.1%), but no statistically significant difference was observed (p=0.066). The incidence rate was also similar to that in the NCRT group (4.6%, p=0.455). When comparing the NCRT group with the NCT group, the incidence of anastomotic stenosis in the NCRT group was also slightly higher than that in the NCT group, but no statistically significant difference was observed (p=0.208). For vocal cord paralysis, the NCIT group exhibited a higher rate than the NCT group (9.0% vs. 2.8%, p=0.027), while no significant differences were found between NCIT and NCRT (9.0% vs. 5.1%, p=0.176). Furthermore, the NCIT group had the highest rate of pulmonary complications (11.5%), which was significantly higher than that in the NCT group (4.1%, p= 0.023) but comparable to that in the NCRT group (8.7%, p= 0.421). No significant difference was observed between the NCRT and NCT groups (p= 0.096). No significant differences were observed among the groups in the rates of incision infection (NCRT 3.6% vs. NCT 4.1% vs. NCIT 2.5%) and cardiovascular events (NCRT 3.6% vs. NCT 2.8% vs. NCIT 4.1%). The 30-day mortality rates (NCRT 1.5% vs. NCT 0.0% vs. NCIT 0.0%) showed no statistically significant differences across all groups(shown in Figure 4). Postoperative complications in the NCIT, NCRT and NCT groups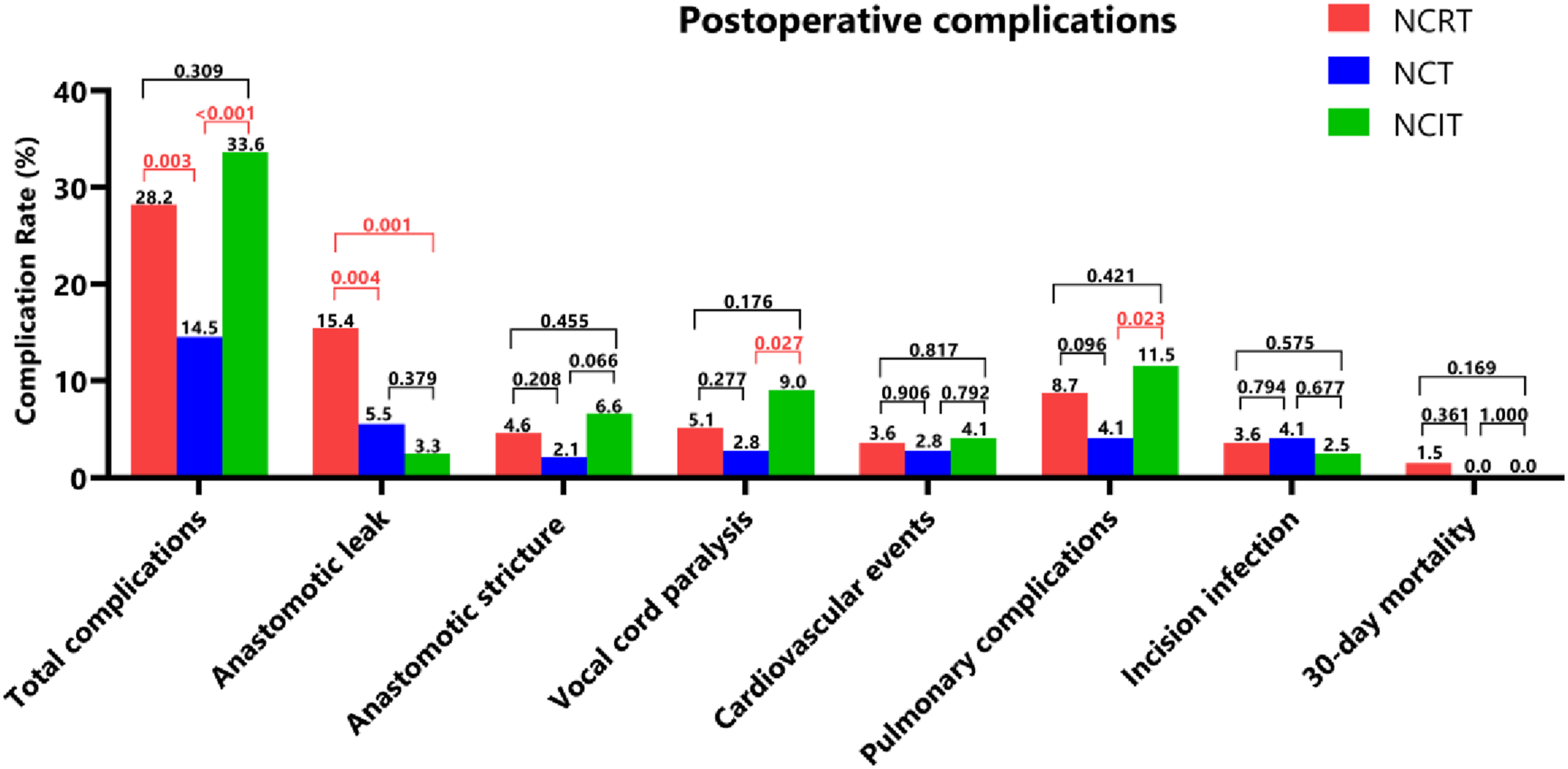
Therefore, the incidence of perioperative adverse events across the three treatment modalities was within an acceptable range, indicating that these approaches were generally safe and manageable. Among them, NCT demonstrated the most favorable perioperative safety profile, while each treatment modality was associated with distinct risks of treatment-related complications.
Recurrence Pattern
Recurrence Patterns in the Three Treatment Groups

Abbreviations: LR, locoregional recurrence; RLN, regional lymph nodes; DM, distant metastasis; RPLD, Retroperitoneal lymph nodes.
Next, this study systematically compared recurrence patterns among the three treatment groups (shown in Figure 5). The results showed that the overall recurrence rate was significantly higher in both the NCRT group (48.2%, 94/195) and the NCT group (44.1%, 64/145) than in the NCIT group (27.0%, 33/122) (p<0.001). In the NCRT group, the incidence of DM was slightly higher than that of LR (43 cases [22.1%] vs. 42 cases [21.5%]); similarly, the NCT group also had a higher DM rate than LR rate (33 cases [22.8%] vs. 27 cases [18.6%]). In contrast, the NCIT group exhibited a lower DM rate compared to its LR rate (14 cases [11.5%] vs. 16 cases [13.1%]). No significant differences were observed among the three groups in LR rates (NCRT 21.5% vs. NCT 18.6% vs. NCIT 13.1%, p= 0.169) or mixed recurrence (Table 3 and Figure 4). However, we observed that the DM rate in the NCIT group was significantly lower than that in the NCRT group (11.5% vs. 22.1%, p= 0.017) and the NCT group (11.5% vs. 22.8%, p= 0.016). Regarding specific sites of DM, the lung remained the most common site across all three treatment groups, followed by the liver and bone. For LR, regional lymph nodes were the most frequent site of recurrence in all three groups. Differences in recurrence patterns among the three treatment groups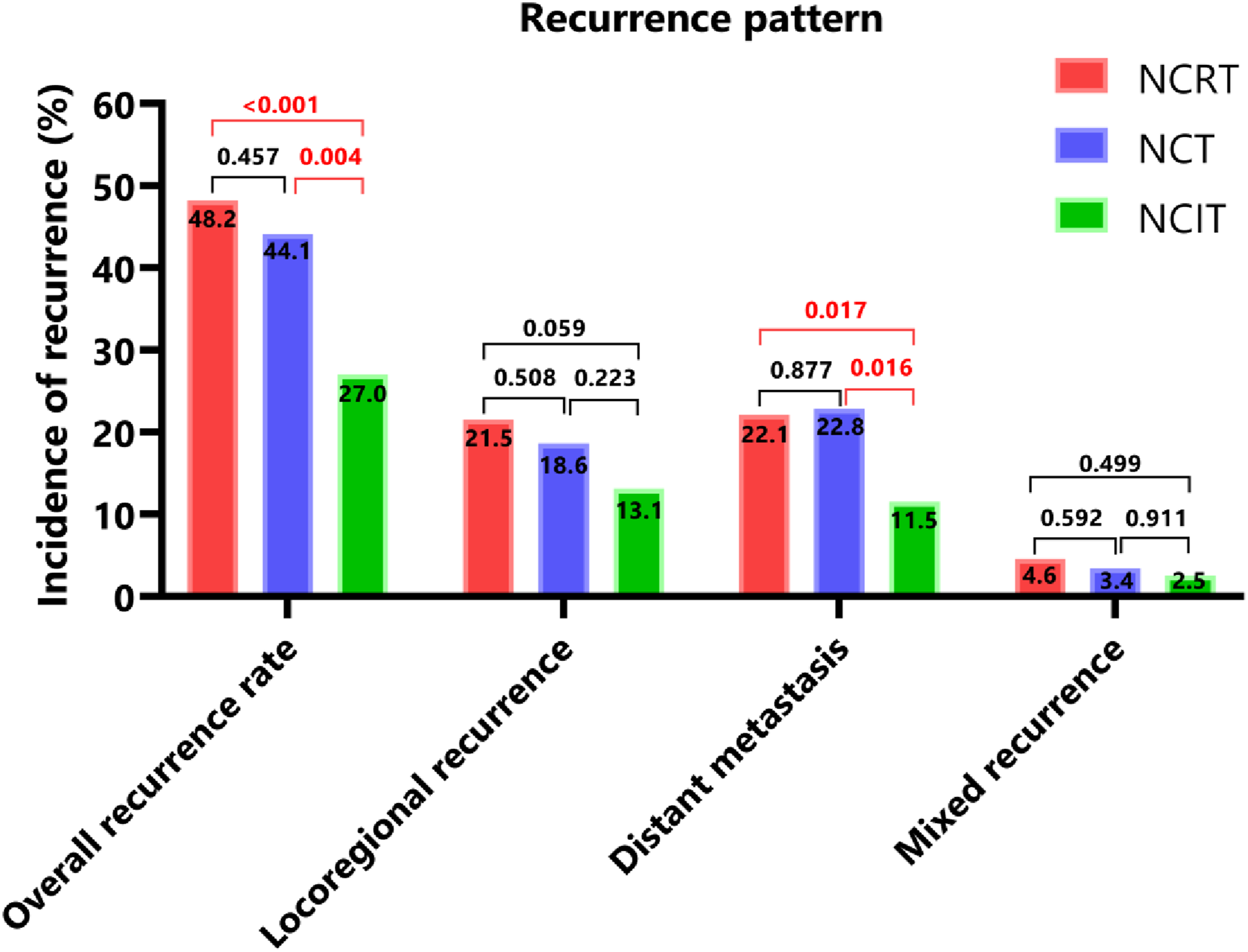
Long-Term Outcomes
The median follow-up durations were 51 months for the NCIT group, 55 months for the NCRT group, and 38 months for the NCT group. The NCIT group demonstrated superior survival outcomes compared to the NCRT and NCT groups. The 5-year RFS rate in the NCIT group was 70.7%, significantly higher than that in the NCRT (49.8%, p < 0.001) and NCT (46.2%, p < 0.001) groups (Figure 6). Similarly, the 5-year OS rate was 72.5% in the NCIT group, which was also significantly superior to those in the NCRT (55.7%, p < 0.001) and NCT (60.8%, p < 0.001) groups (Figure 6A and B). Collectively, these results support NCIT as a promising therapeutic strategy for ESCC. Long-term survival among three neoadjuvant treatment groups and survival analysis between patients achieving pCR and those with non-pCR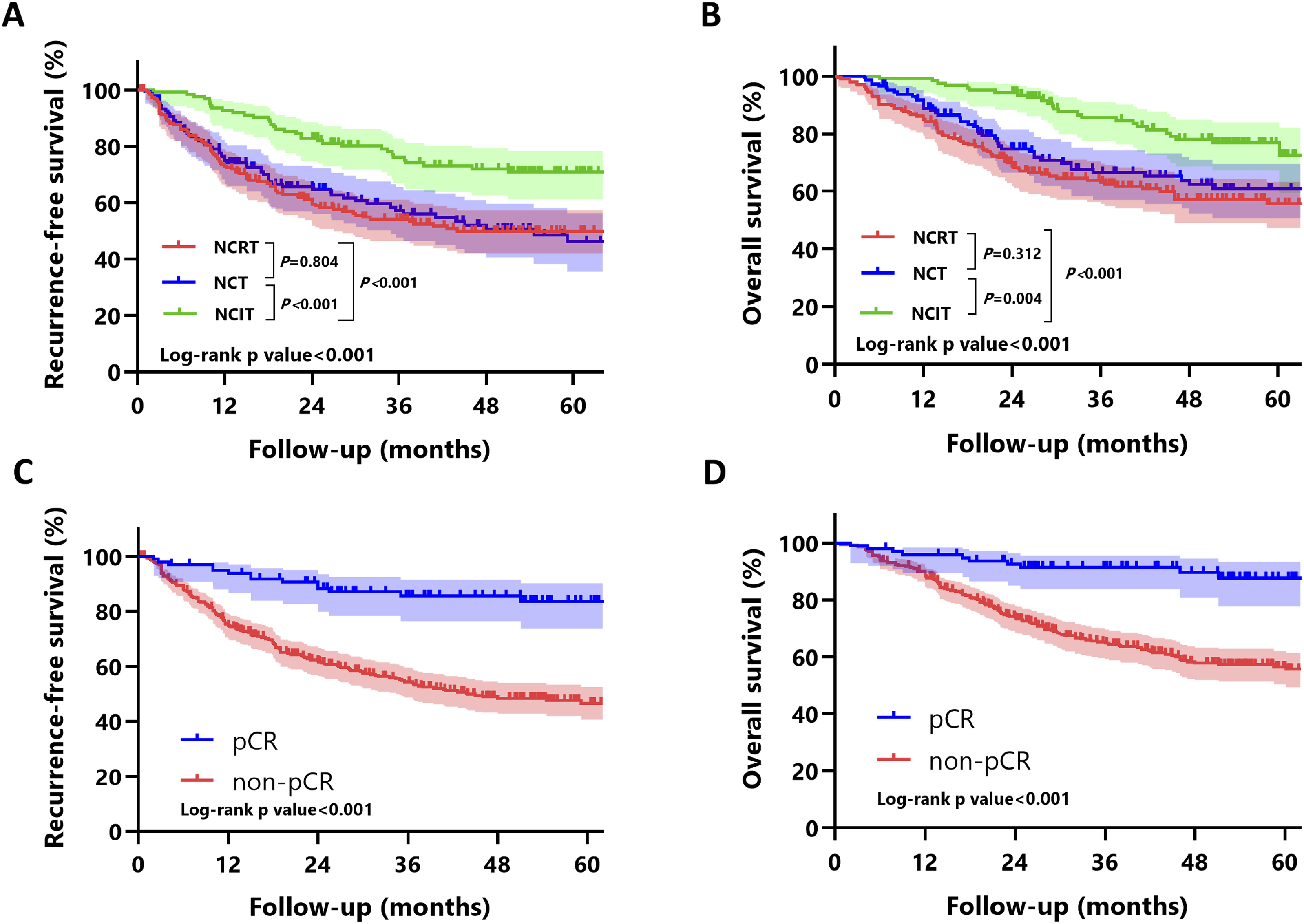
Univariate and Multivariate Cox Regression Analyses of Characteristics Associated With Overall Survival and Disease-free Survival
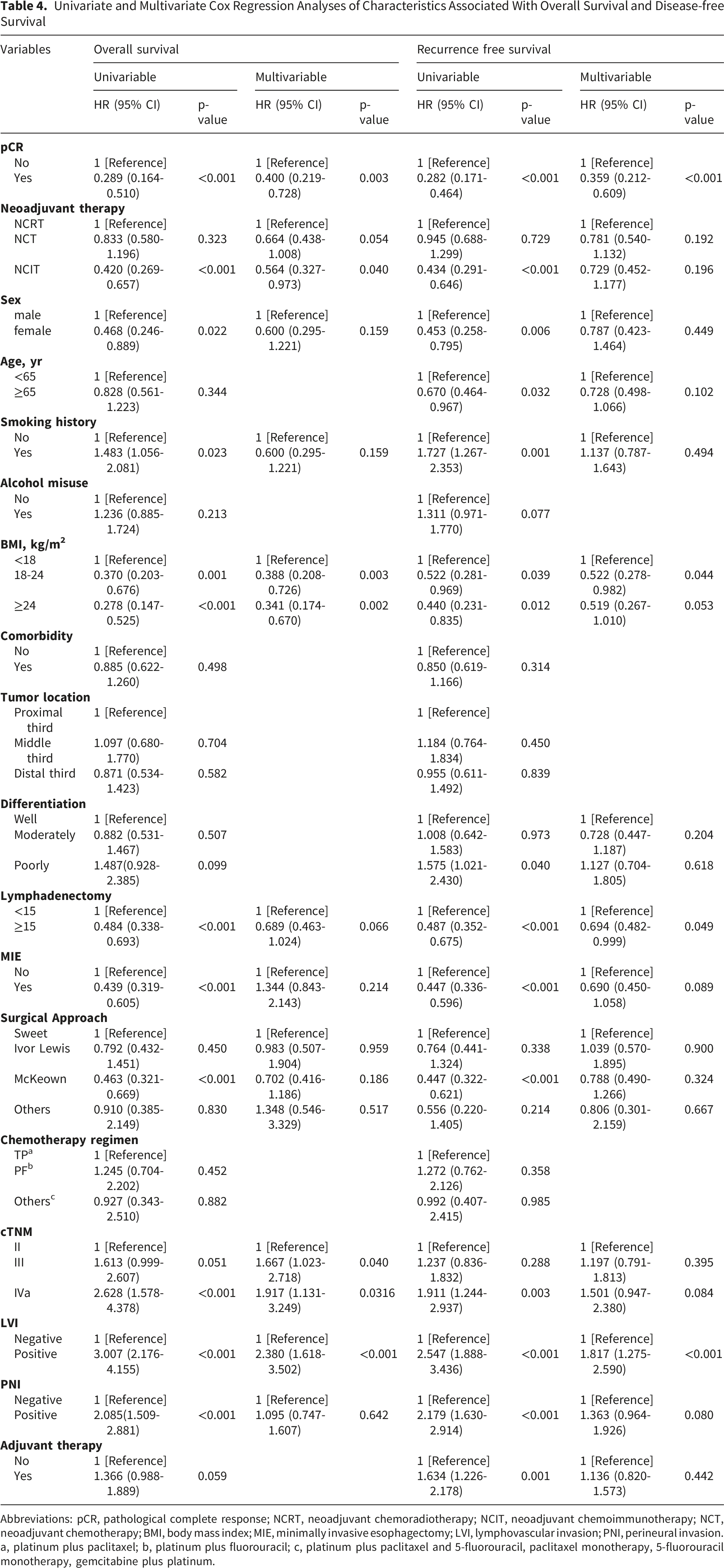
Abbreviations: pCR, pathological complete response; NCRT, neoadjuvant chemoradiotherapy; NCIT, neoadjuvant chemoimmunotherapy; NCT, neoadjuvant chemotherapy; BMI, body mass index; MIE, minimally invasive esophagectomy; LVI, lymphovascular invasion; PNI, perineural invasion. a, platinum plus paclitaxel; b, platinum plus fluorouracil; c, platinum plus paclitaxel and 5-fluorouracil, paclitaxel monotherapy, 5-fluorouracil monotherapy, gemcitabine plus platinum.
Additionally, we found that ESCC patients who achieved pCR had significantly better survival outcomes compared to non-pCR patients. Throughout the follow-up period, the pCR group demonstrated significantly higher OS and RFS than the non-pCR group (5-year OS: 87.7% vs. 55.6%, log-rank p < 0.001; 5-year RFS: 83.6% vs. 46.7%, log-rank p < 0.001) (Figure 6C and D). This survival benefit was observed across all three treatment modalities (Figure S1). In the NCRT group, patients who achieved pCR had significantly better RFS and OS than those without pCR (both log-rank p < 0.001; Figure S1A and S1B). In the NCT group, pCR was associated with numerically improved survival; however, the differences in RFS and OS did not reach statistical significance (log-rank p = 0.298 and p = 0.368, respectively; Figure S1C and S1D). In the NCIT group, patients with pCR also demonstrated significantly better RFS and OS compared with non-pCR patients (log-rank p = 0.039 and p = 0.024, respectively; Figure S1E and S1F). Overall, these findings indicate that the survival advantage associated with pCR was consistently observed in the NCRT and NCIT groups, while a similar trend was present in the NCT group but did not reach statistical significance, possibly due to the limited number of patients who achieved pCR.
In addition, we conducted subgroup analyses of chemotherapy regimens and ICIs. The results showed no significant differences in OS (p=0.584) or RFS (p=0.447) between the TP regimen and other chemotherapy regimens (Figure S2A-B), or between PD-1 and PD-L1 inhibitors (p=0.808 and p=0.234, respectively in OS and RFS) (Figure S2C-D), indicating that different treatment regimens had limited effects on survival outcomes.
Collectively, these findings indicate that NCIT yields superior therapeutic outcomes compared to NCRT and NCT, particularly in patients achieving pCR. NCIT appears to be a promising treatment strategy, and its favorable efficacy may be attributed to its association with a higher pCR rate and a reduced risk of DM.
Propensity Score Matching Analysis
As demonstrated by the preceding survival and multivariate analyses, NCIT significantly improved OS and RFS compared to NCRT and NCT, serving as an independent prognostic factor for patients with LA-ESCC. However, given the significant baseline imbalances among the three treatment groups, we performed propensity score matching (PSM) to minimize the influence of confounding factors and ensure the robustness of our findings, despite having already adjusted for these variables using multivariate Cox regression. Furthermore, since NCRT and NCT are established standard-of-care treatments according to clinical guidelines, matching was only conducted for NCRT vs. NCIT and NCT vs. NCIT. No direct matching was performed between the NCRT and NCT groups.
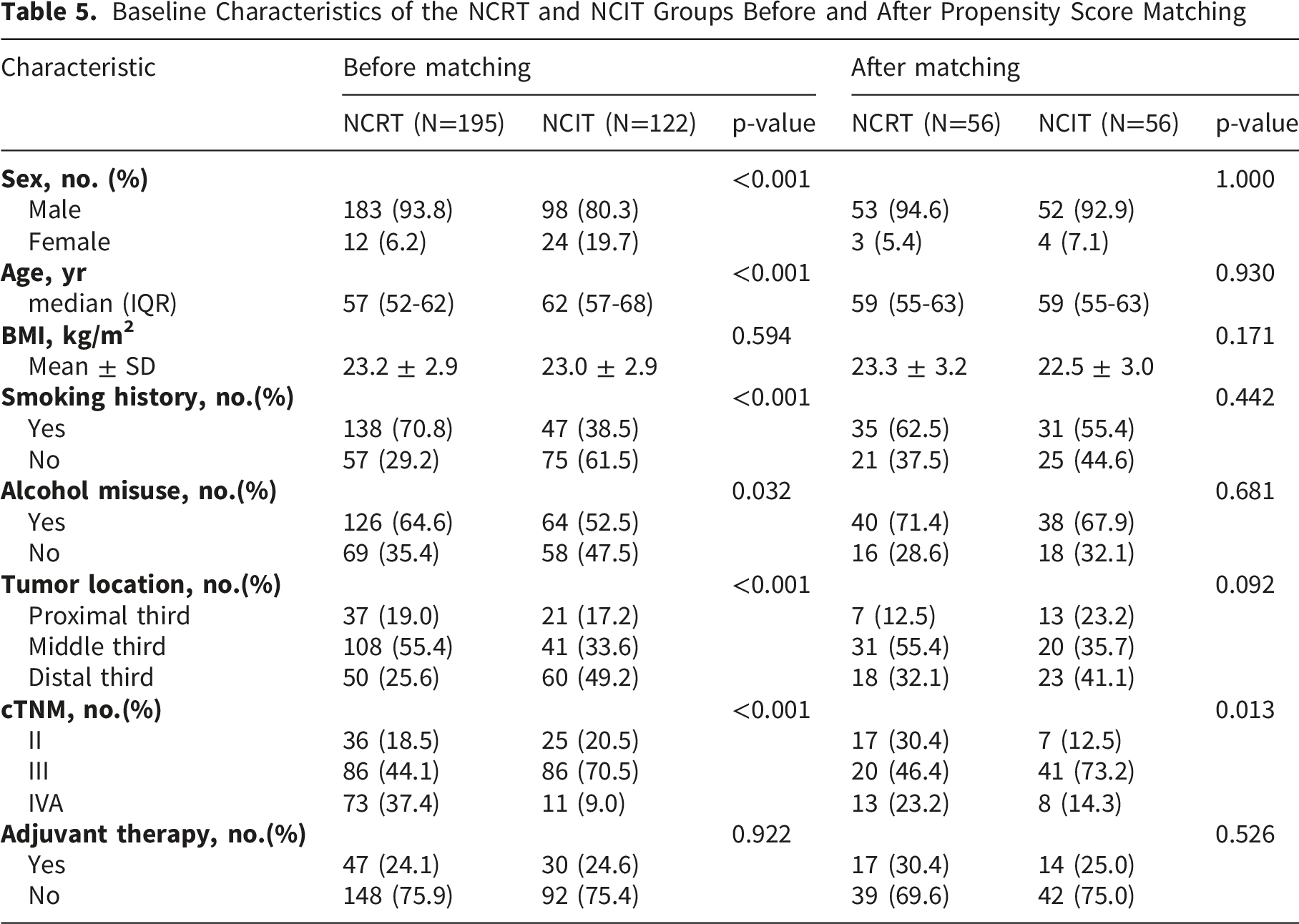
Baseline Characteristics of the NCRT and NCIT Groups Before and After Propensity Score Matching
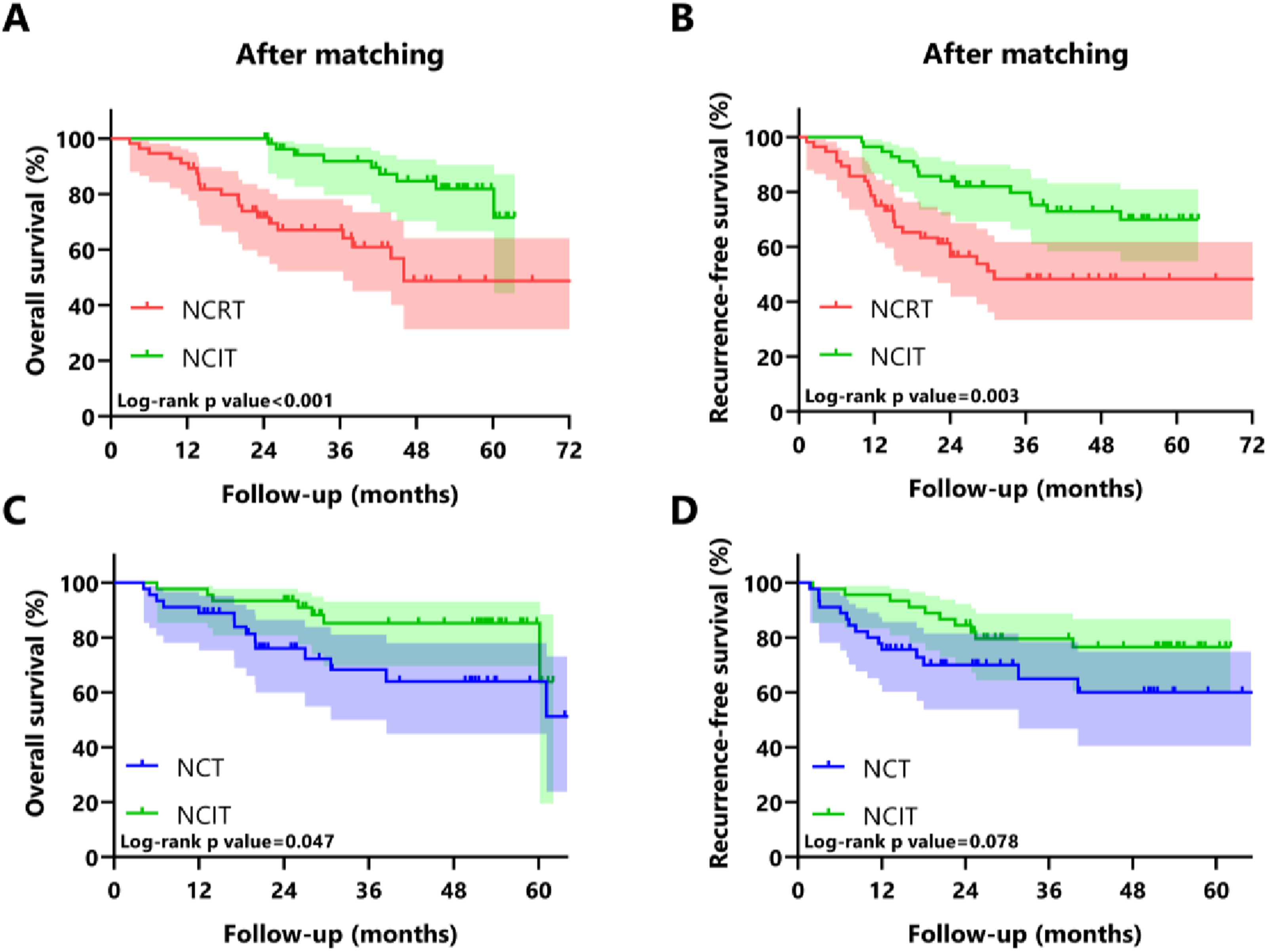
Kaplan-Meier survival curves for overall survival and recurrence-free survival comparing the NCIT, NCRT and NCT groups in the propensity score-matched cohort
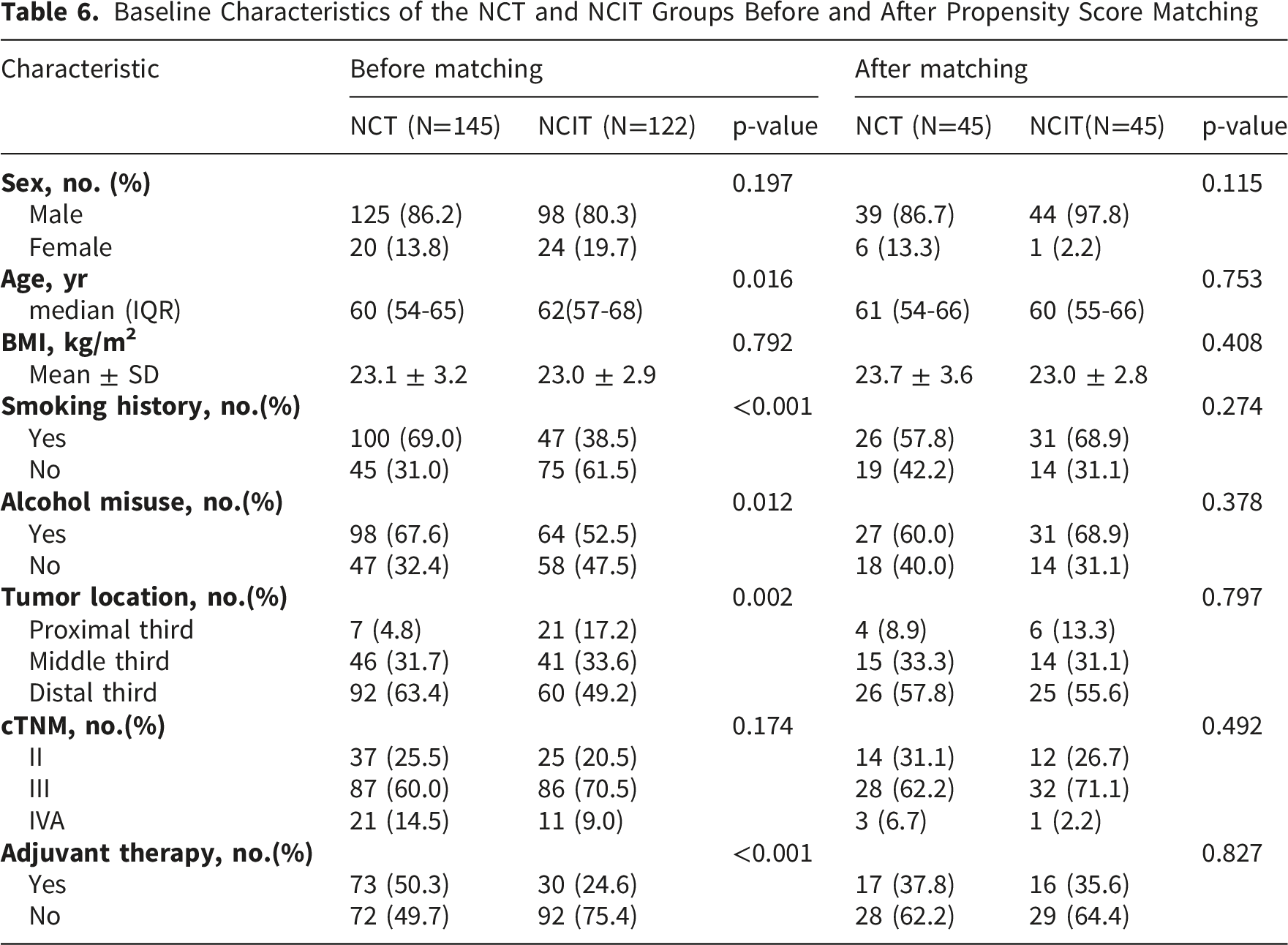
Baseline Characteristics of the NCT and NCIT Groups Before and After Propensity Score Matching
Discussion
This large-scale, retrospective three-arm comparison establishes that NCIT confers superior long-term survival over both NCRT and NCT, despite achieving a pathological response comparable to NCRT and exhibiting a distinct yet manageable safety profile.
Regarding pathological response, the pCR rate in our NCIT cohort (29.5%) was comparable to that in the NCRT group (28.7%; p = 0.880), a result consistent with several recent studies. For instance, the phase 2 REVO trial reported pCR rates of 32.7% for NCIT versus 34.6% for NCRT, 10 and a retrospective analysis by Xu et al 16 also showed no significant difference in pCR between NCIT and NCRT (29.8% vs. 34.0%; p = 0.167). These findings imply that the potent systemic immune activation elicited by NCIT can achieve a level of local tumor control comparable to that of radiotherapy-based local intensification. As expected, and in line with extensive prior evidence,8,17-19 both NCIT and NCRT were significantly more effective at inducing pCR than NCT alone (3.4%; p < 0.001). Furthermore, the consistently high R0 resection rates across all three groups highlight the technical feasibility of surgery following each of these neoadjuvant approaches. While our study focused on comparing NCIT, NCRT, and NCT, recent studies have explored the integration of ICIs into NCRT with the aim of further enhancing treatment response and survival outcomes. In the phase II NEOCRTEC1901 trial, Chen et al 20 reported that adding toripalimab to NCRT achieved a high pCR rate of 50% in patients with LA-ESCC, exceeding the historically reported pCR range of 25%–49% with NCRT alone, with an acceptable safety profile. Mechanistically, Ma and Baran 21 suggested that radiotherapy may enhance antitumor immunity by inducing tumor antigen release, promoting dendritic cell-mediated antigen presentation, activating CD8+T cells, and stimulating cGAS-STING/type I interferon signaling. ICIs may further reverse PD-1/PD-L1-mediated T-cell exhaustion and restore effector T-cell activity, thereby amplifying radiotherapy-induced immune responses. These findings support the biological rationale for NCRT plus immunotherapy as a potentially synergistic strategy to improve both local tumor control and systemic antitumor immunity. However, further validation in phase III randomized controlled trials is still warranted.
The most significant finding from our study is the substantial survival advantage demonstrated with NCIT. Patients treated with NCIT showed markedly superior 5-year OS (72.5% vs. 55.7% for NCRT and 60.8% for NCT) and RFS (70.7% vs. 49.8% for NCRT and 46.2% for NCT). This benefit remained consistent in multivariable analysis, which identified NCIT as an independent prognostic factor for both improved OS (HR, 0.564; p= 0.040), minimizing the impact of confounding factors on survival outcomes and ensuring the robustness of the comparative results. Our findings align with a growing body of evidence supporting the survival benefit of NCIT over NCRT. Yu et al 22 reported improved 3-year OS (91.7% vs. 79.8%) and DFS (87.4% vs. 72.8%) with NCIT, while Yang et al 23 also found significantly better progression-free survival (HR=0.50) in favor of NCIT. Similarly, the recent study by Guo et al 11 demonstrated superior 2-year OS and DFS with NCIT compared to NCRT. Given the long study period, temporal changes in clinical practice may have affected treatment patterns, including surgical approaches, chemotherapy regimens, and neoadjuvant treatment strategies, which could potentially influence survival outcomes. Moreover, heterogeneity in chemotherapy regimens and ICIs types may represent additional confounding factors. To minimize these potential biases, we conducted subgroup analyses according to ICI type and chemotherapy regimen. The results showed no significant differences in OS or RFS between the TP regimen and other chemotherapy regimens (Figure S2A-B), or between PD-1 and PD-L1 inhibitors (Figure S2C-D), suggesting that these treatment heterogeneities had limited effects on survival outcomes. In addition, treatment-related variables that may have changed over time, including surgical approach and neoadjuvant treatment strategy, were included in the multivariable Cox regression model. After adjustment for these factors, NCIT remained an independent prognostic factor for improved OS. Although residual confounding cannot be completely excluded due to the retrospective design and long time span of the study, these analyses helped to reduce the potential impact of temporal changes on our results and support the reliability of the observed survival benefit associated with NCIT.
Subsequently, to ensure the robustness of our findings, we employed PSM to address baseline imbalances across treatment groups prior to conducting survival analyses. The results indicated that the baseline characteristics between the NCRT and NCIT groups were largely balanced. Although the proportion of stage IV patients remained higher in the NCRT group (23.2%) compared to the NCIT group (14.3%), the NCRT group also had a notably higher proportion of stage II patients (30.4% vs. 12.5%). Consequently, the overall proportion of advanced-stage (stage III and IV) patients in the matched NCIT group (87.5%) was significantly higher than that in the NCRT group (69.6%). Despite this unfavorable baseline stage distribution, the post-matching survival analysis demonstrated that both the 5-year OS and 5-year RFS in the NCIT group remained superior to those in the NCRT group. Regarding the comparison between the NCT and NCIT groups, baseline differences were optimally balanced following PSM. Subsequent analyses revealed that the NCIT group exhibited a superior 5-year OS compared to the NCT group. While the 5-year RFS was also higher in the NCIT group, this difference did not reach statistical significance. Given the reduced sample size post-matching, this potential RFS advantage may not have been fully captured; therefore, larger sample sizes are required to validate this RFS benefit. Taken together, after mitigating the impact of confounding factors, NCIT continued to demonstrate a robust trend of survival benefit. These findings strongly warrant further large-scale, prospective studies to confirm the survival advantages conferred by NCIT.
The relationship between pathological response and survival warrants further discussion. Crucially, our analysis reaffirmed the prognostic value of achieving a pCR, as the pCR group demonstrated a significantly higher survival throughout follow-up compared to the non-pCR group (p < 0.001). Although the pCR rates between the NCIT and NCT groups were not statistically different, the NCIT group demonstrated a significant survival advantage. This finding challenges the view of pCR as a universal surrogate endpoint for survival across different neoadjuvant modalities, especially when comparing locoregional (NCRT) and systemically anti-tumor immunity strategies (NCIT). Other studies have also observed a dissociation between pCR and survival, such as the CMISG1701 study, which also reported a higher pCR with NCRT yet no OS benefit over NCT. 16 Also, in our research, the improved prognosis observed in the NCIT group can be attributed to its more effective reduction in postoperative recurrence, particularly the significant decrease in distant metastasis. We propose that the survival advantage of NCIT originates from its capacity to elicit a robust and sustained systemic immune response. By targeting tumor antigens released following chemotherapy-induced cell death, NCIT may effectively eliminate micrometastatic disease, thereby mitigating the risk of distant recurrence—the predominant pattern of treatment failure following NCRT.3,11 This phenomenon is corroborated by the superior RFS observed in our NCIT cohort and underscores the fundamental rationale for incorporating immunotherapy into neoadjuvant regimens for ESCC.
Our analysis delineated distinct safety profiles among the three neoadjuvant regimens. While the NCIT group experienced a higher total complication rate than the NCT group, within an acceptable limit. Consistent with prior literature,24,25 the NCRT group was associated with a significantly elevated risk of anastomotic leakage, potentially attributable to radiation exposure to the gastric fundus. Regarding anastomotic stricture, the NCIT group exhibited a numerically higher rate (6.6%) compared to the NCRT group (4.6%), although this difference did not reach statistical significance (p=0.455). Nevertheless, by avoiding radiotherapy, NCIT may theoretically mitigate the risk of lung function decline caused by radiation-induced fibrotic sequelae. Overall, the safety profile of NCIT was consistent with the known toxicities of its component agents, with no new safety signals identified, and was manageable in the clinical setting.
Several limitations in our retrospective study should be considered. First, despite multivariate adjustments, certain confounding factors and selection biases remain present. Second, as a single-institution study, the generalizability of our findings may be limited, and external validation through multi-center prospective studies are necessary. Finally, the median follow-up duration was longer for the NCIT and NCRT groups compared with the NCT group, potentially resulted in fewer endpoint events being captured in the NCT cohort.
Notwithstanding these limitations, our study holds considerable clinical relevance. The significant survival benefit afforded by NCIT, together with its non-inferior pathological response compared to NCRT and a manageable safety profile, supports its potential as a new standard-of-care option for LA-ESCC. NCIT represents a viable alternative to NCRT, particularly in regions with limited radiotherapy access or for patients at high risk of radiation-related toxicities. Treatment selection between NCIT and NCRT should be individualized, taking into account factors such as tumor anatomy, patient comorbidities, and tumor stage. The ongoing phase III randomized controlled trials Keystone-002 and NICE-2 are anticipated to provide high-level evidence directly comparing these strategies.26,27 Additionally, future studies should prioritize the discovery and validation of predictive biomarkers to enable precision selection of NCIT for individual patients.
Conclusion
This study highlights that NCIT offers excellent efficacy with a controllable safety profile in patients with LA-ESCC, presenting a promising treatment strategy. The excellent therapeutic effect is mainly due to its ability to decrease the recurrence rate, especially for DM. In addition, validation through ongoing large-scale phase III clinical trials is warranted to confirm our results and establish NCIT as a first-line therapeutic option in LA-ESCC.
Supplemental Material
Supplemental Material - Neoadjuvant Chemoimmunotherapy Versus Neoadjuvant Chemoradiotherapy Versus Neoadjuvant Chemotherapy for Esophageal Squamous Cell Carcinoma: A Real-World, Three-Arm, Retrospective Cohort Study From Chinese National Cancer Center
Supplemental Material for Neoadjuvant Chemoimmunotherapy Versus Neoadjuvant Chemoradiotherapy Versus Neoadjuvant Chemotherapy for Esophageal Squamous Cell Carcinoma: A Real-World, Three-Arm, Retrospective Cohort Study From Chinese National Cancer Center by Long Zhang, Zehang Zhang, Guochao Zhang, Chao Zheng, Yuzhuo Zhang, Zhichao Zuo, Shuangping Zhang, Yong Li, Yin Li and Qi Xue in Technology in Cancer Research & Treatment.
Footnotes
Ethical Considerations
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College. The committee approval number is 25/744-5691.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (82573688, 82203154); CAMS Innovation Fund for Medical Sciences (CIFMS) (No. 2025-I2M-C&T-B-058; No. 2025-I2M-C&T-B-011); National High Level Hospital Clinical Research Funding and Cooperation Fund of CHCAMS Beijing & Langfang & SZCH (No. CFA202501002; No. CFA202503003); National High Level Hospital Clinical Research Funding (N0. LC2024D01); Fundamental Research Program of Shanxi Province (202203021221282).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.