
Abstract
TIPE3, encoded by the human TNFAIP8L3 gene, is a member of the TNFAIP8 family of lipid second-messenger transfer proteins that connects phosphoinositide signaling with cancer progression, therapeutic resistance, and clinical outcomes. Unlike other TIPE-family members primarily involved in immune regulation or apoptosis, TIPE3 directly transfers phosphatidylinositol 4,5-bisphosphate (PIP2) and phosphatidylinositol 3,4,5-trisphosphate (PIP3) and modulates the PI3K/AKT, MEK/ERK, Wnt/β-catenin, NF-κB, Hedgehog, and mitochondrial stress pathways. Current evidence indicates that TIPE3 generally facilitates tumor growth, invasion, immune remodeling, autophagy, and platinum resistance across various malignancies, including lung, breast, pancreatic, gastric, colorectal, ovarian, cervical cancers, glioblastoma, and acute myeloid leukemia, whereas it may exhibit tumor-suppressive effects in specific contexts, such as head and neck squamous cell carcinoma. This review emphasizes three key concepts: pan-cancer functional duality, localization- and epigenetic-dependent regulation, and TIPE3-guided therapeutic stratification. We also examine conflicting findings, particularly in colorectal cancer, where disparities in mRNA versus protein assessment, tumor composition, immune contexture, subcellular localization, and treatment exposure may contribute to inconsistent prognostic associations. Finally, we propose a translational framework that integrates standardized detection, localization-aware pathology, multi-omics profiling, organoid and patient-derived xenograft validation, AI-assisted inhibitor discovery, RNA-based delivery, and rational combination therapy. Although no TIPE3-targeted therapies have yet reached clinical application, emerging mechanistic and drug discovery studies underscore TIPE3’s potential as a valuable biomarker and therapeutic target in precision oncology.
1. Introduction
Cancer remains a leading threat to global health, driving an urgent need for sustainable innovations in clinical management and therapeutic strategies. 1 In this context, the ongoing discovery and application of molecular biomarkers are transforming oncology practice, establishing precision medicine as a fundamental component of modern cancer care.2-4 The tumor necrosis factor alpha inducible protein 8-like (TNFAIP8) family has emerged as a novel class of biomarkers with promising potential for personalized therapy. The TNFAIP8 family comprises four structurally homologous proteins: TIPE (TNFAIP8), TIPE1 (TNFAIP8L1), TIPE2 (TNFAIP8L2), and TIPE3 (TNFAIP8L3). Each member contains a conserved TIPE homology domain and a central hydrophobic cavity capable of accommodating lipid molecules, but they differ substantially in tissue distribution, immune-regulatory function, and signaling selectivity.5,6 TIPE is widely involved in cell survival, inflammation, resistance to apoptosis, and tumor progression, whereas TIPE1 is more frequently associated with the regulation of apoptosis and context-dependent tumor suppression.7,8 TIPE2 is most accurately described as a negative regulator of immune activation that maintains immune homeostasis. Previous studies have also suggested that TIPE2 may function as a tumor suppressor in selected malignancies.9-11 In contrast, TIPE3 is characterized by its capacity to transfer phosphoinositide second messengers, particularly PIP2 and PIP3, thereby amplifying PI3K/AKT and MEK/ERK signaling pathways in epithelial and cancer cells. 12
TIPE3 was identified as a transfer protein for phosphatidylinositol 4,5-bisphosphate (PIP2) and phosphatidylinositol 3,4,5-trisphosphate (PIP3), thereby facilitating the activation of PI3K/AKT and MEK/ERK signaling pathways. The N-terminal region is functionally significant, as its truncation markedly diminishes oncogenic activity and modifies its capacity to interact with key downstream pathways. 13 The protein is frequently expressed in epithelial-derived tumors and has been implicated in non-small cell lung cancer (NSCLC), breast cancer, pancreatic cancer, gastric cancer, colorectal cancer (CRC), ovarian cancer, cervical cancer, glioblastoma (GBM), and hematologic malignancies.14-16
However, TIPE3 cannot be regarded as a consistently oncogenic protein. Its function depends on the tumor lineage, epigenetic state, subcellular localization, and microenvironmental context. For instance, membrane-associated TIPE3 may facilitate lipid signaling and tumor progression in NSCLC, whereas cytoplasmic TIPE3 could exert distinct or even inhibitory effects in certain contexts. 17 In head and neck squamous cell carcinoma (HNSCC), TNFAIP8L3 promoter hypermethylation and reduced TIPE3 expression have been associated with tumor progression, while restoration of TIPE3 activity can induce mitochondrial dysfunction and apoptosis. 18 This functional duality is clinically important as a strategy designed to inhibit TIPE3 in one tumor type may be inappropriate in another.
This review synthesizes the current evidence on TIPE3 in cancer with three objectives: first, to characterize the pan-cancer duality of TIPE3 as either an oncogenic driver or a context-dependent tumor suppressor. Second, to elucidate how subcellular localization, epigenetic regulation, and interactions within the tumor microenvironment influence TIPE3 function. Third, to propose strategies for biomarker development, therapeutic stratification, and targeted intervention that are both localization-aware and disease-specific.
2. Oncogenic Functions of TIPE3 Across Cancer Types
As shown in Figure 1, TIPE3 primarily promotes tumorigenesis across a broad range of cancers. However, its functions are highly specific to tumor type, involving distinct downstream signaling pathways to facilitate malignancy. TIPE3-mediated signaling pathways and localization-dependent functions in cancer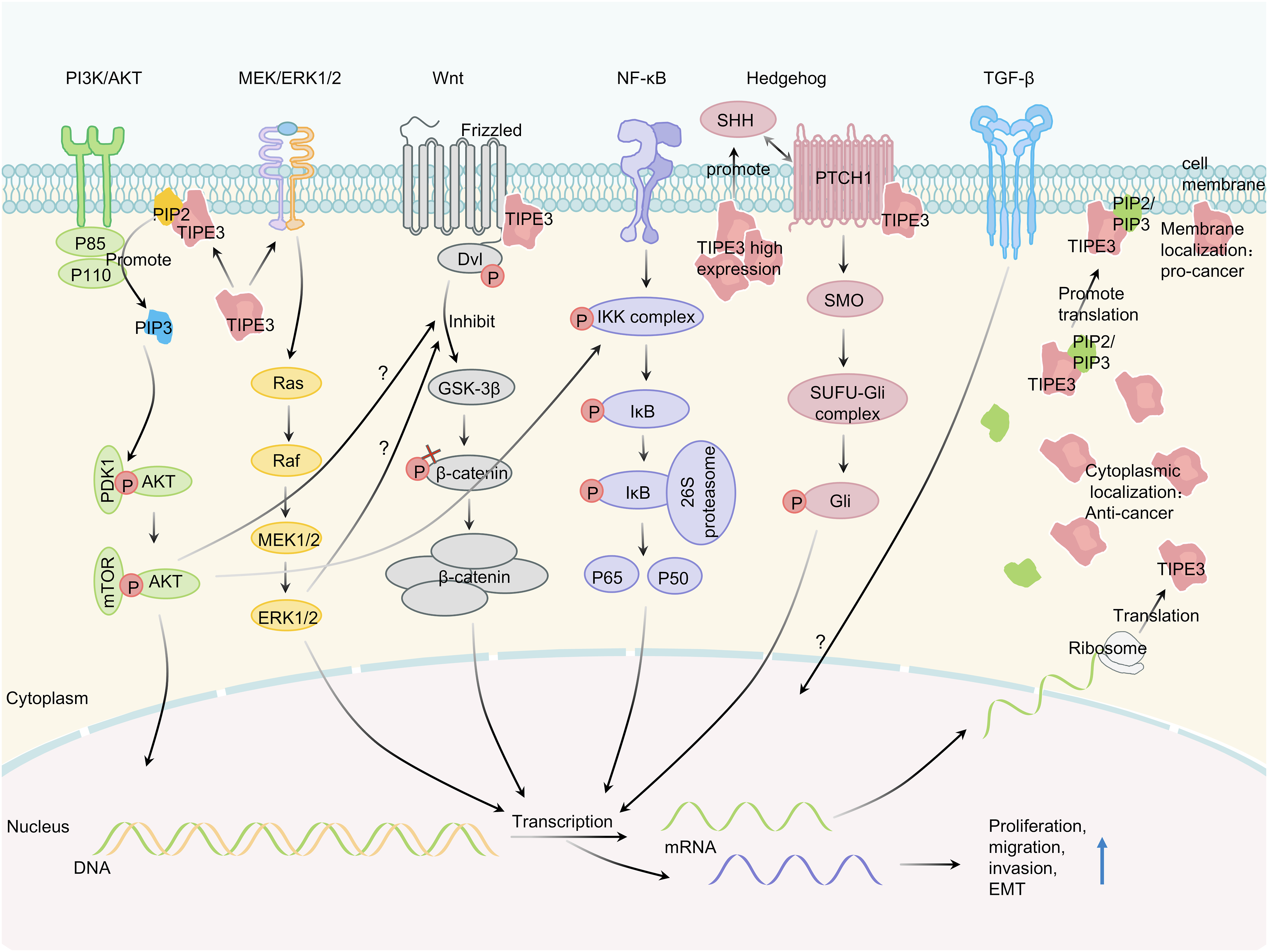
TIPE3 promotes hallmark cancer phenotypes in various carcinomas through recurrent molecular pathways. In NSCLC, elevated TIPE3 enhances proliferation, epithelial-mesenchymal transition (EMT), angiogenesis, and metastasis through the activation of the AKT/mTOR, Wnt/β-catenin, and NF-κB signaling pathways, whereas its knockdown or knockout significantly suppresses tumor growth and dissemination.14,19,20 A key molecular interaction with RAC1 further promotes invasiveness, and the co-expression of both proteins strongly predicts poor patient survival. 21 Notably, the function of TIPE3 in NSCLC is spatially dependent: membrane-localized TIPE3 promotes tumorigenesis, whereas its cytoplasmic form may exert tumor-suppressive effects. 17
Similarly, in breast cancer, TIPE3 expression is associated with pathological grade, lymph node metastasis, and unfavorable prognosis. It facilitates progression through the AKT/NF-κB axis by upregulating MMP2 and uPA, as well as via the AKT/GSK3β/β-catenin/Snail pathway. Moreover, TIPE3 levels exhibit a positive correlation with HER2 expression, indicating synergistic tumor-promoting effects. In gastric cancer, although TIPE3 expression is generally lower in tumor tissues, elevated TIPE3 levels are still associated with poorer survival. Both the long and short isoforms promote proliferation, migration, and invasion primarily through PI3K/AKT activation, with the short isoform exhibiting greater potency. The oncogenic activity is inhibited by the tumor-suppressive microRNA miR-9-5p. 22
Studies on pancreatic cancer have identified elevated TIPE3 expression as an independent poor prognostic factor associated with lymph node metastasis. It facilitates malignant behavior via a RAC1-dependent mechanism that upregulates RhoA and MMP9 (Figure 2).
16
A Chinese experimental study reported that TIPE3 may attenuate CDDP-induced apoptosis in cervical cancer cells, suggesting a possible role in platinum resistance.
23
In ovarian cancer, TIPE3 acts as an oncogenic regulator, contributing to tumor malignancy and poor patient survival. It may enhance immunosuppression by activating the TGF-β signaling pathway, thereby impairing macrophage antigen presentation. Prognostic models incorporating TIPE3 have demonstrated superior accuracy to traditional staging methods in identifying high-risk patients and predicting recurrence, highlighting its potential for guiding individualized therapy.24-26 Tumor type-specific molecular interactions of TIPE3 in cancer progression and suppression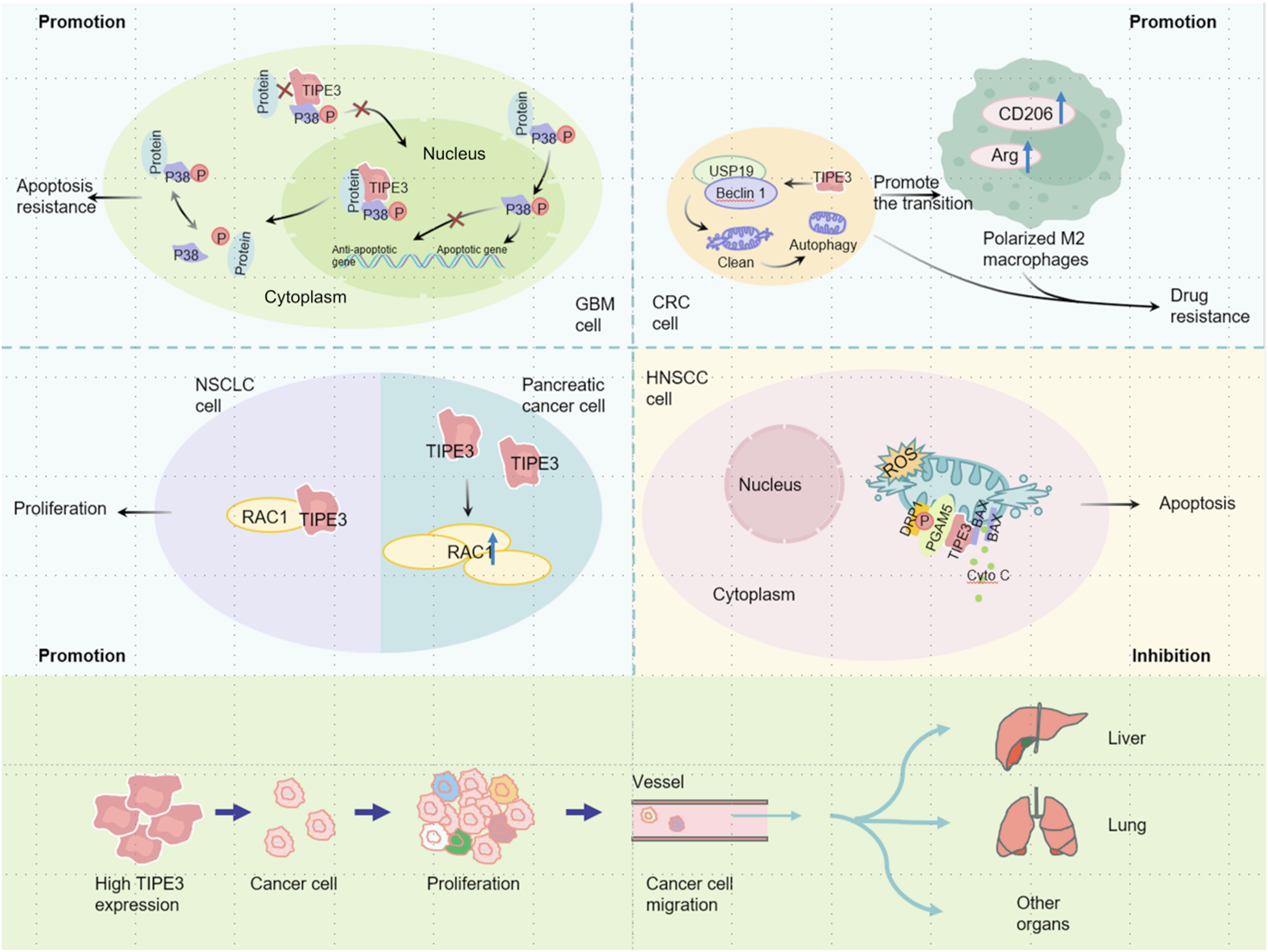
In addition to these common pathways, TIPE3 functions through distinct, tissue-specific mechanisms. In glioblastoma (GBM), TIPE3 is primarily localized in the cytoplasm, and its increased expression is associated with higher tumor grade and unfavorable prognosis. Mechanistically, TIPE3 directly interacts with p38 MAPK through its N-terminal domain within the cytoplasm (Figure 2). This interaction suppresses p38 phosphorylation and impedes its nuclear translocation, leading to reduced levels of nuclear phospho-p38 and subsequent inactivation of the p38 MAPK pathway. Consequently, the expression of downstream pro-apoptotic genes is suppressed, thereby conferring resistance to apoptosis and facilitating the survival of GBM cells. The binding is independent of p38 kinase activity and does not disrupt its nucleocytoplasmic shuttling, which is principally regulated by phosphorylation status. The essential role of the N-terminal domain is demonstrated by the inability of a truncated short-TIPE3 variant to bind p38. Notably, the cytoplasmic localization of TIPE3 in GBM contrasts with its membrane-associated distribution in NSCLC, highlighting the tumor-type-specific regulation of its function. 27 In oral squamous cell carcinoma, its role is notably independent of AKT; instead, it predominantly regulates the phosphorylation of mTOR and STAT3 to promote tumor cell survival and proliferation. 28
Bioinformatics analysis of acute myeloid leukemia (AML) indicates that TIPE3 expression is significantly upregulated and correlates with a high percentage of bone marrow blasts, although it does not constitute a strong independent prognostic factor for overall survival. Furthermore, its expression exhibits a positive correlation with the infiltration of myeloid-derived suppressor cells (MDSCs), indicating a potential role in modulating an immunosuppressive tumor microenvironment. 29
Head and neck cancers serve as the most illustrative example of context dependence. In nasopharyngeal carcinoma (NPC), epigenetic activation of TIPE3 via enhancer-associated mechanisms involving KAT2A and SETD7 contributes to tumor progression through Hedgehog signaling.30,31 In contrast, HNSCC frequently exhibits promoter hypermethylation and reduced TIPE3 expression, and restoration of TIPE3 activates the PGAM5-DRP1 mitochondrial pathway to promote apoptosis. 18
In CRC, clinical and mechanistic studies increasingly support a pro-tumorigenic role for TIPE3, but the literature is not fully consistent. TIPE3 protein is upregulated in CRC tissues in some cohorts and correlates with immune infiltration and poor outcome. A 2025 mechanistic study further showed that TIPE3 promotes oxaliplatin resistance by enhancing autophagy through the USP19/Beclin1 pathway and by stimulating macrophage polarization toward an M2-like phenotype.32,33 Conversely, other analyses suggest that low TIPE3 expression may be associate with better immune-checkpoint inhibitor responsiveness, possibly through links with higher tumor mutational burden and distinct immune infiltration patterns. These apparently conflicting findings may reflect differences in mRNA versus protein assessment, bulk transcriptomic versus spatial localization readouts, tumor-stage distribution, microsatellite instability or immune-subtype composition, antibody specificity, scoring thresholds, and treatment context.34,35 Therefore, CRC should be viewed as a model in which TIPE3 may function differently across molecular and immune subtypes rather than as a tumor type with a single linear association.
Expression Patterns, Functional Roles, Molecular Mechanisms, and Clinical Significance of TIPE3 Across Various Tumor Types
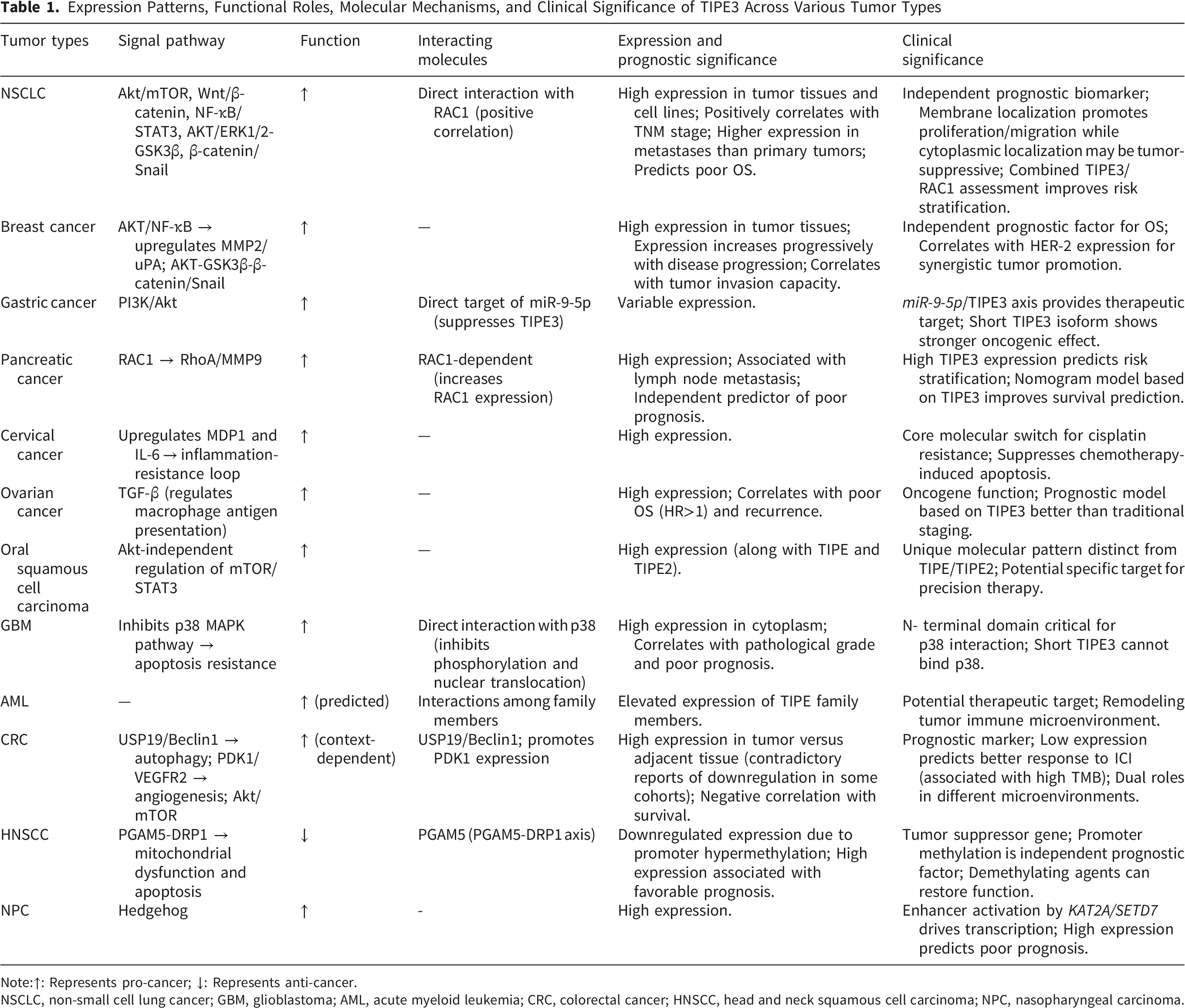
Note:↑: Represents pro-cancer; ↓: Represents anti-cancer.
NSCLC, non-small cell lung cancer; GBM, glioblastoma; AML, acute myeloid leukemia; CRC, colorectal cancer; HNSCC, head and neck squamous cell carcinoma; NPC, nasopharyngeal carcinoma.
3. Context-dependent Tumor-Suppressive Roles of TIPE3
Although TIPE3 is often associated with tumor-promoting activities, evidence from certain cancer types suggests that it may also exert tumor-suppressive properties. This functional divergence appears to be influenced by tumor lineage, epigenetic regulation, subcellular localization, and pathway context, rather than by an inherent, fixed property of the protein.
HNSCC serves as the clearest example of the tumor-suppressive role of TIPE3. In this context, TNFAIP8L3 promoter hypermethylation is associated with decreased TIPE3 expression and tumor progression. The restoration of TIPE3 expression suppresses proliferation, migration, and invasion in vitro, and inhibits tumor growth in vivo. Mechanistically, TIPE3 interacts with PGAM5 and promotes DRP1-dependent mitochondrial dysfunction, leading to the accumulation of reactive oxygen species, activation of mitochondrial apoptotic signaling, and subsequent tumor cell apoptosis. In HNSCC, these findings indicate that the loss of TIPE3 may facilitate malignant progression, whereas the restoration of TIPE3 activity could serve as a context-specific therapeutic strategy. The contrast between NPC and HNSCC further demonstrates that distinct epigenetic regulatory elements may result in divergent TIPE3 expression patterns and functional outcomes across anatomically related tumors.18,30,31
TIPE3 also exhibits localization-dependent functional heterogeneity in NSCLC. Membrane-associated TIPE3 promotes tumor cell proliferation, migration, and tumor growth by activating AKT/ERK-related signaling pathways, with its membrane expression correlating with more advanced clinicopathological features. In contrast, cytoplasmic TIPE3 seems to exert distinct biological effects and may not fully recapitulate lipid-transfer-dependent oncogenic signaling. This spatial segregation supports the notion that the biological effect of TIPE3 expression depends not only on its abundance but also on its intracellular localization. 17
Overall, the tumor-promoting or tumor-suppressive activity of TIPE3 is determined by a complex interaction among cancer type, epigenetic state, subcellular localization, signaling pathway selection, immune microenvironment, and mitochondrial integrity. These observations suggest that a uniform therapeutic strategy for TIPE3 across different cancers may not be appropriate. Future approaches should determine whether TIPE3 ought to be inhibited, restored, or functionally redirected based on the disease-specific molecular context.
4. Clinical Significance of TIPE3 as a Candidate Prognostic Biomarker and Stratification Factor
The tumor-type-dependent expression pattern and functional duality of TIPE3 provide a rationale for evaluating it as a candidate prognostic biomarker and stratification factor. Numerous studies have linked TIPE3 expression and related molecular interactions to aggressive clinicopathological features, metastasis, survival outcomes, and treatment resistance in pancreatic cancer, NSCLC, oral cancer, and CRC.16,17,28,32 However, the strength of clinical evidence varies among tumor types, and the current findings should be regarded as hypothesis-generating rather than as grounds for immediate changes in clinical practice.
For clinical translation, the evaluation of TIPE3 should extend beyond merely assessing bulk expression levels. Protein abundance, subcellular localization, co-expression with pathway partners such as RAC1, autophagy-related activity, macrophage polarization, and the tumor immune contexture may all affect the prognostic or predictive significance of TIPE3. This is particularly relevant in CRC, where inconsistent associations between TIPE3 expression and outcome may reflect differences in mRNA versus protein detection, molecular subtype, immune infiltration, treatment exposure, and localization-specific function.17,21,33-35
Therefore, TIPE3 may be most useful as part of an integrated biomarker framework rather than as a single standalone marker. In future studies, TIPE3-based stratification should be evaluated together with established clinicopathological variables and disease-specific molecular features, such as MSI/TMB status in CRC, RAC1-associated signaling in pancreatic cancer and NSCLC, and epigenetic status in head and neck cancers. Such integrated models may support risk stratification, treatment-response prediction, and patient selection for TIPE3-directed or TIPE3-informed therapeutic strategies after prospective validation.
At present, several barriers limit the clinical implementation of TIPE3. These include the retrospective nature and limited size of many available cohorts, the lack of standardized antibodies and scoring thresholds, insufficient distinction between mRNA and protein-level readouts, limited localization-aware pathology, and the absence of prospective validation. Addressing these limitations will be essential before TIPE3 can be incorporated into clinical decision-making or therapeutic stratification.
5. TIPE3-Mediated Chemoresistance and Therapeutic Implications
While the clinical translation of TIPE3 as a prognostic biomarker encounters challenges, its pivotal role in mediating tumor chemoresistance represents a significant mechanistic breakthrough, providing compelling evidence of its value in personalized medicine.
Research has demonstrated that the overexpression of TIPE3 regulates the cell cycle and promotes the proliferation of CRC cells. 33 In the context of the FOLFOX regimen, a standard treatment for CRC designed to enhance efficacy and minimize side effects, TIPE3 mediates resistance through multiple pathways. It promotes autophagosome formation via the USP19/Beclin1 axis, thereby enhancing autophagy and reducing oxaliplatin (L-OHP)-induced cellular damage and apoptosis. Concurrently, TIPE3 overexpression promotes M2 macrophage polarization, remodeling the tumor immune microenvironment to indirectly promote tumor cell survival and drug resistance. Consequently, CRC cells with high TIPE3 expression exhibit considerable resistance to L-OHP-based chemotherapy. Similarly, in cervical cancer, TIPE3 serves as a key mediator of cisplatin resistance, not only by directly inhibiting cisplatin-induced apoptosis but also by activating a pro-survival inflammatory feedback loop through the upregulation of MDR1 and IL-6, thereby accelerating disease progression. 23
Tumor drug resistance arises from alterations in both intrinsic cellular pathways and the extrinsic microenvironment. TIPE3 facilitates this process through dual mechanisms: direct regulation of tumor cell behavior and modification of the tumor microenvironment. 36 Targeting TIPE3 therefore represents a promising strategy to overcome resistance, particularly L-OHP resistance in CRC. To optimize the efficacy of such therapeutic interventions, single-cell sequencing may be employed to dynamically monitor TIPE3 expression throughout therapy, enabling real-time treatment adjustments and personalized precision strategies. 37
Novel therapeutic agents could be developed to inhibit the USP19/Beclin1 pathway and delivered through targeted systems or in combination with multi-target inhibitors and anti-angiogenic drugs. This strategy would suppress autophagosome formation, prevent M2 polarization, and downregulate anti-apoptotic proteins, thereby remodeling the tumor microenvironment, reversing TIPE3-mediated drug resistance, delaying or preventing its onset, and ultimately improving patient prognosis. 38
In addition to these cancers, TIPE3 also promotes epithelial-mesenchymal transition (EMT), indicating its potential role in conjunction with tumor cell plasticity in conferring resistance to targeted therapies. 39 Combining EMT inhibition with pharmacological treatment may facilitate the elimination of resistant cells or the restoration of drug sensitivity. Regular monitoring of resistance markers and adaptive treatment modulation may further reduce the incidence of non-genetic resistance.
6. Emerging TIPE3-Targeted Therapeutic Strategies
The role of TIPE3 in cancer development is characterized by significant duality and tumor-type specificity, functioning as an oncogene in malignancies such as breast and gastric cancers, while exhibiting tumor-suppressive activity in specific contexts such as HNSCC. The following section systematically outlines the feasible directions for future research on precision medicine and targeted therapy focusing on TIPE3.
TIPE3 mediates reversible phosphatidylinositol transport, with its subcellular localization exhibiting tumor-specific patterns. These differential localization patterns may lead to conflicting prognostic outcomes, even within the same type of cancer. This context-dependent functional paradox establishes TIPE3 as a highly promising and context-specific prognostic biomarker, providing a theoretical basis for the development of individualized diagnostic and therapeutic systems guided by molecular typing. Currently, therapeutic strategies targeting TIPE3 remain in the preclinical stage, with no specific drugs having progressed to clinical trials. 40 Current intervention approaches predominantly focus on the tissue-specific functional heterogeneity, with experimental efforts encompassing multiple levels, including RNA,41,42 DNA,43,44 and protein,38,45 and involving epigenetic regulation, subcellular localization interventions, and bidirectional functional modulation. Furthermore, utilizing TIPE3’s cancer-specific prognostic predictive capabilities to develop a dedicated feature-scoring system may enhance risk stratification, improve predictive accuracy, and serve as a foundation for patient selection in future clinical trials.
Proposed Future Intervention Strategies for TIPE3

At the molecular level, future research should employ tools such as AlphaFold2 50 to predict the N-terminal membrane-binding site of TIPE3, facilitating the design of allosteric inhibitors or PROTAC degraders to inhibit its membrane localization, 51 while also utilizing BET/KAT2A inhibitors to intervene in epigenetic activation and regulate its expression at its origin. 52 At the cellular level, CRISPR gene editing combined with multi-omics validation can be employed to screen and validate interfering peptides in organoid models, 53 while integrated phosphoproteomic and lipidomic analysis can elucidate pathway dependencies. 54 In both preclinical and clinical phases, research should advance toward dynamic monitoring in PDX models and real-world studies, 55 employing ADCs or liposomal siRNA for precise delivery. 56 These stages should also incorporate stratified interventions based on membrane versus cytoplasmic localization of TIPE3, using basket or umbrella trial designs.
The primary breakthrough lies in implementing intelligent strategies, including AI-driven prediction of off-target effects, reversible RNA editing, and the synergistic targeting of metabolic and immune pathways. Integrating spatial omics with single-cell multi-omics technologies will facilitate a systematic analysis of the cellular composition and spatial ecology of TIPE3-high tumors. AI modeling can subsequently predict optimal regimens for targeted immune synergy. This integrated strategy may help prioritize TIPE3-directed therapeutic hypotheses and support biomarker-enriched preclinical and early-phase clinical studies.
7. Current Limitations and Future Perspectives
Although increasing evidence supports the biological and clinical significance of TIPE3 in cancer, several limitations must be acknowledged when interpreting the existing literature. The majority of existing clinical studies are retrospective and involve relatively limited patient cohorts, which may compromise the robustness of multivariable prognostic conclusions. Moreover, transcriptomic analyses based on bulk mRNA expression may not accurately represent TIPE3 protein abundance, subcellular localization, or functional activity. This distinction is particularly important because the function of TIPE3 seems to be substantially influenced by its distribution between the membrane and the cytoplasm. Furthermore, variations in antibody clones, staining procedures, scoring methodologies, and cut-off values may contribute to inter-study variability and limit direct comparisons across cohorts. Therefore, future studies should incorporate standardized pathological assessments, protein-level validation, and localization-specific evaluations to improve the reproducibility and clinical interpretability of TIPE3-based biomarkers.
Colorectal cancer serves as a representative example of these unresolved issues. Several studies have indicated that TIPE3 is upregulated in CRC tissues and may promote tumor progression, autophagy, macrophage polarization, and chemoresistance, thereby supporting its oncogenic role and association with therapy resistance in this disease.33,34 However, other analyses suggest that lower TIPE3 expression may be associated with a more favorable immune contexture and better predicted response to immune checkpoint inhibitors, potentially due to a higher tumor mutational burden and distinct patterns of immune infiltration.34,35 These findings should not be regarded as inherently contradictory. Instead, they may represent biological heterogeneity among CRC subgroups, including variations in microsatellite instability status, tumor mutational burden, consensus molecular subtype, stromal abundance, macrophage polarization, chemotherapy exposure, and TIPE3 subcellular localization. Therefore, CRC characterized by high TIPE3 expression, active autophagy, and abundant macrophages may represent a biologically distinct state from CRC exhibiting low TIPE3 expression, high tumor mutational burden (TMB), and an immune-inflamed phenotype.
Several mechanistic and translational issues remain to be addressed. It remains unclear whether TIPE3 directly regulates immune cell phenotypes or predominantly influences the tumor immune microenvironment through tumor cell-derived paracrine signaling. The necessity of membrane recruitment in TIPE3-driven oncogenic signaling also warrants further clarification, especially given that membrane localization has been associated with pro-tumor signaling in NSCLC, whereas cytoplasmic localization may correspond to distinct biological effects. 17 In addition, the clinical significance of TIPE3 isoforms, the tissue-specific effects of TIPE3 inhibition, and the potential toxicity associated with targeting TIPE3 in normal epithelial tissues remain inadequately characterized. Although deep learning-based small-molecule inhibitors of TIPE3 have recently been identified, their therapeutic selectivity and in vivo efficacy remain to be systematically validated. 40 Addressing these challenges will require integrated approaches that combine standardized immunohistochemistry, spatial profiling, single-cell analysis, organoids, patient-derived xenografts, genetically engineered models, and longitudinal treatment-response cohorts.
8. Conclusion
TIPE3 is an emerging lipid second-messenger transfer protein that connects phosphoinositide signaling, subcellular localization, tumor progression, immune remodeling, and chemoresistance. The available evidence supports TIPE3 as a biologically significant cancer regulator, but its clinical interpretation must consider tumor lineage, epigenetic status, intracellular localization, and microenvironmental context. The most important conceptual advancement is that TIPE3 should not be regarded as a uniformly oncogenic marker; instead, it functions as a context-dependent node that may either facilitate malignancy or, in specific situations, support tumor-suppressive signaling.
The next phase of TIPE3 research should advance from descriptive expression studies to standardized localization-aware assays, mechanistic validation in clinically relevant models, and biomarker-driven therapeutic strategies for translation. If these requirements are fulfilled, TIPE3 may prove valuable for prognostic stratification, prediction of chemotherapy resistance, and development of rational combination therapies in precision oncology.
Footnotes
Consent to Participate
This article does not contain any studies with human or animal participants.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Young Talent of Lifting Engineering for Science and Technology in Shandong, China (No. SDAST2024QTA032), Wu Jieping Medical Foundation Clinical Research Special Fund (No. 320.6750.2024-17-41).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Use of Artificial Intelligence
OpenAI ChatGPT was used to assist with language polishing. No AI tool was used to generate or modify scientific data. The authors critically reviewed and edited all AI-assisted content and take full responsibility for the accuracy, integrity, originality, and final content of the manuscript.